
Abstract
Youth with mental disorders are at elevated risk to experience violent victimization compared to the general population, and several risk factors have been identified. Less understood are factors that promote protection from victimization. Using the resilience perspective, the relationship between risk, protective factors, and violent victimization of youth with mental disorders are investigated. Because there are differential effects across sex on risk factors that are connected to victimization for this population, sex differences on risk and protective factors are also explored. Multivariate logistic regression and predicted probability models split on sex are used to explore how risk and protective factors impact violent victimization. Sex-specific differences in protective factors and violent victimization are discussed, and recommendations for policy and clinicians are explored.
Research has established that people with mental disorders are victimized at greater rates when compared to the general population (Desmarais et al., 2014; E. Silver, 2002), with a recent meta-analysis highlighting that victimization rates for people with mental illness were four to six times greater when compared to the general population (de Vries et al., 2019). Unfortunately, adolescents with mental disorders also experience victimization at greater rates (M. G. Turner et al., 2013), a concerning trend when considering the variety of negative experiences that are often connected to experiencing a victimization event early in one’s life course. More specifically, victimization has been linked to several consequences like exacerbating mental health symptomology (Cuevas et al., 2010; Manasse & Ganem, 2009); negatively impacting self-esteem (DeLisi et al., 2014) or physical health (H. A. Turner et al., 2010); and participating in various criminogenic behaviors like drug usage or offending (Agnew, 2002; Farrell & Zimmerman, 2017; Jennings et al., 2012). Researchers have also explored how demographic subcategories—like biological sex differences—impact prevalence rates of victimization for this population. Specifically, compared to the general population, females with mental disorders experience victimization at higher rates than males with mental disorders (Dean et al., 2018; Goodman et al., 2001; Marley & Buila, 2001). For example, Dean et al. (2018) note that the risk of victimization is consistently higher for women than for men with mental disorders across all categories, especially in the context of violence.
Perhaps because this population are at elevated risk to experience victimization, researchers have identified several domains of risk factors, including: (1) demographic (e.g., socioeconomic status, race; Policastro et al., 2016); (2) theoretically-derived (e.g., conflicted relationships perspective, lack of capable guardianship; Goodman et al., 2001; E. Silver, 2002; Teasdale, 2009; (3) shared with the general population (e.g., substance usage, offending; Johnson et al., 2016; Policastro et al., 2016; E. Silver et al., 2011; Teasdale, 2009); and (4) specific to mental health (e.g., disorder classification, hospitalization; Daquin & Daigle, 2018; E. Silver et al., 2011). Notably, there is evidence that risk factors differentially relate to victimization based on sex for this population, including differences on variables like diagnoses, substance abuse, behavioral/emotional outcomes, and social support measures (Dean et al., 2018; Marley & Buila, 2001). Further, there is some evidence for sex-specific consequences associated with victimization for youth with mental disorders. For example, Kim et al. (2018) found that males exhibited externalizing behaviors like behavioral problems and females showed internalizing behaviors like emotional distress following a victimization event.
Despite growing research on prevalence rates and risk factors associated with victimization for people with mental disorders, few empirical examinations have studied factors that promote protection from victimization. One theoretical perspective that may be useful in identifying factors that foster protection from victimization is the resilience perspective. Indeed, the focus of research on resilience is to examine a dynamic process that involves both risk and protective factors and how these factors impact negative outcomes (Fergus & Zimmerman, 2005; Masten, 2021; Rutter, 2012). Although there has been growing interest in understanding how resiliency relates to criminological behaviors (Christiansen & Evans, 2005; Daigle et al., 2010; Hart et al., 2007; Lauritsen et al., 1992; Resnick et al., 1997), there is little empirical research on factors that protect against experiencing violent victimization for youth with mental disorders. This is surprising, especially when considering that investigations into both—risk and protective factors relationship to victimization—will likely result in holistic approaches to crime prevention (Masten, 2021).
Although there are clear potential benefits of applying the resilience perspective to understanding victimization experiences of people with mental disorders, few studies have empirically examined this topic. Further, within the small research base investigating how risk and protective factors connect to victimization for this population, some researchers have focused on a clinical, adult population of people with severe mental illness (Langeveld et al., 2018). Because of this focus, there is limited knowledge on how resilience relates to victimization for adolescents with varying diagnoses and severity of mental disorders. Doing so is important, as adolescence is already a critical period for development in the life course (Davidson et al., 2015). This is especially true for adolescents experiencing mental health issues. In fact, approximately half of mental health episodes emerge during adolescence (Kessler et al., 2005). Given this backdrop, there is perhaps no other developmental time period in one’s life course more critical to examine factors that protect against victimization than the adolescent time period. For these reasons, using the resilience perspective as a guide, this study investigates how risk and protective factors impact violent victimization for youth with mental disorders. Further, because research has documented sex-specific risk factors for victimization for this population, it is plausible that protective factors will differentially relate to violent victimization across sex. As such, the potential differences on the relationship between risk factors, protective factors, and violent victimization across sex are also explored. In doing so, effective prevention efforts are likely to result through incorporating a holistic approach and identifying group differences based on sex, aligning with the responsivity principle (Andrews et al., 1990).
What is Resilience?
The resilience perspective has spawned a wealth of research across disciplines. Definitions of resilience typically include three components. First, the occurrence of stressful or traumatic experiences must occur, often coined as experiencing adversity (Herrmann et al., 2011). Second, evidence of healthy functioning after adverse experiences must be present, sometimes referred as growing from adversity (Bryant et al., 2022). Examples of healthy functioning include avoiding negative outcomes or negative psychiatric effects (Masten, 2021). Third, the mechanisms thorough which negative outcomes are avoided or ameliorated also need to be present. These mechanisms are referred to as protective factors that promote positive outcomes like avoiding negative trajectories (Fergus & Zimmerman, 2005). Multiple models of resilience have been developed, with the compensatory, protective, challenge, and protective-protective resilience models receiving the most empirical attention (Masten & Obradovic, 2006). Each resilience model incorporates risk and protective factors into the model, varying the ways in which resiliency is empirically examined. For example, the compensatory model refers to a protective factor counteracting or operating in the opposite direction of a risk factor (Fergus & Zimmerman, 2005), which is empirically examined through direct effects of risk and protective factors on an outcome.
More recent work has proposed other methods of conceptualizing resilience. One potential model—the resilience portfolio model (Grych et al., 2015)—may be useful to examine how protective and risk factors impact victimization events. The resilience portfolio model organizes protective factors into three domains—(1) self-regulation (e.g., capacity to manage difficult emotions and individual strengths); (2) interpersonal strengths (e.g., strong relationships to others, community support); and (3) meaning-making (e.g., finding meaning in difficult situations including spiritual or religious avenues). Notably, each domain focuses on malleable factors that can be targeted in intervention efforts (Grych et al., 2015).
