
Abstract
While there is a growing body of research on parent-child visitation among the general carceral population, less attention has been paid to examining parent-child contact practices among parents with mental health illness diagnoses. The current study uses a sample from the 2016 Survey of Prison Inmates to analyze the associations between mental health illness diagnosis and various modalities of parent-child contact. Multivariate analyses of types of mental health illness diagnoses on six parent-child contact modalities demonstrate heterogeneity where not all mental health diagnoses reduce all parent-child contacts. Furthermore, incarcerated parents with multiple mental health illnesses are less likely to experience most forms of contact including in-person visits, phone calls, and mail.
Introduction
Parent-child relationships are built through parental involvement such as spending time together and increased communication including listening to children, being available, and conveying love and empathy (see Ackard et al., 2006). Mental health illnesses and incarceration, independently, can inhibit the formation and strength of parent-child relationships. Stressors associated with caring for one’s mental health can negatively impact coping skills and capacity for parenting, impairing a parent’s ability to build a strong connection with their children (Maybery & Reupert, 2009; Peterson, 2019). Parents who are incarcerated face logistical barriers to establishing and maintaining relationships including physical distance between children and the prison where the parent is housed (Poehlmann-Tynan & Pritzl, 2019). There is an emerging and promising literature outlining the positive effects of in-person visitation among incarcerated parents for those who can overcome issues related to distance. In-person visitation has been shown to improve general mental health and contribute to better parent-child relationships (De Claire & Dixon, 2017; de Motte et al., 2012; Poehlmann, 2005; Poehlmann et al., 2010). However, much of this research has concentrated on general carceral populations, with less emphasis on parent-child contact practices among those with mental health illness diagnoses. Further, the focus on in-person parent-child contacts does not address other modalities that can occur more frequently than in-person visitation (e.g., phone, email, mail).
Understanding parent-child contact practices in prisons is imperative because most incarcerated persons are parents (Mumola, 2000). At present, little is known about various parent-child contact practices among parents with a mental health illness diagnosis because prior studies have not examined the relationship in much detail. The COVID-19 pandemic amplified the need to rely on other forms of parent-child contact including written correspondence (email, traditional mail) and phone calls as in-person visitations became increasingly difficult and were complicated by concerns related to social distancing and reducing the spread of infectious disease (see Dallaire et al., 2021). Despite this shift, the bulk of the research remains centered on in-person contacts. Our study addresses these gaps in the literature by exploring the relationship between mental health illness diagnosis and parent-child contact practices in prisons. Specifically, we examine whether having specific mental health illness diagnoses and number of illnesses are associated with a lower likelihood of parent-child contacts.
Mental Health Among Carceral Populations
The deinstitutionalization of mental health facilities and psychiatric inpatient care has led to law enforcement personnel becoming first responders for public safety incidents involving persons with mental health illnesses (Lamb et al., 2002). Approximately 10% of all law enforcement calls for service involve mental health illness and about 2 million jail bookings each year are for people with serious mental health disorders such as schizophrenia, bipolar, and depressive disorder (NAMI, n.d.; Watson & Angell, 2013). As a result, jails and prisons house more persons with mental health illnesses than state psychiatric hospitals (Bronson & Berzovsky, 2017; Lamb & Weinberger, 2005; The Sentencing Project, 2009; Yi et al., 2017).
Once incarcerated, people with mental health illnesses may not receive necessary treatment. Mental health care is lacking in institutional settings due to insufficient funding, poor mental health screening, and systematic barriers (James & Glaze, 2006; Reingle Gonzalez & Connell, 2014). A mere 14% of prison budgets are allocated for mental health care (Pew Charitable Trusts & MacArthur Foundation, 2014). An analysis of the 2004 Survey of Inmates data showed that more than half of incarcerated parents in state prisons reported a mental health problem, and only a third received treatment (S. Christian, 2009; Glaze & Maruschak, 2008). The undersupply of adequate mental health care services and treatment during periods of confinement can impede rehabilitation efforts during incarceration and hamper successful reentry (Harding & Roman, 2017; Mallik-Kane & Visher, 2008).
Mental Health Benefits of Prison Contacts
While mental health illnesses contribute to social isolation (Crisp et al., 2000; Kohn & Clausen, 1955), visits during incarceration enhance social connections and they alleviate mental health symptoms (e.g., Poehlmann, 2005). In a meta-review of research exploring the effect of prison visitation, De Claire and Dixon (2017) note that several studies consistently found that contact from family members led to reduced depressive symptoms, specifically for women. However, as the authors point out, there is little research on the specific role of parent-child relationships in improving mental health outcomes. One exception is Poehlmann et al.’s (2010) review which found that increasing incarcerated parents’ contact with children resulted in lower stress levels and better parent-child relationships for both mothers and fathers.
Another way to mitigate mental health issues is by strengthening existing familial relationships through parent-child contact (De Claire & Dixon, 2017). In-person visitation from children can enhance parental adherence to mental health treatment and frequent in-person visits by children strengthens parent-child bonds, maintains parental roles, reduces stress, and increases self-esteem (Beckmeyer & Arditti, 2014; Thompson & Harm, 2000; Wallace et al., 2016). Engagement in various types of contact also demonstrates an attempt to provide support which can temper mental health concerns during reentry including abating stress, reducing family conflict, and lowering levels of depression (Bales & Mears, 2008; Ekland-Olson et al., 1983; Mowen & Visher, 2015; Wolff & Draine, 2004).
