
Abstract
This study explored associations between perceived neighborhood walkability and neighborhood-based physical activity (NB-PA) and assessed possible moderation effects of the amount of time spent in the home neighborhood and individual characteristics (i.e., educational level and health-related problems). In 2016 to 2017, 509 Dutch adults, living in the South Limburg area, were included. Context-specific PA levels were measured using the Actigraph GT3X+ accelerometer and the Qstarz BTQ1000XT GPS-logger. Perceived neighborhood walkability, level of education, work status, and health-related quality of life were measured with validated self-report instruments. Results showed that individuals with a lower level of education or health-related problems spent more time in the home neighborhood. The perceived neighborhood walkability only affected NB-PA for individuals spending a relatively large amount of time in their home neighborhood. PA-facilitating features in the home neighborhood, for example, aesthetics, were only associated with more NB-PA for individuals without health-related problems or with a higher level of education.
Keywords
Introduction
Despite the growing attention being paid to physical activity (PA) and its positive effects on health, the levels of physical inactivity of the global population did not significantly change between 2001 and 2016 (Guthold et al., 2018). In 2016, the prevalence of physical inactivity in high-income Western countries was about 37% (Guthold et al., 2018). These insufficient PA levels are present throughout the population, though more disadvantaged individuals, with a lower educational level or lower socioeconomic status (SES), are less likely to engage in leisure-time PA compared with the more advantaged people in society (Demarest et al., 2014). However, socioecological models suggest that PA behavior is not only affected by personal and socioeconomic characteristics, but also by environmental and policy factors (Sallis & Owen, 2015). Accordingly, local governments are starting to adopt more upstream, structural interventions to affect the PA levels of the whole population, for example, by designing healthy, active cities and walkable environments (Capewell & Graham, 2010; Rutter et al., 2017; World Health Organization, 2018). Yet, the literature is still inconclusive about the association between the built environment and PA, partly due to differences in methods, contexts, and individuals’ exposure to the physical environment under study (Mayne et al., 2015; Stappers, Van Kann, Ettema, et al., 2018).
From a socioecological perspective, an individual’s behavior is influenced both by the environment and by individual factors (Sallis & Owen, 2015). This implies that the same physical environment might have different effects on individuals with different characteristics. SES is one of the most investigated individual factors and is mostly indicated by income, educational level, or occupational status. Goodman et al. (2013) demonstrated that new infrastructures promoting PA might be used more often by residents with a higher educational level or income and by those with a better general health. However, other studies found no interactions between the environment and neighborhood-level SES, so the evidence is still inconclusive (Mertens et al., 2017; Van Dyck et al., 2010). In addition, Alfonzo (2005) proposed the hierarchy of walking needs, arguing that the feasibility of walking, that is, the physical ability, is a fundamental factor in the relationship between environment and walking behavior.
These inconsistencies might be due to measurement bias, introduced by differences in the specificity of the measurement methods used (Mölenberg et al., 2019; Perchoux et al., 2013). PA measurements can be roughly divided into time-specific and context-specific ones. Time-specific measurements determine the total amount of PA in a certain length of time, regardless of the environment in which it took place. Over the past decades, several device-based (e.g., accelerometers and pedometers) and subjective (e.g., the International Physical Activity Questionnaire [IPAQ]) time-specific PA measurements have been developed (Craig et al., 2003). Context-specific PA measurements assess the amount of PA in a specified physical environment. As it is a complex matter to determine which physical environments people are exposed to during the day, most context-specific studies focus on the home neighborhood environment when exploring associations between the physical environment and PA. For example, the recently developed neighborhood-adapted version of the IPAQ (N-IPAQ) subjectively assesses PA levels in the home neighborhood, without explicitly defining what the home neighborhood is (Frehlich et al., 2018). In objective measurements, mostly accelerometers and global positioning systems (GPS) are used to assess the amount of PA at a specific location (Jankowska et al., 2015). In these device-based measurements, the home neighborhood is usually defined as a buffer, for example, radial or street-network buffer, around the home address. It is widely recognized that objective and subjective measurements of PA lead to different and sometimes inconsistent outcomes (Prince et al., 2008). Research also suggests that using time-specific or context-specific measurements of PA leads to differences in their association with the built environment (Troped et al., 2010). To date, it is not known whether the amount of time that individuals spend in the home neighborhood is affecting this association as well.
