
Abstract
This article explores women’s temporal experiences of using Assisted Reproductive Technology. The demand for such treatment has increased since the first in vitro fertilisation birth. Assisted Reproductive Technology involves invasive procedures in women’s bodies, uncertain outcomes and temporal challenges. A sample of 11 professional women was drawn from a larger sample recruited for interviews from online infertility forums. Analysis was carried out using a biographical life course approach to draw out the temporal elements of experiences. Four themes were identified: biographical timing and temporalities of fertility treatment; biographical timing and a/synchronicity with friends; temporalities of everyday life when using Assisted Reproductive Technology; and ‘public issue’ or ‘private trouble’ in relation to silences around Assisted Reproductive Technology. Undergoing Assisted Reproductive Technology treatment sets these women apart from friends who conceive without treatment, and they faced challenges for the rhythms of everyday life during this period. Using Assisted Reproductive Technology highlighted public taboos about women’s bodies. Thus for many, this critical phase had to be kept secret. Understanding women’s temporal experiences of using Assisted Reproductive Technology and the challenges involved are important for developing context sensitive theories and concepts that can contribute to deeper insight into the intersecting temporalities of reproductive processes in general and using Assisted Reproductive Technology in particular.
Introduction
The overarching context for our article is women’s temporal experiences of fertility treatment using Assisted Reproductive Technology (ART) when becoming pregnant is not straightforward and does not occur at the planned time. Specifically, we focus on intersections of different levels of perceived temporalities, that is, the subjective dimension of experiencing time (Adam, 1995), involved in fertility treatment within the female life course. The opportunity to bear children is usually limited to the period from the onset of puberty to menopause. Although unexplained infertility for women may occur at any age, difficulties getting pregnant increase with age. The average age of birth of first child has increased in the Western world, especially among women with higher education; in the United Kingdom it was 30.7 in 2020 (ONS, 2021). Under these circumstances, together with increasing demand for childbearing among single women and those in same-sex relationships, the demand for ART has increased significantly since the first successful in vitro fertilisation (IVF) birth in the United Kingdom in 1978.
While the planning of childbearing in the life course can be difficult for a number of reasons, and any pregnancy may be stressful, using ART involves an additional set of challenges. These include demanding and invasive procedures, and the uncertainty of a hoped-for, but ambiguous phase of transition to pregnancy (Franklin, 2022; Gentile, 2013). This may exacerbate a sense of temporal insecurity, especially for women employed in professional or other competitive work environments that typically involve professional careers with promotion opportunities (Nilsen, 2012). 1 During what may be their most fertile period, there is thus a ‘temporal squeeze’ 2 in the life course that challenges the timing and ordering of biographical events. Having children is usually considered a happy experience. It does, however, disrupt women’s trajectories in various areas of life, not only in employment. Pregnancies where ART is not involved follow a trajectory that starts with conception and may bring periods of feeling unwell or complications that could have disruptive effects, and may not result in a live birth. For those using ART, the disruption starts before pregnancy and will thus have a longer trajectory. There is an added dimension of uncertainty during this pre-conception period related to the low success rate of ART (in terms of it resulting in a pregnancy or a live birth) and, in the United Kingdom, limitations in the number of funded treatment cycles provided by the National Health Service (NHS; Human Fertility and Embryo Authority; HFEA, 2021). The time experience during this pre-conception phase has been suggested to include the present moment, waiting, hope and possibly, death of hope (Cipolletta and Faccio, 2013).
Based on a sample of 11 interviews from a study of professional women’s experiences with ART, this article investigates how notions of intersecting temporalities can be of use in researching these experiences from both long-term and short-term angles. We make an implicit comparison with trajectories of non-ART conception and pregnancy to highlight the exceptional circumstances surrounding interviewees’ experiences. As ART involves many phases and turns, we introduce the concept ‘intermittent presents’ inspired by Mead’s (2002 [1932]) notions of time, as an overarching temporal concept to explore this phase. More particularly, we make a distinction between biographical timing, relational temporalities and rhythms of everyday life in order to examine the various aspects of women’s experiences of using ART. We also examine how the public silences surrounding fertility challenges and ART affect the interviewees’ situation during this vulnerable period in their lives. On this topic, we draw on Mills’ (1980 [1959]) concepts of ‘public issues’ and ‘private troubles’.
Below we discuss the context and previous literature on this topic before outlining in more detail our temporal conceptual framework.