Mental Health as a Barrier to Parent-Child Contacts
It is not clear from the extant literature if parental mental health illness diagnosis is a barrier to various forms of parent-child contact during periods of incarceration. Interestingly, Rubenstein et al. (2021) found that general mental health status is not an obstacle to parent-child in-person visitation, though having a clinical diagnosis of a mental health illness (rather than general feelings of poor mental health) was associated with a significant reduction in parent-child visitation. Some scholars suggest that persons with serious mental health illnesses such as schizophrenia and psychotic disorders are less likely to receive in-person visits (Connor & Tewksbury, 2015; Lahm, 2016; Stacer, 2012). Less is known about other forms of parent-child contact such as phone calls, mail, and email among parents with mental health illness diagnoses.
A mental health illness diagnosis can be stigmatizing and isolating, and separation from children during a period of confinement can further exacerbate symptoms (Crisp et al., 2000; Dargis & Mitchell-Somoza, 2021; Kohn & Clausen, 1955). Separation can also contribute to new mental health symptoms such as depression, self-harm, and suicidal ideation among non-incarcerated persons and people who are incarcerated (Calati et al., 2019; Jablonska & Meek, 2018; Macrynikola et al., 2018). Parent-child contact during incarceration may serve as a counterbalance and benefit parents by alleviating mental health symptoms exacerbated by separation due to parental confinement (Dargis & Mitchell-Somoza, 2021; Poehlmann, 2005).
For children, parent-child contact can help to maintain or improve relationships (see Schubert et al., 2016). However, children may already have strained relationship with parents experiencing mental health illnesses (see Källquist & Salzmann-Erikson, 2019) and in-person visitation may not be in the best interest of the child. While parent-child contact for parents is generally viewed positively, such contact during incarceration can have negative effects on children. For example, children may manifest behavioral and attention problems before and after in-person contact with incarcerated parents (Dallaire et al., 2010; Poehlmann et al., 2008). Children with more frequent parent contact via letters and phone calls experienced fewer internalizing problems (e.g., anxiety, depression), while in-person contact contributed to more internalizing problems (Dallaire et al., 2015). Type of in-person contact may also contribute to child outcomes. Pritzl et al. (2022) found that more frequent visits were associated with lower levels of child externalizing problems (i.e., composite measure, Child Behavior Checklist Externalizing Problem Scale), while visits facilitated through Plexiglass were associated with more externalizing problems. Further, children who had frequent contact (e.g., phone calls, mail, in-person visitation) with their incarcerated parent were more likely to express feelings of role reversal wherein they felt responsible to care for their parent rather than their parent caring for them (Dallaire et al., 2012).
Methodology
Data and Sample
This study used data from the 2016 cross-sectional national Survey of Prison Inmates (SPI) administered by the Bureau of Justice Statistics. SPI included adult (18 years of age and older) men and women incarcerated in state or federal prisons within the United States. SPI provides national statistics on a variety of prisoner characteristics including mental health diagnoses, parent-child contact practices, family background, and relevant demographics. The SPI is primarily an administrative dataset that allows for exploratory research using a large, nationally representative sample of incarcerated adults (see Fox et al., 2018; Glaze, 2019). For the current study, we draw on the subset of participants who were parents at the time of survey administration (N = 8,070).
