
Abstract
A significant number of incarcerated women experience severe and persistence mental illness. Even though a sizable body of research finds that mental health can be significantly worsened during periods of incarceration, surprisingly few studies to date have explored how incarcerated women negotiate, manage, and process their clinical diagnoses while in custody. To address this research void, the current study conducted an interpretative phenomenological analysis of (n = 15) women with mental illness incarcerated in a medium-maximum security, state prison located in the Southeastern United States. Respondents cited six themes associated with these experiences: (1) Coming to terms with a diagnosis; (2) Managing mental illness; (3) The value of communication; (4) Negative impacts of mental illness; (5) Stigmatization and labeling; and (6) Isolation. Findings are discussed with reference to policy initiatives aimed at improving the mental and physical welfare of justice-involved women.
Conditions in many correctional facilities can worsen the mental health of individuals in custody. These conditions often include coercive environments, threats of violence, inadequate staffing, and insufficient protocols for screening mental health issues (H. P. Smith, 2024). This is particularly concerning given the high percentage of incarcerated individuals with mental health conditions. For example, it is estimated that 43% of people in state prisons have been diagnosed with at least one mental health disorder (Maruschak et al., 2021). Specifically, around 23% have been diagnosed with bipolar disorder, 22% with anxiety, 14% with post-traumatic stress disorder (PTSD), and 8% with schizophrenia (Maruschak et al., 2021). These mental health conditions are often linked to past experiences of trauma, homelessness, and substance use (Maruschak et al., 2016; Semenza & Grosholz, 2019).
These challenges necessitate that correctional staff receive training and guidance on mental health issues, including programming, management, and reentry support (DeHart & Iachini, 2019; Meyer et al., 2014). The deinstitutionalization movement of the 1970s, combined with a lack of mental health resources in many communities, has resulted in correctional facilities becoming a default mental health system, despite not being adequately equipped for this role (Peternelj-Taylor, 2008; Steadman et al., 1984; H. P.Smith, 2024).
While mental health conditions are common among all individuals in correctional facilities, women in custody experience disproportionately higher rates of mental health challenges compared to men. For instance, 69% of women in state prisons report a history of mental health issues, compared to 41% of men (Maruschak et al., 2021). In federal prisons, 52% of women report a history of mental health problems, compared to 21% of men (Maruschak et al., 2021). These statistics are influenced by various factors such as demographics (e.g., gender, age, race, education), cultural influences (e.g., stigma, community expectations), and access to resources. It is evident that mental health remains a significant concern for incarcerated women.
Women also experience unique ways of identifying, processing, and coping with mental health conditions (King & Smith, 2023). Their mental health challenges are often linked to extensive experiences of victimization, which can lead to severe trauma and substance use (King & Smith, 2023). These factors impact other areas of life specific to women, such as gynecological care (Binswanger et al., 2011; Nijhawan et al., 2010; Sirovich & Welch, 2004), breast cancer screening (Pickett et al., 2018), and motherhood (Glaze & Maruschak, 2010). Incarcerated women often navigate complex processes of mental health diagnosis, which involve negotiating their understanding of symptoms and seeking appropriate care (Bronson & Berzofsky, 2017). The management of these conditions is further complicated by the prison environment, which can exacerbate mental health issues due to isolation and lack of support (Johnson & Thompson, 2023). Effective interventions must consider these unique challenges and provide tailored support to address the specific needs of incarcerated women (Messina & Zwart, 2021).
Research on women in the correctional system has highlighted the critical role of mental health. For example, Chesney-Lind (1997) noted that incarcerated girls and women often face victimization, various physical and mental health issues, and substance use problems that intersect with criminal behavior. This has been supported by Miller (1987), Daly (1992), and Richie (1995), who found that women have different pathways to crime compared to men, with mental health being a common factor. Daly (1992) identified five pathways to crime for women: self-harm, experiences of battering, street life, drug connections, and patterns of “othering.” Key factors leading to mental health issues in incarcerated women include childhood neglect, sexual assault, and interpersonal violence (Daly, 1992; DeHart, 2004, 2008; Green et al., 2016; Kennedy et al., 2015). Brennan et al. (2012) categorized the most persistent mental health issues among incarcerated women as those related to abuse and antisocial behavior, and those related to marginalization, abuse, addiction, psychosis, and suicidal risks.
Despite the high prevalence of mental health challenges among incarcerated women, there is limited research on their lived experiences with these conditions during imprisonment. Most studies rely on surveys, secondary institutional data, and standardized psychological assessments (Drapalski et al., 2009; Houser & Belenko, 2015; Houser & Welsh, 2014; Lord, 2008; Wolff et al., 2013), which do not provide a direct voice to the participants. To address this gap, the current study uses interpretative phenomenological analysis (IPA) to explore the experiences of incarcerated women in a medium-maximum security prison in the Southeastern United States. The goal is to understand how these women manage their mental health while in custody, with the aim of informing policies to improve mental health support for incarcerated women.
