
Abstract
This study examined changes in dynamic risk factors during non-secure therapeutic residential care (TRC) and their association with recidivism among 313 at-risk adolescents in Norway. Risk was assessed using the Youth Level of Service/Case Management Inventory (YLS/CMI) at intake and post-treatment, and recidivism was tracked over a 1-year period after TRC. Significant reductions in YLS/CMI risk scores were observed during treatment, and both post-treatment and change scores were significant predictors of future justice system involvement. Overall, reductions in most dynamic domains were linked to lower odds of recidivism. These findings emphasize the importance of reassessing risk factors to monitor progress, enhance recidivism prediction, inform follow-up services, and highlight the value of addressing criminogenic needs during residential treatment.
Introduction
Despite relatively low crime rates in Norway, there has been a recent increase in youth offending, with persistent juvenile offenders posing significant new challenges to both the justice and child welfare systems (Bhuller & Røgeberg, 2022). As the perils of continuing antisocial behavior into adulthood can have detrimental consequences (Moffitt, 2018; Odgers et al., 2008; Rivenbark et al., 2018), breaking the cycle of delinquency during adolescence is vital. However, this is not always an easy task, and the complexity of factors that fuel criminal behavior necessitates a comprehensive, systematic, and nuanced approach to both assessment and intervention (Mathys, 2017). Norwegian public health agencies have recognized the importance of risk assessment designed to identify justice-involved youth and their needs, as well as to guide intervention to interrupt the path to a criminal lifestyle (Aase et al., 2020). While this approach has been explored and applied in home-based services (S. Hukkelberg et al., 2022), research in residential settings is limited (Berg et al., 2020; Johansen et al., 2020). This is concerning, as young people in out-of-home placements have poorer outcomes (Gutterswijk et al., 2020), and adolescents in Norwegian residential services specifically experience higher crime rates that persist into adulthood (Drange et al., 2022). This study aims to bridge this gap by exploring the utility of risk and needs assessment in treating serious delinquency among adolescents within a non-secure, community-based therapeutic residential setting.
Risk Assessment and the RNR Model
The evolution of risk assessment has a long history, spanning several generations, from unreliable professional judgment to the use of sophisticated fourth-generation Risk-Need Assessment (RNA) instruments, which integrate risk prediction with case management and intervention components (Latessa et al., 2020). Modern RNAs are built on the Risk-Need-Responsivity (RNR) model, which serves as a foundational framework for evidence-based clinical practice aimed at reducing recidivism (Harder & Knorth, 2015; Pyle et al., 2020; Souverein et al., 2013). In the RNR methodology, RNA serves two important functions: first, to assist in risk prediction, allowing services to match the intensity of interventions to the individual risk level (the risk principle); second, to identify and address needs that can promote positive change in a young person’s life (the need principle) (Wormith & Zidenberg, 2018). Within this approach, distinguishing between static and dynamic risk factors is essential. Static risk factors, such as sex and past criminal history, are strong predictors of future offending but are unchangeable. In contrast, dynamic risk factors are modifiable and represent important “criminogenic needs” because they are areas where change can influence criminal behavior (Andrews & Bonta, 2010). The potential for rehabilitation through dynamic risk factors is rooted in the General Personality and Cognitive Social Learning (GPCSL) theory (Bonta & Andrews, 2017), which posits that criminal behavior is influenced by a combination of individual personality traits, cognitive processes, and social learning through interactions with the environment. Bonta and Andrews (2017) highlight eight central domains containing risk factors consistently linked to offending behavior, which are commonly incorporated into RNAs. These include antisocial behaviors and personality traits, pro-criminal cognitions, criminal associates, substance abuse, family relationships, work and school engagement, leisure and recreational activities, and antisocial history. Notably, all but one of the domains are dynamic and therefore constitute important areas to target in treatment.
Dynamic Risk Factors and Recidivism
The theoretical underpinnings of the RNR model, particularly its emphasis on dynamic risk factors, suggest that reassessment is necessary to capture changes in criminogenic needs during treatment. In this context of Risk and Need Assessment (RNA), it is crucial to distinguish between “risk”—the likelihood of reoffending—and “need,” which refers to the specific criminogenic factors that must be addressed to reduce this risk. Most RNA tools operationalize this distinction by providing a structured framework to assess and address both aspects for juvenile offenders. This dual focus allows RNAs to play a central role in both guiding interventions and monitoring treatment progress, making it particularly valuable in therapeutic and rehabilitative settings. However, while the predictive validity of the eight risk domains has been extensively studied (Olver et al., 2014), there is a notable gap in the empirical literature on how changes in risk factors during treatment affect subsequent recidivism in juvenile offenders (Baglivio, Wolff, Piquero, et al., 2017). Nonetheless, emerging work on youth populations has begun to shed light on how changes in risk matter. For example, in a large multistate sample of justice-involved youths, Krushas et al. (2024) found that those whose risk scores decreased at reassessment were less likely to recidivate, whereas those with unchanged or increased scores were more likely to reoffend. Similar findings have been observed in community-based placements (Wolff et al., 2023). Residential studies also indicate that reductions in risk scores during placements are associated with lower recidivism rates after discharge (Baglivio et al., 2021; Baglivio, Wolff, Howell, et al., 2018; Baglivio, Wolff, Piquero, et al., 2017). Notably, studies suggest that certain dynamic domains may matter more than others. For instance, Baglivio, Wolff, Jackowski, and Greenwald (2017) examined a large sample of juveniles returning to the community from residential placement and found that changes in domains such as school status, leisure, peer relations, substance use, antisocial attitudes, and aggression were linked to subsequent reoffending.