Measures
Dependent Variables
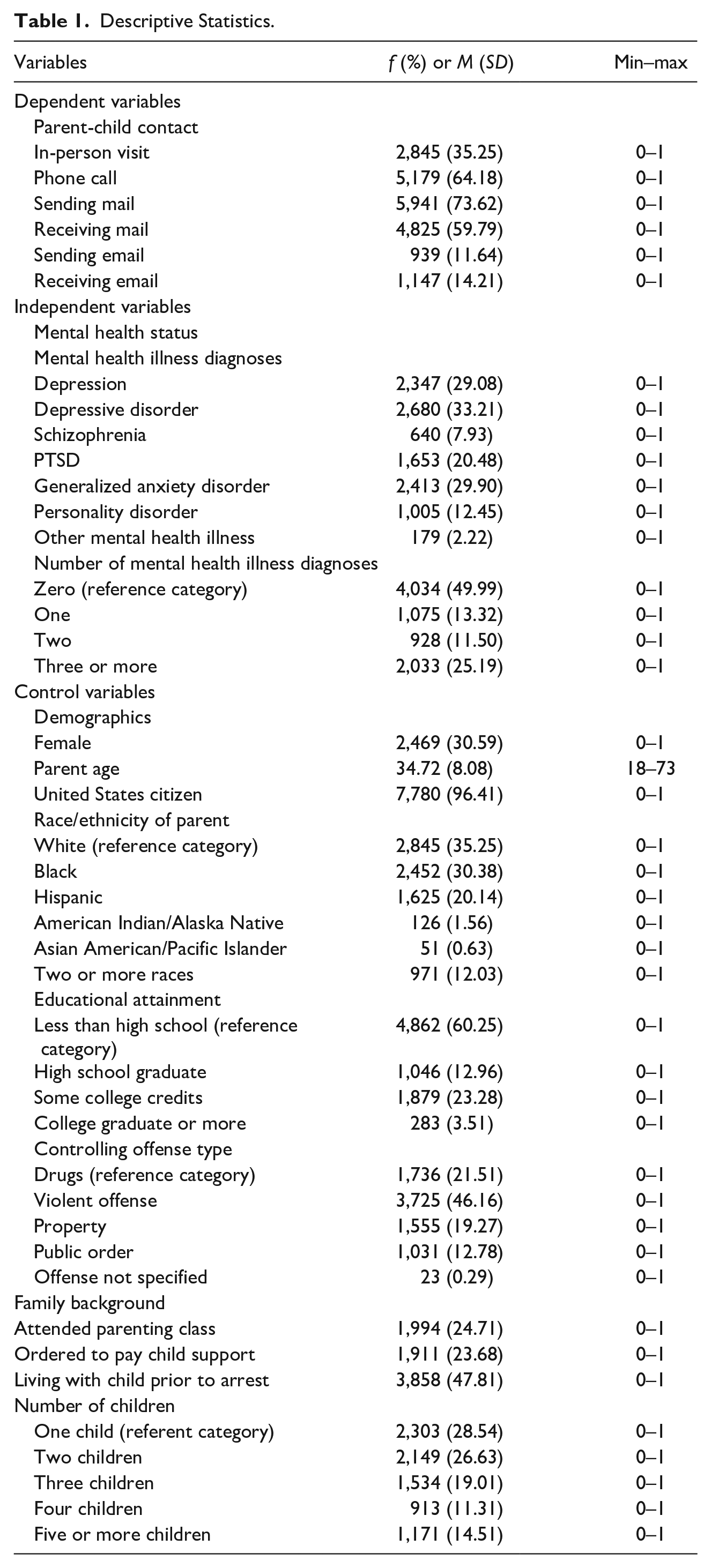
We examined six different types of parent-child contacts: in-person visit, phone call, sending mail, receiving mail, sending email, and receiving email. Each of these dependent variables are coded dichotomously (0 = no, 1 = yes), where “1” means that the incarcerated parent experienced a specific type of contact at least once in the past 12 months. About 35% of the respondents had at least one in-person visit with their children in the past year. The most frequent form of parent-child contact was the parent sending mail to their children (73.62%), followed by phone calls (64.18%), whereas the least frequent form of contact was parent sending (11.64%) or receiving (14.21%) email (see Table 1 for all descriptive statistics).
Descriptive Statistics.
Independent Variables
Consistent with prior research, we generated a series of binary variables (0 = no, 1 = yes) for individuals who reported a clinical mental health illness diagnosis (see Houser et al., 2012; Kopak & Smith-Ruiz, 2014; Rubenstein et al., 2021; Wood & Buttaro, 2013). 1 These dichotomous variables included diagnoses for depression (29.08%), depressive disorder (33.21%), schizophrenia (7.93%), post-traumatic stress disorder (PTSD) (12.45%), generalized anxiety disorder (29.90%), personality disorder (12.45%), and any other mental health illness diagnosis (2.22%).
We also created a categorical variable for individuals with one or more mental health illness diagnosis. An additive scale was used to categorize parents into those with zero mental health illness diagnoses (reference group) and those with one (13.32%), two (11.50%), or three or more (25.19%) diagnoses. About half of the sample (49.99%) did not report any mental health illness diagnosis.
Control Variables
Control variables included respondent demographics: sex, age, citizenship status, race/ethnicity, educational attainment, and offense type. Sex was coded as male = 0 and female = 1. About 31% of the sample was female. Current age was measured as a continuous variable and respondents were, on average, 34.7 years old. United States citizenship status was coded as a binary measure (0 = no, 1 = yes); 96.4% of respondents were United States citizens. Race/ethnicity was measured as White (35.25%; reference group), Black (30.38%), Hispanic (20.14%), American Indian/Alaska Native (1.56%), Asian (0.63%), and two or more races (12.03%). Educational attainment was measured as a categorical variable. Most respondents had less than a high school education (60.25%; reference group), about 13% were high school graduates while almost a quarter attended some college (23.28%), and a few had graduated from college (3.51%). Controlling offense type was measured as drug (21.51%; reference group), violent offenses (46.16%), property (19.27%), public order (12.78%), and offense not specified (0.29%).
We also included relevant variables describing the respondent’s family background. Whether an incarcerated parent attended any parenting classes in prison was treated as a dichotomous variable (0 = no, 1 = yes). Almost a quarter (24.71%) of respondents reported participation in parenting classes while incarcerated. A binary variable (0 = no, 1 = yes) was created to denote if an incarcerated parent was ordered to pay child support, with 23.68% of the sample reporting this as a requirement. We also included whether the incarcerated parent was living with any of their children prior to their arrest for which they are serving time (0 = no, 1 = yes), and less than half (47.81%) reported living in the same household. In the original dataset, respondents’ number of children ranged from 1 to 19. Due to the skewness of the continuous variable, a categorical variable was created to denote each respondents’ number of children: one (28.54%; reference group), two (26.63%), three (19.01%), four (11.31%), or five or more (14.51%) children.