It is important to note, though, that identifying protective factors associated with victimization should not be conceptualized as the opposite of risk factors, a common critique of resilience research (Masten & Tellegen, 2012). Instead, protective factors signal the presence of unique factors that can lower the risk of experiencing negative events. For example, a robust risk factor associated with victimization for people with mental disorders includes negative interactions and relationships with others, often coined as conflicted relationships (E. Silver, 2002). In fact, the effect of negative relationships has been connected to consequences like functional impairment (Ross et al., 2019), increased mental health symptomology (Ibarra-Rovillard & Kuiper, 2011), and heightened stress levels (Aeby et al., 2021), all of which are conducive to victimization experiences for this population. The inverse, or lower levels of conflicted relationships, however, does not translate to the presence of a protective factor. Rather, separate constructs, such as the presence of quality social support, likely operates in differing ways from conflicted relationships, ultimately impacting victimization in differing ways. For example, positive relationships can impact overall emotional and physical well-being (Mertika et al., 2020; Rueger et al., 2016), which is likely to reduce the risk of victimization for this population.
Resilience, Victimization, and Negative Outcomes
Although not a traditional application of resilience theory, criminologists have studied why at-risk youth are able to avoid negative experiences—like experiencing a victimization event—despite the presence of established socio-contextual risk factors (Christiansen & Evans, 2005; Daigle et al., 2010; Lauritsen et al., 1992). In doing so, researchers incorporated empirical and theoretically-derived risk and protective factors into analyses, contributing several findings.
First, protective factors related to interpersonal strengths like social support, social connectedness, and attachment to family provided protection from victimization experiences for youth (Christiansen & Evans, 2005; Daigle et al., 2010; Lauritsen et al., 1992). Pro-social activities related to the school and commitment to school (Daigle et al., 2010; Lauritsen et al., 1992), and protective factors related to neighborhood cohesion (Christiansen & Evans, 2005), also reduce the risk of experiencing victimization. Finally, there is evidence of significant group differences based on sex for certain protective factors. For example, protective factors like support from friends (Crosnoe & Elder, 2004) or parental monitoring (Christiansen & Evans, 2005) mattered for females, but not males in the general population. Although these studies were not applications of the resilience portfolio model, they do suggest that protective factors connected to self-regulation and interpersonal strengths are important candidates to consider in studies examining victimization as the outcome.
Other applications of the resilience framework have been applied to understand how protective factors connect to outcomes like violent offending, risky sexual behaviors, or substance abuse. Broadly, protective factors associated with self-regulation—including positive affect, self-esteem, and future orientation—contributed to avoiding criminogenic behaviors (Resnick et al., 1997; Scheier et al., 2000). Further, higher degrees of religiosity, a protective factor related to meaning making, also impacted antisocial behaviors (Wright et al., 2019). Together, it is likely that each domain of protective factors identified in the resilience portfolio model are important to include when examining the relationship between risk and protective factors, and its relationship to victimization for youth with mental disorders.
Resilience, Victimization, and Mental Health
Despite the importance of research on protective factors, and the potential applicability of the resilience portfolio model to victimization for people with mental disorders, there are few empirical studies (e.g., Langeveld et al., 2018) examining both risk and protective factors, and how they influence violent victimization. Further, none have explicitly tested if and how protective factors associated with victimization may differ based on group differences like sex for this population. Findings focused on a clinical sample of an adult population of people with severe mental illness (SMI), however, found that protective factors related to self-regulation and interpersonal strengths decreased the likelihood of experiencing victimization. Specifically, social support, employment, and mental-health symptom remission decreased the odds of experiencing victimization (Langeveld et al., 2018). These factors may also matter for adolescents with mental disorders, and there could be sex differences on protective factors, a connection that has yet to be explored.
It is notable that the three theoretical frameworks commonly applied to understanding victimization for people with mental illness highlight the importance of lifestyles, guardianship, and social interactions. More specifically, these frameworks are: (1) lifestyles/routine activities theory (L/RAT; Cohen & Felson, 1979; Hindelang et al., 1978; (2) conflicted relationships (E. Silver, 2002); and (3) social interactionist perspectives (Felson, 1992). Briefly, these theoretical perspectives explain that victimization risk varies based on social interactions (E. Silver, 2002), violation of social norms and key rituals (Felson, 1992), and demographic factors (like sex) that can expose a person to high-risk situations and people (Hindelang et al., 1978; Pratt & Turanovic, 2016). Further, the likelihood of a victimization event increases when motivated offenders, suitable targets, and the absence of capable guardians, converge (Cohen & Felson, 1979). Because of the emphasis on how lifestyles, guardianship, and social interactions impact victimization risk, it is likely that protective factors derived from these perspectives may reduce the odds of experiencing victimization for youth with mental disorders.
Resilience and Sex Differences
There are several reasons it is important to examine sex differences in how protective factors impact victimization for youth with mental disorders. First, there are theoretical justifications for examining sex differences. For example, there is some evidence of differences based on sex in the stress coping perspective (Stroud et al., 2002). Among people with mental illness, for example, previous research has shown that females responded to stress through seeking out support from peers, while males responded to stress in line with fight or flight reactions (Teasdale et al., 2006). Stress perspectives also highlight the impact stress has on one’s internal states, specifically arguing that fewer cognitive resources are available in times of heightened stress (Marin et al., 2011). As a result, fewer cognitive resources may hinder interpersonal interactions (which could impact guardianship) and influence external awareness, which can lead to an inability to focus on the external world and engage in self-protection behaviors. As others have suggested, when internal states are in turmoil, external awareness reduces, which heightens target suitability and increases the risk of victimization for people with mental disorders (R. B. Silver et al., 2005; Teasdale et al., 2021). Together, it is possible that protective factors related to interpersonal strengths (e.g., relationships, support from others) of the resilience portfolio model may have a stronger effect in decreasing victimization for females compared to males. Alternatively, given that males appear to have stronger affective reactions to stressful life events, protective factors related to self-regulation (e.g., capacity to manage negative emotions) may matter more in decreasing victimization for males compared to females.
Second, lifestyles/exposure theory asserts that lifestyle differences based on demographics (like sex) may expose people to situations with differing risk for victimization (Hindelang et al., 1978). For this reason, some have suggested that sex can shape daily routines and create a sex-specific relationship with victimization (Novak & Crawford, 2010; Popp & Peguero, 2011). Because of this, research has established sex differences in prevalence rates, risk factors, and consequences associated with victimization. For example, for youth exhibiting symptoms of mental illness, prevalence rates of victimization differed. Specifically, females reported significantly higher rates of victimization compared to males (Kim et al., 2019). Differences in risk factors based on sex have also been examined in which key differences in risky lifestyles have been highlighted. For instance, males in the general population were more likely to be involved in offending, delinquent peers, and gang membership (Bunch et al., 2015), all of which heightens victimization risk. Further, sex differences on guardianship measures have also been established, finding that measures of attachment and supervision, and there connection to victimization, mattered more for females compared to males (Augustyn & McGloin, 2013). Finally, a recent meta-analysis found sex-specific differences on social bonds and routine activities (Pusch & Holtfreter, 2021). Given these differences on the relationship between risk and victimization that is sex-specific, it is likely there are also sex differences on protective factors associated with victimization for this population.