These findings highlight the importance of agencies and clinicians’ reliance on reassessments to monitor and refine intervention strategies. However, most research to date has been conducted in juvenile justice settings, which limits the generalizability to other contexts and jurisdictions. Moreover, variations in settings, programming, recidivism outcomes, and assessment tools emphasize the need to evaluate such an approach locally (Heffernan et al., 2019; Pappas & Dent, 2023). Accordingly, this study investigates whether insights from the treatment and prevention literature can be applied to the unique Norwegian therapeutic residential setting. As convictions and incarceration for adolescents under the age of 18 years are rare (Statistics Norway, 2022), this is the main residential service for juvenile offenders in Norway.
The Rationale of the Current Study
Unlike other European countries, Norway has not established secure institutions for adolescents involved with serious delinquency due to restrictive legislation (Deloitte, 2019). However, following international standards for prioritizing safety, quality monitoring, and adoption of evidence-based practices, the state-level Child Welfare Services in Norway have adopted a risk assessment approach to non-secure Therapeutic Residential Care (TRC) settings (Norwegian Directorate for Children, Youth and Family Affairs, 2010, 2014). These institutions differ from ordinary residential youth care and offer treatment for adolescents with severe delinquency, including repeated and serious offending, violence, and harmful substance abuse. To plan interventions and evaluate treatment outcomes, Norwegian TRC provisions employ the Youth Level of Service/Case Management Inventory (YLS/CMI). The YLS/CMI provides information for targeting and monitoring key areas throughout residential programs and has been shown to be a reliable predictor of recidivism (Olver et al., 2012, 2014). This also holds for its Norwegian translation used in residential care contexts (Kanestrøm et al., 2024). While most research on the YLS/CMI has been centered on predictive capacity, several studies have explored its dynamic properties and case management functions (Peterson-Badali et al., 2015; Vieira et al., 2009). Research has demonstrated that reassessing with the YLS/CMI improves the accuracy of recidivism prediction (Clarke et al., 2017; Mulvey et al., 2016). For example, Barnes et al. (2016) found that both exit scores and dynamic change scores in the YLS/CMI were better predictors of recidivism 1 year after probation than initial scores. Thus, these studies suggest that reassessment with the YLS/CMI should be applied to monitor treatment progress and enhance the precision of recidivism prediction. In Norway, recent studies have employed the YLS/CMI to examine the evolution of dynamic risk factors in adolescents receiving interventions such as Functional Family Therapy (FFT), Multisystemic Therapy (MST), and Treatment Foster Care Oregon (TFCO) (S. Hukkelberg et al., 2022; S. S. Hukkelberg et al., 2023; S. S. Hukkelberg & Ervik-Jeannin, 2022). For instance, S. S. Hukkelberg et al. (2023) found that changes in risk scores predicted the achievement of treatment goals in adolescents receiving MST. Similar investigations with adolescents not eligible for home-based interventions are highly recommended but remain scarce (Aase et al., 2020; Harder & Knorth, 2015; Johansen & Borge, 2023; Pyle et al., 2020). To address some of these shortcomings, the current article explores the association between risk assessment and treatment progress in TRC by using comparative analysis of YLS/CMI intake- and posttreatment scores. The aim is threefold: first, to assess the YLS/CMI’s ability to measure change in risk factors during residential treatment; second, to evaluate the predictive value of change in risk scores; and finally, to examine the relationship between positive treatment changes in dynamic domains (i.e., reducing dynamic risk factors) and recidivism.
Methods
Sample
The sample used in this study stemmed from a register comprising everyone who had been assessed using the YLS/CMI at intake to TRC in Norway. This dataset was merged with administrative register data obtained from Statistics Norway, covering demographic information, general Child Welfare Service measures, and crime outcomes. All participants were referred by local Child Welfare Services to institutional treatment programs under the Child Welfare Act (Norwegian Ministry of Children and Families, 1992). This legislation mandated out-of-home placement in residential care due to severe behavioral problems, defined as serious and repeated delinquency or serious substance abuse. To analyze a change in risk factors, only adolescents who completed a standard TRC course with assessments at both intake and the end of the treatment period were included. This resulted in a final sample of 313 adolescents who received TRC treatment between 2016 and 2019. In instances where an individual had multiple placements, the first residential stay with reassessment was used. Additionally, we identified 217 youths who underwent intake assessments during the same period but did not continue with standard TRC treatment and subsequent reassessment. These individuals were compared to the primary study sample based on intake characteristics to examine potential sample selection bias.
Residential Setting
The sample received treatment in institutions approved for non-secure Therapeutic Residential Care (TRC) under the supervision of the Office for Children, Youth, and Family Affairs (Bufetat). TRC facilities are separated from acute and general youth care institutions to provide more targeted treatment and reduce the potential harmful influence of combining residents with and without major delinquency problems (i.e., deviance training). Furthermore, TRC facilities are risk-differentiated to minimize potential iatrogenic effects of congregated living arrangements: Individuals are assessed by psychologists, risk-matched, and placed in either a clinical “high-risk group” or a “moderate- to low-risk” group. Facilities operate under similar frameworks and objectives and can be approved to manage both risk groups. However, they can offer placements for only one group category at a time to avoid mixing individuals with different risk levels. Consequently, adolescents who received TRC in the same facility were risk-matched but did not receive different levels of treatment. A second clinical category is differentiated by substance abuse problems and is not risk matched. This group is placed in institutions specializing in Residential Substance Abuse Treatment (RSAT). As such, Risk-matched and RSAT institutions were the two main subcategories chosen for this study. These TRC categories share a multisystemic approach aimed at reducing risk and building strengths but are not standardized in terms of intervention dosage or intensity (i.e., not following the risk principle). The institutions are located across Norway and typically operate in small, community-based, unlocked residential homes, providing a structured yet open environment conducive to rehabilitation and positive behavioral change. In most cases, adolescents attend regular schools and participate in recreational activities within the local community surrounding the facility. Institutions are staffed with social workers who focus on providing a positive and stable environment, social modeling, and monitoring and supervision. While restrictive measures can be implemented, staff are required to follow systematic procedures to avoid the use of coercive methods, such as limiting freedom of movement or restricting access to electronic communication. The TRC units collaborate with the adolescent’s family, the Child Welfare Service of the referring municipality, and local agencies and authorities (e.g., schools, mental health services, and police).
