
Abstract
We investigated whether vitamin-mineral supplementation could reduce serious rule violations. In this randomized, controlled, double-blind trial, young adult male inmates were included. For 15 weeks, they received a daily dose with vitamin-mineral supplements of approximately 100% Recommended Dietary Allowance (RDA) (n = 149), or a higher-dose formula (n = 150), or placebo (n = 150). Serious rule violations were the primary outcome. In the lower-dose group there were 39% fewer rule violations than in the placebo group (relative risk = .61; 95% confidence interval [CI]:.41–.90, p = .01). In the higher-dose group the difference did not reach statistical significance. About 100% RDA, but not higher doses supplements, resulted in less serious rule violations than placebo.
Introduction
Rule violation is a major problem in correctional facilities in the U.S., with about 946 incidents per 1,000 inmates per year (Steiner & Cain, 2016, p. 166). About half of the prison inmates violate at least one prison rule each year (Steiner & Cain, 2016, p. 167). The consequences of institutional misconduct are costly, and research has been done to determine what works to reduce this misconduct. Variables concerning both prisoner and prison characteristics predict inmate misconduct and include age <25, crowding, and prison security level (Steiner et al., 2014). Cognitive-behavioral therapy and social learning approaches are among the most studied interventions and have shown mixed results (Auty et al., 2017). In a meta-analysis on the effectiveness of correctional treatment for reducing institutional misconducts, a well designed randomized controlled trial (RCT) with dietary supplements received attention (French & Gendreau, 2006). This RCT showed tentative evidence of a beneficial effect compared to placebo, as vitamin-mineral supplements reduced institutional misconduct.
Three RCTs on the effect of vitamin-mineral supplements on institutional misconduct have been published so far. The first study was a randomized, placebo-controlled trial among 62 delinquents in a maximum-security psychiatric center in Oklahoma (Schoenthaler et al., 1997). The delinquents who took vitamin-mineral supplements for 3 months showed 28% fewer rule infractions than those randomized to placebo (95% CI: 15%–41%, p = .005). This study was adjusted and replicated in 231 young adult male prisoners in the United Kingdom. Those on active supplements showed 26% fewer offenses than those randomized to placebo (95% CI: 8.3%–44.3%, p = .03) (Gesch et al., 2002). Similarly, in 221 young adult male prisoners, there was a reduction of 48% offenses in the active versus placebo group (p = .017, one-tailed) (Zaalberg et al., 2010). An association between healthier nutrition and lower misconduct was also found in open-label studies with a change of prison diet as the intervention (Schoenthaler, 1985), and in observational studies (Schoenthaler et al., 1991). All RCTs showed small to medium effect sizes in favor of the vitamin-mineral supplements, without any excess of adverse effects.
There is no monocausal relation between micronutrients and behavior, but results from numerous studies have shown that an adequate supply of vitamins and minerals is essential for the functioning of the central nervous system (CNS) (Parletta et al., 2013). A sub-optimally functioning CNS can play an important role in the complex interplay of bio-psycho-social and environmental factors that predispose social problem behavior (Jackson & Beaver, 2013; Lee, 2015). For example, imbalances in the monoaminergic neurotransmitter systems can adversely affect executive functions, including self-control (Logue & Gould, 2014). There are multiple mechanisms of action by which vitamins and minerals can influence the CNS, including neurotransmitter synthesis, energy provision, neuroprotection, neuroplasticity, and neurogenesis (Calderon-Ospina & Nava-Mesa, 2020; Kennedy, 2016; Parletta et al., 2013). Vitamins and minerals have complex synergetic actions; therefore, it is not rational to focus on the effect of one isolated micronutrient (Messina et al., 2001), but rather on the combined effect of micronutrients. For practical reasons, vitamin-mineral supplements are used as a proxy for meals with a healthy combination of micronutrients to study the effect of nutrition on behavior.
This study aimed to assess the effect of two different formulas and doses of multi-vitamin and mineral supplements versus placebo on serious rule violating behavior in two California Youth Authority (CYA) institutions. The study was designed as a three-arm randomized, double-blind placebo-controlled trial. One active arm contained approximately 100% of the RDA for vitamins and minerals (i.e., the lower-dose group), and the other (i.e., higher-dose group) received higher doses of vitamins B and C and some additional minerals. We hypothesized that the number of serious rule violations would be lower in the lower-dose group versus the placebo group and that this effect would be more substantial in the higher-dose group versus the placebo group.
Methods
An Oversight Committee appointed by the Chancellor of the University of California Berkeley supervised the procedures. Recruitment and informed consent took place from September 1990 to June 1991 after approval by the California State University, Stanislaus Institutional Review Board (IRB).
Sample
Within the two participating institutions of the CYA, all prisoners aged 17 to 24 were eligible and were approached for participation by the researcher assistants. Four hundred forty-nine male inmates entered the trial after giving informed consent. The participants were housed in 21 residential units. Details of the recruitment and allocation are shown in the flowchart in Figure 1. To compare 3 group means, with a 5% type I error rate and an effect size of d = .20, 120 subjects per group would be required to have 90% statistical power (Faul et al., 2007). Since we expected that approximately 15% of subjects would be lost “due to release,” efforts were made to recruit 150 subjects per group.