Third, patterns of mental health epidemiology (Dohrenwend & Dohrenwend, 1976) may also impact the relationship between risk/protective factors and victimization. Indeed, research has shown that females tend to have higher rates of internalizing disorders like depression (Kessler et al., 1994), while males exhibit higher rates of externalizing disorders like substance abuse/dependence or antisocial disorders (Eaton et al., 2012; Kessler et al., 1994). As a result, males and females tend to express distress in different ways, with males expressing distress through outward behaviors (e.g., externalizing) like substance usage or delinquency, and women expressing distress inward (e.g., internalizing) often resulting in symptoms of depression or low self-esteem (Horwitz & White, 1987). Considering these patterns, certain protective factors like high self-esteem may have a stronger impact on reducing the risk of victimization for females with mental disorders than males. Alternatively, males with mental disorders may benefit from self-regulatory protective factors like commitment to pro-social institutions (like the school), which may mitigate risky behaviors that are conducive to victimization and promote healthy boundaries of antisocial behaviors.
Current Study
Although there have been attempts to incorporate risk and protective factors to understanding victimization for adults with mental disorders (Langeveld et al., 2018), there is still much that is unknown. For example, one unknown includes understanding how risk and protective factors influence victimization for youth with mental disorders and if there are differential effects based on sex. This is surprising when considering calls for holistic approaches to crime prevention (Masten, 2021), and the knowledge that prevention efforts may have more success when targeting group differences based on sex (Andrews et al., 1990). Perhaps through developing interventions aimed at targeting evidence-based protective factors and tailoring such prevention efforts specific to one’s sex, it is possible that the life course of adolescents with mental disorders may be altered from one involving victimization to a trajectory of resiliency. For these reasons, using the resilience portfolio model and prior research to guide variable inclusion, the current study explores if and how risk and protective factors influence violent victimization for youth with mental disorders, and if there are sex differences on these factors using the National Comorbidity Study-Adolescent Supplement (NCS-A).
Method
Data and Sample
Data from the NCS-A, a nationally representative, cross-sectional, community-based sample of adolescents with and without mental disorders (Kessler et al., 2009; Merikangas et al., 2010), were used to explore sex differences in protective factors related to resilience from victimization. Collected through a dual-frame sampling design, household and in-school samples were included. Household surveys were given to youth residing in households identified in the National Comorbidity Replication Study (NCS-R). The in-school sample included a total of 320 schools, with 40 to 50 randomly selected eligible students within each school (Kessler et al., 2009). Data collection ended in 2004 (beginning in 2001), resulting in 904 adolescents in the household sample and 9,244 adolescents in the school sample (n = 10,148). Interviews were based on the Composite International Diagnostic Interview (i.e., CIDI), and administered through a computer-assisted personal interview method (i.e., CAPI). More detailed information on sampling procedures is available (see Kessler et al., 2009; Merikangas et al., 2010). Because of the focus on youth with mental disorders, analyses were limited to adolescents meeting the diagnostic criteria for a DSM-IV diagnoses, resulting in an analytic sample size of 3,970 adolescents with mental disorders after list-wise deletion. 1
There are several benefits to using the NCS-A to explore mental health, protective and risk factors, and victimization. For example, a common methodological critique includes making inferences about mental health and violence through non-representative populations (Whiting & Fazel, 2020). Given that the purpose of the NCS-A was to provide nationally-representative estimates of the prevalence of DSM-IV mental disorders for youth residing in the community (i.e., anxiety, mood, behavioral, and substance disorders), the NCS-A is an ideal candidate to understand how risk and protective factors impact victimization for youth with mental disorders within the community. Further, one goal of the NCS-A was to establish risk and protective factors associated with early expressions of adult mental disorder and patterns of service use for adolescents (aged 13–17) with mental disorders (Merikangas et al., 2010). Because of this focus, the NCS-A is an especially rich dataset that includes validated diagnostic criterion and a broad spectrum of factors related to adversities and protection, lending valuable insight into how risk and protective factors impact victimization for youth with mental disorders.
Measures
Dependent Variable
Violent victimization was captured through seven questions including asking if the participant had ever been: (1) badly beaten up by a parent, (2) badly beaten up by a romantic partner, (3) badly beaten by anyone else, (4) mugged, (5) raped, (6) sexually assaulted, or (7) stalked. Each lifetime estimate of violent victimization was followed up with the question, “how old were you the first time [this victimization event occurred].” To limit the time frame to the past 12 months, if the participant indicated the victimization first occurred during their current age, or their age minus one, then they were coded as a victim. Thus, if a participant experienced any of the seven victimization events within the past 12 months they were coded as 1, and coded as 0 if they had not experienced a victimization event.
Mental Health Indicators
The CIDI, a fully structured interview in which trained interviewers generate clinical diagnostic estimates of DSM-IV diagnoses is used (Merikangas et al., 2010). Hierarchical diagnoses are used when appropriate. 2 Using Kessler and Ustün’s (2004) grouping of disorders, all classifications are dichotomous in which those meeting the clinical significance for that disorder are coded as a 1, and coded as a 0 if not. Classifications included: anxiety related disorders (panic, agoraphobia, generalized anxiety with hierarchy, post-traumatic stress, social phobia disorders); bipolar related disorders (bipolar I, bipolar II, hypomania, mania); depression related disorders (dysthymia with hierarchy, major depressive with hierarchy disorders); substance related disorders (alcohol abuse with hierarchy, alcohol dependence, drug abuse with hierarchy, drug dependence disorders); impulse control disorder (intermittent explosive disorder with hierarchy); and childhood related disorder (attention deficit disorder, separation anxiety disorder, conduct disorders). 3
Independent Variables
Using the resilience portfolio model, theories and perspectives related to victimization, and prior empirical findings to guide variable selection, risk and protective factors are included as independent variables.
Risk Factors Related to Adversities
Three variables drawn from L/RAT were used, including: crime perpetration (dichotomous indicator if committed or arrested for a crime or not), alcohol usage (dichotomous indicator if drank alcohol in past 12 months or not), and drug usage (dichotomous indicator if used marijuana, cocaine, or prescription drugs without doctor’s recommendation in past 12 months or not). Conflicted relationships is captured by summing seven variables (Cronbach’s alpha = .65) in which participants were asked to identify if in the past 12 months they were having serious ongoing disagreements or problems getting along within seven relationships (e.g., romantic partner, friends, parents, etc.) (higher scores indicated greater involvement in conflicted relationships). 4 Finally, following prior researchers (Felson, 1992; Teasdale, 2009), the social interactionist perspective was operationalized as stressful life events. This measure captured 12 different life events that produce stress (e.g., break up with romantic partner, parents getting separated or divorced, etc.) in which the sum was taken, resulting in a variety score where higher scores indicate greater number of stressful life events.
