
Abstract
Assisted reproductive technology (ART) is hailed as “the holy grail” for infertile patients in the mainstream narrative. The existing studies have clearly demonstrated how external social factors shape how ART is to be used, but they ignore the recipients of the technologies, and especially the experiences of women. Based on an investigation conducted in Z hospital’s reproductive center, this article regards embodiment as the methodological orientation for integrating socio-cultural context with female embodied experience in order to show their bio-social entanglement. As fieldwork evidence indicates, ART in practice is far from simple “hope technology”; instead, it throws women into a paradoxical world in which hope and anxiety coexist. Embodied experience, hope, and anxiety are transmitted through the bodies of women, which reveals the inscription of social-cultural context and technical uncertainty on the female body and, meanwhile, women actively learn strategies by which to cope with the technical uncertainty and moral pressures from local culture (including healing the body, folk religion, etc.), so as to hold onto infertility treatment with hope.
Keywords
“Hopeful” technology
October 20, 2016, was the first time that Mrs. Yun came to Z Hospital Reproductive Center after she decided to undergo what she called “test-tube baby” treatment. She appeared unfamiliar with but also excited about all the procedures. Yun was a 38-year-old housewife, her husband worked in a state-owned enterprise, and her 7-year-old son was in the first grade of elementary school. Yun only took the first step towards giving birth to a second child after her husband’s department officially issued a red-letterhead document for opening the “two-child policy” in February 2016; otherwise she would have worried about affecting her husband’s career. However, the delay in pregnancy made her start to feel that something might be wrong with her body. After several examinations and inquiries with different doctors, Yun realized that in vitro fertilization (IVF) (what she thought of as “test-tube baby” treatment) was undoubtedly the “most direct” method of assisting pregnancy at her age. She knew that with IVF technology her neighbor Xiaojing had given birth to her first daughter, who was now five years old. Xiaojing had cryo-preserved her untransplanted embryos at that time. After the two-child policy was released, she quickly transplanted the frozen embryos. As a result, she succeeded in her first attempt, and now she was seven months pregnant.
Two months later, when we saw Yun again, she had already entered the IVF treatment cycle, and her face no longer exhibited the optimism that it showed in our first meeting; instead, it was fraught with sadness. The journeys to and fro had slowly consumed her initial excitement, making it difficult for her to deal with housework and take care of her son’s studies. At the same time, Yun was also deeply trapped in the curse of success rate. “No matter whether the hospital claims that the IVF success rate is 50% or 60%, for individuals, it is actually only 0% or 100%; thus, you either succeed or fail, and there is no such a thing as an intermediate value at all”, she said. Yun added that she had been sleeping very badly recently, “often waking up in the middle of night”, and felt very stressed. She thought about having a baby all day and had nobody to tell. The only thing she could do was to withstand it all by herself. “Test-tube is really a difficult road”, she said.
According to the definitions in “Human Assisted Reproductive Technology Regulations” (2003) and “Ethical Principles of Human Assisted Reproductive Technology and Human Sperm Banks” (2003) issued by the Ministry of Health, assisted reproductive technology (ART) is a medical treatment for curing infertility. It is divided into artificial insemination (AI) and in vitro fertilization and embryo transfer (IVF-ET) technology, and its various technologies in expansion. Among them, “test-tube baby” technology is the colloquial term for IVF-ET technology and its expansions. It refers to the technology of “taking out an ovum from a female body, culturing it in a vessel, adding technically treated sperm, and continuing the culture after the egg is fertilized. When an early embryo is formed, it is then transferred to the uterus for implantation and develops into a fetus until delivery” (National Health Commission of the PRC, 2001). AI is the first stage of the ART process, the success of which determines whether to apply IVF-ET technology. In the following cases, except for one woman who was undergoing a preliminary physical examination, the rest of the women eventually turned to the IVF-ET technology for help.
With the increasing prevalence of infertility, ART has gradually become conventional medical treatment for infertility. According to estimates conducted by the World Health Organization, at least 80 million individuals experience infertility, worldwide, and at least 1 in every 10 couples experiences primary or secondary infertility. By 2002, nearly one million babies had been born through ART around the world, and the proportion in some European countries had reached about 5% (Vayena et al., 2002). According to survey data released by the China Population Association in 2012, there are more than 40 million infertility patients in China, and on average, 1 in 8 couples has reproductive disorders. Since the birth of China’s first IVF baby in the Peking University Third Hospital in 1988, China’s assisted reproductive institutions have developed rapidly. According to statistics from the official website of the National Health Commission, in 2007, 95 institutions across the country were qualified to develop ART. That number had increased to 365 at the end of 2012 and 451 at the end of 2016.
In the mainstream narrative, ART is hailed as “the holy grail” to infertile patients; it is the “hope tech” for curing infertility (Franklin, 1997: 190–197). However, Yun’s experience of “waking up in the middle of night” after entering IVF treatment, together with the other cases, even the treatment experiences of those who would eventually become pregnant, vividly demonstrate the dark side of ART: women are often in a state of extreme anxiety during the whole process of ART treatment (including before and after treatment).
This article uses an ethnographic survey to try to answer the following questions: what causes ART patients’ experiences of both hope and anxiety, and how do people handle this complex experience in the local cultural context? Existing research points out that the anxiety of those who use ART technology mainly stems from medical uncertainty (Bharadwaj, 2006; Franklin, 1997; Lai, 2017). Technology has further exacerbated the harm done to and control exercised over women (Thompson, 2002). The basic point of this article is that in such an embodied experience as undergoing treatment with ART, hope and anxiety coexist. On the one hand, the experiences of ART users are the manifestation of social and cultural situations (not limited to their uncertainty toward the technology itself) imprinted on the female body. On the other hand, while perceiving these experiences, women actively invoke existing cultural resources to deal with complex emotions so as to move forward with hope on the road of infertility treatment.