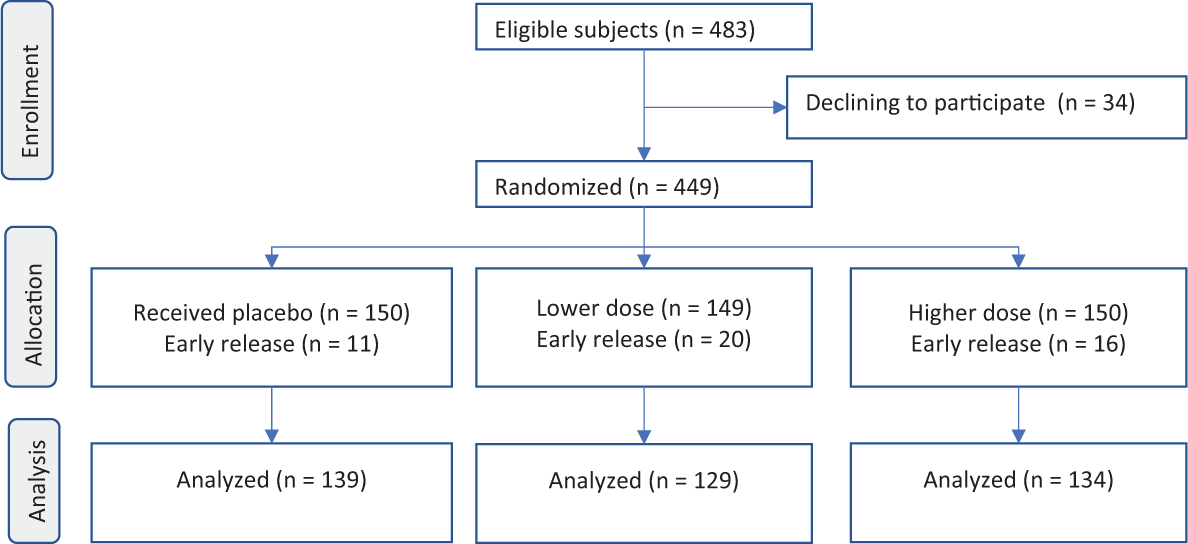
Flow diagram.
Intervention
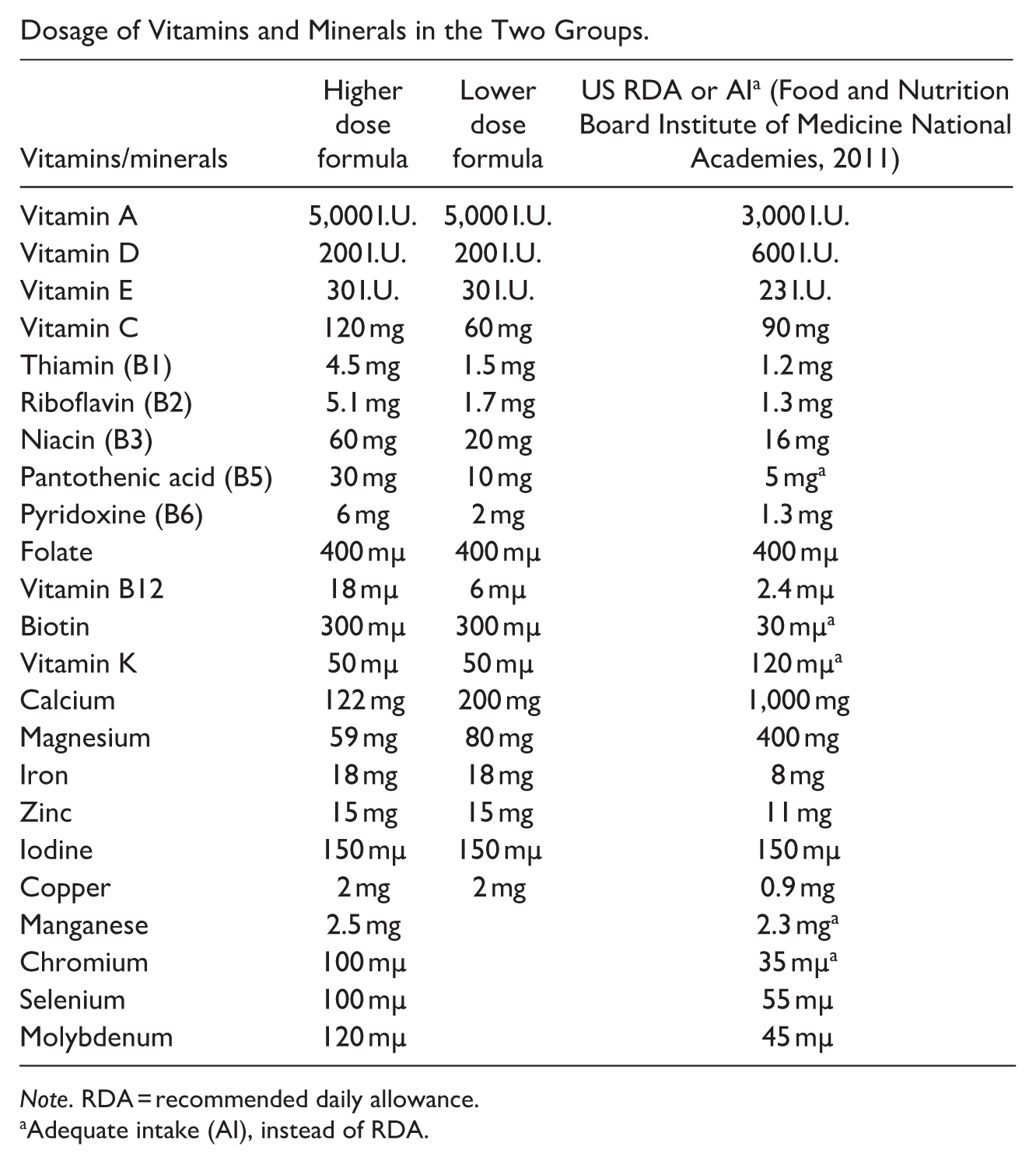
The effect of two different doses of vitamin-mineral supplements and placebos on rule violating behavior was investigated. Booker Nutritional Products Ltd. made the supplements and placebos, of which one active supplement contained approximately 100% of the US RDA for most of the vitamins and minerals; we call this the “lower-dose supplement.” The “higher-dose supplement” had the same amount of vitamin A, D, E, K, Folic acid, Biotin, Copper, Iodine, Iron, and Zinc, but had a higher dose of the water-soluble B and C vitamins and addition of Selenium, Chromium, Manganese, and Molybdenum. In contrary to the other minerals, the dose of Magnesium and Calcium was higher in the lower-dose supplement. The dosages are listed in the supplementary of Appendix 1. We added the most recent US RDAs to the table, because the RDA of some micronutrients changed since 1990. The supplements were delivered in coded boxes, of which the key was held by the oversight committee. The randomization table was generated from a list of randomized numbers published in Social Statistics (Blalock, 1972). Using this table, the research assistants sequentially assigned each participant to a code. During the 15-week intervention period, the participants received their daily supplement from the research assistants who registered compliance. Baseline intervention incident rates were measured from 15 weeks before the start of the intervention. The post-testing measurements took place during the last week of the intervention.