Measures
This study used the Norwegian version of the Youth Level of Service/Case Management Inventory (YLS/CMI) as an RNA tool. This tool offers a comprehensive assessment of the risk factors associated with juvenile offending behavior and key areas of criminogenic need (Hoge & Andrews, 2011). The main measure of risk is the total score, which comprises 42 items/risk factors coded as present (1) or absent (0) across eight domains. Seven domains consist of dynamic (i.e., changeable) risk factors: Family/Parenting (six items), Education/Employment (seven items), Peer Relations (four items), Substance Abuse (five items), Leisure (three items), Personality/Behavior (seven items), and Attitudes/Orientation (five items). The static domain, Criminal History (five items), can only remain unchanged or increase in score.
Recidivistic Outcome
To measure criminal behavior after treatment, the study used official register data on police charges as the outcome variable. Any criminal charges registered within 1 year (365 days) of fixed follow-up time after discharge from TRC institutions were coded as a dichotomous variable (yes/no). The rationale behind using charges as a measure of criminal justice involvement is the minimal age for criminal responsibility (15) and the low conviction rate for those under 18 years in Norway (Statistics Norway, 2022). To illustrate, in 2022, only 47 minors received community sentences, and just 29 youths aged 15 to 17 years received prison sentences, which constitutes about 0.01% of the population in this age group (Statistics Norway, 2022).
Procedure
Clinical assessment data were obtained from nationally standardized procedures recorded in a national casework system. All ratings on the YLS/CMI were conducted nationally by clinical psychologists skilled in risk assessment. At intake, each individual case underwent a comprehensive assessment, including the YLS/CMI, using information from local social welfare services and all other available sources. Based on the results, the adolescents were placed in institutions approved for either a high-risk group TRC facility, residential substance abuse treatment, or a TRC facility for moderate- to low-risk groups. After the treatment period, the same national unit reassessed the YLS/CMI using standardized and comprehensive exit reports from the institutions and, when necessary, interviews with staff.
Statistical Analyses
Descriptive statistics were reported as means and standard deviations (SDs) or counts and proportions for the variables YLS/CMI total score and subdomains, as well as age, sex, immigrant status, prior charges, prior state-level Child Welfare Services, placement recommendation, and days in TRC. To measure change in YLS/CMI risk scores during the intervention period, YLS/CMI totals and subdomains at intake (Time 1) and posttreatment (Time 2) were compared using a paired samples t-test. We reported means (SD) at T1 and T2, mean change (SD), and the corresponding significance level of the t-statistic. To assess the overall predictive capacity of the obtained risk scores, Receiver Operator Characteristics (ROC) analyses were carried out with the YLS/CMI total intake, posttreatment, and change score (YLS/CMI scores T2–T1) and 1-year recidivism after treatment as the outcome. The ROC method is widely used to assess overall predictive accuracy in risk assessments due to its stability across different reoffending rates and its ease of comparison between studies (Rice & Harris, 2005). In this study, we used the Area Under the Curve (AUC) as the effect measure with size descriptions as proposed by Rice and Harris (2005): 0.56 for small, 0.64 for medium, and 0.71 for large effects. To further explore the association between risk scores and outcomes, we employed logistic regression analyses using 1-year recidivism as the outcome and the three main YLS/CMI scores, one at a time, as predictor variables. The analyses were conducted unadjusted and adjusted for the potential confounders age, sex, and days in TRC. For the posttreatment and change score, the intake score was also added as a covariate in the analyses to control for baseline risk score. To evaluate how positive treatment changes (reducing risk factors) were associated with recidivism, logistic regression analyses were employed using the reduced scores in the YLS/CMI dynamic subdomains (T1–T2) as predictors for the outcome variable 1-year recidivism. Separate analyses were conducted for each subdomain and were performed unadjusted as well as adjusted for the listed potential confounders. We report 95% confidence intervals (CI) where relevant, and the level of statistical significance was set at .05. All analyses were conducted using STATA (version 18).
Ethics
This work was conducted as part of a PhD study at The Norwegian University of Science and Technology, in collaboration with a register study by The Ragnar Frisch Centre for Economic Research (project nr. 4821). The PhD study was approved by the Norwegian Regional Committee for Medical and Health Research Ethics, under reference number 347377. All data were anonymized, handled and analyzed at the Frisch Centre within the project approvals.
Results
Descriptive Statistics and Bivariate Analyses
Sample characteristics are presented in Table 1. The total sample consisted of 190 males (61%) and 123 females (39%), with a mean age of 16.3 years (SD = 1.2). Almost a quarter (23%) were registered with immigrant status (born abroad), and more than half (55%) had a prior police charge registered before assessment. Previous use of state-level Child Welfare Services was high in the sample, with 77% having a history of out-of-home placement (institution or foster care), and 91% being registered for home-based intervention at some point before placement. Analyses revealed no significant differences in these characteristics between the study sample and the group that did not proceed with standard TRC (n = 271). However, the latter group had significantly lower total risk scores on the YLS/CMI at intake (M = 19.39, SD = 5.5) compared to the main sample. Additionally, this group included more individuals recommended for moderate- to low-risk group facilities and fewer adolescents qualifying for RSAT (i.e., serious substance abuse problems).