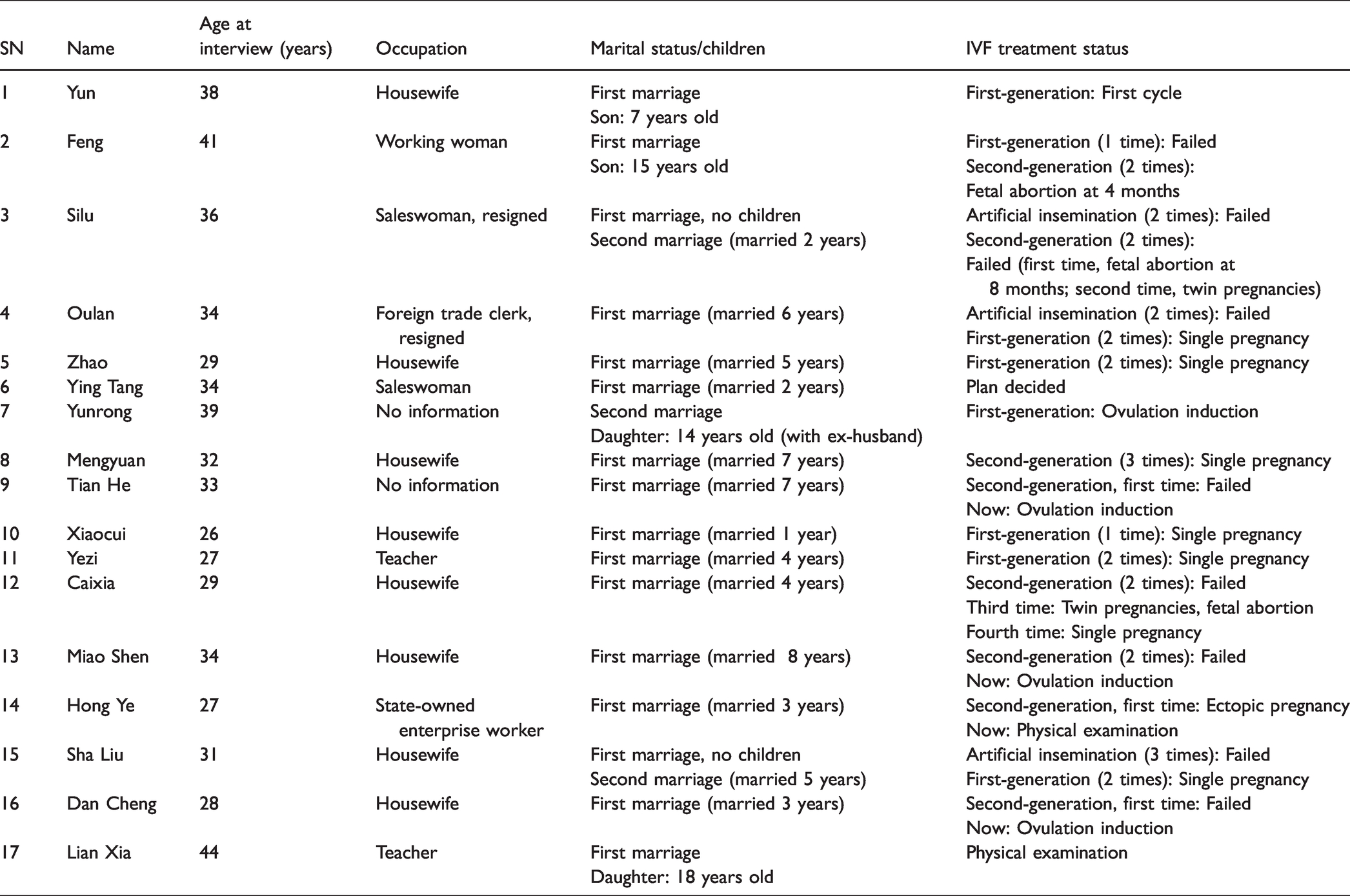
The fieldwork site for this study was the Reproductive Medicine Center of Z Hospital in South China (hereinafter referred to as the “Reproductive Center”). Since the birth of the first “test-tube baby” at the hospital, in 1990, more than 4000 cycles of IVF-ET treatment have been performed every year in the Reproductive Center. From October 2016 to March 2017, the second author of this article joined the daily work of the Reproductive Center as a volunteer, and assisted doctors and nurses with basic tasks in reception for the type B ultrasound room, billing office, file room, and other areas. During this period, a total of 60 female patients, 3 male patients, 2 relatives of patients, and 7 members of staff were interviewed. From March to June 2017, in the previous phase of the survey, the second author of this article established a good relationship with 15 female patients, maintaining long-term contact through WeChat, phone, etc., and accompanying them when they went to the Reproductive Center for treatment in order to track their diagnosis and treatment experiences at different stages. It is important to note that since this investigation was conducted in a formal and qualified reproductive center, activities such as surrogacy, egg sales, and other activities banned by the government do not appear in the information in this article. Information on the individual cases discussed in this article is shown in Table 1.
Personal information of the respondents.
Literature review: Technology, local context and embodiment
The global expansion of ART has challenged many concepts that we used to take for granted. For example, the relationship between sex and reproduction has been broken; the boundaries between nature and culture and between sacred and secular have become blurred; and issues such as whether sperm, eggs, and uteri can be used as gifts or commodities, reproductive tourism, fetal gender selection, and even homosexuality and heterosexuality have once again become widely discussed (Gammeltoft and Wahlberg, 2014; Inhorn and Birenbaum-Carmeli, 2008; Nahman, 2016). In the past 30 years, ART and its derived legal and ethical issues have aroused many scholars’ responses (Becker, 2000; Luna, 2002; Shao, 2009; Wang, 2007; Yang, 2010). Because this technology directly points to the classic fields of study in anthropology, including kinship, marriage and family, sex, bodies, etc., it is of particular interest to anthropologists. In general, anthropological (including research on technology and society, referred to as “STS”) research on ART is mainly based on the following two aspects: (1) re-examining ART in the context of local culture and thinking about the relationship between technology and society; (2) directly focusing on the objects of ART, especially women’s experiences, and reflecting on the intervention, control, and even destruction that ART produces on women’s bodies. This perspective is especially characteristic of feminist anthropologists.
Assisted reproductive technology and local social situation
ART is organized around the biological interpretation of fertility. Pregnancy is only the result of an encounter between the sperm and egg of a couple. Standardized technical operations try to separate the body from ethics and relationships (Franklin, 1997). However, existing research shows that even in European and American countries, ART practices are difficult to separate from local religious beliefs and kinship relationships. Family ideals and norms are also involved in the shaping of ART practices (Inhorn, 2002; Roberts, 2012; Simpson, 2013). As the “receiving end” of ART, the local world will restrict the use of technology based on its unique social, religious, economic, political, and other concepts, or reconfigure technology to adapt to the local social and cultural context (Inhorn, 2002, 2003).
In some countries and regions, the promotion and application of ART needs to be understood within a political and economic framework. The Israeli government strongly supports the development of ART and even includes it in the national medical insurance plan. In March 1996, Israel became the first country in the world to legalize surrogacy, and its related technologies is leading the world. The first rationale for this pronatalist policy was to ensure the strength of the country’s army to compete with those of neighboring countries; the second was to make up for the 6 million Jews who were killed in the Holocaust (Kahn, 2002). In countries that employ population control measures, such as China and India, medical institutions have positioned ART as an “effective family planning supplement”. Under the guidance of eugenics, ART has even been promoted as a medical measure for reproducing healthy offspring, especially individuals with superior intelligence and physical strength (Bharadwaj, 2000; Handwerker, 2002).
Many scholars have also noticed the emergence of political and economic inequality in the field of ART. From a global perspective, ART is not “for everyone” (Daar and Merali, 2002; Inhorn, 2003). Not only is it more difficult for developing countries to use ART, but from the perspective of class, it is also difficult for disadvantaged groups such as the poor and people of color to bear the cost of this technology. Even in the United States, only elites can enjoy ART treatments.
In other words, ART actually exhibits a kind of “stratifying reproduction” (Becker, 2000; Rapp, 2000). The urbanization and globalization of this technology have also given birth to reproductive tourism. Infertile wealthy people try to find treatment options in metropolitan medical centers, and even give birth to “their own children” through the international division of labor, such as finding egg donors and surrogate mothers (Beck and Beck, 2014; Nahman, 2016).
Obviously, more scholars are examining this technology from the perspective of kinship and related cultural constraints. ART breaks the “natural” process of gestation and challenges the kinship and birth patterns that people have long recognized (Bharadwaj, 2003; Inhorn and Birenbaum-Carmeli, 2008; Lock and Nguyen, 2010; Strathern, 1992; Zhu, 2016). The Roman Catholic Church rejects any behavior that separates human reproductive behavior from sexual behavior, refuses to use technology to interfere with “God’s will”, and opposes the implementation of ART (Luna, 2002). Islam also strictly forbids any form of third-party donation of sperm or eggs, because third-party donation will lead to “mixing of relationships”, which will cut off the blood relationship between parents and children, confuse descent and inheritance issues, and lead to possible incestuous marriages between anonymous donors’ children. In Egypt, where patriarchy prevails, people with lower education levels have deep-rooted concepts of parthenogenesis and believe that only male sperm carry genetic materials. ART recognizes the cultural script that sperm and eggs make equal contributions to fertility, and the idea that men provide “everything” for fertility is broken (Inhorn, 2003). In India, infertility treatment involving donations is believed to destroy the cultural boundaries of the family. Infertile couples are more inclined to receive donated sperm in secret to maintain a minimum level of connection with the marriage. The kinship structure will also flexibly accommodate these “invisible” violations (Bharadwaj, 2003). The structuralist master Levi-Strauss (2017) has also discussed ART. He believes that similar methods (mainly a kind of continuation) involved in this modern technology have already existed in some societies, and that the central problem is how to deal with the relationship between biological and social parents.
The interweaving of technology and society has always been a key entry point for anthropologists and STS scholars in studying ART and showing how biomedical technology is produced, accepted, modified, and even resisted throughout the world (Inhorn, 2007). The related research studies by the above-mentioned scholars provide us with the external social background of ART and show how local politics, economy, religion, family, and kinship define “natural” and “appropriate” forms of reproduction and how these social language circumstances directly affect people in choosing or rejecting this technology. However, we should note that too much emphasis on the structural factors behind the technology may blind us to the experiences of its objects, the transformation it introduces to people and their bodies, and the pain this may create, and thus may cause us to become less critical in considering ART itself and the basic care it can provide.