Interpretive Phenomenological Analysis of Mental Illness
Phenomenology was originally developed by Husserl (1931) as a means of interpreting the experiences of individuals from their own perspective, rather than applying one’s own preconceived notions. Within phenomenology, the researcher sets aside (or minimizes) their assumptions, and instead allows the individual experiencing the phenomena to voice their perceptions on it. Interested in existential philosophy, phenomenology was extended by Heidegger (1962) with the addition of hermeneutics. Within hermeneutics, one can interpret the language used by a person as well as their frame of mind regarding the experiences of their lives (Freeman, 2008). In general, phenomenology aims to understand the world of the persons being studied, which consists of their experiences and how they process them (J. A. Smith, 1996; J. A. Smith et al., 1999). Interpretative phenomenological analysis (IPA) as a method allows for a deeper and more critical analysis of a topic, particularly in unique settings where complexity emerges (J. A. Smith, 1996, 2004).
Phenomenology has received significant academic attention in the examination of mental illness occurring outside of the criminal justice system. Here, scholars have been able to gain insight into the self-perceptions of individuals who have been diagnosed with mental illnesses (Powell et al., 2014; Spodenkiewicz et al., 2013; Sutherland et al., 2014; Waite et al., 2015), their mental illness in relation to others (Ko et al., 2014; McCann et al., 2012; Mjøsund et al., 2015; Wills & Hons, 2012), and the effects of stigma on those with mental health diagnoses (de Wet et al., 2015; Knight et al., 2003). Negative self-perceptions appear to be a common theme in this research (Brooke & Horn, 2010).
A subset of these studies has focused exclusively on samples of women. Powell et al. (2014) purposively selected their sample based on a self-disgust scale given to women. The following four themes were identified: (1) The subjective experience of mental illness; (2) The origins of the revolting self; (3) The consequences of self-disgust, and finally, (4) The associated emotional state (Powell et al., 2014). Likewise, Knight et al. (2003) conducted an IPA on women with schizophrenia and identified themes of judgment, comparison, and personal understanding of mental illness. Stigma was apparent both in public and self-domains. Spodenkiewicz et al. (2013) used IPA to explore a sample of adolescents with borderline personality disorder and found the following four themes of emotional experiences (i.e., fear, sadness and pessimism), interpersonal relationships (i.e., solitude and hostility from others), a conformist self-image (i.e., normality and difficulty in projecting into time), and a structuring of discourse characterized by discontinuity. Girls comprised 88% of the sample and connected the meaning of mental illness to a negative self-image that increased distress and hindered care-seeking behaviors (Spodenkiewicz et al., 2013).
IPA investigations of mental illness also reveal positive themes. Sutherland et al. (2014) examined online posts of people who engaged in self-injurious behaviors and found the following themes: self-kindness, common humanity, and mindfulness. An IPA assessment of depression in female adolescents found three inter-connected super-ordinate themes which were communication, hurt self, and difference (Shaw et al., 2009). These perspectives centered on shifts in identity, with communication to family and peers providing a sense of damage, distress, and hurt. The authors suggested that attachment theory represented a suitable framework for understanding this sample of females with mental illness (Shaw et al., 2009). Taken together, the employment of IPA to examine mental illness in women routinely finds negotiation with identity, alienation or belonging, and stigma as overriding findings. While there is far less research on these topics for justice-involved women, it is likely that they would be even more salient in this context, and thus in need of greater empirical exploration.
Phenomenology, Incarcerated Women, and Mental Illness
While mental health conditions are common among all individuals in correctional facilities, women in custody experience disproportionately higher rates of mental health challenges compared to men. For instance, 69% of women in state prisons report a history of mental health issues, compared to 41% of men (Maruschak et al., 2021). In federal prisons, 52% of women report a history of mental health problems, compared to 21% of men (Maruschak et al., 2021). These statistics are influenced by various factors such as demographics (e.g., gender, age, race, education), cultural influences (e.g., stigma, community expectations), and access to resources. It is evident that mental health remains a significant concern for incarcerated women.
Women also experience unique ways of identifying, processing, and coping with mental health conditions (King & Smith, 2023). Their mental health challenges are often linked to extensive experiences of victimization, which can lead to severe trauma and substance use (King & Smith, 2023). These factors impact other areas of life specific to women, such as gynecological care (Binswanger et al., 2011; Nijhawan et al., 2010; Sirovich & Welch, 2004), breast cancer screening (Pickett et al., 2018), and motherhood (Glaze & Maruschak, 2010).
Research on women in the correctional system has highlighted the critical role of mental health. For example, Chesney-Lind (1997) noted that incarcerated girls and women often face victimization, various physical and mental health issues, and substance use problems that intersect with criminal behavior. This has been supported by Miller (1987), Daly (1992), and Richie (1995), who found that women have different pathways to crime compared to men, with mental health being a common factor. Daly (1992) identified five pathways to crime for women: self-harm, experiences of battering, street life, drug connections, and patterns of “othering.” Key factors leading to mental health issues in incarcerated women include childhood neglect, sexual assault, and interpersonal violence (Daly, 1992; DeHart, 2004, 2008; Green et al., 2016; Kennedy et al., 2015). Brennan et al. (2012) categorized the most persistent mental health issues among incarcerated women as those related to abuse and antisocial behavior, and those related to marginalization, abuse, addiction, psychosis, and suicidal risks.