The abovementioned inconsistencies in the literature demand further, in-depth exploration of the relationship between the built environment and PA, using individual-level personal characteristics and context-specific PA measurements. Therefore, the first aim of this study was to explore neighborhood-based PA levels and sedentary behavior (SB) and to assess differences between more and less advantaged individuals in society, based on educational level and health-related problems. Subsequently, we assessed the associations between perceived neighborhood walkability and neighborhood-based PA. As we expected the PA behaviors of individuals who spend more time in their home neighborhood to be affected more by the perceived neighborhood walkability, the second aim was to study the effect of the time that was spent in the home neighborhood on the relationship between the perceived neighborhood walkability and neighborhood-based PA. Finally, we explored whether these associations differed for subgroups based on educational level and health-related problems.
Method
Study Design and Sample
Data for this cross-sectional study were collected between September 2016 and July 2017 in two cities in the South Limburg region of the Netherlands: Maastricht and Heerlen. The Maastricht University Medical Center (MUMC+) medical ethics committee reviewed the study protocol and concluded that formal ethical approval was not required (METC 16-4-109). All participants received written information and provided signed informed consent. Eligible participants (≥18 years, able to walk without walking aids) were recruited via social media, posters, flyers, advertisements in local and regional newspapers, and personalized mailing, which resulted in a total of 758 included participants. The study materials were handed out to the participants in their community centers, and after completion of the measurements, the materials were picked up by the researcher at the participants’ home.
Accelerometry and GPS Measurements of PA Behavior and Location
To measure context-specific PA, both PA and location data were collected. The participants were instructed to wear an Actigraph GT3X+ activity monitor (Actigraph, Pensacola, FL, USA) and a Qstarz BT-Q1000XT GPS-logger (Qstarz International Company, Taipei, Taiwan) for 7 consecutive days (Kerr et al., 2011). The devices were worn on an elastic belt on the right hip. In the daytime, the devices were only removed during activities involving water, for example, bathing and swimming. Participants were asked to remove the belt and charge the GPS-logger overnight, using the supplied charger.
Questionnaires
During the week of the device-based measurements, participants completed a questionnaire asking about sociodemographic characteristics, health-related quality of life (HRQoL), and the perceived neighborhood walkability.
Sociodemographic Characteristics
Participants reported their gender (0 = male; 1 = female), age, educational level (recoded into 0 = lower educated; 1 = higher educated, for higher professional education or higher), work status (recoded into 0 = not employed; 1 = employed), height, weight, home address and, if applicable, working address. Body mass index (BMI) was calculated using self-reported height and weight. The dichotomous variable for educational level was used in the subgroup analyses.
HRQoL
The validated EuroQol-5 Dimension (EQ-5D) questionnaire was used to assess the HRQoL in five domains (mobility, daily activities, self-care, pain/complaints, and mood) and at three levels (no problems, some problems, and severe problems; The Euroqol Group, 1990). For all five domains, a dichotomous variable was created for experiencing no problems (0) or experiencing any/severe problems (1). A problem score was defined as either experiencing no problems in any of the domains (0) or experiencing any/severe problems in one or more domains (1). The dichotomous variable “experiencing health-related problems” was used in the subgroup analyses.
Perceived Neighborhood Walkability
The perceived neighborhood walkability was assessed using the abbreviated version of the Neighborhood Environment Walkability Scale (NEWS-A), which is a validated measure for neighborhood walkability (Adams et al., 2009; Cerin et al., 2009). The following subscales were included in the questionnaire: access to facilities, aesthetics, infrastructure and safety for walking, traffic hazards, crime, lack of parking spaces, hilliness, and physical barriers. All NEWS-A items were scored on a 4-point scale, and if necessary, items were recoded to create scales in which higher scores reflected a more activity-friendly neighborhood environment. Scores ranged from 1 (nonwalkable neighborhood environment) to 4 (very walkable neighborhood environment).
Data Processing
Actigraph raw vertical axis data (30 Hz) were downloaded into Actilife version 6.11.7 (Actigraph) and transformed into activity counts for 10-s epochs. Qtravel software version 1.52.000 (Qstarz International Company) was used to set the GPS-logger to record data at a 10-s epoch and to download the data afterwards. GPS and accelerometer data were merged using the Personal Activity and Location Measurement System (PALMS), which is a validated tool to combine these types of data (Carlson et al., 2015). In PALMS, vertical axis cut points were used to identify SB (0–99 counts per minute [cpm]), light PA (LPA; 100–1,951 cpm), and moderate-to-vigorous PA (MVPA; >1,951 cpm) (Freedson et al., 1998). A valid measurement day consisted of at least 8 hr of combined GPS and accelerometer wear time, and a valid week consisted of at least 5 valid days, which could include weekends (Wolff-Hughes et al., 2016).