Female experiences with assisted reproductive technology
Apart from the macro-level social and cultural situation that ART is facing, some scholars, especially feminist scholars, focus on the experiences of women (and occasionally men) so as to challenge the ideal of ART as a “hopeful technology”. They believe that this technological “progress” has not liberated women, but actually intensified control over their bodies and reproduced the existing norms for women (Thompson, 2002). In the era of ART, the “social drama” of infertility is performed on the bodies of European and American women. Whether the husband or the wife has the infertility problem, in the end, it is the woman who bears the pain and shame of infertility, and it is also the woman who bears the main burden. Infertility treatment involves the monitoring of the body during the treatment cycle, the ups and downs of disappointment and hope, and the difficult choice between success rate and physical risk. In the process of treatment, the female body is metaphorically referred to as a “machine” that requires medical intervention, and uncontrolled bodily functions may lead to women’s self-devaluation. Even after the treatment, the concept of the body’s morbidity is engraved on the heart (Balen and Inhorn, 2002; Becker, 2000; Clarke et al., 2006; Greil, 2002; Inhorn, 2003).
For example, Franklin (1997) focused on female anxiety caused by ART in his research in the United Kingdom. ART is often described as a “simplified” and “natural” means of assisting natural reproduction technically. However, in the actual treatment process, women experience extremely complicated treatment procedures, and treatment occupies almost all of women’s lives. In addition, the fallible segments in the cycle are unpredictable and highly uncertain. There are high risks at each stage, and some failures cannot be explained. Therefore, women often describe their actual experience as “an obstacle course”. Although some women have fully understood this in advance, they are still emotionally and psychologically traumatized and may even become desperate because of the treatment. However, in the face of serious treatment failures, under pressure from all parties, they still have to show their belief in scientific progress, belief that technical treatment is a program of “having to try” and “having to choose”.
Specific to certain aspects of ART (such as pre-embryo transfer detection technology, obstetric ultrasound examination technology, etc.), the original desire to strengthen control over pregnancy and birth and create positive reproductive results may put women and their families into a world of accidents, ambivalence, and disorientation (Gammeltoft and Wahlberg, 2014). Obviously, some technical methods are not used only for assisted reproduction, but in all fertility examinations. For example, the prenatal check-up will intensify pregnant women’s awareness of disease risk and health responsibility ethics, and thereby an anxious maternal experience is formed (Lin, 2011). Even postpartum newborn screening may have this effect. The line between disease and health is blurred. As to whether a child with no clinical symptoms whose birth has been facilitated by ART should be diagnosed as ill, even an experienced doctor can hardly give a definitive answer. The child’s family, especially the mother, is often in a state of anxiety (Timmermans and Buchbinder, 2013).
The above-mentioned research tells us that while ART improves human health, it also creates painful and anxious experiences. These experiences confirm that medical science itself is filled with risks and uncertainties (Webster, 2002). However, we should note that uncertainty does not only create anxiety in a negative sense, it may also indicate the existence of hope; anxiety, as an emotional experience acquired by the individual body, cannot be separated from the overall social and cultural context. If people only see the anxiety brought about by the uncertainty of technology, they will fall into a blind critique of biomedical technology.
The theoretical framework and methodology of this article
The above-mentioned literature has undoubtedly increased our overall knowledge and understanding of ART. First, it provides an opportunity to test the relationship between technology and local social and cultural contexts. Technology itself is the product of society, and its application and practice must be deeply rooted in the local social and cultural context. Only when it is recognized by cultural norms and power relations can it be implemented (Inhorn and Birenbaum-Carmeli, 2008; Shiling, 2011; Webster, 2002). Second, it reveals that the reality of undergoing ART treatment is far from the overwhelmingly positive image that is created by the medical community and propagated in the media. Patients, especially women, reveal the emotional challenges it brings: stress, tension, anxiety, and feelings of helplessness, which can lead to excessive deprivation of the body. Obviously, the former’s insights are contextual, revealing the social basis of technology applications, while the latter’s are experiential, realizing a criticism of technology and society in the painful experiences of patients. Therefore, fundamentally speaking, both emphasize the external environment: neither the social situation nor the technology itself gives the experience associated with ART and its female subjectivity a reasonable place.
The theoretical framework of this article is designed not only to give the female experience an essential position, but also to bridge the gap between the context and the individual. Through ethnographic information, this article attempts to thoroughly describe the anxious and hopeful contradictory experiences of infertile couples (especially women) during assisted reproduction (including before and after treatment). This experiences is characterized by duality: on the one hand, the inscription and control of the body by the local context and technology have shaped the above-mentioned contradictory experiences; on the other hand, it shows that women actively learn strategies from existing cultural resources when perceiving the above-mentioned experience, so as to cope with the constraints of the social situation, which illustrates their subjectivity and individuality.
If we want to emphasize the shaping of the body by social-cultural contexts on the one hand, and on the other hand we also include people’s subjectivity within the scope of consideration, then this requires a methodological strategy. The concept of “embodiment” has the theoretical potential to resolve the dichotomy of situation and individual, structure and behavior, society and biology. The “body” is a biological material entity, and embodiment belongs to the field of methodology. Scholars represented by Maurice Merleau-Ponty, Pierre Bourdieu, Margaret Lock, etc., use embodiment as a converter, or a link, to try to surpass the subjective–objective, behavior--structure, and biological–cultural dualism that has plagued philosophy, anthropology, and related disciplines for a long time. Merleau-Ponty’s (2005) perceptual phenomenology assumes that the body is a setting in the relationship of the world, and consciousness is the projection of the body to the world. That is to say, perception begins with the body and acts on the object through reflective thinking. At the level of perception, there is no difference between subjective and objective. For Merleau-Ponty, the body has never been a simple biological object, but the embodiment of consciousness, the origin of intentions and various practices. Bourdieu’s (2017) practical theory also emphasizes that culture is neither derived from individual motivations and actions, nor is it a product of underlying rules and structures, but is actively constructed by social actors based on physical habitus, and is also the result agreed upon with the previous rules, the product of the interaction between rules, actions, and action strategies. Through the strategy of embodiment, Bourdieu’s practical theory not only gives status to structure, but also gives autonomy to behavior. He tried to find a way out from and an alternative position beyond individual behavior determinism and structural determinism. Lock and Nguyen (2010) put more emphasis on the embodied situational nature and the resulting variability and plasticity: body and culture are intertwined, and they are inevitably embedded in the evolutionary, historical, life-cycle, and temporal and spatial changes of the surrounding environment, which are characterized by plasticity and contingency.
Adhering to the embodied theoretical insight, the experience of female patients in ART advocated in this article is not an emotional category at the individual psychological level, but an embodied experience. It emphasizes the interwoven relationship between the female body and the external situation (Figure 1): external situations (such as social moral pressure, uncertainty of medical technology, etc.) shape, inscribe, and even control the bodies of female patients and present them through their perceptions and experiences; women also take actions and devise strategies involving their bodies (such as body conditioning, worshiping folk deities like Guan-yin, etc.) in the local context (such as medical discourse, diet therapy culture, and folk beliefs) to participate in the process of infertility treatment. Because women exhibit subtle and differentiated experiences at different stages of treatment, we also incorporate the variability and procedural nature of their experiences into the framework of analysis.

Research framework.