Outcome
Correctional facilities distinguish between serious and less serious rule violations. Serious violations include, for example, the use of violence against another person, hazard to facility security, and serious disruption of facility operations (15 CCR 3315). Less serious misconduct includes misuse of food, vulgar or obscene language, and failure to meet work or program expectations (15 CCR 3314). The primary outcome was the difference between the assignment groups in the sum of all registered serious rule violations committed by the prisoners during the 15-week intervention period. Participants who were paroled, released, or transferred within 6 weeks from the start of the intervention were excluded. Subsequently, we made a distinction between violent and non-violent offenses.
Questionnaires
The secondary outcome was the change in Total Mood Disturbance during the intervention period measured with the Profile of Mood States (POMS) (McNair et al., 1971). The POMS is a self-report questionnaire with 65 questions on a 5-point Likert scale ranging from “not at all” to “extremely.” It measures six dimensions of mood states: Tension, Anger, Vigor, Fatigue, Depression, and Confusion. The Total Mood Disturbance is calculated with the formula: (Tension + Depression + Anger + Fatigue + Confusion + (32—Vigor)). The psychometric qualities of the POMS are reasonable, with Cronbach’s alphas on the subscales; .90 (Tension), .92 (Anger), 95 (Depression), 93 (Vigor), .93 (Fatigue), .81 (Confusion), and .92 (Total Mood Disturbance), the reliability of the scale is good (Curran et al., 1995).
To measure personality traits, we used the Eysenck Personality Questionnaire revised version (EPQ-r) (Eysenck et al., 1985). It is a self-report scale with 94 items that measure four dimensions of personality: Extraversion, Neuroticism, Psychoticism, and Lie. The reliability of the scale varies with the dimensions measured with lower reliability for the dimensions Psychoticism (.66) and Lie (.77) than Extraversion (.82) and Neuroticism (.83) (Caruso et al., 2001).
We measured the Intelligence quotient (IQ) with the non-verbal subset of the revised Wechsler Adult Intelligence Scale (WAIS-R) consisting of “picture completion,” “picture arrangement,” “block design,” “object assembly,” and “coding.” Among a prison population, the non-verbal subset of the WAIS-R is preferable because verbal items could cause bias (Jensen & Faulstich, 1988).
Blood Analysis
Blood samples were analyzed at baseline and in the last week of the trial. Blood values were measured for vitamins A, B1, B2, B3, B5, B6, and E, folic acid, iron, chromium, calcium, manganese, copper, selenium, zinc, and magnesium. Vitamins were assayed using micro-protozoan growth techniques (Voigt & Eitenmiller, 1978) and minerals with atomic absorption spectrometry.
Adverse Effects
The interventions consisted of a placebo or one of two over-the-counter supplements for which no serious side effects were expected. In order not to worry the participants unnecessarily, there was no active assessment of side effects.
Statistical Analyses
The primary hypothesis was that the count of serious rule violations in the intervention period was lower in the two treatment groups than in the placebo group. Because the primary outcome measure was count data, and there was evidence of overdispersion, we used a negative binomial distribution for the primary analysis (Hilbe, 2014). We incorporated as an offset variable into the analysis the logarithm of the subject’s number of days at-risk during the intervention. The dependent variable was the sum of the incidents during the experimental period, and treatment assignment was the grouping variable. A zero-inflated model was fitted to compare the effects on rule violations among the randomized groups. This model was compared to the negative binomial model using the Vuong test (Desmarais & Harden, 2013). A post hoc analysis was used to explore whether the effect would be more robust in a violent and non-violent fraction.
The secondary outcome was the effect of the intervention on the mood states. The difference on Total Mood Disturbance score was used as dependent variables, and treatment as the grouping variable. These variables were analyzed using a analyses of variance (ANOVA) model.
In addition, change from baseline to endpoint on total non-verbal IQ, and the four dimensions of EPQ-r were explored using ANOVA. Differences in the micro-nutrient blood values were explored using ANOVA, with posthoc Tukey tests. Finally, the Chi-square test was used to assess whether participants guessed their group assignment.