Despite the high prevalence of mental health challenges among incarcerated women, there is limited research on their lived experiences with these conditions during imprisonment. Most studies rely on surveys, secondary institutional data, and standardized psychological assessments (Drapalski et al., 2009; Houser & Belenko, 2015; Houser & Webb, 2014; Lord, 2008; Wolff et al., 2013), which do not provide a direct voice to the participants. To address this gap, the current study uses interpretative phenomenological analysis (IPA) to explore the experiences of incarcerated women in a medium-maximum security prison in the Southeastern United States. The goal is to understand how these women manage their mental health while in custody, with the aim of informing policies to improve mental health support for incarcerated women.
Method
Sample
Interpretative phenomenological analysis (IPA) involves the collection of data from a homogeneous, purposive sample (J. A. Smith & Osborne, 2008). J. A. Smith (2011) argues that IPA investigations should feature sample sizes of eight or more to meet saturation of themes and understand topics more comprehensively. In accordance with this suggestion, the current study includes (n = 15) women recruited from a medium-maximum security, state-operated prison located in the Southeastern United States. Permission to pursue this study was granted by members of a human subjects review board, along with administrative officials of the host Department of Corrections. The following eligibility criteria were used to recruit respondents: (1) Participants must have been women incarcerated in a state prison; (2) They must have been diagnosed with a mental health disorder, and (3) They must have been willing to communicate personal details of their experiences with mental illness while in custody. Table 1 provides a demographic breakdown of the sample where it will be seen that an overwhelming majority were Black (10/15; 66.6%), and under the age of 40 (73.3%).
Sample Demographics.
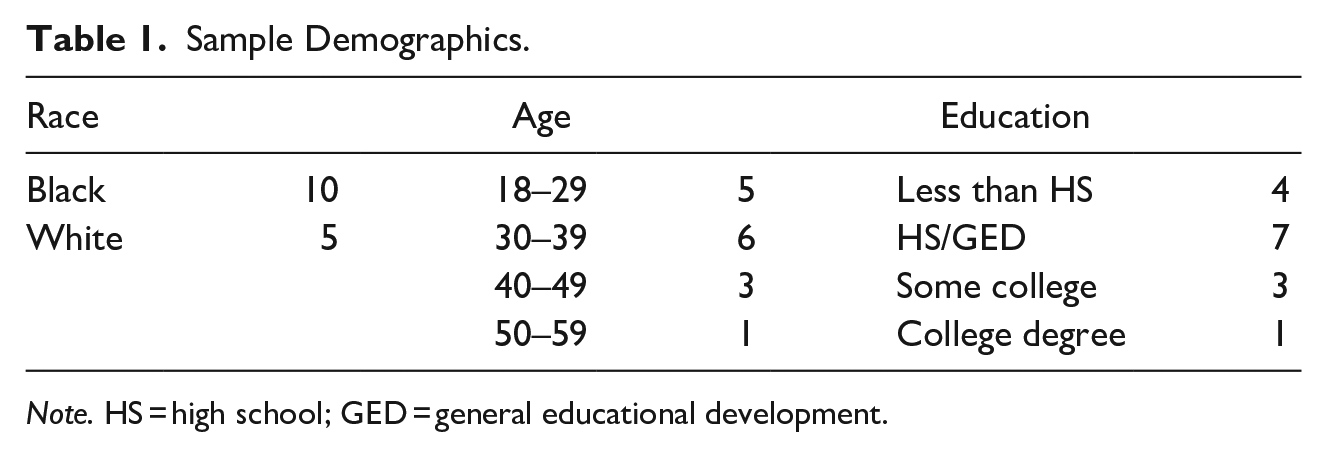
Note. HS = high school; GED = general educational development.
Mental health professionals working in the prison of study took the lead in recruitment. This afforded mental health staff the opportunity to refer potential participants most relevant to the proposed topics, with a focus on potential participants who would engage in dialogue with researchers. It also allowed participants the opportunity to engage with a treatment professional should any adverse events occur. Prospective sample members were notified that researchers would be visiting the prison to conduct voluntary and confidential interviews regarding their experiences with mental illness while serving time in custody. Anyone interested in participating was informed of the scheduled visit date. To uphold respondent safety, security, and privacy, they were asked to communicate their willingness to be interviewed directly to the research team when they arrived on-site. This protocol includes signing a consent form, with reinforcement that engagement in the research was voluntary and that participants could stop at any time. Every interview was held in a private room outside the presence of staff, and was audio-recorded and later transcribed, both with respondent signed permission, to accurately document their statements. Data were collected during the summer of 2022, with each interview lasting between 30 minutes-3 hours in length.
Interview Guide and Data Analysis
Three questions borrowed by Sierka’s (2015) IPA were posed to our sample, and they included: “What have your experiences been with mental illness while in this prison,” “How have you processed and managed your mental illness during your time in custody,” and “can you offer any other insight concerning your experiences with mental illness while in this prison?” Follow up questions were generated in relation to the perspectives offered by participants. These questions were asked while participants completed a life history calendar (LHC) with one researcher. The LHC design consists of a calendar-type grid, with time units and life events in either the columns or the rows (DeHart & Moran, 2015). LHCs aid participants in recalling life events by providing visual and temporal cues, with memorable events recorded first, followed by less salient events that may require explanation (Freedman et al., 1988). During interviews, the interviewer filled in the grids of the calendar, which provided a visual cue to participants in recalling past events (Peterson et al., 2014; Roberts & Wells, 2010; V. C. Smith, 2017). Due to complex lives where trauma, criminal behavior, mental illness, substance abuse, and incarceration intersect, the LHC can serve as an effective timeline to properly document the order of these experiences. During data collection, the researcher collected written notes on responses, including salient life events.