Home and work addresses were geocoded using ArcMap version 10.6.1 (Environmental Systems Research Institute, Redlands, CA, USA). Street network buffers of 1.0 km around home and work addresses were created for each participant (Frank et al., 2005). These buffers defined the personal home and work neighborhoods. Individual-level street network buffers and the merged PA and location data were combined in a PostgreSQL databases (PostgreSQL Global Development Group, Berkeley, CA, USA) to analyze when and for how long participants engaged in SB, LPA, and MVPA in the prespecified home and work buffers, and to calculate outcome measures of context-specific PA levels.
Statistical Analyses
All statistical analyses were conducted using SPSS version 23.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to describe sample characteristics, mean values, and standard deviations of sociodemographic characteristics, HRQoL, perceived neighborhood walkability, PA levels, and SB. Independent sample t-tests were used to assess if context-specific PA levels differed between subgroups.
Associations between personal characteristics, perceived neighborhood walkability, and PA outcomes were assessed using multivariate linear regression analyses. To assess the main effects of environmental characteristics on PA, we used a hierarchal regression method with two blocks. The first block contained sociodemographic characteristics, and the second block contained the subscales of the NEWS-A. The backward deletion method was used for each block to exclude the least significant variables until all remaining variables were statistically significant (p < .05). The final model, containing both blocks, is presented in the “Results” section.
Interactions between the time exposed to the home neighborhood environment and perceived neighborhood walkability were calculated and added to the model, to test a possible moderation of the amount of exposure on the associations between the perceived neighborhood walkability and neighborhood-based MVPA. Stratified analyses were performed in case of significant interactions (p < .10; Stone-Romero & Liakhovitski, 2002). Finally, interactions between the perceived neighborhood walkability and individual characteristics (i.e., educational level and health status) were added to the model, to explore possible interactions between the perceived neighborhood walkability and individual factors. In case of significant interactions (p < .10), additional sensitivity analyses were conducted with stratification by educational level and health status.
Results
Participant Characteristics
Of the 758 participants who were included in this study, 37 (5%) did not provide valid questionnaire data. Another 212 (28%) participants failed to provide at least 5 valid days of PA and location data, leaving 509 participants in the final sample. Table 1 presents the participant characteristics, HRQoL, and the perceived neighborhood walkability of the total sample and the subgroups based on educational level and health-related problems. Of the total sample, about half was male, and half of the sample had a higher level of education. About 46% of the participants was not employed, which included unemployed and retired persons and individuals declared unfit to work. The mean BMI was 25.1 kg/m2. The sociodemographic characteristics, HRQoL, and the perceived neighborhood walkability are presented in Table 1 both for the whole sample and for the subgroups.