Context: ART use and impact
The use of ART is increasing in the Western world and the most common procedure is IVF. In the United Kingdom, where the research reported in this article took place, figures from the HFEA (2021) show that in 1991 there were 6700 IVF cycles recorded at fertility clinics, increasing to 69,000 in 2019. The average age of women undergoing IVF increased in this period to 35.7 years in 2019, which is notably older than the average age (30.7 years) of birth of first child (HFEA, 2021). The proportion of all IVF cycles involving women aged 40 and over has increased from 10% in 1991 to 21% in 2019. However, older women also have the lowest live birth rates: in 2019, live birth rates for women aged over 42 were only 5% when having IVF using their own eggs (HFEA, 2021), thus reinforcing temporal pressures. Not all women are eligible for NHS-funded ART. 3 Women who do not qualify or who wish to have additional cycles, may have private treatment, but this is financially prohibitive and costs frequently escalate.
Reasons for seeking ART treatment are diverse and include fertility challenges due to health concerns, age, lifestyle factors, lack of partner, and so on (van den Akker et al., 2017). The difficulties and challenges that lead women to make use of ART, as well as the treatment itself, may be disruptive factors in the life course. Studies show that, for example, combining employment with ART is challenging for the employment situation; daily management of work is difficult and disruption to work may damage career trajectories (Payne et al., 2019). However, employment is needed to fund ART, especially where women are denied NHS-funded treatment. Thus, finances are a significant worry and financial security may be impaired (Lundborg et al., 2017). However, as Hall (2023) observed, financial worries may also be associated with an overall situation of austerity in society that impacts on families’ everyday lives and may lead to the postponement of planned pregnancies.
Fertility challenges may also create strain in relationships with a partner and with family and friends, thus potentially causing damage to social networks and support structures (Wagner et al., 2015). In particular, social stigma may be an issue, especially in cultures where being childless is a source of shame (Daibes et al., 2018; Ergin et al., 2018). This is problematic because social support is associated with better mental health in people with fertility challenges (Mahajan et al., 2009) and fertility challenges have significant mental health impacts, including suicidal feelings (Kjaer et al., 2011; Payne et al., 2021). Such impacts are particularly associated with a lengthy fertility journey, which may include many unsuccessful cycles of treatment, miscarriage and stillbirth (Verhaak et al., 2005).
Although ART is not exclusively a female issue (Halcomb, 2018), research shows that women have higher levels of distress in relation to such treatment (Greil et al., 2010) and ART impacts on women’s bodies. Each IVF cycle involves the daily administration of intravenous hormones, frequent clinic visits for scans and blood tests, and unpleasant, invasive egg collection and embryo transfer procedures. This makes both the physical and temporal experiences more disruptive than non-ART conception and transition to pregnancy. Moreover, as only a small percentage of treatment cycles are successful in producing a pregnancy and a live birth (HFEA, 2021), the disruption to the life course is often protracted. Taken together, these factors underpin the importance of exploring the temporalities involved in the lives of women using ART.
Conceptual framework: intersecting temporalities in the life course of women
There is a wide literature on different aspects of pregnancy and motherhood. In recent years, surrogacy has become a topic of interest in this literature (Culley and Hudson, 2009; Jacobson, 2021). Others have focussed on how motherhood through surrogacy and ART may or may not have emancipating potentials from a feminist point of view (Corradi, 2021). While these are important and interesting approaches to reproduction and motherhood, our focus is more specific. Our primary interest is on the temporalities involved when women make use of ART to conceive and become pregnant, since this important aspect has received less attention in research.
Time as a concept refers to observable measurements of chronological time while temporality involves a subjective dimension of experiencing time (Adam, 1995). Among the earliest theories in sociology of relevance is Mead’s (2002 [1932]) ideas of the present: ‘Past, present and future belong to a passage which attains temporal structure through the event’ (p. 53). The past is always seen through the lens of the present as is the future. Experiencing actual events constitutes the temporal dimension, the passing of time is in lived reality, in the present. Time is processual but: ‘For us to be able to conceive of events, change, continued existence, the present or even time, there has to be becoming and disappearing’ (Adam, 1995: 79). In relation to experiences with ART, the hoped-for transition to pregnancy can be analysed as a stage involving many decisive events. Rather than considering this phase a case of a ‘protracted present’, it can be viewed as a series of ‘intermittent presents’, which creates a particular type of temporal framework that can be investigated. While both ART and non-ART pregnancies may involve disruptions, complications and may not result in a live birth, non-ART pregnancies are contrasted with ART pregnancies due to the ‘intermittent presents’ during the protracted pre-conceiving phase.