Analytical Approach
We employed a series of multivariate logistic regression models to analyze associations between mental health illness diagnoses and six types of parent-child contact. Before finalizing each multivariate model, we ran AIC (Akaike Information Criterion) and BIC (Bayesian Information Criterion) goodness of fit tests, and report results from models with lower AIC and BIC scores which suggest better model fit. 2
Results
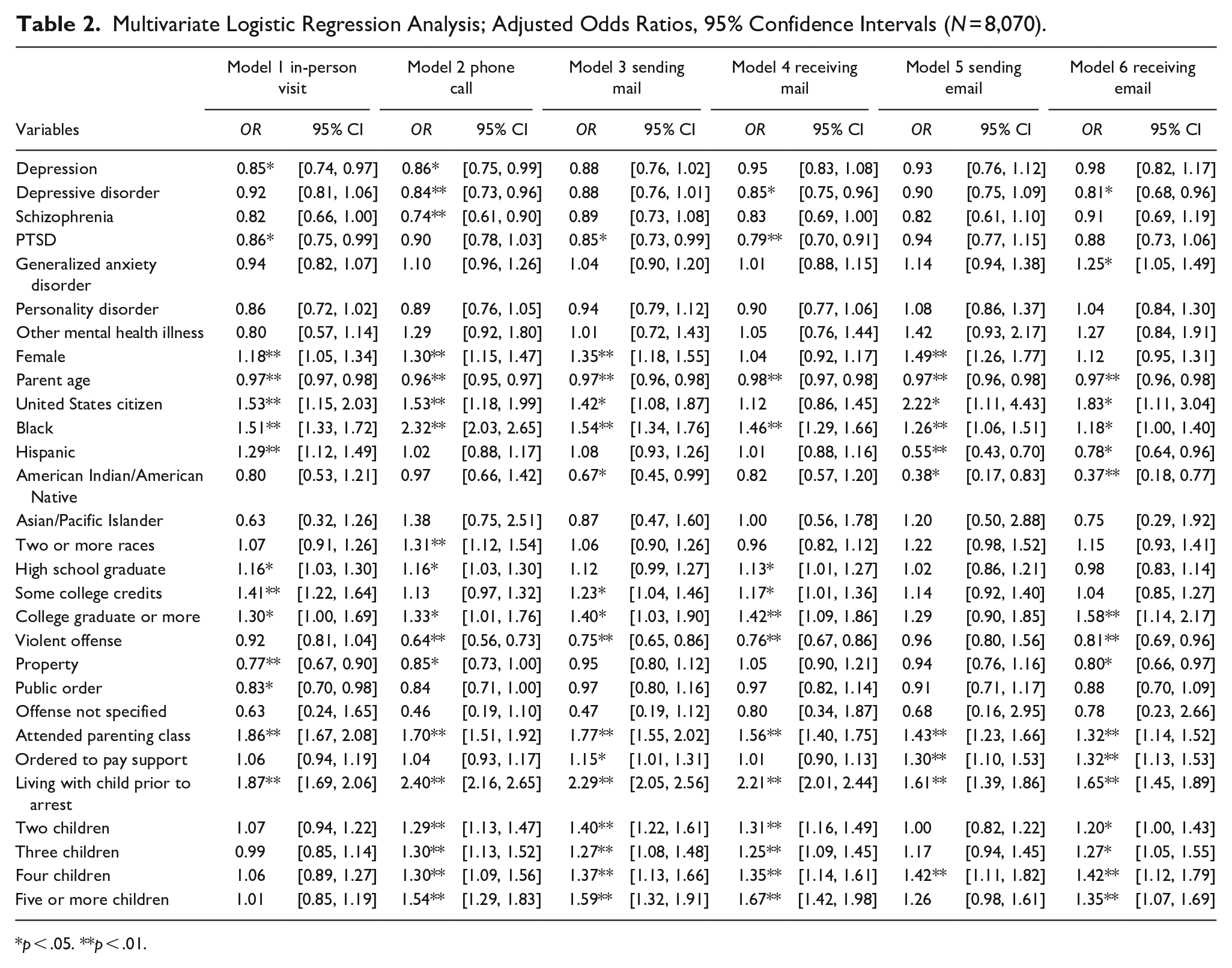
Table 2 presents multivariate logistic regression models assessing predictors of parent-child contact modalities. In-person visits were 15% less likely among parents with depression (OR = 0.85, p < .05) and 14% less likely among parents with PTSD (OR = 0.86, p < .05). Phone calls were 14% less likely among parents with depression (OR = 0.86, p < .05), 16% less likely among those with depressive disorder (OR = 0.84, p < .01), and 26% less likely among parents with schizophrenia (OR = 0.74, p < .01). Only parents with a PTSD diagnosis were significantly less likely to send mail to their children (OR = 0.85, p < .05). Parents were 15% and 21% less likely to receive mail from their children if they were diagnosed with depressive disorder (OR = 0.85, p < .05) or PTSD (OR = 0.79, p < .01), respectively. A parent’s mental health illness diagnosis did not influence the likelihood of sending their children emails. However, those who were diagnosed with depressive disorder were 19% less likely to receive email (OR = 0.81, p < .05) while parents with generalized anxiety disorder were 25% more likely to receive email from their children (OR = 1.25, p < .05).
Multivariate Logistic Regression Analysis; Adjusted Odds Ratios, 95% Confidence Intervals (N = 8,070).
p < .05. **p < .01.