The interviews were analyzed using interpretative phenomenological analysis (IPA), a methodological approach used to obtain rich, meaningful data (Larkin et al., 2006; J. A. Smith, 1996, 2004, 2011; J. A. Smith & Osborne, 2008). IPA is an inductive, idiographic approach to investigating lived experiences, moving beyond a review of social processes toward exploration of meaning. The transcribed qualitative interviews were entered into NVivo, and techniques suggested by J. A. Smith et al. (2009) were applied to analysis. Specifically, these techniques first involved using inductive reasoning to carefully inspect the transcripts to identify interrelationships between them. To enhance inter-rater reliability, every answer provided was independently evaluated by all members of the research team to see if similar conclusions were drawn about the meaning of the data. This process involved familiarization with the transcripts by reading them multiple times, and then creating initial codes (J. A. Smith et al., 2009). Afterward, focused coding procedures followed in which key concepts, or themes, were identified (J. A. Smith et al., 2009). Cases were entered and analyzed while looking for a saturation point, which occurs when nothing new is being gained from a sample (Ravitch & Carl, 2016).
A note on both positionality and reflexivity is in order. Positionality, described as an “individual’s worldview. . .towards a research task” (Hesse-Biber & Leavy, 2011, p. 11), can sometimes bias the analysis of qualitative data. Mainly this is because the researcher applies their own worldview to the findings. Reflexivity, defined as the practice of acknowledging biases and finding ways to overcome them, must be pursued by those analyzing qualitative forms of data (Meyer & Willis, 2019). Beginning at data collection, a number of different reflexive approaches were adopted to avoid biasing interpretation of the transcripts. First, the research team established rapport with respondents to gain their trust. The research team did this by communicating the intentions of this project, which were to improve respondent health. Second, and in fully recognizing that as outsiders to the prison context, the research team is in a position of learning, we deferred to the expertise of study participants. They were the ones who possessed the knowledge we were seeking, and thus our fundamental priority was to privilege their voices. Research staff therefore approached the entire study with an inquisitive mindset to learn from participants. Finally, and during the analytical phase, the research team, who all have extensive backgrounds in qualitative research, applied objectivity to the interpretation of the data.
Results
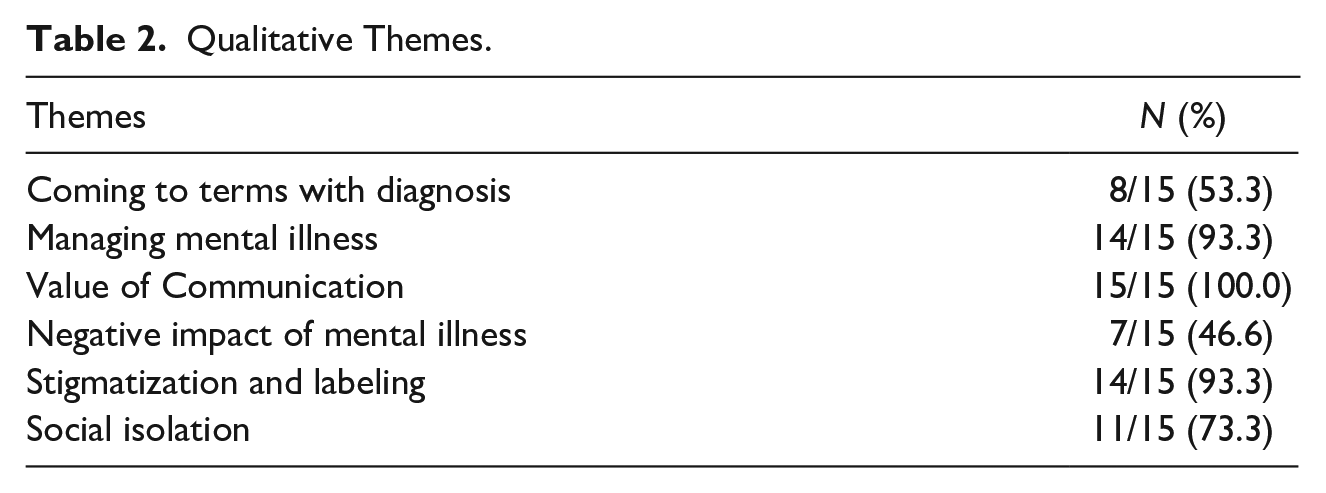
The interpretative phenomenological analysis produced the following six super-ordinate themes: (1) Coming to terms with a diagnosis; (2) Managing mental illness; (3) The value of communication; (4) Negative impact of mental illness; (5) Stigmatization and labeling; and finally, (6) Social isolation. Each theme provided insight in how participants felt about having a mental illness over their life course, including during their time while in custody. To preserve respondent confidentiality, after citing a quotation of theirs, it is labeled with the following identifier (R#). Table 2 provides a summary of these qualitative themes followed by key examples.