Sociodemographic Characteristics, Health-Related Quality of Life, and NEWS-A Scores of the Total Study Sample and Subgroups.
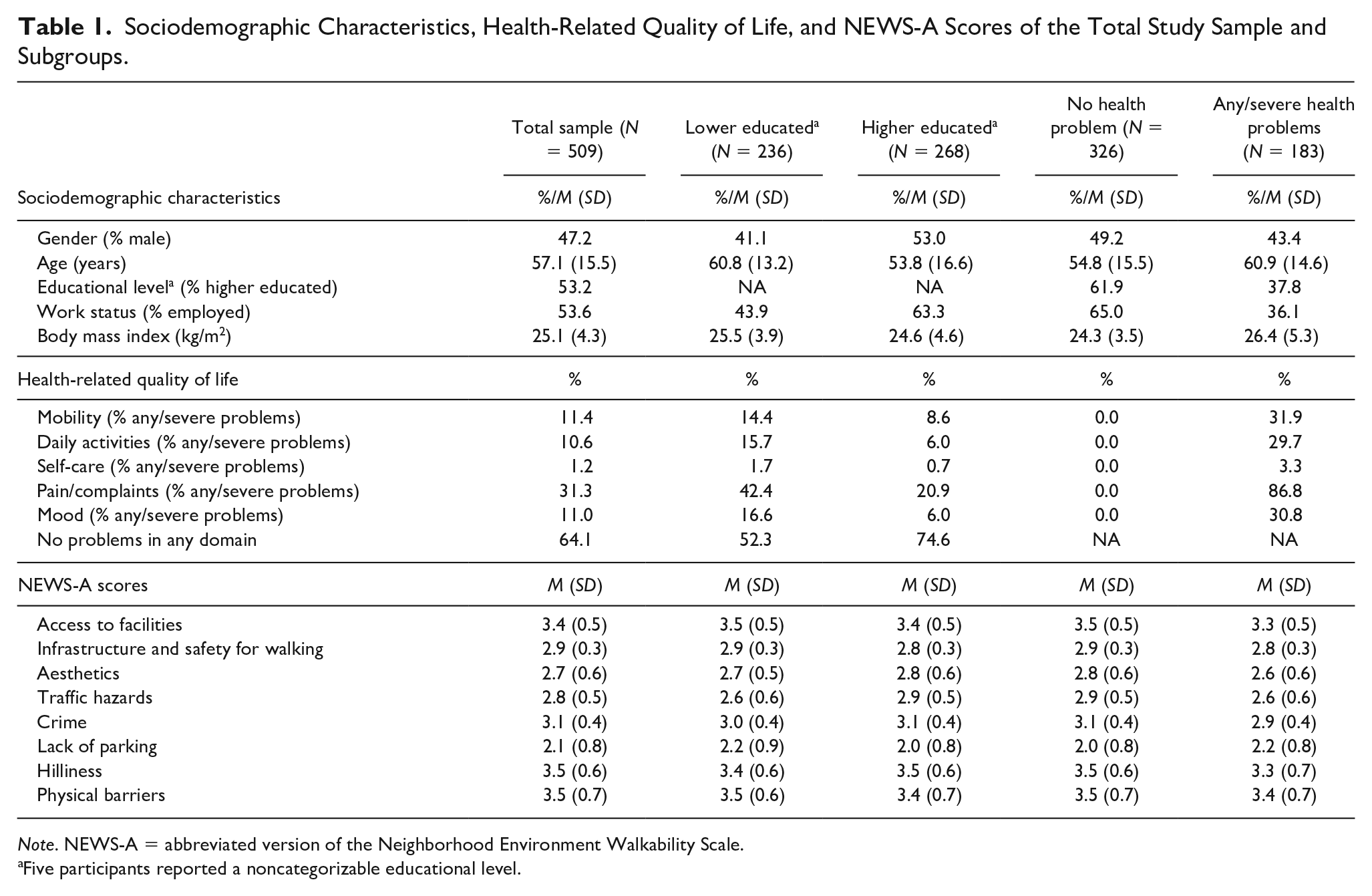
Note. NEWS-A = abbreviated version of the Neighborhood Environment Walkability Scale.
Five participants reported a noncategorizable educational level.
Of the total sample, hardly any of the participants experienced problems regarding self-care. About 10% to 11% experienced problems regarding mobility, daily activities and/or mood, while almost a third of the study sample experienced pain/complaints. Overall, about 63% of the participants did not experience any problems in any domain. The lowest score for neighborhood walkability (NEWS-A) was found for the subscale lack of parking spaces (M = 2.1, SD = 0.8). The subscales hilliness and physical barriers had the highest mean score (M = 3.5, SD = 0.6; M = 3.5, SD = 0.7, respectively).
Overall and Context-Specific PA Levels
Table 2 shows the overall and context-specific PA levels of the total sample as well as of subgroups within the sample. The average wear time of the total sample was 14.2 hr per day, of which 64.2% was spent in SB, 31.4% in LPA, and 4.2% in MVPA. More than half of the total wearing time was spent at home or in the home neighborhood. When present at home or in the home neighborhood, most of the time was spent in SB.
Total and Context-Specific Physical Activity Levels for the Total Sample and Subgroups Based on Educational Level and Health-Related Problems.

Note. SB = sedentary behavior; LPA = light physical activity; MVPA = moderate-to-vigorous physical activity.
Five participants excluded based on noncategorizable educational level.
PA levels based on educational level
The average wear time per day did not differ between lower educated and higher educated individuals, but lower educated individuals spent significantly more time at home and in their home neighborhood. Overall, higher educated adults spent significantly more time in SB compared with lower educated individuals, while lower educated individuals spent relatively more time in LPA. Sensitivity analyses showed that the differences in total SB and LPA were due to differences in PA levels at work and the work neighborhood (supplementary Table S1). Whenever they were present in the home neighborhood, the relative time spent in SB, LPA, and MVPA was similar for lower educated and higher educated adults.
PA levels based on health-related problems
The average wear time was similar for individuals with and without health problems. Overall, the two groups spent the same relative amount of time in SB and LPA, but individuals without health-related problems spent significantly more time in total MVPA. Individuals with health-related problems spent a greater share of the total time at their home and in their home neighborhood compared with individuals without health-related problems. The relative amount of time spent in SB, LPA, and MVPA whenever present in the home neighborhood did not differ between the two groups. Because MVPA levels at work and in the work neighborhood did not explain the differences in total MVPA levels between individuals with and without health-related problems (supplemental Table S1), we focused our subsequent analyses on the associations between the perceived neighborhood walkability and neighborhood-based MVPA.