Women were significantly more likely than men to experience four forms of parent-child contact. Mothers were 18% more likely to have in-person visits (OR = 1.18, p < .01), 30% more likely to have phone calls (OR = 1.30, p < .01), 35% more likely to send their children mail (OR = 1.35, p < .01), and 49% more likely to send emails (OR = 1.49, p < .01). There were no significant differences in mothers and fathers receiving mail and email from children. Parent age was inversely related to all forms of contact; with each yearly increase in parent’s age, there was a 2% to 4% decrease in likelihood of experiencing a parent-child contact modality. Incarcerated parents who were United States citizens were more likely to experience five of the six forms of parent-child contact compared to non-citizens. There was no statistically significant difference in receiving mail for citizens compared to non-citizens.
Black parents were significantly more likely to experience all six forms of parent-child contact than White parents. Hispanic parents were 29% more likely than White parents to have in-person visits with their children (OR = 1.29, p < .01). However, Hispanic parents were 45% less likely to send email (OR = 0.55, p < .01) and 22% less likely to receive email (OR = 0.78, p < .05), relative to White parents. American Indian/American Native parents were 33% less likely than White parents to send mail (OR = 0.67, p < .05), 62% less likely to send email (OR = 0.38, p < .05), and 63% less likely to receive email (OR = 0.37, p < .01) from their children.
Compared to parents who did not graduate from high school, high school graduates were 16% more likely to have in-person visits and phone calls with their children (OR = 1.16, p < .05). High school graduates were also 13% more likely than parents who did not graduate from high school to receive mail from their children (OR = 1.13, p < .05). Parents who attended college but did not graduate were 41% more likely to receive in-person visits (OR = 1.41, p < .01), 23% more likely to send mail (OR = 1.23, p < .05), and 17% more likely to receive mail (OR = 1.17, p < .05). College graduates were significantly more likely to experience five of the six parent-child contact modalities; sending emails did not reach statistical significance.
Compared to those with a drug controlling offense, parents with violent offenses were significantly less likely to make phone calls (OR = 0.64, p < .01), send mail (OR = 0.75, p < .01), receive mail (OR = 0.76, p < .01), or receive email (OR = 0.81, p < .01). Parents incarcerated for property offenses were 23% less likely to receive in-person visits with their children (OR = 0.77, p < .01), 15% less likely to have phone calls with their children (OR = 0.85, p < .05), and 20% less likely to receive email (OR = 0.80, p < .05). Parents incarcerated for public order offenses were 17% less likely to receive in-person visits, compared to drug offenders (OR = 0.83, p < .05).
Turning now to family background variables, the likelihood of all six forms of parent-child contact was significantly higher for those who engaged in parenting classes while incarcerated. Parenting classes increased in-person visits by 86% (OR = 1.86, p < .01), phone calls by 70% (OR = 1.70, p < .01), sending mail by 77% (OR = 1.70, p < .01), receiving mail by 56% (OR = 1.56, p < .01), sending email by 43% (OR = 1.43, p < .01), and receiving email by 32% (OR = 1.32, p < .01). Parents who were ordered to pay child support were significantly more likely to send mail (OR = 1.15, p < .05) and emails (OR = 1.30, p < .01), and receive emails (OR = 1.32, p < .01). Parents who were living with their children prior to their arrest had significantly greater odds of all forms of contact. Having more than one child was not associated with a greater likelihood of in-person visits. However, incarcerated parents with a greater number of children were significantly more likely to make phone calls, send mail, receive mail, send email (four children only), and receive email.
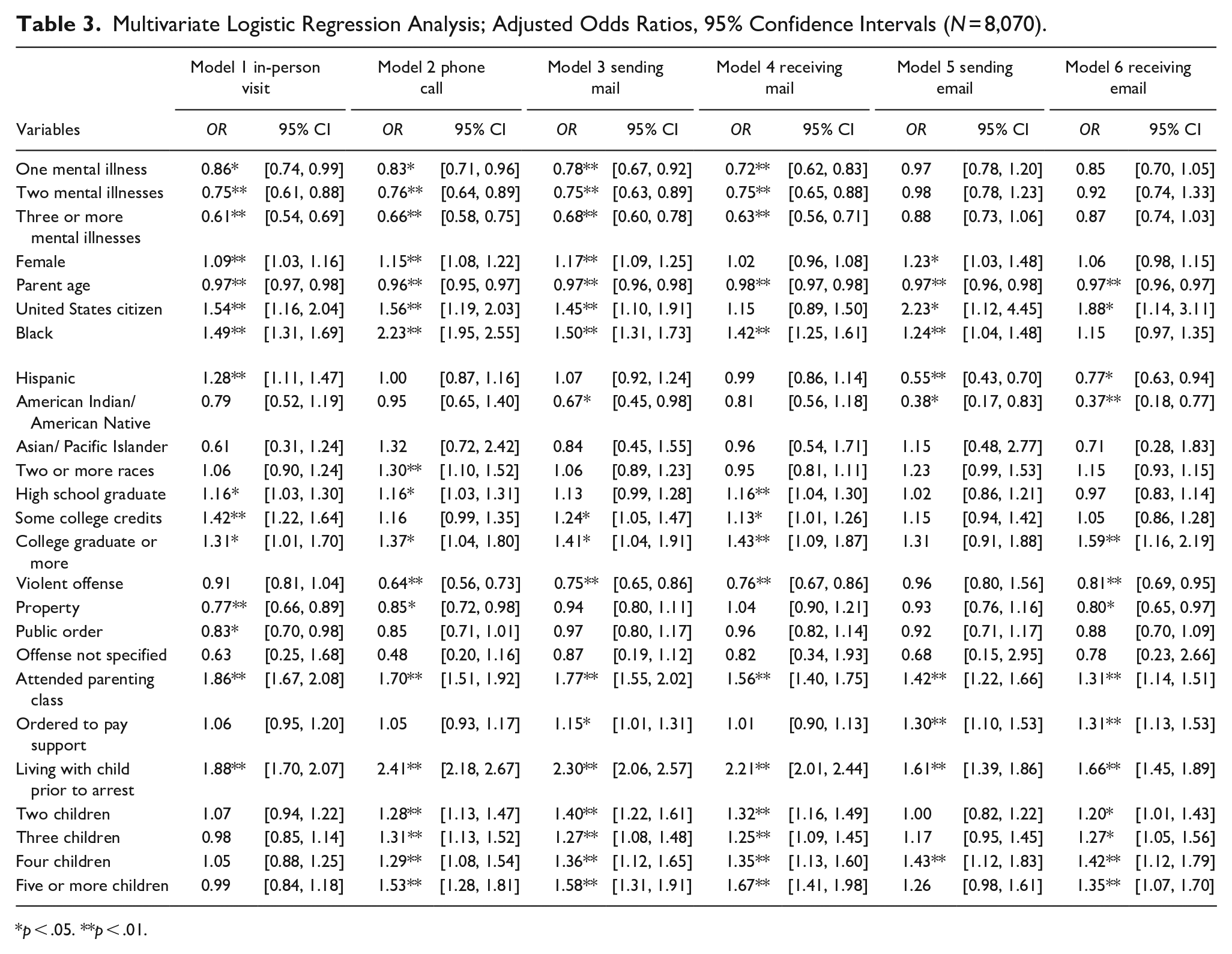