Protective Factors Related to Self-Regulation
Three protective factors related to self-regulation (e.g., individual-level strengths; Grych et al., 2015) were included. First, self-esteem was captured through a shortened version of Rosenberg’s (1965) self-esteem scale in which four statements were used (e.g., “overall, I am satisfied with myself”). Responses ranged from (0) not at all true to (3) very true. The mean of the four statements was taken, where higher scores indicate greater self-esteem (Cronbach’s alpha = .72). Because one’s commitment to school influenced positive outcomes from victimization (Daigle et al., 2010; Lauritsen et al., 1992), two measures were used. The first is one that captures students’ grades. Two ordinal measures (e.g., one measure capturing current students and one measure capturing those who are not currently students) were combined (e.g., “what kind of grades do you get?”; “what sort of grades did you get in your last years at school?”). Responses included below average (0), average (1), and above average (2). Higher scores indicate higher grades for participants both in and out of school. The second measure captures one’s commitment to school. Specifically, participants were asked about nine different statements about their perception and commitment to school (e.g., “I try/tried hard at school,” “I feel/felt as if I don’t/didn’t belong at school” [reverse coded]). Responses ranged from not at all true (0) to very true (3). The mean of the nine items was taken, where higher scores indicate greater levels of commitment (Cronbach’s alpha = .79).
Protective Factors Related to Interpersonal Strengths
Five protective factors related to interpersonal strengths were included. First, peer support was captured through three questions (e.g., “how much can you rely on your friends for help if you have a serious problem?”). The peer support measure was created by first standardizing the measures, and then taking the mean of the responses, with higher scores indicating greater levels of peer support (Cronbach’s alpha = .60). 5 Adult support was created through two questions in which participants were asked to list how many adults they felt comfortable talking to about personal life issues and to list the number of adults they felt cared a lot about them. Both measures were added together and the natural log was taken to account for the skewness of the variable. Higher numbers indicate greater adult support. Two measures related to parental support were also included. The first measure includes five different questions assessing the participant’s relationship to their mother (e.g., how emotionally close?; how much love and affection did she give them?). Responses ranged from (0) not at all to (3) a lot. To create the parental connectedness measure, the mean of the five items was taken, where higher scores indicate greater perceptions of connectedness to one’s mother (Cronbach’s alpha = .77). The second parental support measure reflects the degree of parental supervision, as this was a protective factor that significantly differed based on sex in prior studies examining resilience and victimization (e.g., Christiansen & Evans, 2005). Specifically, three questions were included in which participants were asked how much their mother stopped them from doing things other kids were allowed to do or how strict she was. Responses ranged from (0) not at all to (3) very. The mean of the three items was taken, resulting in a parental monitoring variable in which higher scores indicate greater parental monitoring (Cronbach’s alpha = .61). 6 The last measure relates to ones’ psychological sense of community, ones’ attraction to neighborhood, and the degree of neighboring through three different questions (e.g., “how happy are you living in your neighborhood?”). After standardizing the three items, the mean was taken in which higher scores reflect greater sense of neighborhood cohesion (Cronbach’s alpha = .56). 7
Protective Factors Related to Meaning-Making
Previous research argues that religious and spiritual meaning making are key avenues in which people cope with violence (Hamby et al., 2018). As such, a religiosity measure is included. After standardizing four questions (e.g., when you have problems or difficulties in your family, work, or personal life, how often do you seek comfort through religious or spiritual means?), the mean was taken to create a measure of religiosity in which higher scores indicate greater religiosity (Cronbach’s alpha = .88).
Control Variables
Age, race (i.e., self-report measure reflecting Black, Hispanic, Other, or White [referent category]), and a poverty index ratio to capture socioeconomic status (i.e., ratio of family income to family poverty threshold level and size) were included. More specifically, socioeconomic status reflects a categorical measure of the poverty index where the household income that is less than 1.5, less than or equal to 3, less than or equal to 6, or greater than 6 times the poverty line (referent group) was used (see Merikangas et al., 2010).
Analysis
Several steps were taken for the analyses. First, to account for the complex sampling design of the NCS-A, weights were applied and the svyset command in Stata 17 was used. Second, univariate and bivariate group differences on all the variables were examined. Lastly, following the resilience portfolio model as a guide, risk factors connected to adversities, three domains of protective factors, and control variables were included in a multivariate logistic regression model split by sex, consistent with prior scholarship (Gonzalez-Mendez et al., 2021; Hamby et al., 2018). Since the dependent variable is nonlinear, Mize’s (2019) guidelines for best practices to estimate, interpret, and present interaction effects were followed. Because the coefficient on the interaction term can be a misleading representation of the effect in nonlinear models, Mize (2019) and others (Mood, 2010) recommend testing interaction effects through predicted probabilities as opposed to regression coefficients. For this reason, predicted probabilities were estimated through marginal effects using the margins command in Stata to examine sex differences on significant protective factors. 8 In doing so, both sides of the interaction effect are examined through 95%confidence interval in plotted figures of the predicted probability of being resilient from victimization. Notably, when confidence intervals do not overlap across biological sex, significant group differences exist (Mize, 2019, p. 90).
Results
The descriptive statistics for the total sample are presented in Table 1. As shown in Table 1, approximately 14% of the total sample of adolescents with mental illness experienced violent victimization. More specifically, the majority of females (85%) and males (87%) with mental illness did not experience victimization. The average age for males and females was 15, and over half reported that they were White. Diagnostic prevalence rates differed across females and males. For females, over half had a diagnosis of an anxiety disorder, followed by depression (33%), childhood (33%), impulse control (27%), substance (22%), and bipolar (12%) disorders. Across males, approximately 38% were diagnosed with an anxiety disorder, followed by childhood (37%), impulse control (37%), substance (32%), depression (18%), and bipolar disorders (12%). Notably, statistically significant differences at the bivariate level emerged on the majority of variables for females and males.
NCS-A Descriptive Statistics of Youths With a Mental Illness.