Associations Between Perceived Neighborhood Walkability and Neighborhood-Based PA
In the total sample, being younger was associated with more MVPA in the home neighborhood (Table 3). When controlling for age, a better perceived access to facilities and an increased perception of a lack of parking spaces were associated with more MVPA. A significant interaction was found for time of exposure to the home neighborhood and perceived neighborhood walkability (Aesthetics × Exposure; t = 1.972, β = .085, p = .049). We stratified for the median amount of exposure to the home neighborhood (median = 505 min/day). For individuals spending more time in the home neighborhood, there was a negative association between age, gender (men), BMI, and educational level with more neighborhood-based MVPA. For individuals spending less time in their home neighborhood, only age was associated with neighborhood-based MVPA. The lack of parking spaces was associated with more MVPA, but only for individuals who spent less time in their neighborhood. Access to facilities was positively associated with more MVPA, but only for individuals spending more time in their home neighborhood. The explained variance of the final model was 5.3% higher for individuals spending more time in their home neighborhood, compared with individuals spending less time in their home neighborhood.
Associations Between Personal and Environmental Characteristics, and MVPA in the Home Neighborhood, for Individuals Spending More or Less Time in Their Home Environment.
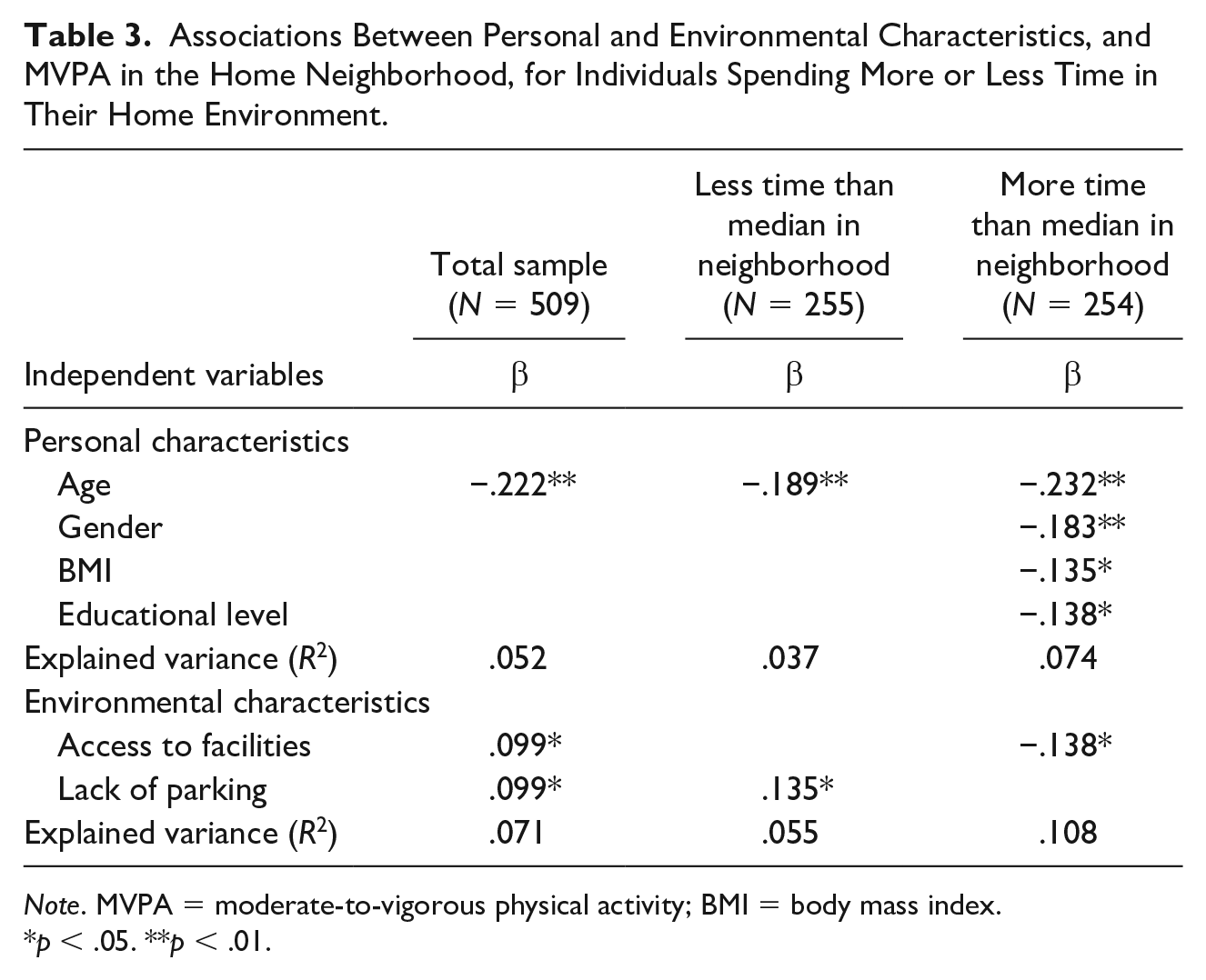
Note. MVPA = moderate-to-vigorous physical activity; BMI = body mass index.