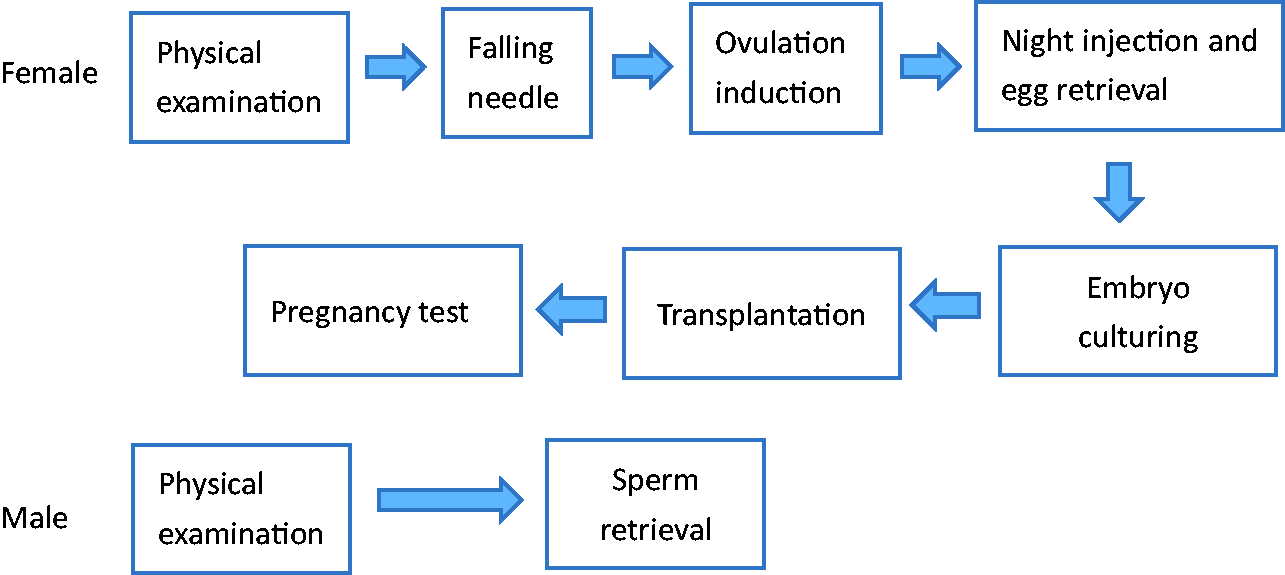
Routine process of first- and second-generation IVF-ET technology.
Triple moral pressure
Existing ethnographic data show that no society, culture, religion, or law is neutral in the face of fertility (Vayena et al., 2002). It is generally believed that fertility is a “normal” life issue. In most Western societies, fertility is linked to personal happiness and gender roles. Therefore, even if individuals have the right to choose whether to have children or not, infertility is still regarded as an interruption of continuous life, a failure to achieve gender roles, and a challenge to the stability of social relations. In non-Western societies, the social and economic reasons for fertility are more prominent. Childbirth is regarded as the basis of family and social continuity. Infertility often results in stigma, even the breakdown of marriages, social exclusion, and violence against women (Balen and Inhorn, 2002; Fei, 1998; Greil, 2002; Pashigian, 2002). Fundamentally speaking, the cultural inevitability of reproduction has become the main reason for infertile couples to choose ART. However, the fertility culture also stipulates which fertility forms are “normal” (Balen and Inhorn, 2002). ART may be regarded as violating people’s expectations of natural reproduction, destroying traditional parent--child relationships, and even carrying stigmas, factual or imagined. Therefore, women who seek help from ART at the least face the triple moral pressures of infertility, assisted reproduction, and the national policy mentioned below.
Oulan, 34, was married in 2011 and had not been pregnant. Due to family and social pressures, she had to quit her job to make time for her body. Speaking of her decision to resign, which she still regretted, she said: I was stupid: when I resigned, I said that I might condition my body for half a year prior to doing the test-tube treatment. As a result, the company thought that I was going to enter test-tube treatment directly when I resigned. A colleague chatted with me before I left; I said I would go to do insemination [artificial insemination] if I had no other choice, and she also asked, “did your husband agree to this?” implying that the sperm would not be my husband’s. Now I am very regretful, it should not have been said. But I will not tell them that it is a test-tube baby if I get pregnant. I will tell them that I cured myself by taking Chinese medicine, and I just took an ovulation injection. (Oulan, 34 years old, married in 2011)
Even so, in contrast to the stigma and moral pressure of infertility, people still choose ART as the “last straw” under circumstances in which they have no other choices. For most patients, natural pregnancy is the first choice. Even if some patients have entered the stage of ART treatment, they will not give up the possibility of trying to get pregnant naturally. During the investigation, from time to time I heard that some patients had conceived naturally after failing to get pregnant with IVF treatment. When a natural pregnancy is unsuccessful, the first thing that a female patient thinks of is whether Chinese medicine, Western medicine, or some other folk medicine might treat the infertility through physical conditioning, surgery (such as dredging the fallopian tube), or even rituals. When these attempts are ineffective, finally they will choose ART. This also means that ART is often the last choice for the treatment of infertility.
Mrs. Zhao was 29 years old and was from Sichuan. She had married in 2011. Her husband was from Zhuhai, and they had been living in Chengdu since their marriage. Mrs. Zhao had always had symptoms of irregular menstruation, and there was no sign of pregnancy a year after marriage. She first turned to a famous Chinese medicine doctor in Chongqing. After a period of treatment, she became pregnant, but she had a miscarriage when she was two months pregnant. After that, Mrs. Zhao was unable to get pregnant, so she went to the hospital for an examination again. This time she was seen in a gynecology department, where the doctor told her that there was a problem with one of her fallopian tubes and surgery was needed. If she did not have a child within six months after the surgery, this might be due to tubal adhesions. Six months later, Mrs. Zhao was still not pregnant, so she underwent a second fallopian tube surgery. This time the doctor also suggested that she undergo a IVF procedure. I was born in a small county, unlike in Guangdong. I didn’t know what a test-tube baby was at that time. I thought it was not my own child, so I said that I didn’t want to do test-tube treatment. After half a year, I still couldn’t get a baby. Gradually I understood what a test-tube baby was. (Mrs. Zhao, 29 years old, married in 2011)
Unlike patients who are having their first child will try many other treatments before trying ART, women of childbearing age who are having their second child are more decisive in their choice of ART. Women facing secondary infertility, in which they have previously given birth and thus already have one child as a “guarantee”, face less stigma and pressure than those with no previous births who are experiencing primary infertility. The disadvantage of the woman with secondary infertility, however, lies in their age. They often regard ART as the “most direct” means of assisting in pregnancy, and eagerly want to use this technology so as to catch the last train of the “birth of a second child”. As with Mrs. Yun, 44 years old Lian Xia decided to turn to ART in August 2016 after the universal two-child policy was introduced. She said: After the policy was released last year, I felt that there was such an opportunity, and I was really unwilling to waste it. I first looked at Qingyuan Hospital last year. The doctor said that the conditions were good, and I went home to prepare for pregnancy, but I could not get pregnant. When I had myself checked again, there really was a problem. The doctor said that one side of my fallopian tube was blocked. My husband and I have been working hard on our own for so many years. Now we have bought three houses and a car, and with the new policy being introduced, I really want to have another child. (Lian Xia, 44 years old, daughter 18 years old)
During fieldwork it was observed that the Reproductive Center has been facing a surge in demand since the two-child policy was introduced. The number of infertile couples seeking ART treatment has suddenly increased. For a time, the supporting facilities and services of the Reproductive Center were in short supply. According to patients’ personal experiences, those undergoing first-generation and second-generation IVF treatment had previously been able to enter the IVF treatment cycle immediately after completing various preliminary physical examinations. But, since mid-2016, patients must be scheduled to enter treatment after completing the physical examination, sometimes even waiting for one to three months or even longer.
Here, we see not only the continuation of traditional fertility culture, but also the governance capabilities of state power and policies in controlling populations and female bodies (Foucault, 2012; Yan, 2006). In 2014 and 2016, local governments successively launched the “second-child” and “universal two-child” policies. The collaboration of the national fertility policy with the traditional fertility culture (in addition to the exaggeration of the media) not only gives “giving birth to two children” a scientific and policy basis, but also is morally binding. Having a second child is a policy advocacy for the country, and it may be a good expectation for the family. For women, especially older women of childbearing age, it means constant physical conditioning, transformation, and repairing, and it is also a source of anxiety and stress.
Uncertainty of the treatment process
Biomedicine has played an important role in improving the level of human health since its development (Lock and Nguyen, 2010). However, in reflections on science and progress, the limitations of science and its “natural defects” have been exposed to the public (Beck, 2004; Lock and Nguyen, 2010). Among them, medicine, often designated as a branch of natural science, is undoubtedly a place filled with risks and uncertainties (Webster, 2002). In terms of reproductive medicine, when a pregnancy is successful, the biological “facts of life” can provide a causal explanation, but when infertility occurs or pregnancy fails, it is often difficult to find an exact biological explanation (Franklin, 1997). Doctors often give uncertain explanations, such as “an unexplained cause”, “it may be a problem of a fallopian tube”, or “the endometrium may be too thin”. Pregnancy has become a simple, but also very complicated and unpredictable, process. Facing this kind of helplessness due to an uncontrollable and uncertain future, people often experience anxiety (May, 2010; Zhang and Huang, 2017). However, the uncertainty of the outcome also implies the possibility of physical and medical miracles, which makes women still maintain hope along with the anxiety.