Qualitative Themes.
Super-Ordinate Theme 1: Coming to Terms with a Diagnosis
Eight participants expressed “coming to terms” with their mental illness, though only one explicitly stated “accepting” the diagnosis. For others, coming to terms meant cognitively framing mental illness as normal.
Sub-ordinate theme 1A: Acceptance
Six participants expressed acceptance of their diagnosis by acknowledging that they are facing a potentially lifelong illness. These individuals specifically came to terms with requiring medication, “answers” to a diagnosis, and that because their mental illness cannot be changed, they should not fault themselves for it. While participants still struggled with acceptance, these factors provided a sense of relief, as seen here: I think medicine is better in me. . .and I think for the long run I think I’m [going to] have to be on this for the rest of my life because it settles me. It calms me down. (R15) It’s helpful for me because I know, like I said, now that I know what’s wrong, I know how to handle it, how to deal with it. . .so if anything it, it helps knowing than me not knowing, so I’m okay with it. (R13) I hate it. I hate it but I can't change it. I just accept it. (R10)
Sub-ordinate theme 1B: Normalization
For six participants, having a mental illness was expressed as being “normal.” Two in particular believed that the normalization process surrounding mental illness increased during incarceration, particularly when they interacted with other incarcerated women who had similar illnesses. This took place in prison settings where mental illness was ubiquitous, as documented in the following accounts: I just feel like it’s normal. . .It’s a normal part of life. . . I have not felt like I was normal until I came here at this institution and have been placed with people that experience the same thing. (R4) I feel like it’s normal. . . I think everybody’s got some kind of crazy in them. In prison, its just the way it is and that’s ok. We talk to other women, and it makes you think about us all being the same. (R9)
Super-Ordinate Theme 2: Managing Mental Illness
A total of 14 participants described ongoing challenges with managing their mental illness. This appeared to be bifurcated with some participants attempting to “control” their symptoms, while others using avoidance techniques.
Sub-ordinate theme 2A: It’s a battle
Managing the symptoms of mental illness resulted in participants commonly using war terminology, such as “battle,” “fight,” and “warfare.” This revealed a fluctuating state with “good days and bad days.” A typical statement reflective of this included: I don’t know if my mind just be playing tricks on me, but I know like some people follow all the way through what their mind be saying, but I don’t, like I don’t know, I just be praying about it. It’s just a battle. (R12)
A failure to adequately manage symptoms not only had a profound impact on participant mental health, particularly mood, behaviors, and perceptions, but also elevated their risk for violence and physical illness. For example, one participant stated that due to the diagnosis of antisocial personality disorder, violent reactions to low emotional states were problematic. This particular respondent explained that when attempting to prevent violent outbursts, her legs would start to tremble, resulting in the following statement: “I’ll just let people know—you have no idea how difficult it is for me right now to not hurt someone.” (R2)
Sub-ordinate theme 2B: Control
Nine sample members described a reliance on control to address symptoms of mental illness. This included prevention strategies and avoidance of triggers such as recollections of traumatizing birthdays and anniversaries that could instigate depressive symptoms, as explained in the following quotation: I learned all I could about it [mental illness], and I tried to beat it before it hit. . .by the time it hit me, I was okay. Being locked up, and there are events [going on outside prison] is hard. (R14)
Another expressed concern related to decision-making. In regards to this, one participant diagnosed with schizophrenia explained how she tries to control her auditory hallucinations because she does not want to make decisions based on what is being heard in her mind. She implied that positive thoughts would result in positive auditory hallucinations that would help keep her from making poor choices, stating the following with respect to this: I try to think positive. . .I try not to listen to the voices. (R8)
Sub-ordinate theme 2C: Distraction
Eight sample members described their continued effort to stay busy as a means of distracting themselves from their symptoms. This was particularly salient when avoiding repeated, invasive thoughts, which is evident in the following accounts: I find whatever I have to. If it’s cleaning or walking whatever needs to be done at that moment. . .to make me get through the situation. Just keep moving. (R4) I make myself get out of the bed and I throw myself into my job. I make sure my whole day is filled up. (R10) Give me anything to do with keep my thoughts from just being there. Still to no avail. Still nothing to do. I sit on the dorm all day every day to my thoughts. If we go into lockdown then I am stuck. Just me and my nonstop thoughts. (R7)
Super-Ordinate Theme 3: The Value of Communication
Every participant interviewed emphasized the value of communication as being central to coping. For all 15, it was crucial they have someone to talk to about their feelings. Not only did this dialogue offer utility for coping with mental illness in prison, but it provided a sense of humanity as the person was being recognized as present and real. Participants did differ regarding their preferred communication point, with some relying on other incarcerated women, while others prioritized dialogue with licensed counselors working in the prison.