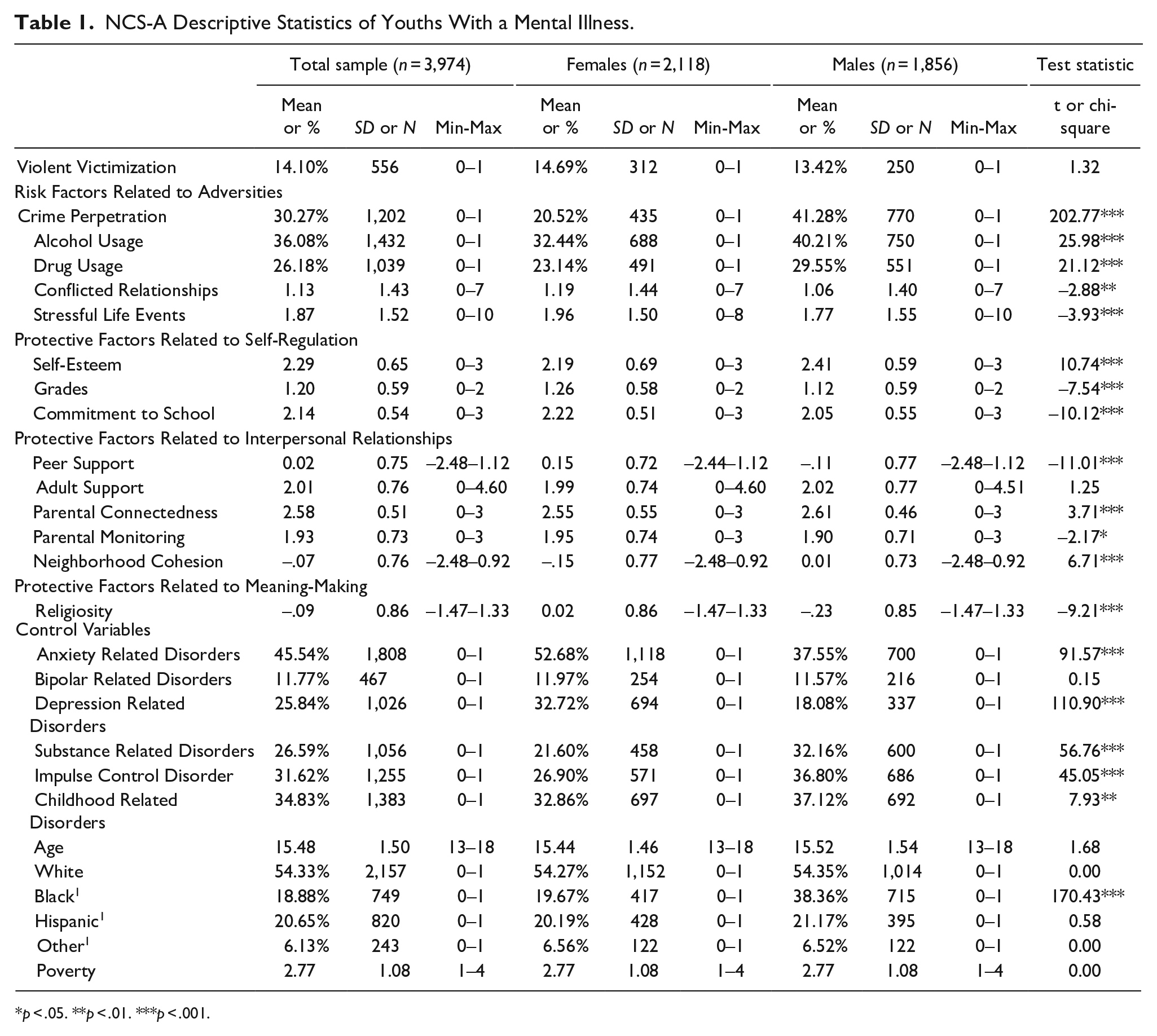
p < .05. **p < .01. ***p < .001.
To explore how risk and protective factors impact violent victimization, multivariate logistic regression models were used. As shown in model 1 of Table 2, several risk factors related to adversities increased the odds of violent victimization for the total sample of youth with mental disorders. Specifically, crime perpetration (OR: 1.55, p < .001), conflicted relationships (OR: 1.11, p < .05), and stressful life events (OR: 1.22, p < .001) significantly increased the odds of experiencing violent victimization. Surprisingly, only one protective factor related to self-regulation—self-esteem (OR: 0.75, p < .001)—decreased the odds of experiencing violent victimization for the total sample. Notably, the majority of protective factors related to interpersonal relationships and meaning-making did not significantly decrease the odds of victimization. Rather, one factor—parental monitoring (OR: 1.18, p < .05)—increased the odds of victimization. Finally, several control variables were also significantly related to victimization including: bipolar related disorders (OR: 1.73, p < .05), childhood related disorders (OR: 1.49, p < .05), and age (OR: 0.86, p < .05).
Multivariate Logistic Regression Predicting Violent Victimization Within the Past 12 Months Among NCS-A Youths With a Mental Illness.
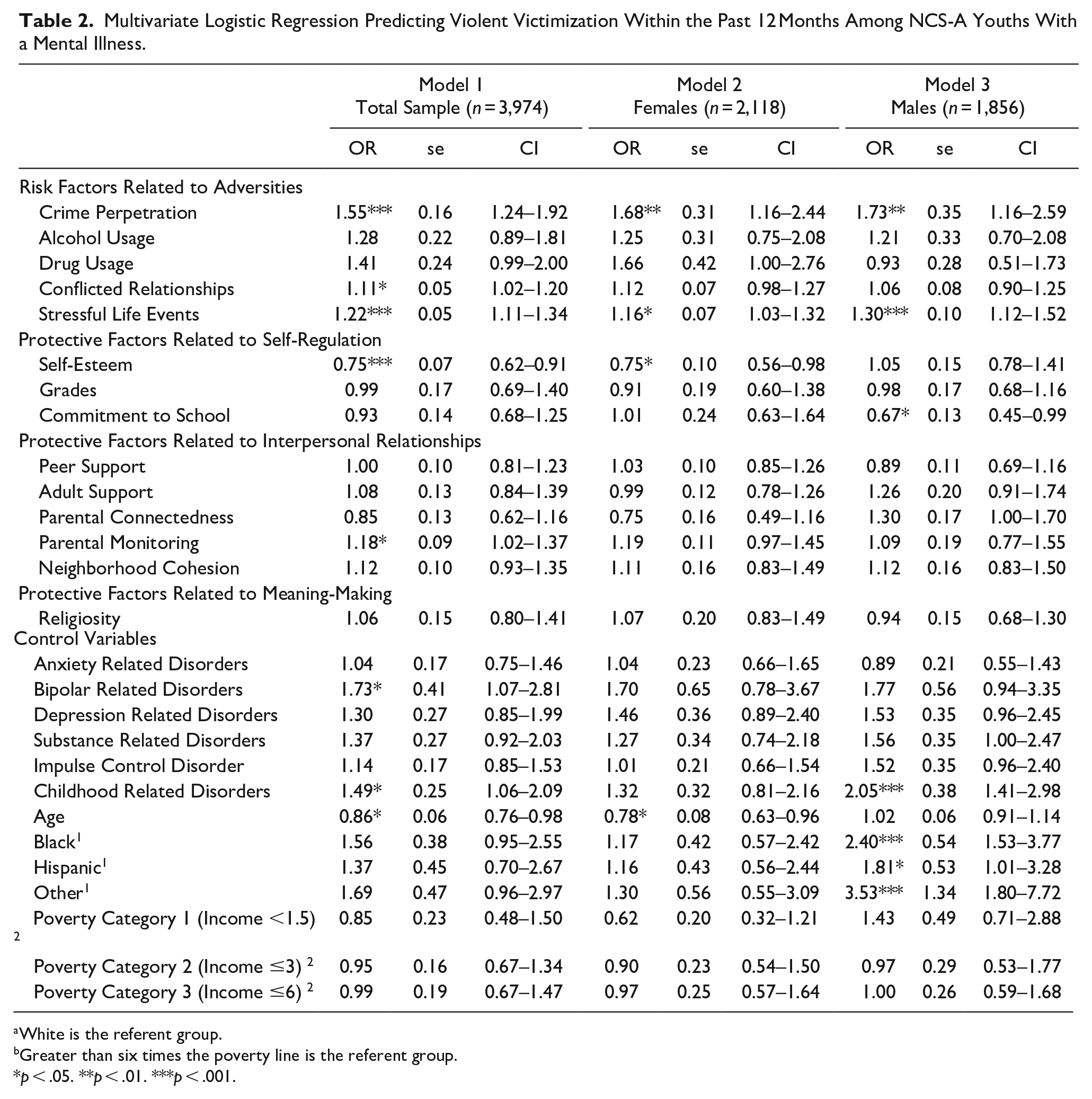
White is the referent group.