Descriptives of the Sample and Those Not Included Reported as n (%) Unless Otherwise Noted.
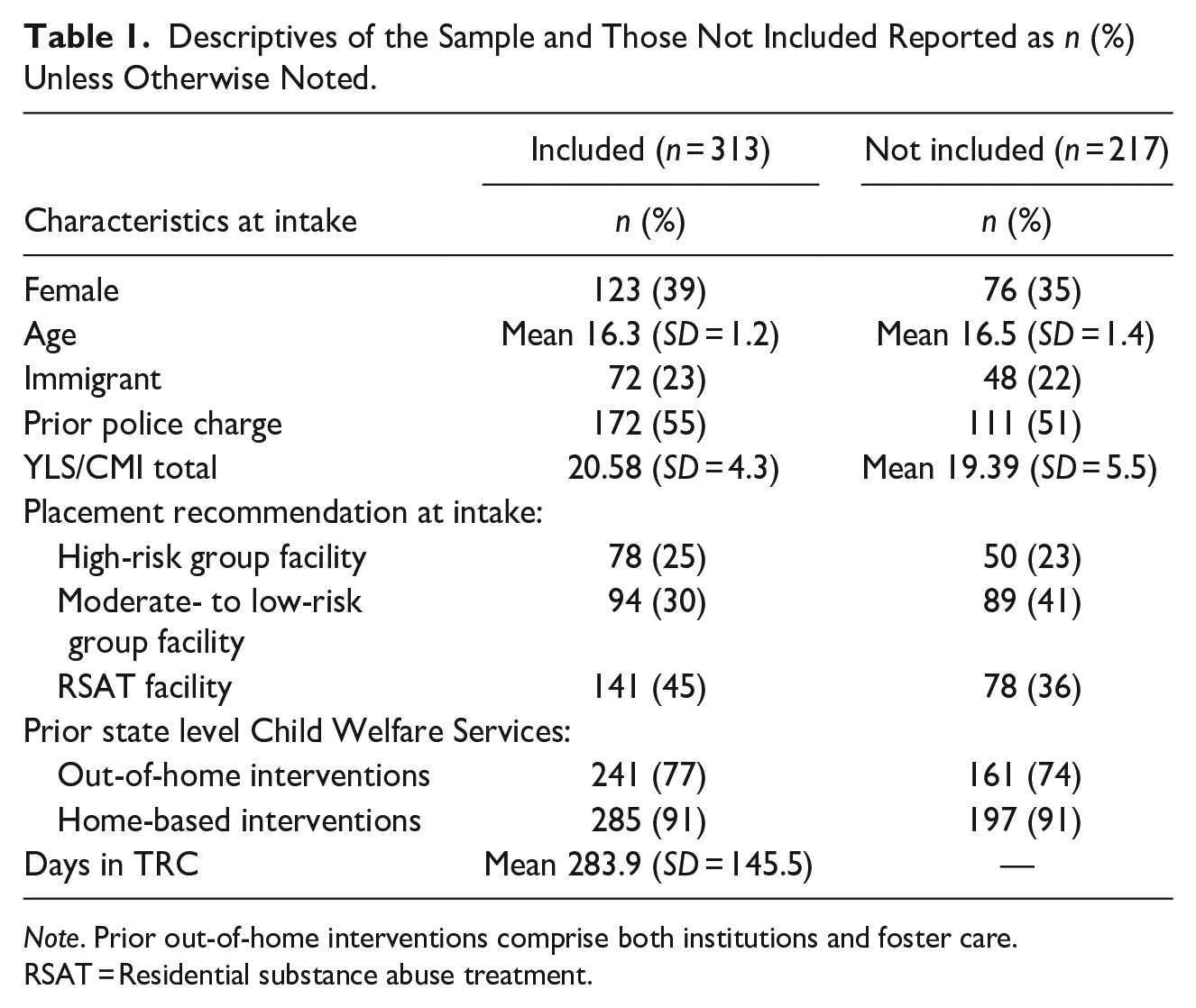
Note. Prior out-of-home interventions comprise both institutions and foster care. RSAT = Residential substance abuse treatment.
Regarding residential treatment characteristics, the mean number of days in care was 283.9 (SD = 145.5). Of the total sample, 55% received treatment in risk-matched institutions (30% in facilities for moderate- to low-risk groups, 25% in facilities for high-risk groups), and 45% were placed in RSAT institutions. Table 2 presents the change in mean risk scores from intake (T1) to the end of treatment (T2). On average, significant reductions were observed in the YLS/CMI total score and all dynamic domains. The exceptions were the Peer Relations and Substance Abuse domains in risk-matched institutions. Conversely, a mean increase was observed in the static domain pertaining to new offending behaviors during the treatment period. Notably, this domain can only remain the same or increase in score.
Mean Scores (SD) on YLS/CMI Measures at Intake (T1) and End of Treatment (T2).