p < .05. **p < .01.
Interactions between perceived neighborhood walkability, health status, and educational level were tested for individuals spending more and less time in their home neighborhood. Significant interactions were found for these personal characteristics, but only in individuals spending more time in their home neighborhood (Health status × Access to facilities, t = −1.731, β = −.110, p = .085; Educational level × Aesthetics, t = 2.458, β = .148, p = .015). Stratified analyses were performed to explore these interactions further (Table 4). For individuals spending less time than median in their home neighborhood, none of the environmental characteristics was associated with neighborhood-based MVPA. For the lower educated individuals who spent little time in their home neighborhood, no significant associations were found at all. The explained variance of the final models ranged between 0% and 7.3%.
Associations Between Personal and Environmental Characteristics and Neighborhood-Based MVPA, Stratified for Educational Level and Time Spent in Neighborhood.
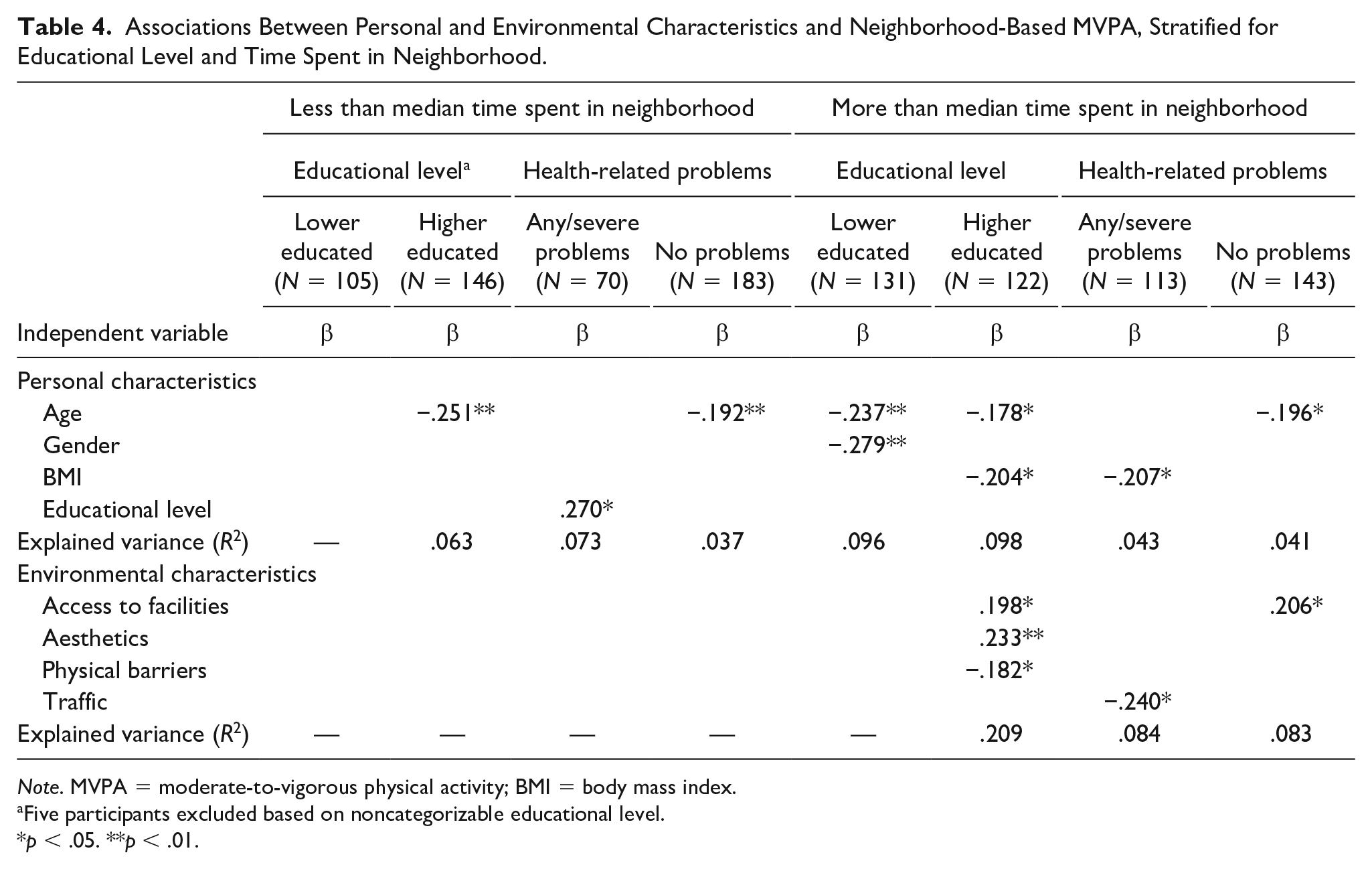
Note. MVPA = moderate-to-vigorous physical activity; BMI = body mass index.