Sub-ordinate theme 3A: Feeling heard
Eight women in this study described having someone that they could confide in to “feel heard.” These participants found therapeutic value in having the opportunity to express themselves to those they trust. One participant stated that having someone to talk to helps you “get it out your system” (R3). There was a tendency to express emotional states, while not necessarily requesting nor expecting tangible solutions in response, as evidenced by the following statements: You have to have that outlet, so that’s why I said the counseling would probably be a big thing for me, and it’s having somebody to talk to that I can confide in. Someone that won’t judge me and they will just listen. (R13) I’ve never not had anybody to talk to. . . if I needed somebody to talk to, I find them. You have to have someone to talk to or you can get really sick. (R14) And I like talking so. . .somebody said ‘you need to just go ahead and be a mentor or something so you can, you love to talk to people.’ So, I listen to other inmates with mental illness now. I don’t stop them, I just listen. (R15)
Sub-ordinate theme 3B: Feeling unheard
For seven respondents, there were struggles in connecting with a mental health professional in the prison, and a sense of frustration and fear stemming from feelings of being ignored. For these sample members, they linked this emotional state to previous trauma, such as sexual victimization during childhood and/or adolescence. Feeling unheard was also linked to psychotropic medications as these accounts suggest: Like the medication will help a lot of stuff but then there’s just so much left over that I can’t seem to get help with. I might need another medication or someone to talk to more. I don’t know. (R2) Taking medication. . .That’s about all I get, cause trying to talk to a counselor here in prison is like pulling teeth. I don’t feel like to get some attention, that I need to tell somebody, ‘I’m going to hurt myself’, just for somebody to talk to me about what is wrong. As an adult, I know when I don’t feel right or out of sync or off kilter cause of my mental illness, so if I’m coming to you please don’t ignore me. (R1)
Super-Ordinate Theme 4: Negative Impact of Mental Illness
Sub-ordinate theme 4A: Anger and rage
Seven participants identified a link between mental illness symptoms and dysfunctional interpersonal relationships. This revolved around feelings of rage, which can be seen in the following accounts: My mental status a lot to do with my anger and rage. . .I’m an assaultive inmate because I’ve been in so many fights. You can check my sheet, my mental illness acts up, and I get angry, and I fight. (R6) It gets me in trouble. Gets me in a lot of trouble. . .I just get so mad, so angry, and I just start thinking about everything that’s going on with me and I just lash out and just take it out on whoever is around me. (R3)
Sub-ordinate theme 4B: Criminogenic behaviors
Seven women in this study felt that their mental illness had a role in their criminal activity that ultimately led to their incarceration. For one participant, the connection was from not taking antipsychotic medication. For other participants, their mental illness negatively impacted their decision-making: Because of what I’ve done this time. . .I was having paranoia schizophrenia. I could not stop it. (R8) I know and I think that if I had medication when I was on the street. . .my actions would have been different. I wouldn’t have been quick to do things that I was just doing out of boredom or felt like I had to do. . .And I probably would’ve coped with whatever I had going on more better if I was on medicine. . . I probably wouldn’t be here now. (R15) In a way I probably wouldn’t have made the decision with them people that night, if. . .I wasn’t dealing with mental illness. (R11)
Sub-ordinate theme 4C: Victimization
Six of the participants used the lens of mental illness to explain criminal behavior in people close to them, especially in cases where the participant was victimized. One participant stated that people with mental illness “don’t think about others,” because she did not care about the feelings of others before she was incarcerated, and that violence in prison was often the result of untreated mental illness. Another participant expressed that bipolar disorder was the explanation for her mom’s violent demeanor and abusive actions: She had a lot of anger, like violence, because of her illness. Yeah, she had an extremely bad temper. I will put it that way. As children, we were on the receiving end of that mental illness. (R6)
According to another participant, mental illness could help explain why her brothers sexually abused her during her childhood and adolescence: I would assume that it was an issue of mental health for my brothers to start molesting me. And that doesn’t seem like it would be like normal thinking. (R2)
Super-Ordinate 5: Stigmatization and Labeling
Almost the entire sample, 14/15 respondents, were acutely aware of the stigma associated with their mental illness. These participants felt different from others, thought they were the target of derision, and as such, were quick to reject stereotypical labels commonly attached to those with mental health impairments. Shame of having a mental illness was also acknowledged.