A contextualist life course approach involves interpreting biographical events in light of the historical context in which they occur (Elder et al., 2003). The biographical timing of life course events follows standards of ‘timeliness’ that are considered normative in specific societies (Hareven, 2000). Pregnancy can only happen during a limited phase in women’s lives, which coincides with many life course events and transitions (Nilsen, 2012). The timing of pregnancy and childbirth for women, especially those with higher education who have professional careers in competitive work environments (Nilsen et al., 2012), creates a ‘temporal squeeze’ in the life course. Several levels of temporalities intersect in challenging ways when many transitions happen simultaneously, for example, the transition from education to work and the start of a career coinciding with entering a couple relationship and planning children.
In addition to the individual biographical level, there are also relational temporalities involving being in sync with peers. Being in or out of sync with friends with regards to important life course events and phases such as pregnancy is important for relationships (Hareven, 2000; Nilsen et al., 2012). 4
For women of reproductive age menstruation is a significant temporal element in the monthly rhythm it creates. In a non-ART conception of a planned pregnancy, the absence of the menstrual period marks the start of a different temporality; pregnancy. For women using ART, this temporal element is replaced by a phase of ‘intermittent presents’ of possible conception making the process potentially more disruptive for both biographical and relational temporal structures.
At the level of everyday, life habits and routines are established that organise the days and weeks into temporal patterns (Adam, 1990; Zerubavel, 1985). For women using ART, the phase of trying to conceive with its ‘intermittent presents’, may be expected to be disruptive for the everyday rhythm of life. The treatment goes through phases involving challenges of different types. In one phase, women have to administer injections; in another phase, frequent visits to a clinic also break up the habitual everyday pattern. The medical procedures and hormones are invasive and may add feelings of unwellness that make it hard to keep the pace of daily activities, thus affecting everyday temporal rhythms.
Thus a conceptual framework of intersecting temporalities can uncover the many challenges women using ART face and how these differ from those of non-ART conception and transition to pregnancy. Using ART protracts the pre-pregnancy phase, if pregnancy happens at all, and breaks this phase up into ‘intermittent presents’ that become disruptive on many levels – and an ambiguous dimension of biographical uncertainty is exacerbated. Using this framework, we aim to obtain a more nuanced understanding of women’s experiences during this phase. There is widespread public silence surrounding reproductive issues such as miscarriage, stillbirth and fertility challenges (Bellhouse et al., 2018), which affect women in society. The interviewees in this study, however, are in or have previously experienced a particular vulnerable period in their lives while using ART, and through a focus on them we also aim to contribute to a raised awareness of such issues in the public domain.
Method
The sample analysed for this article is purposive (Silverman, 2020), drawn from a larger sample of 37 interviewees, comprising mostly cohabiting or married women but also 5 single women and 6 men, interviewed primarily to explore experiences of combining work and fertility treatment (Payne et al., 2018; van den Akker et al., 2017). The overarching research questions for the original study were about experiences of ART among professional women. The best way of sampling for that was found to be getting in contact with volunteers who were mainly recruited from online infertility forums. Those who volunteered were heterosexual, white and in professional or other white-collar occupations and their mean age was 36. Half the sample were in treatment during the interviews, while the other half had gone through treatment with a successful outcome and reflected on this retrospectively. This way of recruiting produced a bias towards white, highly educated professional women, which is the case for much research in this area that relies on participants to volunteer (Earle and Letherby, 2007). Despite this limitation, the embodied processes will be similar for all women who use ART. Furthermore, the focus on professional women was an aspect of the ‘temporal squeeze’ common to all participants. The purposive sampling for this article followed a sociological logic (Silverman, 2020), thus generalisability of cases is to theoretical propositions rather than to populations. Moreover, generalisability also involves characteristics of cases being transferable to those of similar properties beyond a particular context (Gobo, 2008).