Five participants excluded based on noncategorizable educational level.
p < .05. **p < .01.
For individuals spending more time than median in their home neighborhood, differences were found in the final models for lower educated and higher educated individuals and for individuals with and without health problems. None of the environmental characteristics were associated with neighborhood-based MVPA in lower educated individuals. For higher educated individuals, access to facilities, and aesthetics were positively associated with MVPA. Fewer physical barriers were associated with less MVPA. Neighborhood-based MVPA levels were negatively associated with less traffic for individuals spending more time in their neighborhood and experiencing any/severe health-related problems. For individuals without health-related problems, a higher score on aesthetics was associated with more neighborhood-based MVPA. The explained variance of the models for individuals spending more time in their home neighborhood ranged between 8.3% and 20.9%.
Discussion
The aims of this study were to explore context-specific PA behavior in more and less advantaged individuals in society, to assess the associations between the perceived neighborhood walkability and neighborhood-based PA, and to determine the effect of the time spent in the home neighborhood and individual characteristics on this association.
We observed differences in the total amount of PA per day and context-specific behaviors between subgroups based on educational level and health status. Regarding the total PA per day, lower educated individuals spent less time in SB and more time in LPA. Subanalyses showed that this was mainly explained by the differences in PA and SB levels at work and in the work neighborhood. These differences between higher educated “white-collar” employees, with highly sedentary jobs, and lower educated “blue-collar” employees were also found in other European studies (Buck et al., 2019; Lakerveld et al., 2017; Van Dyck et al., 2010). We also found lower levels of total MVPA in people experiencing any/severe health-related problems compared with people without health-related problems, which is also in correspondence with the existing literature about the relationship between HRQoL and PA (Bize et al., 2007). Also, individuals with a lower educational level and/or experiencing health-related problems spent significantly more time in their home neighborhood, which creates an opportunity to increase PA levels by improving the PA friendliness of the home neighborhood.
Associations between the perceived neighborhood walkability and neighborhood-based MVPA differed for subgroups. The identified associations between the accessibility of facilities, lack of parking spaces, and neighborhood-based MVPA in the overall sample supported the results of previous studies (Humpel et al., 2002). However, the presence of PA-facilitating characteristics was only associated with MVPA for higher educated individuals, or individuals without health-related problems. On the contrary, the absence of PA-hindering factors, such as the lack of parking spaces, was only associated with more MVPA for the less advantaged. Both findings are in line with a previous study (Stappers, Van Kann, De Vries, & Kremers, 2018). In light of the hierarchy of walking needs, it might be that for the less advantaged subgroups the lower order needs, that is, feasibility, accessibility and safety, have not been fulfilled, while for the more advantaged subgroups these needs were fulfilled and the higher order needs, that is, comfort and pleasurability, became more important (Alfonzo, 2005).
Besides socioeconomic factors, the amount of time that was spent in the home neighborhood also affects the relationship between the environment and PA. Notably, we identified no associations between the perceived neighborhood walkability and neighborhood-based MVPA for individuals spending relatively little time in the home neighborhood. The explained variances in these models were low (0%–7%), in line with findings by De Bourdeaudhuij and colleagues (2003). For individuals spending relatively more time in the home neighborhood, the explained variance of the final model increased up to 20.9%. This implies that the perceptions of the physical environment have more effect on PA levels for individuals spending more time in their home neighborhood, which are often the more disadvantaged people in society.