The complexity of the process and the uncontrollable body
For most patients with infertility, the complexity of the process of treatment with ART is completely unexpected. In the “New Patient Reception Process” brochure issued by the Reproductive Center, only the stages of registration, medical consultation and evaluation, three-certificate review, signing of informed consent, and entry into the treatment process are shown. Even if the patient knows this in advance through other people’s accounts and online materials, once the treatment cycle is truly entered, the complexity of the ART treatment process is still dizzying.
For new patients, the preliminary physical examination is the beginning of a true understanding of the process. This stage can be regarded as the preparation stage before the patient officially enters the treatment cycle. Women need to be checked on at least 15 items, such as ovarian function combination and syphilis combination, and men need to be checked on 5 items, such as syphilis combination and semen routine (Figure 2). The doctor will decide on the appropriate treatment plan based on the patient’s physical examination results. After entering the treatment cycle, the first step is to induce ovulation. First, down-regulating drugs are used to inhibit the pituitary gland to make it insensitive to estrogen, to prevent women from ovulating prematurely, and then ovulation drugs are used to stimulate the simultaneous development of multiple follicles. During this period, women need to be injected with drugs every day and the growth of their follicles regularly monitored through vaginal ultrasound. The second step is night injection egg retrieval and sperm retrieval. The follicle detection board shows two bars to indicate the maturity of the follicles. The night injection should be given at about 9 p.m., and the egg retrieval performed two days later; at which point the man’s semen is also collected. The third step is embryo culture. The laboratory combines the sperm and egg and observes the fertilization of the egg. The fourth step is transplantation. Generally, four to six days after the egg retrieval, the doctor will select a certain number of embryos to be transplanted into the woman’s uterus according to the regulations. The woman must be injected with progesterone continuously before and after the transplantation to provide luteal support. The fifth step is the pregnancy test. About 14 days after transplantation, pregnancy is determined via urine and blood tests. If the woman is pregnant, she must continue to receive the corpus luteum for two months. If she is not pregnant, the drugs must be discontinued (Zhuang, 2005).
On the day of the interview, Ying Tang had just decided on the IVF treatment plan and had officially entered the treatment cycle. This was her first IVF treatment. As Ying Tang spoke of her mental journey since starting the IVF treatment process, she became tearful: For so long, I feel that I have been very confused, and I don’t know what to do next. What is the “long plan” and the “short plan”? The woman who just chatted with me said that she was using the long plan. I was so confused that I didn’t know what it is. I only know that the doctor asked me to come back for checkup after 20 days after menstruation. The “sisters” [i.e. the other patients in the facility] are still talking about fresh embryos and blastocysts. When I listened to the lecture before, I heard the teacher say these terms, but I didn’t understand what the difference between these two is. When I went to check my vaginal discharge, it was not until I came that I found that I had to have a clean menstruation for more than four days and I couldn’t have sex. It’s so annoying, I didn’t know before, so I had to come again. (Ying Tang, 34 years old, married in 2016)
After the treatment cycle has started, every procedure becomes a serious concern for the patient; for example, the accurate time schedule of inspection and injection, the definite dietary requirements, any subtle part of which could affect the process of the cycle. Faced with increasing numbers of patients, doctors and nurses barely have time to answer women’s questions. Nevertheless, the patients themselves are passionate to communicate about all kinds of medical terms and procedures, aiming at enriching their experiences. Some knowledgeable patients even become “think tanks” for others; they are familiar with the IVF treatment process and are able to explain all kinds of diagnostic test parameters so that they can relieve the confusion of other patients. However, according to Lai (2017), this seemingly rational action of the patients for coping with complicated medical procedures by enriching their knowledge could actually produce “secondary anxiety”; as the old saying goes: “He that increaseth knowledge increaseth sorrow”.
The counterpart of the complexity of the IVF treatment process is the uncontrollable nature of the patient’s body, including menstrual disorders and the varied thicknesses of endometria. This uncontrollability becomes a torture for the patient, diluting her excitement and expectations with unforeseen incidents and endless waiting. My period has been delayed for 11 days this month. How could retrieving eggs affect me so greatly? Every day I felt pain and distension in my abdomen, but my period just didn’t make an appearance. One day, I even dreamed of my period coming. I’m literally expecting my period every day so that I can end the cryopreservation. In the beginning I made the appointment for embryo transfer in December last year, but my period just kept coming late every month. Then the Chinese New Year vacation in the month before last delayed the transfer again, again and again till now it is February, yet I still haven’t entered the IVF treatment cycle. I don’t even know if I should go to the hospital for inspection. (Yunrong, 39 years old, second marriage, with a first-born 14-year-old daughter) When my period was delayed for the third time, I didn’t really know what I should do. I’m worried that the next transfer will have to be postponed again. The missed period is driving me crazy, for the third time it has been late for half a month. What’s more, some of my inspection results are not qualified yet and extra treatment is needed; it makes me want to cry out loud! I wish I could conduct the transfer earlier, but I keep waiting and waiting endlessly. Moreover, I’m also worried that extra medicine could affect my period. The transfer seems so far away, and I have failed it two times. I really want to cry. (Mengyuan, 32 years old, married in 2009) During my last transfer cycle, I started to take Clomifene on the fifth day of my period. But on the tenth day, medical ultrasound showed that my endometrium thickness was 3.6 mm. Therefore, the doctor prescribed drugs to thicken the endometrium. However, on the twelfth day, ultrasound showed that it was only 3.8 mm thick, which according to the doctor was too thin to continue this transfer cycle. In the end I had to let go of that follicle. It’s such a misery, waiting after waiting for month after month. (Mrs. Feng, 41 years old, married in 2001, with a first-born 15-year-old son)
Generally speaking, the best condition for implantation is when the endometrium is 8–12 mm thick. In the patients’ usual metaphor, the endometrium is compared to soil, which should have suitable thickness for the seed, as an analogy of the embryo, to implant. When the condition of the endometrium is not suitable for implantation, the doctors advise patients to give up this cycle or cryopreserve the embryo, waiting for the time to come. No matter what the decision is, it always means an interruption of the cycle for the patient and uncertainty regarding the beginning of the next cycle. Menstruation and endometria are natural parts of women’s somatic experiences; however, women can feel that their own bodies are out of their control during the treatment. This experience of being somatically out-of-control alienates the self from the body, making future treatment procedures unpredictable, and even becoming a source of self-defeat and sorrow (Clarke et al., 2006).
Treading on thin ice
Women with infertility often describe the IVF treatment experience in terms of “treading on thin ice”. The procedures, from physical examination to final transplant and pregnancy, are closely linked, yet suffused with latent hazards: the possibility that they are declared unfit as a result of physical examination, the possible maldevelopment of a follicle in the process of ovulation induction, the possible lack of ova for retrieving eggs, the possible failure of implantation, and even after a successful implantation the possibility of subclinical abortion. Failures can lurk anywhere, and any failure can impede treatment, leading the whole cycle to fail. The failure in this case means a failure of the IVF treatment cycle, indicating that the expected pregnancy has failed. Instead, success in this case is not only relative, which indicates the success of every procedure in the cycle, but also an absolute success, which is the success of reproduction (Franklin, 1997).