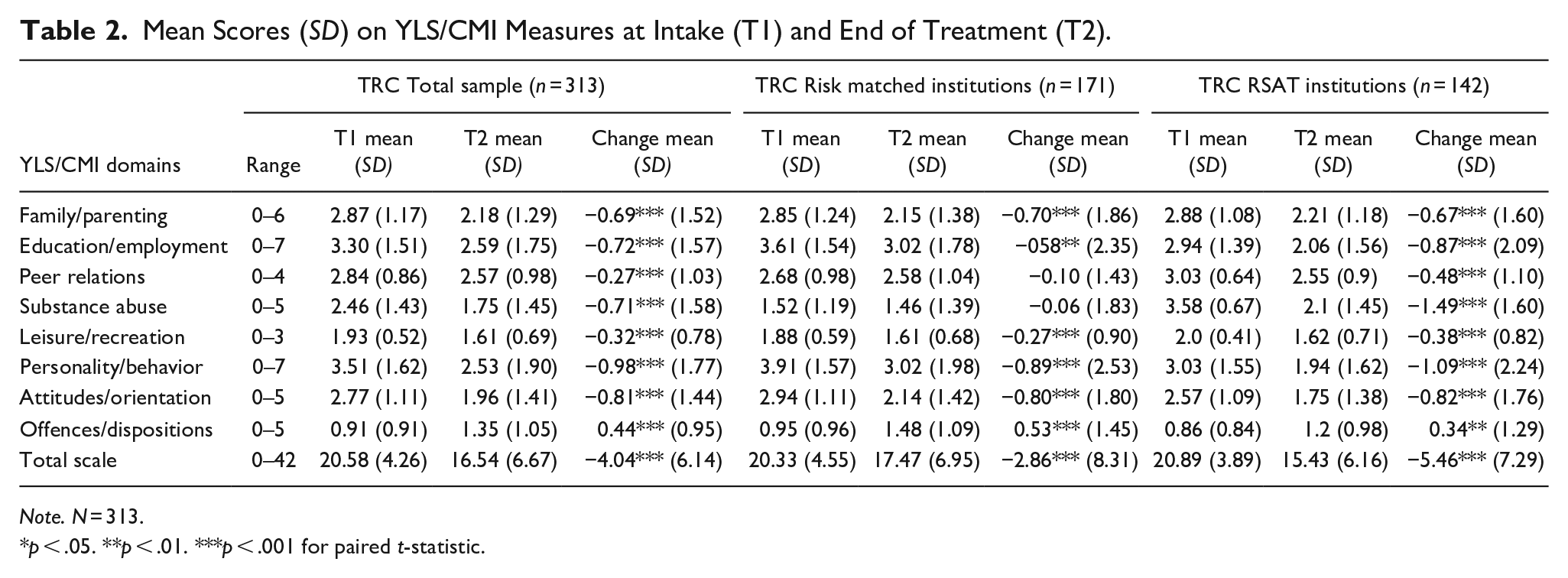
Note. N = 313.
p < .05. **p < .01. ***p < .001 for paired t-statistic.
Classification and Regression Analyses Using YLS/CMI Total Scores
To investigate the overall classification ability of the total scores, Area Under the Curve (AUC) statistics were derived from Receiver Operating Characteristic (ROC) analyses. As shown in Table 3, the YLS/CMI total score at intake was not a significant predictor. However, post-treatment and change scores yielded small to moderate effect sizes, except for the change score in the risk-matched group. The association between YLS/CMI total scores and recidivism was further examined in a series of logistic regression analyses with age, sex, and days in TRC as covariates. As presented in Table 4, the YLS/CMI total intake score displayed no significant association with recidivism, except for the risk-matched subgroup. However, the odds ratio (OR) did not remain significant after adjusting for covariates. The YLS/CMI post-treatment score was a significant predictor in all models, with unadjusted OR = 1.08 (95% CI [1.05, 1.13]) and adjusted OR = 1.08 (95% CI [1.04, 1.13]) for the total sample. Similarly, the YLS/CMI total change score significantly predicted recidivism, both adjusted and unadjusted, for the total sample (OR = 1.08, 95% CI [1.04, 1.13], OR = 1.09, 95% CI [1.04, 1.14], respectively) and across TRC types.
AUC Values for YLS/CMI Scores With 1-year Post Treatment Recidivism as Outcome.
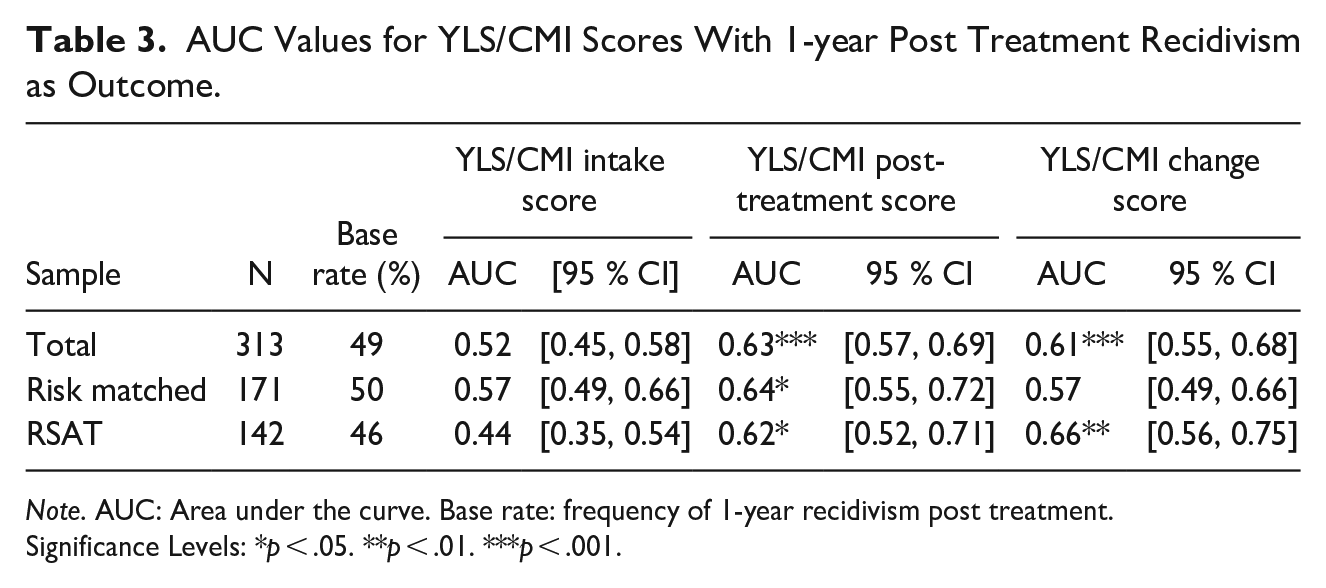
Note. AUC: Area under the curve. Base rate: frequency of 1-year recidivism post treatment.