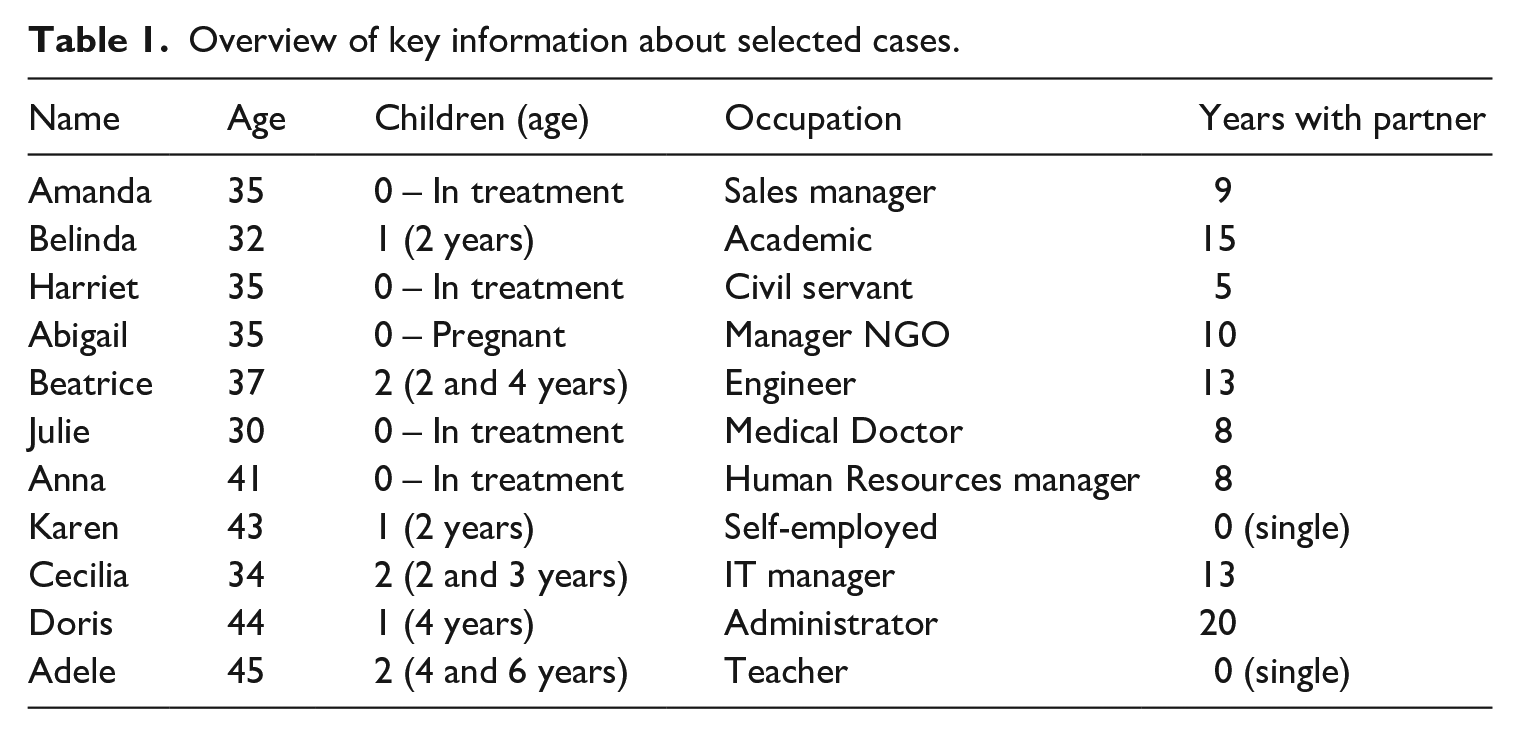
The subsample selected for this article included nine married or cohabiting women and two single women (see Table 1). Those who had completed treatment were primarily selected for analysis in order to capture a longer temporal horizon in their retrospective reflections about the phase of using ART. However, four who were still in treatment and had been for a longer period of time were also included because they experienced a longer phase of hoped-for conceiving but also shared the experiences of the pre-conception trajectory that was common for them all regardless of length of treatment. We thus selected the subsample for an in depth temporal understanding of the processes involved.
Overview of key information about selected cases.
Although the original interview primarily focused on combining work and fertility treatment, it covered when participants started thinking about becoming a parent, when this became more important to them, the decision to use ART and experiences and outcomes of using ART. Therefore, temporality issues were highlighted as meriting specific attention. Interviews were digitally recorded and lasted between 45 and 120 minutes. Verbatim transcriptions were used in the analysis. The study was approved by the University Ethics Committee and participants were informed and provided consent according to the committee’s guidelines.
As the aims in this article are to gain an understanding of the temporalities involved in ART, analysis was informed by a biographical life course perspective (Elder et al., 2003) in order to draw out the various temporal elements in the interviews (Adam, 1995; Nilsen, 2023). In addition a case study approach (Gomm et al., 2000) in the analysis is a method that is helpful in framing the ART experience within a longer biographical time frame. Analysis of cases also allows themes to emerge from the data. We identified four themes related to our overarching research question: biographical timing and temporalities of fertility treatment; biographical timing and a/synchronicity with friends; temporalities of everyday life when using ART; and ‘public issue’ or ‘private trouble’ in relation to silences around ART.
Some cases are foregrounded and citations from others are included to underpin points made by these cases. They have been given pseudonyms to protect their anonymity.
Biographical timing and temporalities of fertility treatment
The interviewees were asked about their thoughts about motherhood, when it had become important in their lives, and when it had become clear that they would need assistance. All thought that children would ‘happen’ ‘automatically’. As one interviewee said, ‘You just automatically assume it is something that is going to happen’ (Anna). For most, such events are pushed into the future.