Greater than six times the poverty line is the referent group.
p < .05. **p < .01. ***p < .001.
Next, sex differences were explored. As shown in models 2 and 3 of Table 2, two significant risk factors related to adversities emerged for males and females—crime perpetration and stressful life events. Specifically, for females with mental disorders, crime perpetration (OR: 1.68, p < .01) and stressful life events (OR: 1.16, p < .05) increased the odds of experiencing violent victimization. Similarly, for males with mental disorders, crime perpetration (OR: 1.73, p < .01) and stressful life events (OR: 1.30, p < .001) also increased the odds of victimization. Unlike risk factors, there were differential findings on significant protective factors across sex. More specifically, for females with mental disorders, the odds of victimization decreased by 25% for every one-unit increase in the self-esteem scale. Alternatively, for males with mental disorders, for every one-unit change in the commitment to school scale, the odds of violent victimization decreased by 33%. Surprisingly, none of the protective factors related to interpersonal strengths or meaning making influenced the odds of experiencing victimization for both males and females with mental disorders. One control variable—age (OR: 0.78, p < .05) —significantly decreased the odds of victimization for females with mental disorders. For males with mental disorders, however, several control variables increased the odds of experiencing victimization including having a childhood related disorder (OR: 2.05, p < .001), being Black (OR:2.40, p < .001), or identifying as Other race/ethnicity (OR: 3.53, p < .001).
Lastly, predicted probability models were used to examine significant protective factors identified in the split models. Interestingly, significant sex differences were pronounced for females with lower levels of self-esteem; however, as self-esteem increased, sex differences decreased (see Figure 1). Thus, for youth who score in the top percentiles of self-esteem (e.g., 2.5 or 3 out of 3), differences across males and females with mental illness are no longer significant. There is also considerable overlap between male and female confidence intervals on the lower end of the commitment to school scale (e.g., 0–1.5 out of 3), suggesting that there are not significant sex differences for youth who are not as committed to school. Significant sex differences were present, however, on the high end of the commitment to school scale (e.g., 2–2.5 out of 3), suggesting that for males with mental disorders, higher levels of commitment to school can significantly decrease the risk of experiencing violent victimization (see Figure 2).
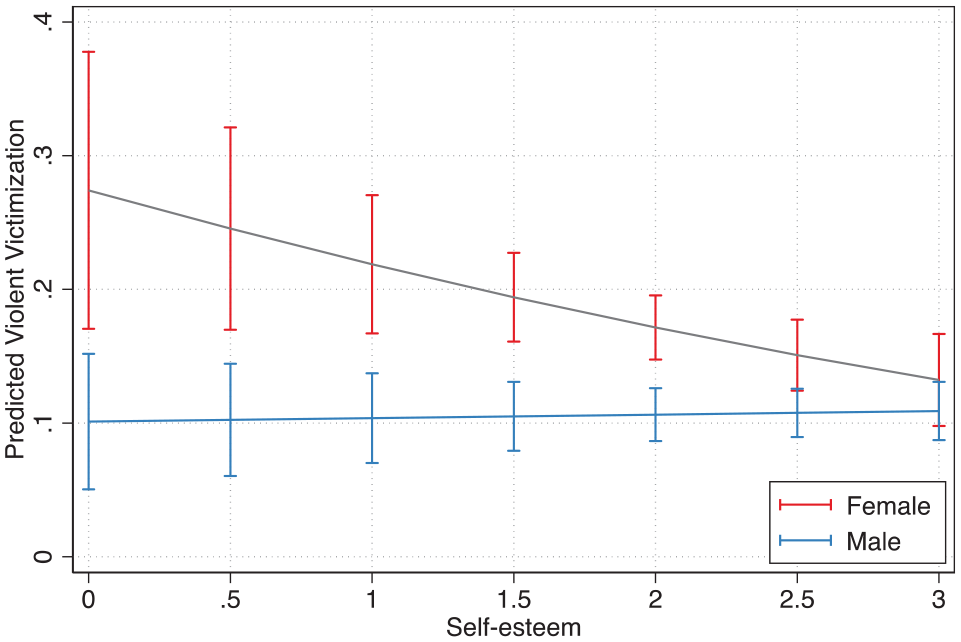
Sex difference on self-esteem.
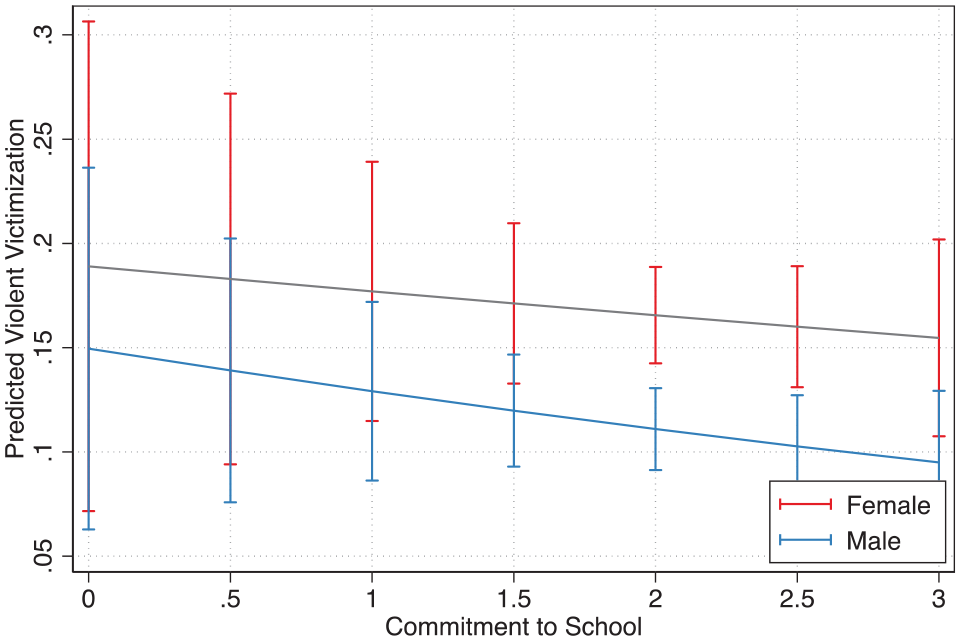
Sex difference on commitment to school.