Significance Levels: *p < .05. **p < .01. ***p < .001.
Logistic Regression Analysis With Recidivism as Dependent Variable and YLS/CMI Total Score as Covariate, Unadjusted and Adjusted for Age, Sex, and Days in TRC.
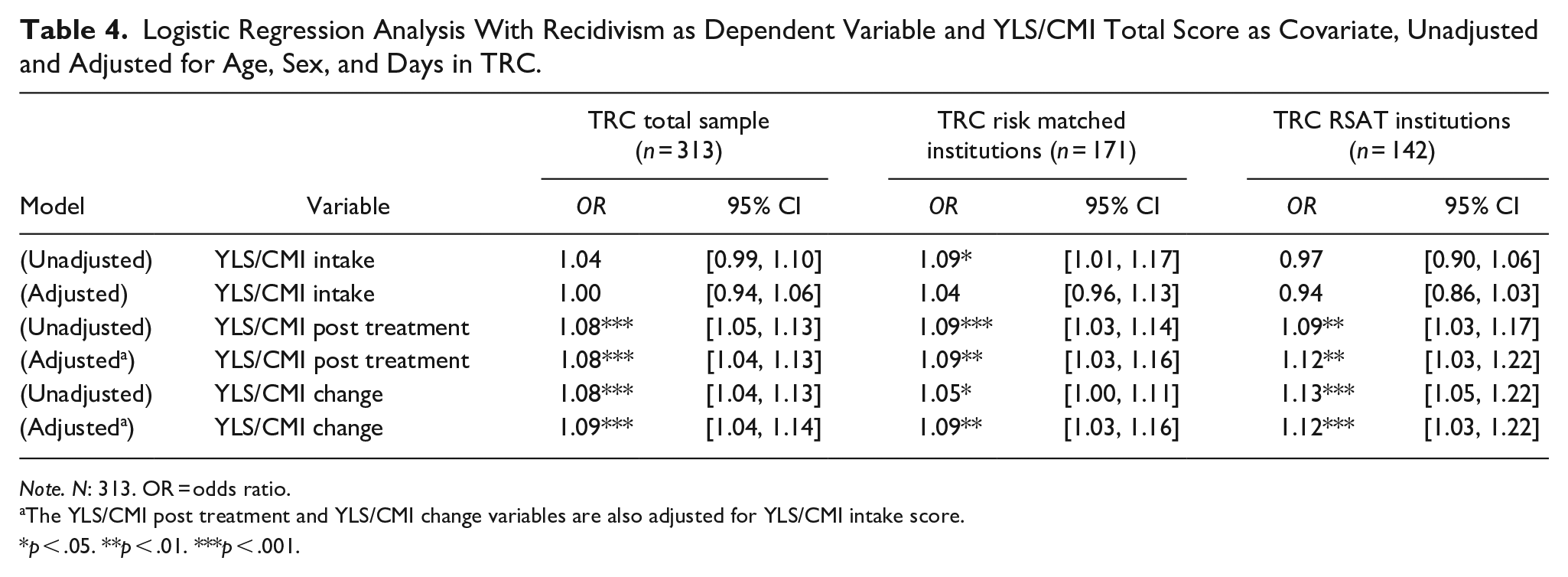
Note. N: 313. OR = odds ratio.
The YLS/CMI post treatment and YLS/CMI change variables are also adjusted for YLS/CMI intake score.
p < .05. **p < .01. ***p < .001.
Regression Analyses Using YLS/CMI Dynamic Subdomains
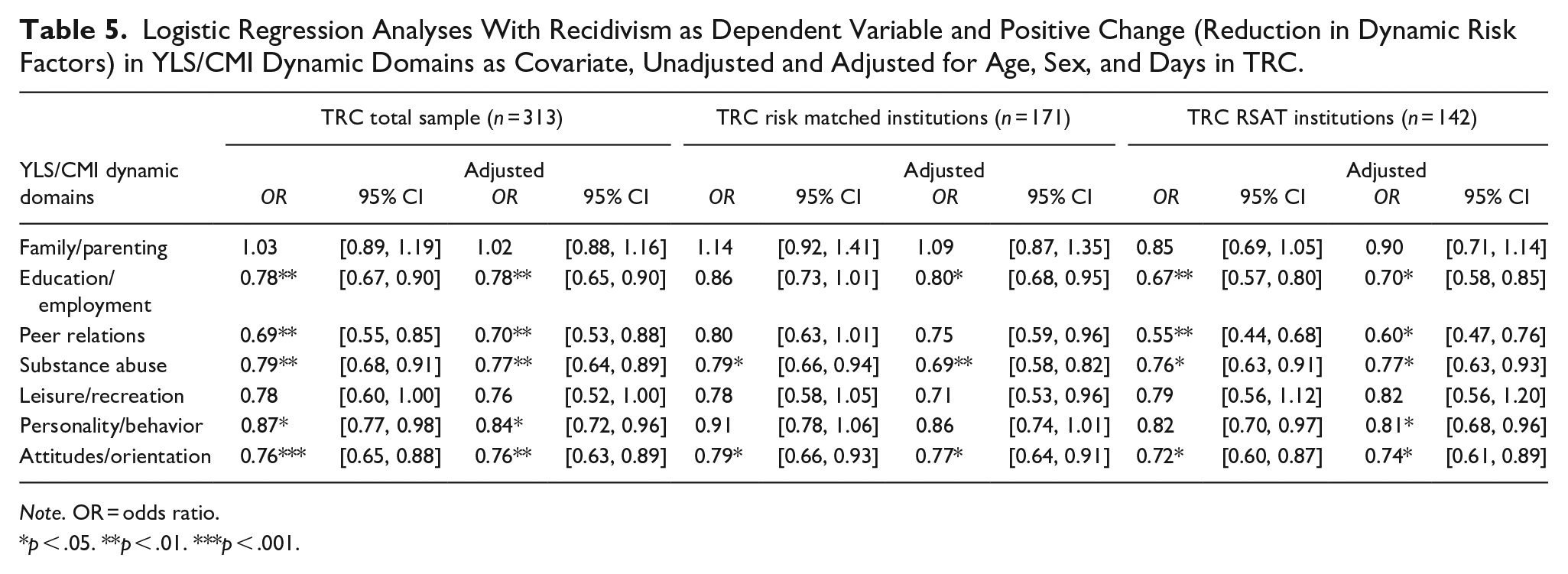
As the change scores indicated that risk factors were, on average, reduced during residential placement, an important question was whether positive treatment progress in dynamic domains led to reduced odds of recidivism after treatment. Accordingly, the impact of reduced risk factors in the dynamic subdomains was explored in a second step of logistic regression analyses. As can be seen in Table 5 for the total sample, reduced scores in five of seven dynamic domains had significant effects on recidivism. Moreover, reductions in risk scores for Education/Employment, Substance Abuse, and Attitudes/Orientation were consistently associated with significantly lower ORs across subgroups. The effects remained relatively unchanged after adjusting for the potential confounders.
Logistic Regression Analyses With Recidivism as Dependent Variable and Positive Change (Reduction in Dynamic Risk Factors) in YLS/CMI Dynamic Domains as Covariate, Unadjusted and Adjusted for Age, Sex, and Days in TRC.
Note. OR = odds ratio.
p < .05. **p < .01. ***p < .001.
Discussion
The present ’study fills a notable gap by demonstrating that risk evolves over time and that assessing changes in risk factors matters in non-secure therapeutic residential settings. Specifically, assessing treatment progress with the Youth Level of Service/Case Management Inventory (YLS/CMI) is particularly important for prediction, and reduced criminogenic needs in several dynamic domains are associated with lower odds of recidivism.
Changes in Criminogenic Risk Factors During TRC
The results demonstrate that criminogenic risk factors change in multiple areas in a young person’s life during TRC. More importantly, for most adolescents, this change represents a positive shift in behaviors, attitudes, peer relations, leisure, school functioning, substance use, and family dynamics. Nonetheless, the historic domain (offenses) significantly increased during the treatment period. This finding was anticipated, as TRC cannot physically prevent criminal behavior in the same way as secure detention, and prior research has shown that new offenses during residential placements are relatively common (Kanestrøm et al., 2024). Across the subtypes of TRCs, the greatest reductions in overall risk factors were found in RSAT placements, suggesting more impactful interventions that target criminogenic needs in these services.