The statistical packages’ “pscl” and “MASS” for the R statistical software (R version 3.6.0; R Foundation for Statistical Computing, Vienna, Austria, 2016. URL: https://www.R-project.org) and IBM SPSS statistical software (version 25, IBM Corp) were used for the analyses.
Results
Of the 449 inmates who gave informed consent, 47 were released or transferred within 6 weeks of the start of the intervention and left out of the analysis, reducing the sample to 402 adult males, with a mean age of 19.4 years (SD 1.4). Days at-risk of offending ranged from 42 to 104, with a mean of 96.8 days (SD 16.2). Group characteristics are listed in Table 1. These included the non-verbal part of the WAIS-R, EPQ-r, POMS, race, age, and the use of coffee, cigarettes, and soft drinks. At the start of the trial, the group means were not significantly different for any of these variables, and neither was there a significant difference in the mean pre-intervention rule violations per person per day.
Baseline Demographics and Characteristics of the Randomized Groups.
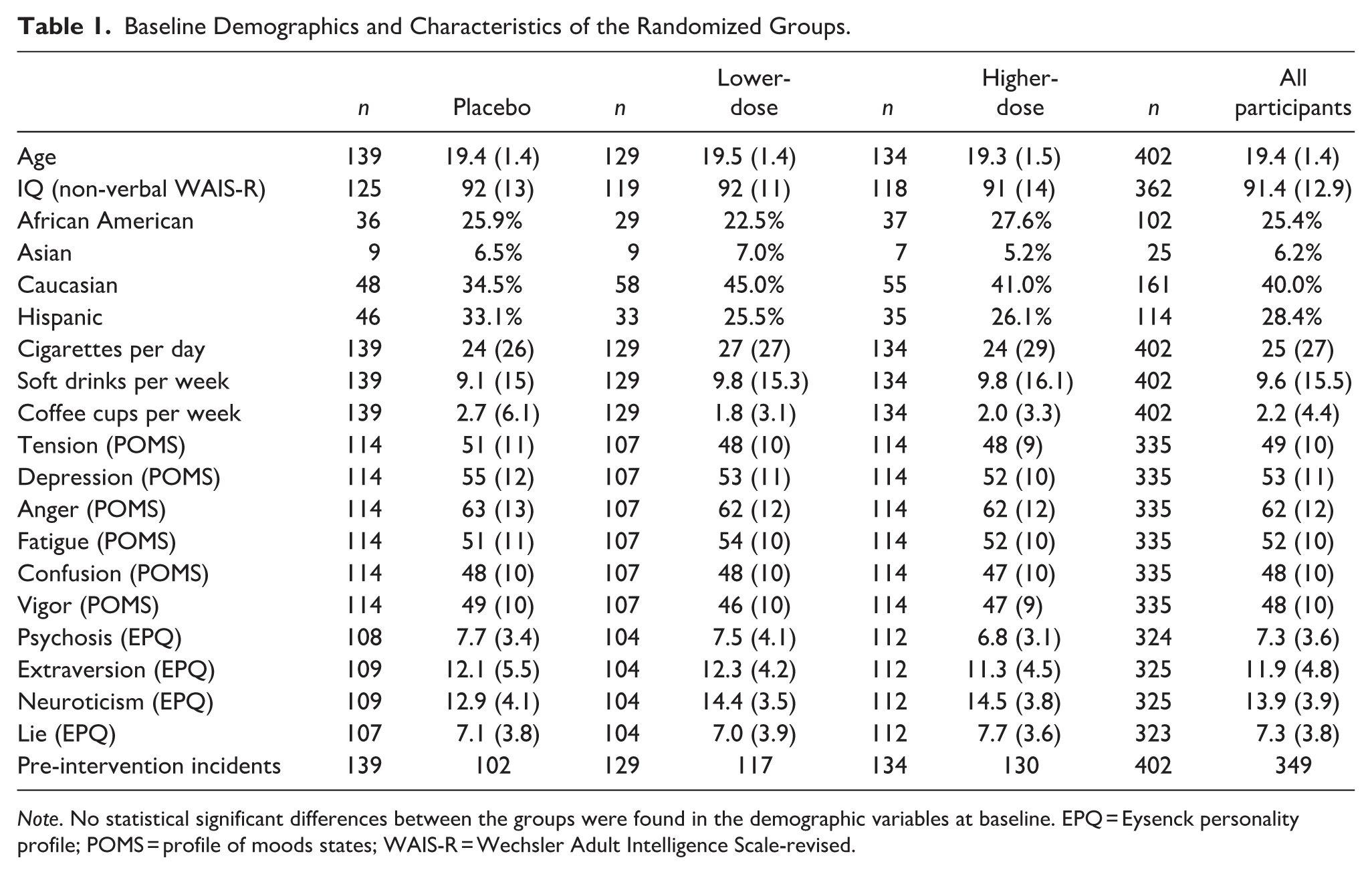
Note. No statistical significant differences between the groups were found in the demographic variables at baseline. EPQ = Eysenck personality profile; POMS = profile of moods states; WAIS-R = Wechsler Adult Intelligence Scale-revised.