Abigail and her husband had tried for some time to get pregnant before they realised that there were difficulties.
It was always in the plans. My husband and I had talked about starting to try for a family at 30. But we waited. To just kind of sort out money and some other stuff. (. . .) And so once we’d made the decision then it became the most important thing we were doing. Or trying to do.
Initially when nothing happened, they were relaxed about it, but that changed when Abigail found out that there was something wrong with her fallopian tubes so IVF was the only option. It took some time to get into treatment, and as they had left it late she said, ‘having a family it’s kind of the next few years or never’. Other interviewees echoed these sentiments of urgency, and that (biological) time was running out to conceive: ‘I’m not getting younger, I have five, six, seven years may be left to, to try this (. . .) the right time now’ (Amanda) and ‘Age comes into it because I guess more and more my time is running out so it is becoming more and more of a priority and more and more highlighted that it’s what I want’ (Anna). When the expected outcome in the biographical timing of pregnancy within the boundaries of their perceived timeliness, failed, ART became the first of several options they tried.
The life course approach to these questions highlights the urgency that many women feel when coming to the end of their reproductive phase and they have not succeeded in conceiving. After a period of youth, a more reflective phase follows, especially when events do not happen according to the timeliness of expected standard biographical events. Cecilia’s interview illustrates this point: I think when you are young, like in your early 20s (. . .) Yes, I’m not so sure actually because I’m too busy having fun and going on holiday and working and being able to go out in the evening to nice bars and restaurants and stuff. But I think deep down I always thought I’d have children one day.
Doris and her husband tried to get pregnant from when they were in their 20s. It did not happen but they were not aware of any fertility issues until later. Motherhood was very important in Doris’ life.
It’s what I was born to do. It’s such a cliché but it’s just made me a whole person. (. . .) Going through IVF and fertility it’s not something that you forget. You always appreciate what you’ve got because you’ve had such a journey to achieve that.
Having tried for a baby for so long and experiencing a miscarriage, finally having a child when they felt they were nearly out of biological time due to age, was a joy in Doris and her husband’s life. Her reflections on the process she has been through and what infertility means in people’s lives, resemble many of the other interviews.
Well, it’s very difficult when you are facing infertility. There’s always hope, and I think that’s what keeps you going at the end of the day.
The matter of age and timing in the life course came up again and again in the interviews. For some it had been pointed out that it was not only your chronological age that mattered, ‘I didn’t have much time and I was old, and they all tell you that you’ve got old eggs’ (Karen).
Temporal aspects of when to have children are not only a matter of biographical timing in women’s and couples’ lives. Beatrice could afford to have ART in a private clinic as both she and her husband were high earners who had made their careers first priority for some years. Becoming a mother was very important in her life and her temporal horizon related to this stretched beyond the biographical. Motherhood had made her realise the importance of family bonds with a future intergenerational temporal perspective.
(. . .) assuming that they are for the rest of my life that’s a relationship that I’ll have and develop with my kids and any grandchildren or whatever happens in the future – that’s just the centre to life for me.
These thoughts about the emotional connection to kin and family through having children were found in other interviews.
Biographical timing and a/synchronicity with friends
Being in sync with your age group when experiencing important life course events is an essential element of social life and for societal cohesion. This section focuses on relationships with friends and how these may impact on thoughts the interviewees have in relation to experiences of ART, when in synchrony with their peers, or when their timing was ‘off’ compared to their age group. The interviews suggest being in treatment set them apart from friends who went through pregnancy without treatment. Thus, the feeling of sharing the same experience at the same age, often comes after the child is born.
Beatrice illustrates the overall importance of friends: (When did becoming a parent become important?) I think that was probably when my first school friend had a child, and I guess it makes it ‘oh, that’s something that we could do now’ as opposed to ‘that’s something I’d like to do in the future’. But my partner wasn’t interested, so it had to wait.
Amanda was in treatment at the time of interview. Her reflections were thus related to the phase she was going through. For her and her husband, the support from family and friends who were in treatment, was very important.
Yeah, I mean, yeah support from some of my friends who are undergoing the same kind of treatment. (. . .) my husband’s cousin was going through exactly the same thing at exactly the same time as us. So we were just constantly talking the whole time and without each other’s support, I think it would have been much harder for us to get through it.
Sharing the experience of ART can bring friends closer. Karen, who had tried to get pregnant for a long time, said, I was going through IVF with another friend at the same time, and she and I became incredibly close as a result. So you make new friendships and you meet new people. (. . .) My parents were very supportive as were my sister and my brother. But it was mainly friends around me.
Belinda was also in a phase of the life course when her friends were having children. However, she felt her experiences from ART set her apart from them.