Discussion
Although research has established that youth with mental disorders are at a higher risk for victimization when compared to the general population, less understood is why certain youth with mental illness are not victimized, despite elevated risk. Further, numerous risk factors that increase the likelihood of victimization for this population have been established. What has yet to be fully explored are the mechanisms that protect against negative outcomes like victimization. One useful perspective to explore in understanding factors that promote protection from victimization is the resilience perspective. Recent work has begun to apply the resilience framework through studying how risk and protective factors influence victimization using adult samples of people with serious mental illness (Langeveld et al., 2018). Despite this, there is limited knowledge on how the resilience framework connects to understanding victimization for people with less severe forms of mental disorders, and differences that may exist for an adolescent sample. For these reasons, using the resilience portfolio model (Grych et al., 2015), the relationship between risk factors, protective factors, and violent victimization are explored and sex differences are examined, contributing several findings.
First, at the bivariate level, there are several significant differences on risk and protective factors across sex. Specifically, significant sex differences were present on every risk factor related to adversities and every protective factor but one (e.g., adult support), further signifying the importance of examining sex differences on risk and protective factors associated with violent victimization for youth with mental disorders. In doing so, interventions can be designed to be sex-specific, which are likely to influence effective interventions (Andrews et al., 1990).
Second, aligning with prior scholarship (e.g., Johnson et al., 2016; E. Silver et al., 2011; Teasdale, 2009), two risk factors related to adversities significantly impacted victimization experiences across sex. Specifically, for youth with mental disorders, who engage in risky behaviors like crime perpetration, the likelihood of experiencing victimization increased, aligning with the large body of criminological research showing substantial overlap between offenders and victims. Indeed, prior research indicates that people who engage in offending behaviors are also more likely to be victimized, often coined as the victim-offender overlap (Lauritsen & Laub, 2007; Sampson & Lauritsen, 1990). Notably, previous research has found support for the victim-offender overlap for a sample of adults with mental disorders (E. Silver et al., 2011). Thus, in the context of L/RAT, youth who engage in offending behaviors likely lack capable guardians to prevent victimization experiences, may be among motivated offenders, and might be a suitable target for victimization experiences, aligning with previous findings of people with mental illness (e.g., Johnson et al., 2016; E. Silver et al., 2011; Teasdale, 2009).
Similarly, the risk factor—stressful life events—significantly increased the odds of being victimized, supporting Felson’s (1992) argument that stress and victimization should be correlated. Indeed, during times of heightened stress, one has fewer cognitive resources available (Marin et al., 2011), which may hinder interpersonal interactions. As explained prior, if persons are behaving in ways that are outside societal norms for interactions, social control attempts may escalate to violence, thereby resulting in victimization. Alternatively, researchers have postulated that when peoples’ states are turned inward (such as times that are highly stressful), they may be less aware of the world around them, and may not engage in self-protective behaviors to prevent victimization experiences (R. B. Silver et al., 2005; Teasdale, 2009). Thus, stress can impact external awareness, which can also heighten the risk of being a suitable target, a component of L/RAT (Cohen & Felson, 1979; Hindelang et al., 1978). It is interesting that these patterns were consistent across sex, suggesting that youth with mental disorders, in general, would benefit from stress management intervention efforts. Promising examples include creative art interventions (L. Martin et al., 2018), exercise-based interventions (Stubbs & Rosenbaum, 2018), or interventions designed to reduce stress (e.g., relaxation techniques, cognitive-behavioral therapy, mindfulness; Holman et al., 2018), all of which have shown positive outcomes for people with mental disorders. Notably, when examining the total sample, one other risk factor related to adversity also significantly increased the odds of experiencing violent victimization—conflicted relationships—aligning with E. Silver’s (2002) theory and prior findings. Because E. Silver (2002) used an adult sample of people with SMI from three different sites, it is informative that using a nationally-representative sample of youth with mental disorders, whom are involved in conflicted relationships, also heightened the odds of experiencing victimization, highlighting the importance of quality social support. As such, attachment-based interventions (see Moretti et al., 2015), many of which are tailored to the needs of youth with mental disorders (see Diamond et al., 2003) may be especially helpful in preventing victimization experiences for this population.
Third, only one domain of protective factors outlined in the resilience portfolio model—those related to self-regulation—significantly impacted experiencing violent victimization. More specifically, self-esteem decreased the odds of experiencing a victimization event for the total sample, aligning with other research that shows for people with mental illness, higher degrees of self-esteem can increase the probability of other positive outcomes (Kao et al., 2017). In examining sex differences on protective factors related to self-regulation, it is interesting that for females—self-esteem—and for males—commitment to school—decreased the odds of being victimized for youth with mental disorders. Although speculative, these findings are likely linked to sex differences in mental health epidemiology and pathology. As discussed, females often internalize psychological distress, which can result in heightened levels of depression or anxiety (Kuehner, 2003). Because perceptions of one’s self can be distorted as a result of internalizing disorders like depression, researchers have noted troubling trends of distorted cognitive functions that alter one’s perception of the environment around them. These distortions can lead those suffering from internalizing disorders to evaluate their performance as dissatisfactory (Coyne & Gotlib, 1983), often attributing good outcomes to unstable and external factors when compared to those without internalizing disorders (Seligman et al., 1979). Psychological resources, like self-esteem, however, can impact psychological distress (Nurullah, 2010), and help promote healthy psychological functioning (Baumeister, 1993). With these trends in mind, it makes sense that self-esteem would significantly decrease the odds of experiencing victimization for females, who often internalize distress, compared to males, who often externalize distress.
Alternatively, males tend to externalize psychological distress through antisocial behaviors (e.g., substance abuse, aggression, oppositional behaviors), some researchers have examined factors that contribute early expressions of externalizing problems, and how they relate to one’s life-course (Campbell et al., 2000). Indeed, as one moves through the life-course, characteristics related to the school, such as relationships formed with teachers for example, can impact subsequent behavior. In fact, researchers have found that externalizing behavior significantly decreased as teacher-child closeness increased (R. B. Silver et al., 2005). As follows, then, it is logical that commitment to school would be an important protective factor for males, who often externalize psychological distress and may benefit from the structure the school provides, compared to females. Further, it is also possible that the school may be serving as a means of informal social control (see Daigle et al., 2010). Thus, it is likely that the structure and commitment to school may discourage and even possibly prevent externalizing behaviors that are common for males with mental disorders.