Predictive Properties of YLS/CMI Intake, Post-Treatment, and Change Scores
Changes in risk factors during the residential period had a notable impact on the predictive capacity of the YLS/CMI. While the total intake score was generally not associated with charges in the year following TRC, the posttreatment, and change scores were significant predictors. This finding aligns with previous research indicating that the predictive capacity of YLS/CMI and other RNA tools may depend on the recency of the assessment (Baglivio, Wolff, Piquero, et al., 2017; Barnes et al., 2016; Clarke et al., 2017; Mulvey et al., 2016). According to the RNR perspective, this is to be anticipated, as the initial assessment before programming serves as a guide for case management and interventions toward specific areas of risk, and thus, could “expire” after treatment changes. This underscores the importance of reassessment procedures in recidivism prediction and, therefore, organizing appropriate follow-up services according to updated risk levels. Although both YLS/CMI posttreatment and change scores predicted recidivism, the AUC coefficients indicated modest effect sizes in their classification ability. This may reflect the need for a formal customization (i.e., item analysis) of the YLS/CMI inventory in Norway (Kanestrøm et al., 2024), but also the limitations of the outcome variable, as there are regional differences in case processing, investigation priorities, and clearance rates (Riksrevisjonen, 2022). Another possible explanation is the influence of factors not controlled for during the post treatment period, such as the quality and consistency of post-treatment support, reintegration, or other external influences like peer associations or family dynamics. Nonetheless, regression analyses controlling for covariates reinforces the link between dynamic risk and recidivism. Both post-treatment and change scores showed significant associations in the anticipated directions after adjusting for covariates, echoing previous studies from residential and community-based contexts (e.g., Baglivio, Wolff, Jackowski, et al., 2017; Krushas et al., 2024).