We identified some unexpected negative associations. In contrast to, for example, Foraster et al. (2016) and Jongeneel-Grimen et al. (2013), less perceived traffic was associated with less MVPA in our current study. This might be due to the fact that people who are more physically active in their neighborhood are more aware of the traffic. Similarly, fewer perceived physical barriers were associated with less MVPA. This could be due to the increased directness of routes without physical barriers such as highways and rivers, leading to shorter trips. However, longitudinal data are necessary to explore these unexpected associations further.
To our knowledge, this is the first study that takes into account the actual time spent in the home neighborhood when assessing the relationship between the perceived neighborhood walkability and PA. Previous experimental studies reported that people living closer to an intervention in the built environment are more affected by it compared with people living further away (Goodman et al., 2014; Heinen et al., 2017; Hirsch et al., 2017). This study adds that it is necessary to measure the actual exposure to the environment of interest because the physical environment might only affect individuals who spend more time in that specific environment.
Although several studies identified associations between the physical environment and PA, only a few identified differences between subgroups in society (Compernolle et al., 2016; Sallis et al., 2016; Sundquist et al., 2011; Van Dyck et al., 2010). This might be due to the mismatch of the level (i.e., individual or neighborhood level) or context specificity of measurements. PA behaviors are typically measured at the individual level, while objective neighborhood environment or neighborhood walkability is often measured at the neighborhood level using administrative neighborhood boundaries (Sallis et al., 2009; Sundquist et al., 2011; Van Dyck et al., 2010). Some of these studies also used neighborhood-level characteristics to stratify subgroups in their sample (Sallis et al., 2009; Van Dyck et al., 2010), while it is not known whether these characteristics are applicable for all participants of the particular neighborhood. The use of individual data on all levels, that is, PA, environmental characteristics, and sociodemographic characteristics, might be helpful in future research clarifying possible differences between subgroups in society.
The strength of this study is the objective and context-specific measurement of PA and the incorporation of the time that individuals were actually present in their home neighborhood. This study is one of the first that explored subgroups based on health status, which seems to impact the associations between the environment and PA. Furthermore, we reached a high compliance with the wear protocol, with only a few participants excluded and a mean wear time of 14.2 hr a day. One limitation of this study is its cross-sectional design. It was not possible to detect causal relationships using this research design. Another limitation is the age distribution in the study sample. As the mean age of the participants was 57.1 years, a substantial proportion of them was retired. Thus, the amount of time spent in the home neighborhood was possibly higher in the study sample compared with the total population. This implies that the generalizability of the results might be better for a slightly older population than for the general population of adults. Finally, it should be noted that our results concern associations between the perceived neighborhood walkability and PA. Research suggests a limited correlation between the perceived environment and the objectively measured environment, for example, measured by geographical information systems (Ball et al., 2008), which implies that a change in the environment might not directly evoke a change in the perceptions of the environment.
Conclusion
Individuals with a lower educational level or with health-related problems spend more of their time in their home neighborhood, which creates opportunities to increase PA levels by improving the quality of that neighborhood. For those individuals, however, facilitating features in the physical environment, for example, appealing aesthetics and access to facilities, might not have the same positive effect they would have on individuals without problems or a higher education. The results of this study suggest that the neighborhood environment might only affect individuals who spend relatively much time in their neighborhood. We recommend that researchers and city planners take into account the subgroup differences in associations between the perceived neighborhood walkability and PA when designing PA-promoting environments. From a health-equity perspective, city planners should consider whether their plans affect lower SES populations with at least as much impact as they affect higher socioeconomic groups. Our results underline the relevance of this consideration, because the variance in MVPA levels in lower educated participants could not be explained by perceived neighborhood walkability. Longitudinal experiments, controlling for exposure, are necessary to confirm the identified associations and subgroup differences.
Supplemental Material
Supplementary_material – Supplemental material for Combining Accelerometry and GPS to Assess Neighborhood-Based Physical Activity: Associations With Perceived Neighborhood Walkability
Supplemental material, Supplementary_material for Combining Accelerometry and GPS to Assess Neighborhood-Based Physical Activity: Associations With Perceived Neighborhood Walkability by N. E. H. Stappers, J. Schipperijn, S. P. J. Kremers, M. P. M. Bekker, M. W. J. Jansen, N. K. de Vries and D. H. H. Van Kann in Environment and Behavior
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by The Netherlands Organisation for Health Research and Development (ZonMw) (Project 531001316).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.