We had lots of friends who were getting pregnant as I was going through treatment and that was extremely difficult. We kind of withdrew socially from our circle and although we were very public about what we were going through (. . .) actually I don’t think we really spoke to them about what it entailed. (. . .) But I think it was the fact that within our circle no one had ever gone through anything like this so it was an expectation – ‘oh yeah, you just have some eggs taken and you mix it in a petri dish and everything will be fine!’
Harriet had similar experiences; feeling that ‘all’ of her friends and peers got pregnant affected her relationships: ‘it does have an impact on relationships with friends because at my age, a lot of my friends have had children or are pregnant or having babies’
Julie did her best to stay away from contexts where women were pregnant or had small children.
I’ve almost deliberately stayed at my current placement because a lot of the people there are older. And although they do tend to talk about their grandchildren I know that none of them are about to get pregnant. (. . .) I just couldn’t bear to be in the same office as somebody who was pregnant at the moment.
Being at an age and in a life course phase when the timing for getting pregnant was ‘right’ for friends was distressing for many women undergoing treatment. The uncertainty involved was emphasised because being in treatment in many contexts is, if not taboo, then at least not a common topic of conversation.
Temporalities of everyday life when using ART
Pregnancy is a challenging time for women in a number of ways. When using ART, the temporal aspects involved become more complex and many layered and the uncertainty issues are exacerbated. The analysis in this section demonstrates the many challenges for the rhythms of everyday life during this pre-conception period.
Harriet, who had been in treatment for some time at interview, made some important observations about the dissimilarities between conceiving with and without ART, and how the temporal impact of the former permeated everyday life.
If people are trying naturally, they don’t really know the details of what’s happening. They have sex and then they find out a bit later that they’re pregnant and they don’t know all the stuff that happens in the meantime. When you’re having treatment, even if you’re having the most basic kind and nothing else at all, you are being scanned every couple of days so you know everything that is going on in your body. You’re having scans, and your blood tested to track how your ovaries are responding and what your hormone profile looks like and so on (. . .) you’re constantly second guessing, what’s the result, what’s the next set of results are going to be like?
Not only is the everyday temporal rhythm affected by ART, but there are more medium term temporalities to take into consideration that set the treatment procedures apart: ‘But if you have an IVF cycle that fails you have to wait three months before you can have another treatment cycle. So, you’re constantly waiting for it which is pretty stressful in itself (. . .)’.
Harriet was young enough to have more cycles. However, the finite number of funded cycles available on the NHS and the huge expense of private clinics add to the uncertainty and stress involved and make the temporal aspect urgent for those who need ART.
Julie was younger than Harriet but she had been through a lengthy period of treatment with all the pain and uncertainty it involves.
I’ve had three full IVF cycles and a frozen embryo transfer and an operation in between times. There’s never really been a period of more than a couple of months where we’ve not been in treatment. And even when we’ve just been waiting for treatment, so I wouldn’t really say we’ve been out of treatment.
For Julie, a long phase of her life and her everyday existence had been steeped in the experiences of the different aspects of treatment. It had affected her at work and at home in family relationships.
Doris managed to conceive through treatment and has a small child. She gave a detailed account of the different phases of treatment and what they entailed in her everyday life. We include this here because of the information value it has for readers not familiar with the procedures involved and how they are experienced in women’s lives.
Obviously the treatment itself is broken down into stages. The first stage is called down regulation (. . .) that essentially stops your body producing hormones and stops your body ovulating and essentially puts you into a state of menopause because it shuts down your natural cycle. So, you don’t have periods. You have hot flushes; you have dizziness; I had panic attacks; loss of memory – there’s a whole range of symptoms that you can go through. Some people it doesn’t affect too badly.
Menopausal symptoms are hard for many women and enduring these in the process of treatment to get pregnant is disrupting for the normal rhythm of everyday life.
But the next stage of treatment is stimulation, where the ovaries are stimulated to produce more than one egg. It makes things a lot easier; but the only downside to stimulation is (. . .) your body produces more than one so you can be very bloated and constipated, you can be very moody and irrational. And obviously because of the stress you’ve (. . .) got all that pressure for it to succeed (. . .) especially if you’ve only got three NHS attempts.
During the next phase a lot more interaction with health personnel is involved, which means disruptions of everyday temporal rhythms related to both work and family life.
Obviously once you’re stimulated that’s when you get a lot more scans to check the womb lining, the thickness of that; obviously check on the number of follicles that your body is producing (. . .) And then obviously you go to egg collection. Hopefully your eggs do get fertilised. And then any embryos that are made they will pick the best quality ones and transfer them. And then obviously you have two weeks to wait until you can do a pregnancy test.