The Impact of Positive Treatment Progress
Perhaps the most compelling finding of this study was the association of positive change (i.e., reduced scores) in different dynamic risk domains with the likelihood of recidivism. In the total sample, reduced risk factors in domains such as Education/Employment, Peer Relations, Substance Abuse, Personality/Behavior, and Attitudes/Orientation were all associated with a significant decrease in the odds of a criminal charge 1 year after treatment. To illustrate, reducing a risk factor in the Attitudes/Orientation risk domain was associated with a 24% decrease in the odds of recidivism (OR = 0.76). These findings support the underlying rehabilitative assumptions of the RNR model and reinforce the idea that targeted interventions focusing on modifiable risk factors can lead to substantial improvements in behavior and long-term outcomes (Bonta & Andrews, 2017). Notably, risk reduction in the family and leisure domains remained non-significant, which suggests these are areas to explore and strengthen in all TRCs. The strongest effects in criminogenic need areas were observed in RSAT, which implies more focused interventions in these institutions. For example, reduced scores in the Peer Relations domain in the RSAT setting were associated with a notable reduction in the odds of recidivism. This might be attributed to the treatment structure addressing these relations to a greater degree due to the risk of relapse if this area is not prioritized (Griffin & Botvin, 2010; Strickland & Smith, 2014). As such, reducing affiliation with delinquent and drug-abusing friends and increasing connection with prosocial peers should also be prioritized to improve outcomes in risk-matched institutions.
Implications for Practice and Policy
As the current study employs a national sample assessed over several intake years, the findings have important implications for service provisions in Norway. The study reinforces the utility of an RNR approach in non-secure TRC settings to improve long-term prospects for these adolescents, especially regarding the risk of persistent delinquency into adulthood (Drange et al., 2022). Key priorities in the future development of these services are stepping beyond risk matching and adjusting intensity to risk level and meeting criminogenic needs with individualized treatment. Enhancing treatment fidelity by integrating Risk and Need assessment (RNA) and RNR methodology into daily practice via case management standardization and staff training could improve treatment outcomes (Baglivio, Wolff, Howell, et al., 2018; Lipsey, 2009, 2014). Likewise, this study advocates for sustaining and strengthening routine reassessment at the end of TRC placements to track progress and identify aftercare needs. Given that adolescents leaving care often engage in higher-risk behaviors such as delinquency and substance abuse than their peers (Petäjä et al., 2023), it is critical to provide comprehensive follow-up services for those with the highest assessed risk. In a meta-analytic review of aftercare programs for young offenders, James et al. (2013) emphasize the importance of well-implemented programs, individualized treatment, and prioritizing high-risk youths. Similarly, Cuevas et al. (2019) highlight the need for providing multisystemic services immediately upon release for individuals at the greatest risk, ensuring a smooth transition, continuity of care, and preventing further involvement with the justice system. As such, a shared RNR approach with collaborating agencies could ensure consistency in services and provide a more long-term perspective for treating at-risk individuals.
Strengths, Limitations, and Future Directions
Key strengths of this study were the use of a national, multiyear clinical sample from numerous institutions across all geographical regions in Norway, and the use of a validated RNA tool coupled with administrative registers for outcomes and covariates. Thus, there was no attrition, and rigorous control for multiple covariates. The sample included was comparable to those who did not complete standard TRC on key background characteristics, reducing concerns of selection bias. The non-included group represented a slightly lower-risk population at intake, likely reflecting case withdrawals and diversion to alternative home-based services in line with standard practices. Notably, the study design restricted the tracking of outcome data for the non-TRC group, as recidivism outcomes were limited to a fixed 365-day period post-treatment completion. Several other limitations should also be acknowledged. First, while results are promising, long-term follow-up studies are needed to assess the sustainability of these positive changes. Studies have shown that YLS/CMI risk scores can increase after subsequent decreases among justice-involved youth (Kitzmiller et al., 2022). Second, the reliance on criminal charge as the sole measure of offending does not fully capture the range of criminal behavior and recidivism. Future research should explore alternative measures of offending, both more liberal (e.g., self-reports, aftercare service records) and conservative (e.g., adult convictions). Third, specific aspects of institutions (e.g., adherence to case management plans) and characteristics of treatment facilities (e.g., number of residents, locations, and treatment milieu) could not be investigated. As noted within other therapeutic residential services (Harder & Knorth, 2015), much of the Norwegian TRC treatment content remain too much of a “black box”, and especially risk-matched institutions lack formal treatment models and frameworks that guide interventions. Future studies should explore the specific elements within residential care programs that most significantly contribute to risk reduction and positive outcomes. For instance, solid implementation and adherence to RNR methodology are essential (Wormith & Zidenberg, 2018), especially tailoring programs to individual risk/need to optimize intervention “dosage” and length (Baglivio, Wolff, Howell, et al., 2018; Baglivio, Wolff, Jackowski, et al., 2018). Fourth, as aftercare services are exercised by the local municipalities, the study did not control for possible interventions that the individuals received in the follow-up period. Thus, this is an important covariate that was not examined in this study and should be explored in future studies.
Conclusion
This study expands the current understanding of how dynamic risk factors relate to future involvement in the justice system and highlights the critical role of continuously monitoring these factors in therapeutic residential care (TRC). The findings demonstrate the potential for treatment programs to foster positive behavioral changes in adolescents and reduce delinquency. Moreover, this research highlights the relevance of the Risk-Need-Responsivity framework in non-secure residential settings and supports a broader integration within the Norwegian residential system and related services.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was conducted as a part of a PhD at the Norwegian University of Science and Technology, with collaboration from larger register study by The Ragnar Frisch Centre for Economic Research. The PhD study was funded by The Norwegian Directorate for Children, Youth and Family Affairs with financial support from The Research Council of Norway through the Public sector Ph.D. scheme. Grant number 327254. The register study was funded by the Norwegian research council, grant number 288813.
Ethical Approval Statement
The study was conducted in accordance with procedures approved by the Norwegian Regional Committee for Medical and Health Research Ethics (reference number 347377). Since obtaining individual consent was not feasible and any potential privacy concerns were deemed minimal compared to the anticipated societal benefits, the project was granted special authorization to deviate from standard protocols for informed consent and information disclosure. All data were securely managed on a protected platform and anonymized prior to analysis.
Data Sharing Statement
Due to the sensitivity of the data, they are not publicly available.