Compliance and Blinding
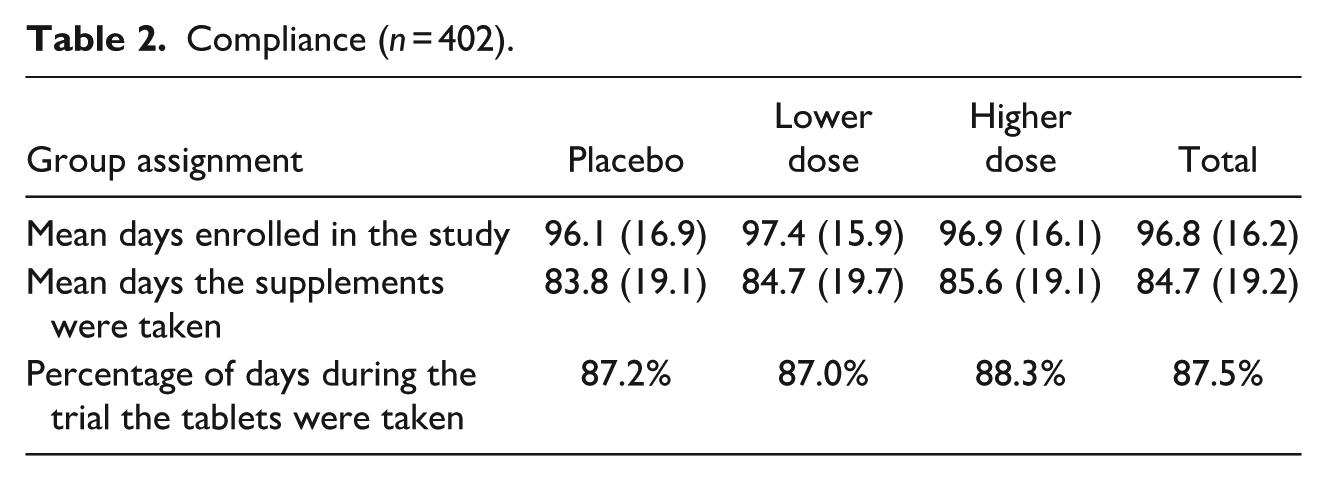
We operationalized compliance as the total number of supplements the participants took during the research period of 105 days, registered by the research assistants. The mean number of days the participants took the supplements was 84.7 (87.5%, see Table 2), in all 402 participants, and there were no statistically significant differences among the three randomized groups (F(2, 399) = .284, p = .753).
Compliance (n = 402).
The micronutrient blood values were measured at baseline in 259 participants and at the endpoint in 194 participants (n = 153 for both time points). Appendix 2 shows the post hoc analysis (Tukey’s test) of blood values in the active groups compared to the placebo group. These results showed increases compared to the placebo group in the 16 micronutrients, of which six were statistically significant. The increase in blood micro-nutrient levels was mainly caused by the higher dose group, confirming that compliance was considerable.
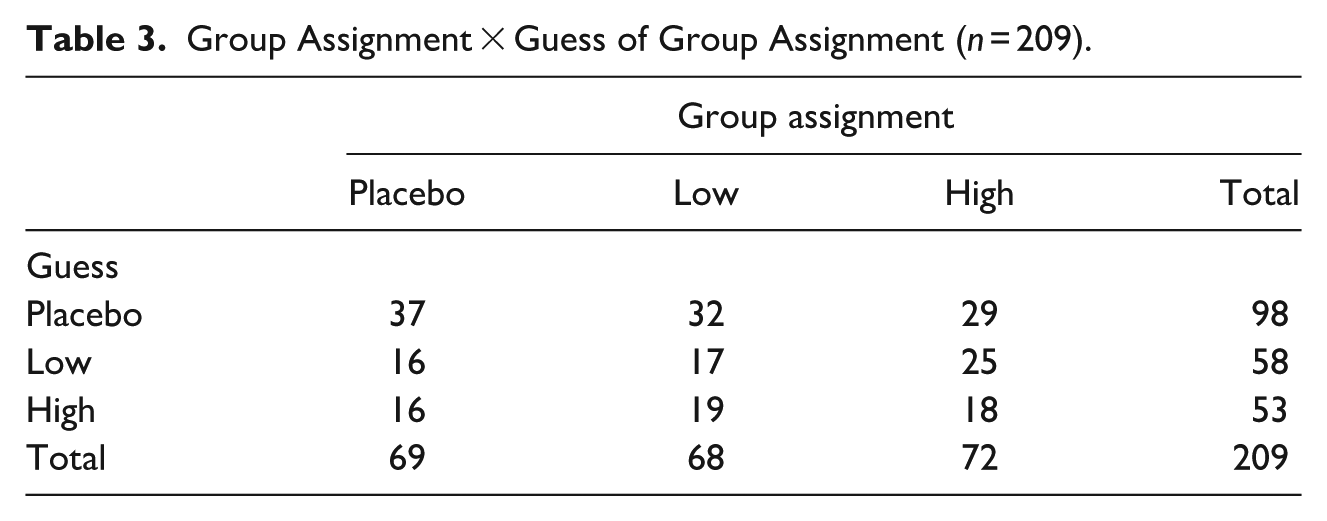
After the study, each participant was asked to guess whether he had received placebos or supplements, and 209 of the 402 participants responded (Table 3). While most participants guessed that they had been using placebo supplements, there were no statistically significant differences among the groups (χ2(4) = 3.61, p = .46).
Group Assignment × Guess of Group Assignment (n = 209).