The Reproductive Center’s brochure claims definitively that the pregnancy rates after IVF-ET treatment are approximately 50%. The pregnancy rates here indicate the clinical pregnancy rates calculated by dividing the number of transfer cycles into the number of clinical pregnancy cycles (Luo, 2014). However, after clinical pregnancy there still exists the risk of miscarriage and ectopic pregnancy, which means that the clinical pregnancy rate is higher than the live birth rate. For example, if there were 600 females who had undergone embryo transfer, among whom 300 reached clinical pregnancy, but in the end only 260 of them had successful childbirths, the pregnancy rate would be 50%, yet the live birth rate would be 43.3%. Almost none of the women we met during the fieldwork of this study had ever doubted the veracity of the 50% success rate; on the contrary, their primary concern was that there is another 50% chance left for failure, which terrifies them. Before the IVF treatment cycle, women often felt that they could be one of those lucky women on the right side of this 50-50 split. During the IVF treatment cycle, however, their dominant feelings are fear and anxiety about failure. Recently I have lost sleep all night long. Sometimes I can’t stop crying even when I’m asleep. I’m really scared that this time it is going to fail again. I keep worrying about things, what if the condition of my ovary is not good enough? What if the egg could not be retrieved successfully? What if after the retrieval, the quality of the follicle is not good enough and is unable to fertilize an embryo for transfer? Other 34-year-old women are already striving for their second child, but I don’t have my first birth yet. I am also worried that my body could be affected badly by the treatment, resulting in my not being able to have a second birth in the future. (Ying Tang, 34 years old, married in 2016)
During the IVF treatment cycle, some critical nodes exist that determine the success of treatment: oocyte retrieval, in vitro fertilization, embryo transfer, pregnancy testing, and the final pregnancy. In what follows in this article, we will use the procedures of oocyte retrieval, embryo fertilization and pregnancy testing as examples to illustrate the uncertainty and experiences of women in ART treatment.
There are two reasons why oocyte retrieval is seen as a critical process. First of all, it is the most painful process for women in the whole treatment; secondly, the number of follicles retrieved in this process affects the number of embryos directly. The technical term for oocyte retrieval is “transvaginal ovum retrieval”, an operation carried out under a general or local anesthesia. Under ultrasound guidance, a needle penetrates through the vaginal wall and into an ovarian follicle. Female patients often chat about their numbers of eggs retrieved and numbers of embryos; those who have more embryos are jokingly called a “wealthy family”, which parallels the follicles and embryos as a kind of wealth. Under general conditions, with the help of ovulation induction, 30–40 oocytes could be retrieved from a young woman at one time. However, women over 30 years old are faced with recession in fertility function, which could decline even more gravely after 35 years old, accompanied by a declining number of follicles and lower quality of eggs. After the retrieval, the eggs will be fertilized in vitro by the sperms and come to form zygotes (which generally takes 3 days). When ova are plentiful, the zygotes of good quality will be cultured for two more days and come to form blastocysts. The formation of blastocysts will naturally screen out zygotes of low quality, making the success rates of transfer higher. But this process of culturing is also risky, especially when the number of ova retrieved is not large, under which circumstance the doctors would not advise culturing the zygotes further in case there is no embryo left for transfer. The woman’s age is directly related to fertility function, and thus older women have a highly sense of crisis about their age, being beset by anxiety that “this could be my last chance to have a child”. I used to lose sleep all night, now I have to force myself to sleep … Before the retrieval I made a wish in my mind: please do not fail me again since I finally got more follicles this month. I cared about nothing other than these ten follicles of this month, it’s really rare to have them so I have to make full use of them. Some nights I fell asleep but woke up at midnight then suffered from insomnia … During the retrieval I felt nothing, but after the operation I felt so hurt and started to cry. My husband said that other people were all looking at me, but I was not crying out loud, just crying silently. I was not crying for fear of pain, but for feeling so sorry for myself after the retrieval. God is not fair with us … Actually, the result was not bad. Five eggs had been retrieved and two embryos transferred, the other two were cryo-preserved. I feel myself lucky enough to have four successfully cultured embryos. (Oulan, 34 years old, married in 2011) The retrieval is actually not that painful, but the cleaning before the operation is really painful, I had never felt that pain in my life before. Remembering the pain of taking out leucorrhea, the pain of cleansing, the pain of taking injection, all kinds of pain, I really thought of giving up at that time. I have no idea how my ovarian function could become better, since I’m at a difficult age. Under such conditions, I did not have much confidence in success. I felt like taking all these injections was useless, it didn’t make any difference since I didn’t feel chest distress or abdominal distension just as usual. After the retrieval, the dull pain lasted for more than a week. (Tian He, 33 years old, married in 2009)
With a fit body condition, female patients could undergo the operation of embryo transfer 3–5 days after the retrieval. Two weeks after the transfer, they could test for pregnancy through a urinalysis or blood test, which was metaphorically referred to as the “lottery draw”. The lottery draw was a check for the results of the previous cycle of ovulation induction, oocyte retrieval, and embryo transfer, and also offered a crucial reference for subsequent miscarriage prevention and body care, therefore becoming another critical node of the treatment. A successful pregnancy was referred to as a “jackpot”, revealing that pregnancy was filled with randomness, even with the assistance of technology. Besides the medical evidence of urinalysis and blood test, women also used every somatic sensation they could to judge whether they had won the lottery. It was on the eighth day that I used a pregnancy test kit and found myself pregnant. I did not even dare to feel happy, fearing that it could be a false alarm. I literally dared not to be happy, because I was afraid of a disappointment and blow. I had not even told my husband about it and planned to wait for the assured result. The next day, I went to do a blood test, and the HCG level was higher than 400. At that moment the only thing I wished for was that I would give birth to my child safely and soundly. Later, on the twelfth day, I went to draw the lottery, and it turned out that my HCG level was about 1800. The doctor said that it could be twins. But there have been chromosome problems, so there is still a long way to go. (Silu, 36 years old, remarried in 2014) One day feels like a year. The test-tube treatment is such a spiritual trial, it is so hard to face everything indifferently … On the ninth day, I felt strong distension in my womb, and the trace on the test kit was more obvious than before, yet I was still afraid that it could be a false alarm … On 11 November, I went to check my HCG level, which was 873, making me feel such a relief. (Xiaocui, 26 years old, married in 2015) Time passes by as slow as a snail. Women always feel that time flies quickly while they look on others’ waiting after transfer, but actually, the others themselves are experiencing one day as being like a year. For me that was the longest week in my life. On the tenth morning, the test kit showed nothing. After a few days it still showed nothing, I felt that there was no need to go to hospital for further tests anymore. (Yezi, 27 years old, married in 2012)
Only after experiencing an accurate HCG (Human Chorionic Gonadotropin) inspection can female patients finally determine if they are pregnant. Nonetheless, even if the inspection indicates pregnancy, women can still be stuck in anxiety about upcoming risks, reflected in different levels of HCG: if the level is too low, this indicates a high possibility of subclinical abortion; if the level is high, it could indicate the possibility of premature implantation, generally resulting in a pregnancy or morbidity like a molar pregnancy. Female patients in the IVF treatment cycle have experienced procedures of physical examination, ovulation induction, oocyte retrieval, embryo transfer, and the “lottery draw”, and some of them have even come through more than one IVF cycle to see the silver lining of pregnancy. The more painful the course is, the more people cherish their every uneasy step forward; the more people cherish it, the more they worry about the unpredictable risks of ectopic pregnancy, miscarriage and fetal deformity. However, the risk does not arise for certain, so they always refer to the cases of others for self-comfort: “I heard that another ‘sister’ had the same condition as I have before, but in the end, she gave birth smoothly—everything is possible”. Everything is unpredictable: an embryo of good quality may end in failed implantation, while a low HCG level could still result in a successful childbirth. These risks and miracles are not only probability statistics in books, but real stories that we may have heard of. The risks are always lurking until the moment of childbirth, and anxiety and hope intertwine in this fluctuant state.
The uncertainty of ART makes women realize that failure could happen at any point, that success is always temporary and could be replaced by failure at any time. Every procedure in the IVF cycle could come to nothing, and the failure for an “unknown reason” would be even more unacceptable for women (Franklin, 1997). Under normal conditions, people tend to seek more accurate information when faced with the uncertainty of medicine. In the case of ART, the existing knowledge is not sufficient to explain the reasons for failure completely. Even the most experienced doctor can only give approximate answers. This dilemma reveals that women are eventually faced with inadequate knowledge and unable to change a thing, under which circumstances they are trapped in doubts toward medicine and the reproductive technology itself, and in the meantime they comfort themselves, seeing the other side of uncertainty as a kind of opportunity and hope.