Sub-ordinate theme 5A: Awareness the stigma
Participants routinely expressed awareness of the stigmatization of having a mental illness. Stigmatization was present from early childhood and reified by a positive diagnosis. These views can be seen here: I wouldn’t get on medicine because in my mind, the only kids at school on medicine were kids that were crazy, so I didn’t want to be seen as a crazy kid. (R13) You get a 20-year sentence, you might be on medication, too! (R14)
Four participants described instances where they considered the stigma of having a mental illness. For one in particular, minimizing the views of others was an effective strategy, as she said, “I don’t let it define me as much as I used to. They can think whatever they want” (R8). Other participants negotiated stigma by finding nuances in terms, for example: I’m not crazy, I may be mentally ill, but I’m not crazy by any stretch of the imagination. (R1)
Sub-ordinate theme 5B: Negative labeling
Eleven participants had been negatively labeled as having a “mental illness,” or heard of other individuals with similar mental health problems being pejoratively stigmatized because of their condition. Oftentimes, they were referred to as “slow,” “sick,” “crazy” as well as being told “you aren’t all there” and “something is wrong with you.” One participant experienced this labeling from a mental health counselor after her suicide attempt during adolescence, which is described in the following account: She would say. . . ‘do you realize you tried to kill yourself and only crazy people kill yourself, try to kill they self. . .what’s wrong with you?’ (R14)
Several participants stated that they experienced individuals close to them labeling them, but they stressed a key difference when that person was being serious instead of lighthearted. One participant acknowledged being called “crazy” in a “playful way.” This is also evident in the account by the other participant: I mean, when you’re, not meaning, it’s one thing if we’re joke. . .laughing and talking, but it’s different ways of saying. Your inflection on how you’re saying it. We joke around in prison, but you tell what a person means when they say things. (R1)
Rejection of the negative labeling also involved distinguishing the diagnosis from factors like being a good person or being intelligent, as documented in these accounts: They even say ‘even though she’s bipolar and crazy. . .deep down she’s, she’s good people, she’s sweet, she’ll do anything for you.’ (R12) I’m mentally ill, not stupid. . .I’m mentally, I have a mental illness. I’m not stupid. I’m smart, I am mentally ill, but I can say I’m smart. (R8)
Sub-ordinate theme 5C: Shame
Six participants experienced shame with their mental health diagnosis. After chronicling an extensive list of mental health conditions, one participant said they make her sound like “a hot mess” (R1). Other participants stated: Sometimes I feel ashamed, I feel like I’m not normal. (R8) I think the time before the medication I was embarrassed to say that I needed it because I felt that I was a strong person that I could do it on my own. But after talking to my mental health counselor, she let me know that it might be a slight chemical imbalance. She will say, “it’s not your fault. It’s nothing to be ashamed of.” Once she told me that, I felt okay about it. I’m okay with it, you know. It’s nothing that I’ve done wrong to get the mental illness. (R14)
Super-Ordinate Theme 6: Social Isolation
Eleven participants socially isolated from others while incarcerated. This isolation served multiple purposes, and these participants were confident that isolation represented an effective coping mechanism.
Sub-ordinate theme 6A: Withdrawing and being alone
Eight individuals included in this study described themselves as loners, or as not wanting to interact with others. In some cases, this worked as a short-term response to mental health symptoms, with the use of “hibernation” or “anti-social sleep” to cope. Their accounts can be seen here: I feel like I’m pulled on a little and sometimes I just don’t feel like being bothered. I just stay in bed all day, or I go hibernate in my cell for a while. (R14) I stay to myself, I don’t bother people, and when I shut down just leave me alone. That is a sign that I need to be alone. (R15)
Three in particular expressed no desire to interact with others because they are more comfortable by themselves. This extended to more long-term approaches of defining oneself as a “loner” or “outcast.” This is evident in the following account: I’m much more comfortable being alone. And it just works better for me. I tried it and it works. Now as I can see where my little circle is very small, but that is the best thing for me. I am more a loner than not. (R1)
Sub-ordinate theme 6B: A protective measure
For six participants, social isolation offered a means by which to protect themselves from psychological harm while incarcerated. These accounts tended to reflect the prison environment, or at minimum, criminogenic peers as shown here: If I had my choice. My best company would be myself, it’s safe. I’m not going to let myself down. People in prison will let you down when you are mentally ill. I want to get out of here, I need to stick to myself. (R1) Hanging out with people is what got me here. I didn’t commit my crime, but you know, the hand of one is the hand of all
1
and when you do something here it’s the same way. You get punished for what others did. With my mental illness I can’t have that happen again. (R11) There’s groups, like counselling groups you can go to, but those are full of inmates. And then they’ll know my vulnerabilities and I have to be here forever. I got a life sentence; I need to protect myself and my illness from others. (R2)
Discussion
The women in this study who are incarcerated and living with mental health conditions provided insights that can be categorized into six main themes: coming to terms with a diagnosis (i.e., acceptance, normalization), managing mental illness (i.e., “it’s a battle”), the value of communication (i.e., feeling heard), negative impacts of mental illness (i.e., criminogenic behavior), stigmatization and labeling (i.e., awareness of stigma), and social isolation (i.e., withdrawing). The IPA revealed several negative concepts that were also present in the literature on women with mental health conditions who were not incarcerated, such as stigma, labeling, and normalization. This suggests that mental health conditions generally involve a struggle to find meaning, apply and accept labels, and address damaged self-assessments, particularly disgust (Powell et al., 2014), pessimism (Spodenkiewicz et al., 2013), and a disrupted sense of self (Sierka, 2015). For the women in this study, these issues were lifelong, beginning in abusive and traumatic childhoods and extending into deviant peer groups and eventual incarceration.
Many of these women felt their mental health conditions were normalized when they were incarcerated with others who had similar experiences. This shared environment provided a sense of commonality and understanding, reducing feelings of isolation and stigma (Johnson & Thompson, 2023). The normalization of mental health conditions in this context highlights the importance of peer support and shared experiences in managing mental health within the prison system.