Doris gave an account of her own period of waiting during the 2 weeks before the pregnancy test, which in vivid detail tells how it affected her life at this time.
The nearer you get to your official testing date you just pace the floor; you don’t sleep; you don’t eat; you feel sick. (. . .) You just want to know what’s going on. You look for symptoms; you’re in the toilet constantly checking to see if you’re bleeding or if you’ve got any discharge. And it just plays havoc on your mind, it really does.
Being in treatment affects everyday life in numerous ways. The daily rhythms, the routines that are normally followed in a woman’s life are disrupted through the various phases of the treatment. Whereas pregnancy without ART may generally not disrupt everyday life until the pregnancy is a fact, for women who go through treatment, the phase of getting pregnant, if they get pregnant, affects every temporal and practical aspect of living. Doris’ detailed account gives insight into all the practicalities that are usually not talked much about in the public domain, and thus gives valuable insight into the ‘silent’ aspects of the procedures treatment involves.
‘Public issue’ or ‘private trouble’? Silences around ART 5
Although our main focus of analysis was on temporality issues, the theme of ART as a private or personal problem emerged strongly throughout, especially in relation to taboos about women’s bodies. This has temporal elements because during the ART phase many women feel that a huge part of life must be kept secret and silent in conversations with family, friends and colleagues who may lack understanding. If parts of life must be bracketed in social interactions the taken-for-granted temporal flow of social life is disrupted.
Beatrice talked about the experience undergoing ART as traumatic not only because of the treatment’s physical aspects but also because she and her partner could not share it with people around them. She found it difficult to get across to her family what she was going through because of general public prejudices and images of what ART entails.
I think the only thing that anybody really knew is the original IVF news about test tube babies . . . . I tried to explain it to people, but (it was difficult to know) whether they really genuinely wanted to know what we were doing or whether they were asking to be polite. (. . .)
Beatrice revealed how discussing anything associated with getting pregnant was considered gross and this spilled over to her attitudes to talking about her own experiences with ART.
I do remember earlier in life, I can’t remember who, maybe my stepdad saying oh it’s so gross when people are talking about how they’re trying; nobody wants to know about that. And I suppose I must have had that ingrained in my psyche that people don’t want to hear about that; that it’s not an acceptable topic for conversation really.
Julie echoed some of these feelings: There are a lot of people, probably the majority of people who undergo treatment, don’t disclose to anybody or only disclose to very close family that they’re going through it, or it’s too private in our society to be something that is acceptable to talk about.
Anna highlighted the feelings of failure, isolation and loneliness associated with the public silences about ART. In her experience, the treatment took over her whole life, yet there were very few she could talk to about it.
You feel a bit of a failure first of all. (. . .) you should be able to do this yourself? That was the first thing that went through my head (. . .). You feel like you can’t talk to people about it. You feel like you are on your own. As a couple you spend a lot of time talking about it so it kind of dominates your relationship. It makes you tired; it makes you sick.
Cecilia’s experiences were similar. She did, however, have to tell a wider circle of family and friends because of the expectations to take part in celebrations.
And IVF treatment was carried out over Christmas so I had to tell my close family anyway because I wasn’t drinking (. . .) so they’d wonder what I was doing and the worst thing would be someone assuming I was pregnant when actually that wasn’t the case at all.
The taboos around talking about the intimate and invasive processes of ART underpin lack of public awareness, which in turn can exacerbate stress for women and their partners during treatment. It also breaks up the temporal flow of social interaction when a huge part of life cannot be a topic of everyday conversation among family, friends and colleagues.
Concluding discussion
This article set out to explore different levels of intersecting temporalities involved in using the demanding and invasive procedure of ART within the female life course, among a sample of professional women caught in a ‘temporal squeeze’ in the life course. We also examined how public silences surrounding fertility represent challenges and how using ART affects interviewees’ situation during this vulnerable period in their lives. We made a distinction between biographical timing, relational temporalities and rhythms of everyday life in order to examine the various aspects of women’s experiences of using ART.
The participants’ accounts highlight concerns about age and biographical timing and in particular a sense of urgency as women approach the end of their reproductive phase. Earle and Letherby (2007) examined time as a tool for understanding perceptions of conception and also found that time running out was a central issue for women. The authors acknowledge that while socially constructed clock time is useful in understanding normative expectations about when in the life course pregnancy should occur, Adam’s (1992: 15) has argued, ‘we also are clocks . . . The rhythms of our body . . . need to be recognised in conjunction with our socially constructed clock time’.