Main Finding
The count of serious rule violations during intervention was 311 in total, 72 in the low-dose group, 112 in the higher-dose group, and 127 in the placebo group (Figure 2). The overall negative binomial test showed that the mean number of serious rule violations per day differed between the groups (p = .039). The difference between the placebo and lower-dose group was statistically significant with a rate ratio (i.e., Exp(B)) of .61 (95% CI: .41–.90; p = 013). This can be interpreted as 39% fewer rule violations in the lower-dose group relative to the placebo group. There was a small and statistically nonsignificant difference between the placebo and the higher-dose group with a rate ratio of .90 (95% CI: .63–1.30; p = .58). Moreover, the difference in the count of total rule offenses for the higher-dose versus lower-dose group almost reached statistical significance (with a rate ratio of 1.48; 95% CI: .99–2.23; p = .06). The effect estimates of the post hoc analyses to explore whether the effect would be more robust in a violent and non-violent fraction were not importantly different from those with the total rule offenses, although the confidence intervals were slightly wider (Figure 3).
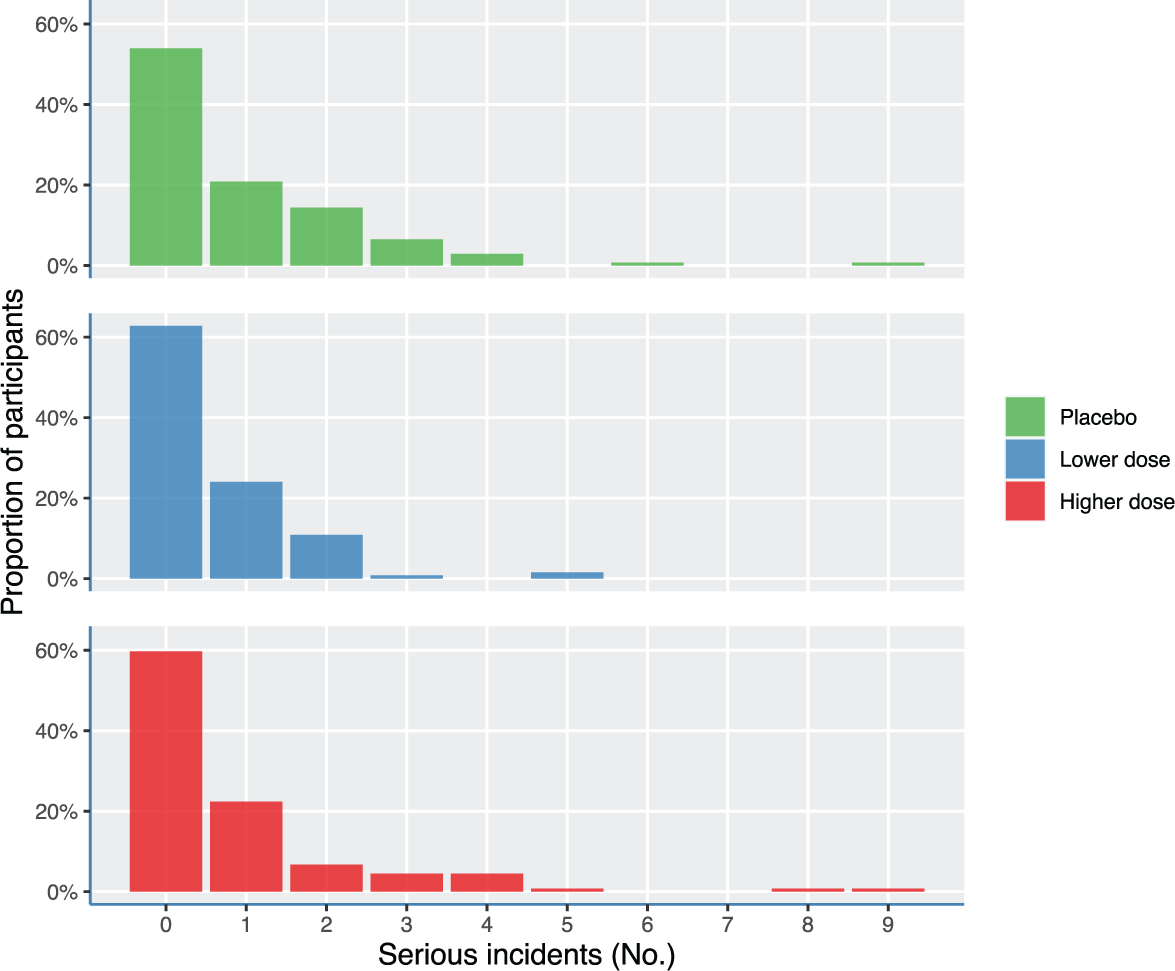
Number and percentages of rule violations during the intervention period according to the randomized groups.