Table 3 presents results from the logistic regression models to assess differences in parent-child contact among parents with multiple mental health illness diagnoses. Compared to parents without a mental health illness diagnosis, persons with one mental health illness diagnosis were 14% less likely to receive in-person visits (OR = 0.86, p < .05), 17% less likely to have phone calls (OR = 0.83, p < .01), 22% less likely to send mail to children (OR = 0.78, p < .01), and 28% less likely to receive mail from children (OR = 0.72, p < .01). Persons with two mental health illness diagnoses were 25% less likely to receive in-person visits (OR = 0.75, p < .01), 24% less likely to have phone calls (OR = 0.76, p < .01), 25% less likely to send mail to children (OR = 0.75, p < .01), and 25% less likely to receive mail from children (OR = 0.75, p < .01). Likewise, incarcerated parents with three or more mental health illness diagnoses were 39% less likely to receive in-person visits (OR = 0.61, p < .01), 34% less likely to have phone calls (OR = 0.66, p < .01), 32% less likely to send mail to children (OR = 0.68, p < .01), and 37% less likely to receive mail from children (OR = 0.63, p < .01).
Multivariate Logistic Regression Analysis; Adjusted Odds Ratios, 95% Confidence Intervals (N = 8,070).
p < .05. **p < .01.
Results of models specifying number of mental health illness diagnoses reflect the findings from the models in Table 2 which specified mental health illness diagnoses. Once again, women were more likely to experience four types of parent-child contact relative to men: in-person visits (OR = 1.09, p < .01), phone calls (OR = 1.15, p < .01), sending mail (OR = 1.17, p < .01), and sending email (OR = 1.23, p < .05). Older parents were less likely to experience all parent-child contact modalities. United States citizens were more likely than non-citizens to experience most contacts, except receiving mail. When controlling for the amplified effect of number of mental health illness diagnoses, Black parents were significantly more likely than White parents to experience contact with their children—except in the case of receiving email. Those who participated in parenting classes were significantly more likely to experience all forms of contact with their children. Likewise, those who were living with their children prior to their arrest also had higher odds of all six types of contact with their children while incarcerated.
Discussion
Incarceration policies in the United States have resulted in many parents with mental health illness diagnoses being sent to prisons and separated from their children (Glaze & Maruschak, 2008). In prison, day-to-day parent-child interactions are removed, and contacts are bound by institutional rules and practices. Positive parent-child contacts during periods of incarceration are important to foster parent-child relationships which are critical for child development and parent success both in and out of the facility (De Claire & Dixon, 2017; Poehlmann et al., 2010). Our study contributes to the understanding of a broad range of parent-child contacts by concentrating on parents with a mental health illness diagnosis.
Consistent with other research, like that of Stacer (2012), our study finds that incarcerated individuals with specific mental health illnesses have lower odds of in-person visitation during incarceration. For example, parents with depression in our study were significantly less likely to have visits with their children. Depression may negatively affect parent-child relationships through weaker attachments (see Manning & Gregoire, 2006) and in-person visits may not have positive outcomes, reducing their desirability as a means of contact. As noted by Turanovic and Tasca (2019), individuals who suffer from depressive symptoms respond more negatively (e.g., arguments, stress, guilt, sadness) to in-person visits increasing the importance of fostering the use of other parent-child contact modalities. However, in our study, parents with depression or depressive disorder were also less likely to connect with their children through phone calls (depression and depressive disorder) or by receiving mail or email (depressive disorder only). This suggests that facilities need to aid parents in developing communication skills to reduce conflict and support parents as they process interactions after contact with their children.