Furthermore, participants’ feelings of being different or even in some cases, a failure, are exacerbated by lack of synchronicity with peers who become pregnant within the expected time range of the life course. The procedures disrupt biographical timing at all levels and the temporalities are experienced in what we have termed a series of ‘intermittent presents’. The analysis demonstrated how the treatment became the centre of life and directed the temporal rhythms of everyday life. The ‘silent’ aspects of treatment procedures also affected the everyday in numerous ways. A strong theme is that the women found it difficult to discuss their experiences with others due to public silences and taboos surrounding the process. It seems that these silences persist, for a diversity of reasons, despite the growing numbers of women involved in such procedures. The secrecy and silence surrounding fertility issues affected temporalities of social life because the taken-for-granted flow of conversations was disrupted when large parts of personal life had to be withheld as a topic.
Inspired by Mills’ (1980 [1959]) distinction between ‘private troubles’ and ‘public issues’, we argue that the ‘privatisation, that is the sense of not feeling comfortable with sharing experiences of fertility treatment, obscures its importance as part of a wider ‘public issue’ that reproduction represents in society (albeit more acknowledged in some societies than others). The public silences and lack of knowledge about the impact of ART procedures on women’s bodies and their wellbeing, and pushing the topic of fertility issues under the rug of ‘private troubles’ is neither in the interest of women nor of society at large. Reproduction is an important ‘public issue’ related to the public and political concerns in many societies about decreasing reproduction rates often framed in terms of the need for future labour and consumers.
The silences around the topic are all the more striking given the increased openness in some societies around sexuality issues. Contraception in many forms from the 1960s onwards started the increased divide between reproduction and sex (Greer, 1971). Details involved for women’s bodies relating to reproductive purposes remain shrouded in a public veil of silence in most societies. Women’s ways of NOT talking about ART in their wider social circle reflect norms about discussing women’s bodies more broadly. For example, the maternal or reproductive body, defined in terms of all aspects of women’s capacity for reproduction (Gatrell, 2013; Gatrell et al., 2017; Millward, 2006) has long been regarded as a private and even taboo topic in workplaces, often associated with stereotypes about the impact of women’s hormones on their career motivation and professionalism (Gatrell et al., 2017). Gatrell (2013) argues that topics including menstruation, menopause and pregnancy, and especially their bodily manifestation are often taboo in workplaces. In research on ART, Payne et al. (2018) highlights that ‘body time’, that is, time when the body is ready for each phase of treatment, as well as the associated bodily and hormone-related symptoms interferes with work time and being seen to remain ‘professional’. The temporal also goes beyond ‘body time’ in that keeping experiences ‘out of sight’ means time consuming practices that add to the burden of keeping up a professional façade.
There have been some shifts in public discussion of the menopause (Atkinson et al., 2021) in recent years, and scrutiny of attitudes to menstruation and menopause by feminist scholars (Johnston-Robledo and Stubbs, 2013), including considering menopause as a temporally constituted phenomenon (Jack et al., 2019). However, the pervasiveness of taboos surrounding talk of women’s bodies is well illustrated by Chrisler (2013) who considers reasons why women’s reproductive processes receive so little attention in psychology courses and public discussion generally. Chrisler argues that too many women are ashamed and embarrassed by reproductive and other aspects of their bodies and too many men and women absorb negative attitudes towards menstruation and menopause from popular culture, which in turn can affect broader attitudes. Girls may learn early that it is socially taboo to talk about menstruation (Kissling, 1996).
However, although menstruation and menopause are phases in women’s standard life course, as is non-ART pregnancy for many women, assisted reproduction arguably remains doubly stigmatised due to assumptions that conception is or should be unproblematic within a female biographical trajectory. Of course, all pregnancies have the potential to be impacted by disruptions, complications, miscarriage or stillbirth, and there is stigma around speaking about this ‘private trouble’ (Bellhouse et al., 2018). However, the overarching temporal framework in this article has highlighted the additional challenges women using ART face. The protracted conception and transition to pregnancy phase that using ART involves, if pregnancy happens at all, breaks time up into what we have named ‘intermittent presents’ and an ambiguous dimension of biographical uncertainty is exacerbated.
This article has highlighted the temporal experiences of a sample of women who volunteered to be interviewed. Future research can build on the findings by strategically targeting more diverse samples. For example, as social stigma relating to fertility challenges is especially common in cultures where being childless is a source of shame (Daibes et al., 2018; Ergin et al., 2018), a targeted ethnically diverse sample may heighten the issue of silences around the topic. A wider range of social class- and occupational backgrounds would do the same. Also, as single women and those in same-sex relationships are increasingly using ART (HFEA, 2021), future research could examine the impact of more diverse relational status on the challenges of timing and temporal issues in the life course discussed in this article.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.