Going ahead with hope
Under the moral pressure of reproduction, women seek help from the “hopeful technology” of ART, which is actually not so direct or convenient as it seems, but instead is filled with difficulties and obstacles. That physical traumas are caused by reproductive technology goes without saying (for instance, the pain of oocyte retrieval and ovarian hyperstimulation syndrome). While these traumas may be temporary and concealed, the real, long-standing torture lies in the persistent anxiety, helplessness, and panic caused by all kinds of pressures and uncertainties. In spite of these tortures, women, especially those who have not yet had a first birth, will not flinch passively out of anxiety. Instead, faced with uncontrollable technology, they try to make changes on their own and utilize all kinds of extrinsic faith to eliminate their pressure and anxiety. Their actions, on the one hand, manifest the agency and tactics of individuals, and on the other hand, they reveal to us how the technology is embedded in daily life and experience, eventually becoming integrated with local knowledge.
Mediating the body
From the Foucauldian perspective (Foucault, 2002: 102–105), biomedical power as a kind of “biopower” has the ability to discipline an individual’s body. As noted above, in the context of ART there are many bodily indicators of whether the IVF cycle can be carried out, for instance, the menstrual cycle, the number and quality of ova, the condition of the endometrium, etc. These biomedical discourses are constantly shaping women’s perceptions of their own bodies. Women use all kinds of methods to manage or maintain their bodies, hoping that they can make a little change by themselves even when the technology is out of their control. Exercise and diet therapies are the most common methods of body care among them. I have insisted on sport walking for three months and doing a foot soak every night for one month. The foot soak is really useful, since I can sleep soundly without dreaming. After all, I have already done all that I can do, soaking my feet and doing exercise, striving for the best results and leaving the rest for God to decide. God will prefer those who have prepared. Doing exercise does make things better. Before the treatment I never cared about sports and never did exercise; it was only at the end of last year that I became aware of how important health is. (Silu, 36 years old, remarried in 2014) It’s useless to go fishing for three days while drying the net for two days. I used to be lazy, but this year I have changed. Before the transfer I insisted on running every day. Last year I was just so lazy, I only soaked my feet when it came to my mind; if I forgot about it then I just let it be. However, this year, after I came to Guangzhou, I have insisted on running every day. (Caixia, 29 years old, married in 2012) It is said that eating durian can help the endometrium grow, while eating apples would make it thinner. In the previous two cycles, I hadn’t eaten them, but this time I’ve tried to eat anything that could be helpful. Recently, the price of durians has risen to more than 20 yuan per 500 grams, it cost me hundreds of yuan to eat three durians, and this time my endometrium has finally grown better. (Mrs. Feng, 41 years old, married in 2001, with a 15-year-old first-born son) Many “sisters” are drinking soybean milk, so I started to drink it before the ovulation induction, as it is said to be helpful for the endometrium. Maybe because of the soybean milk, in this cycle my endometrium is in quite good condition, everything goes well, including the embryo transfer, so I plan to keep drinking it after that. (Mrs. Zhao, 29 years old, married in 2011) I fry eggs with mugwort and yellow rice wine using camelia oil. All these ingredients are taken from my old home. Every morning I eat them on an empty stomach so as to mediate my qi and blood and to warm up my uterus. I got this recipe from one of my relatives when I went home for the lunar new year; she said that I had to keep eating these things since I was in poor health. Since I had a miscarriage in 2011, I became aware that my body condition was not as good as before. That relative of mine told me eat some meat from undomesticated animals, and repeatedly asked me to stick to this habit. (Miao Shen, 33 years old, married in 2008)
In China, the homology of food therapy and medicine has always been an important part of the food culture, which includes both the “food nutrition theory” that focuses on daily diet and the “food therapy prescription” that uses food as medicine. It is believed that the type and amount of food one eats is closely related to one’s health, and that, in a sense, food is also medicine (Zhang, 2003: 254). The cultural delicacy of food and health is even more evident when combined with the concept of balance between yin and yang, hot and cold. We cannot judge the actual effectiveness of the various foods presented in the above cases (e.g. durian, soy milk, gum, eggs, etc.) in aiding pregnancy, but once they become the remedies recommended or not recommended by the “other sisters”, these foods take on a moral connotation and a judgment of good or bad. People do not readily say “no” to a folk remedy as long as it is accessible and could alleviate illness. Although all the ART procedures are fraught with uncertainty, these women still want to increase their probability of success somewhat by actively managing their own bodies. Their active management also shows that they are doing their best rather than being passive, which helps to alleviate moral censure under the circumstance that the treatment fails.
Yuan, fate, and Guan-yin worship
Faced with the uncertainty of ART and the incoherence of medical explanations for treatment failures, women are inclined to invoke spiritual faith and establish a connection to supernatural forces to compensate for the incompleteness of medical science itself (Bharadwaj, 2006). Yuan (缘, “predestined relationship”) and fate (ming 命) are two idioms these women use frequently. Something will occur if it belongs to your fate; if not, do not ask for it. Last time I went for an ultrasound examination 45 days after the implantation, which was about six weeks; theoretically, the gestational sac could be seen at that stage, but it didn’t show up, and even the doctor was unable to tell whether it was an ectopic pregnancy or not. I couldn’t believe it and went to do an HCG inspection after several days. It finally turned out to be an ectopic pregnancy, and I had to be hospitalized in the ICU for two days. Yuan really matters! (Hong Ye, 27 years old, married in 2013) Before having the IVF treatment, we all thought that it would succeed first time, but only after having experienced it did we come to know how difficult it is to have a child. It’s really hard. It’s not the case that two seeds implanted will definitely result in two fruits, in fact, what the two transplanted embryos will result in is totally a matter of yuan. Without yuan, ten embryos transferred could result in nothing. In my family, the zodiac sign of my parents and my sister is the rooster; a baby born this year shall be a rooster too, I think it indicates we have the bond of yuan as a family. (Sha Liu, 31 years old, married in 2011)
How can we tell if there is enough yuan? It is believed that an embryo is already a life and has the spirituality to determine whether it has yuan with the mother. Silu experienced the tragedy of twin abortion after her embryo transfer. She said, “The baby will only come to you when you have enough yuan, which is ordained by God. I had embryo damage once, I guess it’s because the twins don’t want to be my babies yet” (Silu, 36 years old, remarried in 2014). In her opinion, the embryo has the potential to develop into a baby and is therefore alive and able to choose its parents on its own. If there is no yuan with the parents, the embryo will not implant in the woman’s womb. If there is enough yuan, the embryo will definitely implant in the woman’s uterus and be given birth successfully, regardless of the medical judgment about bad quality of embryo or bad condition of the maternal body.