Our findings also show that parents with a PTSD diagnosis were less likely to receive in-person visits with their children and send or receive mail. A lack of contact could be the result of PTSD effects on detachment towards children (see Ruscio et al., 2002). However, this finding contrasts with a recent study which found a positive relationship between PTSD and in-person visits among a veteran inmate population (Logan et al., 2021). It would be interesting for future research to explore whether there are parent-child contact differences for veterans with PTSD compared to non-veterans.
Interestingly, only one mental health illness diagnosis showed a positive relationship among the six parent-child contact modalities. Parents with generalized anxiety disorder were significantly more likely to receive email from their child(ren). Generalized anxiety disorder is more likely to run in families (see Aktar et al., 2017) and it is possible that children whose parents have generalized anxiety disorders also present with this mental health illness. Children may send emails to their parents to assuage their own discomfort with having a parent incarcerated as having a parent processed by the criminal justice system and removed from the home can be an anxiety provoking experience (Murray & Murray, 2010). Maintaining even limited contact could provide some symptom relief to both parent and child. Additional work is needed to understand why other forms of parent-child contact such as sending and receiving mail among parents with generalized anxiety disorder do not reach statistical significance.
We also examined the amplified effects of multiple mental health illness diagnoses on parent-child contact. Incarcerated parents with three or more diagnosed mental illnesses were the least likely to have any form of contact with their children—in-person visits, phone calls, sending or receiving mail, and sending or receiving email. While the prison experience can be isolating for individuals without medical complications, these results suggest that having multiple mental health illnesses may further isolate incarcerated parents from their children. Not all types of contacts may be welcome or beneficial; for example, parent-child in-person visitation may add another layer of hardship to the incarceration experience (Houck & Loper, 2002), especially for those managing multiple mental health diagnoses.
We also found evidence that parent demographics conditioned all six parent-child contact modalities. Women in our study were more likely than men to maintain most forms of parent-child contact (see also Cochran et al., 2017). This is not surprising given that at their time of incarceration women are more often caregivers of children (Cobbina & Bender, 2012; Shlafer & Poehlmann, 2010; Tasca et al., 2016). Results also show that older parents are significantly less likely to have any type of contact with their children. Older parents may have less contact with their children who are more likely to have matured beyond dependence or become estranged (Western et al., 2015; see also Cochran et al., 2017).
One surprising finding was the higher odds of almost all forms of parent-child contact among Black parents compared to White parents. This finding conflicts with prior literature suggesting fewer resources among families of color to travel great distances to prisons or pay for phone calls (J. Christian, 2005; Cochran et al., 2017). The finding is consistent, however, with research suggesting that, “Just as incarceration has become a normal life event for disadvantaged young Black men, parental incarceration has become commonplace for their children” (Western & Wildeman, 2009, p. 235). Instead of shielding children from the carceral experience, Black families may proactively work to maintain social connections through parent-child contact. Similarly, Hispanic parents were more likely than White parents to receive in-person visits perhaps due to cultural expectations surrounding the importance of family (Stacer, 2012).
Consistent with prior research, parents convicted of more serious offenses had fewer contacts while incarcerated (see Gibson & Krohn, 2013). More contextual information about factors such as family dynamics, barriers to parent-child contact, and geographic location of children compared to the prison would help establish a greater degree of accuracy to understand why there is less contact, though presumably these parents are in prison for a longer time perhaps weakening social connections.
Our findings also show that participation in parenting classes was associated with a significant increase in the likelihood of all six parent-child contact modalities. Parenting classes provide guidance on how to maintain contact with children and improve parenting effectiveness, even while the parent is incarcerated (Loper & Tuerk, 2011). These results should be interpreted with caution; it is not clear if the parenting programs were mandatory, recommended, or voluntary for participants in the current study. Understanding parents’ motivation to participate in such a program could provide further nuance into assessing their influence on parent-child contact practices and offer ways to increase program participation among parents with mental health illness diagnoses. Parenting classes may also serve a different function for older parents whose adult children could provide social supports and aid reentry efforts in a different way than dependent children.
Requiring the payment of child support was associated with sending mail, as well as email, initiated by both parents and children. This finding may indicate a vested interest on behalf of the parent to maintain contact and demonstrate a traceable presence in their child’s life. Persons providing child support may be ordered to do so as part of a divorce settlement and the mode of parent-child contact may depend on the relationship between the parents. Email may also simply be a preferred form of communication in an increasingly digital landscape.
Finally, parents who were living with their children prior to arrest were also significantly more likely to engage in all forms of contact while incarcerated. It could be that these children have strong social bonds to their parents and therefore are willing to initiate and maintain contact during incarceration (Cochran, 2012; Mitchell et al., 2016). Quality relationships prior to periods of incarceration can also increase the likelihood of visitation (see Atkin-Plunk & Armstrong, 2018).
Policy and Program Implications
A key practical implication of this study would be to strengthen programming aimed at providing increased support for those parents with mental health illness diagnoses. Generally, practitioners should consider how parent-child engagement can be increased during parental incarceration. However, not all contacts are welcomed or positive experiences. Negative experiences can worsen mental health conditions (see Baker et al., 2022). Thus, practitioners should consider how they can facilitate supportive parent-child contacts. Community-based programs that target parenting efficacy and family functioning have demonstrated some success though they have not been adequately tested in carceral situations (see Suarez et al., 2016). The results of this study indicate parents with multiple mental health illnesses also engage in fewer parent-child contacts suggesting additional support is needed to facilitate positive parent-child relationships and reduce stressors associated with incarceration (see Milavetz et al., 2021). Promising programs such as Parenting Inside Out offer a multimodal approach to developing parenting skills within the context of challenges faced by correctional populations (see Eddy et al., 2013, 2019).