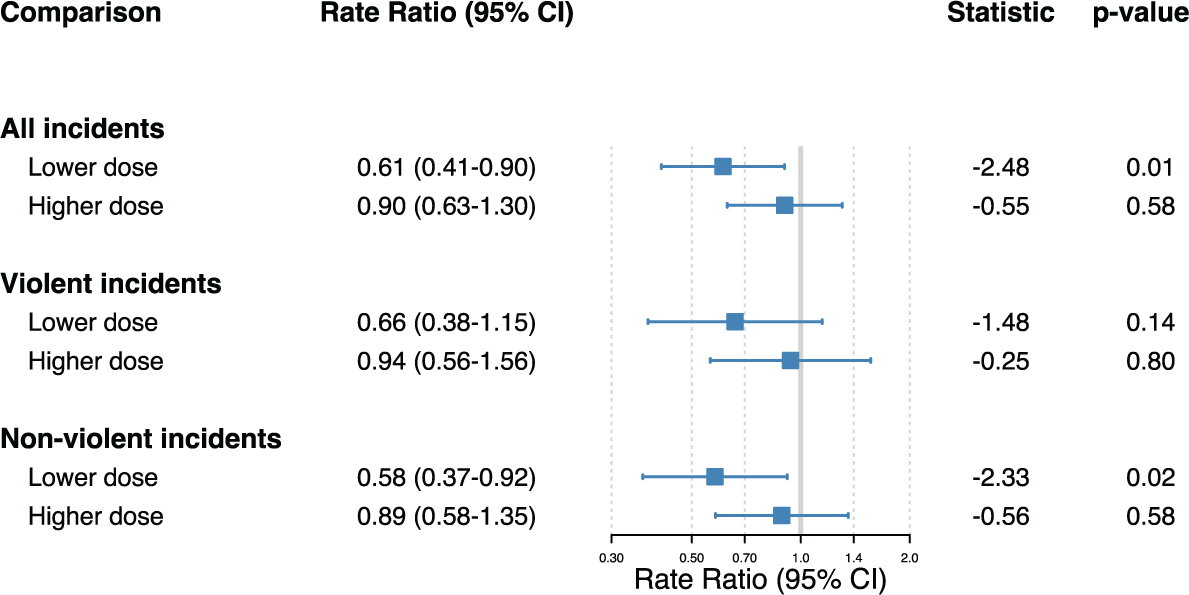
Forest plot of the rate ratios with 95% confidence intervals (CI) of all rule offenses, and those partitioned into violent and non-violent fractions.
Because of the large number of participants with zero incidents, an additional zero-inflated model was used. The Vuong test comparing the zero-inflated model with a negative-binomial regression model was statistically significant, indicating that the zero-inflated model better fitted the count data (AIC-corrected, z-statistic = −2.41, p = .016, BIC-corrected z-statistic = 2.99; p = .001). The odds ratio for structural zero incidents did not differ significantly, neither for the lower-dose group (lower-dose vs. placebo; OR = 0.80; 95% CI: .27–2.34), nor for the higher-dose group (higher-dose; vs. placebo; OR = 1.04; 95% CI: .75–1.44).
Secondary Findings
We found no statistically significant difference between baseline and endpoint on the Total Mood Disturbance (F(2, 215) = 1.30, p = .275). Likewise, we found no significant changes in non-verbal IQ (F(2, 273) = 2.05, p = .131), nor was there a significant difference on, Extraversion (F (2, 213) = 1.07, p = .344), Lie (F (2, 210) = .11, p = .892), Neuroticism (F (2, 213) = 1.61, p = .203), and Psychosis (F (2, 209) = 2.53, p = .082).
Adverse Effects
No adverse effects were reported.
Discussion
There were 39% and 10% fewer serious offenses in the lower-dose and higher-dose groups, respectively, compared to the placebo group. Only the effect in the lower-dose group was statistically significant. The null finding in the higher-dose group was unexpected and did not support a dose-response relationship. Our findings suggest that physiologic rather than supraphysiologic doses of minerals and vitamins benefit this outcome. The difference in the lower and higher dose effects is difficult to explain and can only be speculated. The dosages of vitamins and minerals used in other studies vary. In the other studies among young adult male inmates, doses of approximately 100% RDA were used and obtained similar results as in our lower-dose group (Gesch et al., 2002; Zaalberg et al., 2010). On the other hand, studies among children with attention deficit hyperactivity disorder (ADHD) and autism spectrum disorder (ASD) found a positive effect of higher doses of multi-vitamin and mineral supplementation on behavior (Adams et al., 2011; Rucklidge et al., 2018). Whether age, gender, and psychiatric comorbidity may explain the discrepancies should be further investigated, as these are of critical importance for determining the most effective dosage of supplements.
Institutional misconduct generates higher costs for prisons in more than one way. First, there is direct damage caused by the misconduct, such as the replacement of destroyed property or hospitalization. Secondly, the misconduct can raise the expenses on personal and safety precautions, for instance, the necessity for the employment of more staff or the investment in security systems. It also contributes to additional costs due to increased work stress and burnout of the prison staff (Keinan & Malach-Pines, 2016). Finally, institutional misconduct can affect the parole decision-making process and cause longer periods of incarceration (Mooney & Daffern, 2011). The serious misconducts in the California Youth Authority are “B-level” incidents that must statutorily delay parole from 3 to 6 months with an average of 4 months. According to the California Legislative Analyst’s Office, the costs of confinement for each inmate per year was $21,582 for health care, $2,437 for rehabilitation, and $3,484 for food and activities, equaling $9,168 for 4 months of added confinement per infraction (LOA, 2018). The inmates receiving the lower-dose formula produced 49 fewer incidents than baseline at $9,168 per incident totaling $449,232. Apart from these problems in the prison environment, there is limited support that misconduct in prison can predict post-release recidivism (Mooney & Daffern, 2015; Trulson et al., 2011). These findings are supported by the meta-analysis of (French & Gendreau, 2006), showing that interventions causing a reduction in institutional misconduct are associated with a reduction in recidivism.