It is notable that there is evidence supporting these arguments. For example, many females in this sample met the diagnostic criteria for disorders that internalize psychological distress like anxiety or depression disorders. Further, most males met the diagnostic criteria for diagnostic types that are often accompanied with externalizing psychological distress such as substance, impulse control, and childhood related disorders, all of which were statistically significant differences at the bivariate level. In fact, in the multivariate model, childhood disorders (e.g., ADD, CD, etc.) significantly increased the odds of being victimized for males with mental disorders but did not do so for females. Considering that males often externalize distress through substance abuse or delinquent behavior that may be commonly correlated with childhood disorders like conduct disorder or ADD, it would make sense that this diagnostic type emerged as significant for males but not females, and that this disorder type was connected to victimization for males. Relatedly, it is also logical that as age increased, the odds of experiencing victimization for females decreased, but had no significant impact for males. Stated differently, because males and females mature at different rates (Waber, 1976), it is likely that females age out of risk faster than males (Mahalik et al., 2013), thereby decreasing the risk of victimization.
Fortunately, there are prevention efforts that improve perceptions of self-esteem and strengthen relationships to the school for youth with mental illness. For example, cognitive behavioral therapy (CBT) interventions have shown success in improving levels of self-esteem for people with mental disorders, especially females with mental disorders (Morton et al., 2012), and can even improve mental health symptomology such as depression or anxiety (Kunikata et al., 2016; Morton et al., 2012; Rigby & Waite, 2006). As such, CBT interventions aimed at increasing self-esteem may be especially useful to implement for adolescent females with mental disorders. Further, there are promising interventions that could be implemented for males with mental disorders, possibly because schools often play a significant role in enhancing student’s mental health and overall well-being (Das et al., 2016). Because of this, it is likely that the school is another institution that can target known risk factors for victimization for males with mental illness, which would ultimately reduce the likelihood of a victimization event from occurring. Many school-based mental health interventions include targeting and training students on certain resources—in other words, protective factors—such as interpersonal skills, self-esteem, self-efficacy, or optimism (Das et al., 2016). As a result, it is possible that school-based interventions would also provide strategies to reduce externalizing behaviors, with some school-based interventions showing a significant increase in overall mental health and decrease in problematic behavior (Shoshani & Steinmetz, 2014).
Fourth, contrary to expectations, it was surprising that there was a lack of findings supporting the other domains of protective factors outlined in the resilience portfolio model—such as protective factors related to interpersonal strengths and meaning making—for the total sample and across sex for youth with mental disorders. In fact, for the total sample, one protective factor related to interpersonal relationships, parental monitoring, actually increased the odds of experiencing victimization. Because of the cross-sectional nature of the NCS-A data, it is possible that youth may rebel against increased parental monitoring, which may result in youth engaging in risky behaviors, like sneaking out the house for example, that could result in a victimization experience. In fact, Sasson and Mesch (2014) found that for youth with restrictive parental supervision, such supervision practices actually increased risky online behaviors. Alternatively, it is also possible that victimization leads to increased parental monitoring (see Stavrinides et al., 2015).
Nevertheless, the insignificance of these domains of protective factors outlined in the resilience portfolio model suggests that people with mental illness are unique, and nuances related to risk and protection should further be explored for this population. Stated differently, it is notable that through empirically testing the resilience portfolio model, both risk and protective factors are incorporated into a model predicting healthy functioning (or in the case of the current study- avoiding victimization despite heightened risk). Given this, theoretical and empirical risk factors specific to the general population (e.g., L/RAT) and specific to people having a mental illness (e.g., conflicted relationships and social interactionist perspectives) were included. Further, established protective factors that influence resilience from negative outcomes and victimization within the general population were also included (Christiansen & Evans, 2005; Daigle et al., 2010; Lauritsen et al., 1992). Despite prior studies highlighting the applicability of these protective factors, the lack of findings on significant protective factors for youth with mental disorders is surprising. Because youth with mental illness are already at heightened risk to experience victimization, it is also possible that the magnitude of the strength of these theoretically-derived risk factors may be overpowering any potential positive effects of protective factors. In other words, it could be that this population may either need a greater number of protective factors or more robust protective factors to increase the odds of resilience from victimization. Future research should examine how other protective factors specific to mental health may influence victimization experiences like heightened psychological resources (see Pearlin et al., 1981), a possibility I was unable to test within the current data.
With that said, however, it is encouraging that protective factors related to self-regulation promoted a reduction in victimization experiences for males and females with mental disorders, even when accounting for well-established risk factors related to victimization and factors related to disadvantage for this population (e.g., SES, race, diagnostic type). Further, the importance of tailoring interventions based on sex was supported in this study, considering that there were no similarities on protective factors that influenced victimization based on sex. Perhaps one of the most important implications of this study is the recognition that intervention efforts should especially be designed differently for females and males during the adolescent time period (Ma & Huebner, 2008). Collectively, these findings are important because clinicians can target protective factors that show a direct effect on decreasing the probability of experiencing victimization, and can tailor these prevention efforts to be sex-specific. Thus, interventions given in a school-setting, aimed at increasing academic drive, may be especially important for adolescent males with mental disorders. Alternatively, interventions aimed at increasing self-esteem for adolescent females with mental disorders are likely to translate to a reduction in victimization experiences.
Limitations
Despite these novel findings, there are some limitations. First, certain scales included in the analyses had low reliability levels. Although exploratory factor analyses indicated that each scale included in the analyses loaded onto one latent construct, caution should be taken when interrupting these results. Further, only one variable connected to meaning-making was available in the current dataset. Because of this, there is the potential for omitted variable bias connected to the construct of meaning-making. Future research should apply other measures of meaning-making like measures connected to spirituality. Further, these data are cross-sectional, limiting the ability to establish temporal ordering. Although the dependent variable, violent victimization, was restricted to the past 12 months in an effort to establish some temporal ordering, future research should incorporate longitudinal research designs.
Conclusion
Despite these limitations, this study explored if and what sex differences emerged on risk and protective factors that influenced violent victimization for youth with mental disorders. In doing so, sex differences were shown on one domain of protective factors outlined by the resilience portfolio model—those related to self-regulation. This investigation into sex differences on protective factors related to victimization suggests the need for continued research on resiliency for this population, as protective factors are likely more malleable and easier to target in intervention efforts than risk factors (which are often static and thereby difficult to change), as highlighted by others (Grych et al., 2015; Masten, 2021). Further, identifying group differences in protective factors for this population, such as the investigation into sex differences, are likely to translate to more effective interventions, ultimately leading to a reduction in violent victimization rates for adolescents with mental disorders.
Footnotes
Acknowledgements
I would like to thank Brent Teasdale for commenting on earlier drafts of this manuscript.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.