In contrast to previous studies, there was a lack of positive support structures in place for these incarcerated women with mental health conditions. For example, Sutherland et al. (2014) found self-kindness, empathy, self-care, and other beneficial themes in their IPA. This sample did not report this perspective; instead, they relied on an individual “pull yourself up by your bootstraps” approach to address mental health conditions. This strategy appeared to be a result of a lack of trusting and supportive relationships extending from parents and peers to government workers (i.e., teachers, police, court personnel, etc.), a mistrust of authority and support structures, and barriers to care. More research is needed to better understand if racial and ethnic cultural considerations also influence decisions to seek care or access institutional treatment, including resources in the community prior to incarceration. However, it is apparent that for a subset of these women, the effort toward individual (non-supportive or non-group) efforts at addressing their mental health conditions placed them at risk for emotional detachment.
Even within a state prison population, these women used isolation, withdrawal, and loner behaviors as a protective device when experiencing mental health conditions. Policy interventions would benefit from accessing this at-risk population and providing therapeutic and social support structures in line with the individual preference for incarcerated mentors or staff members (or perhaps both). With recognition that only one-third of incarcerated people at the national level receive a visit from anyone per year (H. P. Smith, 2024), it is crucial that incarcerated women with mental health conditions not self-isolate at extreme levels. Practical recommendations for policymakers and correctional institutions include implementing peer support programs and increasing access to mental health professionals who can provide consistent care. Additionally, creating a more supportive environment through regular mental health screenings and individualized treatment plans can help address the unique needs of these women (Johnson & Thompson, 2023).
Related to this finding of alienation in this sample was the theme of communication. Not only was communication perceived as an effective coping mechanism for these women, but this concept extended into recognition of the individuals’ humanity. Previous IPA research noted that stigmatization plays an important role in the experiences of women with mental health conditions (Spodenkiewicz et al., 2013), though stigma may be increased in justice-involved women who experience trauma, crime, mental health conditions, and incarceration (Ncube-Sibanda & Dube-Mawerewere, 2019; Patel, 2023). This moves stigmatization from a purely psychological construct to one that relies heavily on the social milieu as normalization of mental health conditions. Patel (2023) and Sierka (2015) both mention the high prevalence of mental health conditions in incarcerated women and argue for ecological approaches that can be used to “design a more supportive and evidence-based service delivery system to justice-involved people” (Patel, 2023, p. iii).
Limitations and Future Research
The current study produced rich, qualitative data that documents the experiences of a sample of incarcerated women with mental health conditions; however, it is not without limitations. Fifteen female participants were included in the sample from a medium-maximum security prison in one southeastern state. Outcomes might be different in other states or regions, and within different prison settings, thus limiting the generalizability of the study. Additionally, while the sample was purposive and included incarcerated participants who had been diagnosed with a mental health condition, official records and other forms of information were not included to verify these conditions. Instead, the study relied only on self-report of the participants’ symptoms and diagnosis, who may have received confusing and conflicting information about their mental health status over the life course. Moving forward, it would be beneficial for future studies to enhance interviews with the triangulation of alternate data sources that can offer further confirmation of study results, including institutional records and interviews with treatment staff working with this population for a more holistic perspective. Such an endeavor could also incorporate more detailed demographic information to examine how culture, socioeconomic status, and race influence this topic.
Concluding Remarks
The current study provided insight into an often-ignored perspective, that is, the experiences of incarcerated women with mental health conditions. This population will be valuable for future research as they have considerable, often unique, experiences over the life course, and they continue to occupy a disconnected, alienated relationship to broader society. These women have extensive knowledge regarding their mental health, in some cases, using it as a lens to evaluate the behaviors of themselves and others. This denotes the unexpected finding that their own victimization, and explanations for their perpetrator’s behavior, could be best explained as expressions of mental health conditions (rather than deviancy). While more research is needed to explore this perspective, this sample offers insight into mental health conditions occurring in prison.
As a final research note, while there is a lack of research that uses IPA to access the meaning of mental health conditions for incarcerated women, in recent years there has been a movement in theses and dissertations toward addressing this gap (Ncube-Sibanda & Dube-Mawerewere, 2019; Patel, 2023; Sierka, 2015). This may represent a heightened appreciation by emerging scholars of the value of IPA in accessing, coding, and analyzing the views of incarcerated people. This provides a research agenda that can “give a voice to the marginalized, often misrepresented group of women, many of whom were determined to have their story heard” (Sierka, 2015, p. 110). This study provides a foundation for further research in this area.
Footnotes
Acknowledgements
The authors wish to recognize Sarah Potvin for her assistance with feedback, minor edits, and reference formatting.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Declarations
Data reported in this study were not presented at any other venue, including other journal outlets, or at conference presentations. The findings from this study have exclusively been reported to this journal alone. Further, none of the data were posted on public forums such as listservs, or other websites as this would have violated the terms of the Institutional Review Board requirements. Only within this specific manuscript submitted exclusively to Criminal Justice and Behavior have findings from our data been shared.
In accordance with the human subjects panel that reviewed our study, data are stored solely on the password-protected University-issued laptop of the lead author. As part of Institutional Review Board requirements, we were not permitted the opportunity to share the raw data in any public forums as this was perceived as a violation of the anonymity and confidentiality of research participants. However, should a third-party be interested in collaborating on future research projects from these data, the lead author would be willing to do this, all the while maintaining private and confidential the data by keeping them stored on the aforementioned University-issued password-protected computer. Finally, none of the work associated with this study was pre-registered.