Some limitations need to be discussed. First, the trial was conducted in the years 1990 and 1991; as the prison population and nutritional insights have changed since then, the interpretation and implementation of these older data need to be done with care. For example, in more recent times, the number of inmates with criminogenic needs has increased, while participation in institutional programs has decreased (Chamberlain, 2011). In addition, there is little detailed information on trends in the food supply for inmates, but research indicates that there is much room for improvement in the current prison diet (Collins & Thompson, 2012; Cook et al., 2015; Smoyer, 2019). As mentioned before, there were shifts in the RDA of micronutrients since 1990, causing the lower-dose formula to deviate from what is nowadays regarded as 100% RDA; see Appendix 1 for details (Food and Nutrition Board Institute of Medicine National Academies, 2011). The finalization for publication of the data was delayed for many years by someone with a critical stance against research on improving the welfare of prisoners and filed a protracted federal lawsuit against the state for authorizing this study. Eventually, the federal courts dismissed the court case. Second, adverse effects may have been underreported as these were not proactively monitored. A third limitation concerns the interpretation of the blood values. The blood analyses results should be interpreted with caution because of the high number of subjects who rejected giving blood samples and the use of currently outdated measurement techniques with a high relative measurement uncertainty (± 20%) (Zhang et al., 2018). A fourth limitation was that the data of 402 (89.5%) of the 449 randomized participants were analyzed, and therefore no intention-to-treat (ITT) analysis was conducted. The oversight committee determined the exclusion of inmates who participated in the trial for less than 6 weeks because they believed it would take several weeks for the micronutrients to affect behavior. As shown in Figure 1, the percentage of early releasers is much higher in the active than in the placebo groups, making it unlikely that omitting the early releasers would have inflated the intervention’s effect size. Likewise, parole due to good behavior was likely to attenuate the effect size, as a weight (i.e., offset) factor based on days present was included in the analysis. Finally, there was a substantial heterogeneity in the number of incidents per participant (ranging from 0 to 9 incidents during the intervention), which was partly take into account by the dispersion parameter in the negative binomial regression analysis, but also led to larger confidence intervals of the effect estimates.
This trial’s strengths are the large sample size, the relative homogenous group, which guarantees internal validity, and relatively good compliance. However, findings are not straightforwardly generalizable to other groups and settings. A recommendation for further research would be to investigate the effect of dietary supplementation in other settings with high problem behavior, such as special education schools, chronically admitted psychiatric inpatients, and residential care for people with intellectual disability. As the proportion of older inmates with typical misconduct has increased in recent times (Blowers & Blevins, 2014), it may also be interesting to include middle-age inmates in future studies on this topic.
It is important to emphasize that serving sufficient meals in an institution does not ensure that all recipients will eat it. Many inmates still make unhealthy food choices (Eves & Gesch, 2003; Schoenthaler et al., 1991). Sarris et al. (2015) published a position paper in the Lancet where they wrote that: “there is a need to move toward a new integrated framework in Psychiatry, whereby consideration of nutritional factors should be standard practice.” This paper and several systematic reviews show that their position has empirical support in criminology (Benton, 2007; Rucklidge & Kaplan, 2013). Sufficient nutrition is a precondition for classical deterrence theory to deter crime generally or rehabilitation theory to deter crime among specific offenders.
In this study, we found that supplementation of multi-vitamins and minerals in doses of approximately 100% RDA, but not of a higher dose, can help to reduce the number of serious rule violations in prisons. Although achievement through a high-quality diet is to be preferred, controlled trials are essential to help to support the hypothesis that there is a causal relationship between nutritional supplements and rule violations.
Footnotes
Appendix 1
Dosage of Vitamins and Minerals in the Two Groups.
| Vitamins/minerals | Higher dose formula | Lower dose formula | US RDA or AI a (Food and Nutrition Board Institute of Medicine National Academies, 2011) |
|---|---|---|---|
| Vitamin A | 5,000 I.U. | 5,000 I.U. | 3,000 I.U. |
| Vitamin D | 200 I.U. | 200 I.U. | 600 I.U. |
| Vitamin E | 30 I.U. | 30 I.U. | 23 I.U. |
| Vitamin C | 120 mg | 60 mg | 90 mg |
| Thiamin (B1) | 4.5 mg | 1.5 mg | 1.2 mg |
| Riboflavin (B2) | 5.1 mg | 1.7 mg | 1.3 mg |
| Niacin (B3) | 60 mg | 20 mg | 16 mg |
| Pantothenic acid (B5) | 30 mg | 10 mg | 5 mg a |
| Pyridoxine (B6) | 6 mg | 2 mg | 1.3 mg |
| Folate | 400 mµ | 400 mµ | 400 mµ |
| Vitamin B12 | 18 mµ | 6 mµ | 2.4 mµ |
| Biotin | 300 mµ | 300 mµ | 30 mµ a |
| Vitamin K | 50 mµ | 50 mµ | 120 mµ a |
| Calcium | 122 mg | 200 mg | 1,000 mg |
| Magnesium | 59 mg | 80 mg | 400 mg |
| Iron | 18 mg | 18 mg | 8 mg |
| Zinc | 15 mg | 15 mg | 11 mg |
| Iodine | 150 mµ | 150 mµ | 150 mµ |
| Copper | 2 mg | 2 mg | 0.9 mg |
| Manganese | 2.5 mg | 2.3 mg a | |
| Chromium | 100 mµ | 35 mµ a | |
| Selenium | 100 mµ | 55 mµ | |
| Molybdenum | 120 mµ | 45 mµ |
Note. RDA = recommended daily allowance.
Adequate intake (AI), instead of RDA.
Appendix 2
Acknowledgements
We would like to thank (a) Assemblyman Darrell Steinberg and Senator Robert Presley, who sponsored the required legislation to allow this study in California, (b) the Oversight Committee at the University of California, Berkeley, who approved the protocol and monitored the study, and (c) Martin Torn M.D. for his assistance in preparing this paper. We also thank the California Youth Authority for its support and the California State University, Stanislaus, for supporting this area of research.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Neither the authors nor the University of California, Berkeley Public Health Department Oversight Committee, has or had any conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.