Secondly, parenting classes aimed at improving men’s identity as a father and how they can parent from prison are important first steps to increasing father-child contacts (see Arditti et al., 2005). Programming also needs to be sensitive to the needs of fathers versus those of mothers and should consider race and ethnic differences in parenting practices (Antunes & Ahlin, 2021). While it has been well established that men and women take different pathways to prison, correctional facilities have not fully identified treatment modalities that best fit the needs of men versus those of women, especially for parents (Hoffmann et al., 2010). While women experiencing incarceration often have greater access to gender-informed treatments and programs, additional work is needed to provide prenatal and parenting programming to fathers and develop curricula that embrace parenting differences between mothers and fathers (see Palkovitz et al., 2014).
Thirdly, a focus on parent-child programming that incorporates support for the children who face the dual complexities of having an incarcerated parent with a mental health illness is imperative. Prisons should consider implementing extended visitation and expanding in-prison parenting programs to help children and their parents maintain a relationship during periods of incarceration. Schubert et al. (2016) evaluated an extended child-centered visitation program that had more flexible rules (e.g., physical contact), offered structured activities, and was longer than traditional visitation. Their investigation showed both mothers and children preferred this program to normal visitation. Additional research is needed to discern if the enhanced visitation programs come with positive experiences for both parties beyond satisfaction and whether such programs can improve parent-child contact for those diagnosed with mental health illnesses and fathers.
Finally, various correctional policies could enhance parental engagement with their children. Our findings indicate that mental health illnesses were not a barrier to parents sending emails to their children. However, access to the digital landscape is not uniform across correctional facilities. Policies aimed at increasing electronic access and enhancing digital literacy could facilitate electronic parent-child contacts and could also contribute to skill development needed for reentry (McDougall et al., 2017; Reisdorf et al., 2022). Analogously, access to electronic messaging systems is often monetized and only available to those who can afford to pay associated fees (Katzenstein & Waller, 2015). Policies reducing or eliminating the costs of electronic based parent-child contacts could mitigate some of the financial barriers to in-person visitation (J. Christian, 2005).
Limitations and Future Directions
The administrative nature of the data used in the current study does not provide detailed information about the parent-child relationship or ability to engage in the six parent-child contact modalities. For instance, economic disadvantage and distance between the prison and home may prevent some parents from receiving in-person visits with their children (see Clark & Duwe, 2017; Rubenstein et al., 2021; Tewksbury & DeMichele, 2005). Despite positive mental health benefits of visitation (de Motte et al., 2012), less than half of incarcerated parents receive in-person visits from their children (see also Roxburgh & Fitch, 2014). In-person visits, specifically, may be limited when incarcerated parents are unwilling to meet with their children because they wish to keep their children away from the criminal justice system (McLeod & Bonsu, 2018). Similarly, children may be unwilling to maintain contact with their parents (Beckmeyer & Arditti, 2014; Shlafer & Poehlmann, 2010), especially when parents are experiencing severe mental health issues. A natural progression of this work is to analyze parent-child relationships prior to prison; data were not available on this important factor which could influence parent-child contacts. As noted, parents with mental health illnesses may have strained relationships with their children, which can impact children into adulthood (see Källquist & Salzmann-Erikson, 2019).
It is also imperative that future studies examine facility capabilities as each prison has different technological advances, rules, and costs surrounding its use and visitation and mail policies are not uniform across prisons. Further studies also need to be carried out to validate these findings. Our study relied on administrative self-report data for the categorization of mental health illness diagnosis. The rate of mental health illness may in fact be higher if medical diagnoses are pending, persons report inaccurately or do not wish to disclose their medical history, or their symptoms have not risen to the level that would bring a mental health illness to the attention of the prison medical team. Additional research is needed to investigate the generalizability of results in other detention-based populations, including persons housed in jails. Despite these limitations, “[a]dministrative data may. . . be helpful to researchers who want to place their own data collection in the context of the larger population they are studying” (Fox et al., 2018, p. 56). Administrative data can be a cost-effective approach for exploratory research and provide access to a large, nationally representative sample of adults incarcerated in state prisons (see Fox et al., 2018; Glaze, 2019).
Conclusion
Despite its exploratory nature, this study offers some insight into parent-child contact practices among prisoners with mental health illness diagnoses. While the prison experience can be isolating for persons without medical complications, our results suggest that having mental health illnesses can amplify parent-children separation during periods of incarceration. Additional work is needed to understand how mental health illness diagnoses differentially impact parents and children in their ability or desire to maintain contact.
Moreover, in a time of fiscal austerity, there is little to suggest that mental health care offerings in correctional facilities will change considerably soon. Facilities need to leverage and enhance existing programs and policies that can improve the mental health of residents, in general, and those who have mental health illness diagnoses, more specifically. Improving parent-child relations are positive and low-cost methods to ease mental health illness symptoms, improve reentry prospects, and aid prison management. The study also raises important questions about the effects of parenting programs on parent-child contact and especially for those who suffer from mental health problems.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.