Sometimes the yuan is not limited to the topic of pregnancy, but also refers to the fateful coincidence with the hospital itself, which is considered yi yuan 医缘 (nosocomial yuan). Mrs. Zhao was a rather optimistic lady among the interviewees; although her first transfer did not result in success, she still believed as follows: I think I really have yuan with this hospital, and so does my mother, who says that this is yi yuan. Other patients say that queueing up to register is really difficult, but for me everything went smoothly. Every time I come to the hospital, I can see the specialist doctor whom I want to consult. Yuan really matters; those who do not go well in one hospital could change to another one so that things would turn out smoothly. (Mrs. Zhao, 29 years old, married in 2011)
If yuan and fate are determined by a higher power, then “luck” could be considered an undetermined element. Worship of the Chinese folk fertility deity Guan-yin is one action by which patients try to bring themselves good luck or change their luck. Though the Reproductive Center is a medical institution based on modern biomedical science, statues of Guan-yin are displayed in four areas: the outpatient clinic, the medical ultrasound room, the blood sampling lab and the surgery room. These four areas correspond to four different treatment procedures: the outpatient clinic is for the physical examination, the ultrasound room and blood sampling lab function in the process of ovulation induction, while the surgery room is where ova and sperm retrievals as well as embryo transfers are performed. Since the surgery room is where the dual procedures of retrieval and transfer are performed, the Guan-yin statue beside it is worshipped most frequently. In front of the statue there is an iron plate for placing tributes. Every day the plate is filled with fruits, including grapes, apples, pomegranates, and oranges, and sometimes there could be “red envelopes” and snacks. These tributes are not chosen randomly but intended to be good omens; for instance, grapes and pomegranates signify “more children more happiness”, and apples symbolize safety and peace due to their Chinese pronunciation. One of the female patients said: At the start, I only knew that there was a Guan-yin statue in the outpatient clinic, so before I underwent the retrieval, I only worshipped that one. Later on, I found that there was another Guan-yin on the fourth floor (where the surgery room is), so on my transfer day, I went to worship the Guan-yin in the clinic first, and then I worshipped that surgery room one. Many “sisters” have no idea where the Guan-yin is, so I especially spread the locations in our WeChat group. They all say that they will come to worship next time. (Dan Cheng, 28 years old, married in 2014)
On Mrs. Feng’s third transfer attempt, she brought a bunch of grapes as a tribute to the Guan-yin statue near the surgery room. She said: When I previously saw Guan-yin in the blood sampling lab and ultra-sound room, I simply made a bow to them. But today is the big day, so I’ve bought some tributes. I haven’t bought much as there might not be enough room in the plate. As long as Guan-yin receives my tribute, she will be like, “I have received your regard, here’s your baby.” If I make it this time, on my next pregnancy check-up I will buy fruits to pay back her mercy. Not long ago, the Guan-yin who used to be here was missing; it might have been changed to somewhere else by nurses. Yet I still saw people worshipping towards that empty table. (Mrs. Feng, 41 years old, with a first-born 15-year-old son)
The available literature also reflects the fact that neither institutions nor individual women have been passive in the face of negative experiences such as anxiety but both have mobilized all kinds of accessible resources to actively respond to them, religion being one of those approaches. In Ecuador, symbols of God are found throughout clinics, and religious rituals are incorporated into medical practice. In clinics there hang statues of the Virgin Mary or crucifixes, and at important moments such as during the process of egg retrieval, the moment after sperms and eggs are being placed in petri dishes, and before the transplantation, laboratory specialists pray to God for help and hope for a good outcome. The power of life is in the hands of God; infertility or conception is destined by God, and the doctor is only God’s instrument (Roberts, 2012). In India, the success and failure of ART is similarly understood to be “in the hands of God”. Various Hindu idols are distributed in the halls of clinics and doctors' offices, and couples in pursuit of childbirth will travel to temples all around the country to worship, thus giving rise to “clinical theodicies”. In the face of modern technology representing science, people have turned partly to religious explanations and prayers, which, in effect, demonstrates the “incompleteness” of ART itself and its lack of rational explanations (Bharadwaj, 2003).
Modern hospitals in China were once the strongholds of Western missionaries on “medical missions”, but since the 1930s, modern hospitals in China have gradually removed the remnants of religion (and also of folk beliefs) and moved towards being scientific institutions (Yang, 2006).
However, our observations revealed that the statues of the Guan-yin placed in several areas of the Reproductive Center were not removed to prevent them from disturbing order or spreading superstitions. On the contrary, there seems to be a consensus between medical staff and patients that they should tacitly accept the prayers and worship in order to cope with the uncertainty of treatment and alleviate the anxiety of the patients. People’s belief in yuan and fate as well as their devoutly worshipping gods such as Guan-yin further demonstrates that ART is still an incomplete science that forces people to draw on local cultural resources and traditions so as to explain the unknown and unpredictable outcomes of life. Although ART is cutting-edge biomedical technology, in people’s everyday understanding, it seems to be nothing more than a modern version of a traditional child-bearing deity like Guan-yin.
Conclusion
In mainstream narratives, ART is often hailed as a “holy grail” for infertility patients. Our fieldwork focused on women’s embodied experiences at different stages of ART treatment and has enabled us to reveal the triple moral pressures faced by women undergoing the treatment: the pressure of infertility, the pressure of ART, and that of national policy, while the uncertainty of the technology itself places women in a world of heightened anxiety yet offers them a glimmer of possible hope. In other words, what this technology brings to women is far from the purely positive vision of a “technology of hope”, nor does it only bring them the anxiety that has been unilaterally emphasized in the previous literature, but rather it brings women an experience characterized by the coexistence of anxiety and hope. These two emotions are embodied experiences which are not only expressed through words but also through patients’ physical states, dreams, bodily rituals, etc., such as long-term insomnia, crying in their sleep, waking up in the middle of the night, tending to their bodies, and worshipping Guan-yin. This paper argues that anxiety and hope are not only the results of medical practice, but also cannot be separated from local socio-cultural contexts. Infertility is seen as primarily a woman’s fault, leaving her in the predicament of not being able to fulfill her moral obligation and realize the ideal of an intact family. In fact, many women have to quit their jobs and embark on a “journey” dedicated to the process of IVF treatment. The more dedicated women are, the more anxious they become. Of course, they do not retreat from their anxiety and give up easily. They still have faith in the technology, either by conditioning their bodies or even invoking the power of gods to rebuild their confidence and continue the path of treatment with hope.
In the study of ART, the existing literature has mostly adopted the perspective of the interaction between technology and society, which often takes a static yet macroscopic view of the social-cultural limitations and constraints towards these technologies, such as the analysis of how the local politics, economy, religion, and family and kinship relations define the “natural” and “reasonable” forms of human reproduction. Feminist research studies focused on women’s experiences are seemingly concerned with experiences, but, in fact, are meant as critiques of technology and society. This article shows that if we focus too much on the social basis of technology, or if we aim only to criticize society and technology, we will ignore the contradictory embodied experiences of pain, helplessness, hope, satisfaction, and joy under the impact of technology, and we will also lose our basic foothold of concern for humanity. The original intent of this paper was to include both the social context and the patients’ embodied experience as well as their subjectivity in the analytical framework.
In terms of research design, this paper is an attempt to apply embodiment to a fieldwork case. For a long time, research on the body has mainly been oriented to naturalism (mostly by scholars with a biological background) or social-constructivism (mostly by sociologists). Embodiment as a conceptual or methodological strategy is expected to dissolve the long-standing dichotomy of the bio-cultural and the individual-social. However, while phenomenological embodiment focuses on philosophical reflection on human perception, and Bourdieu’s theory of practice introduces the concept of bodily “habitus”, yet both paths still focus on the priority of structure and on the productive function, meanwhile lacking concern about the creativity of the body itself (Yu, 2016). This paper draws on the strategy of embodiment, rejecting both sociocultural and biological determinism, but emphasizing the biological and experiential nature of the body while linking these to the external context, thus stepping out of the dilemma of bio-cultural dualism on the one hand, and avoiding the phenomenological neglect of the social context and the indifference of practical theory towards the creativity and fluidity of the body on the other hand. We intend to emphasize that in the process of in vitro fertilization, the body and culture are intertwined and inevitably situated in the midst of the fluctuations of history, life cycle, and circumstances. The core of embodiment does not emphasize the strictures of social structures simply, but rather the plasticity, fluidity, and tactile sensations of the body as it interacts with the external environment. The embodied experience differs from individual and psychological levels of perception and emotion since it both emphasizes the bodily inscription by the external context and underlines the body’s agency. In this sense, the experience of female patients undergoing IVF treatment is neither a merely physiological or psychological response, nor a consequent product of structure, but a result of the intertwining of the external context and the body itself.
The research in this article is limited to the legal practice of ART. Illegal practices such as surrogacy and ova trading, though equally fraught with imaginings on the part of anthropology and related disciplines, are beyond the scope of this paper. The hope and anxiety stimulated by ART are mainly experienced in the period before the “lottery draw”. Once the pregnancy is successfully generated, the later processes and experiences are actually similar to those in a normal pregnancy, which are also not described specifically in this paper. With further regard to ART, if we were to compare the recipients of the first, second, and third generations of IVF technology, and include men and family members in the study, or even take into account the cognition and behavior of different cultural groups towards ART, many meaningful findings may be generated. In any case, to quote Xunzi, “Life is the beginning of man; death is the end of man. A good beginning and a good ending are enough”. Fieldwork on ART has allowed us to confront the beginnings of life and to understand the creativity and also limitations of medical science and human beings. Every stage of life is mingled with people’s expectations, as well as countless hardships and sacrifices. The pursuit of life is always an interwoven process of nature and culture, and of society and individuals.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.