
Abstract
When are politicians willing to liberalize abortion laws? While restricted access to legal abortion affects millions of women around the world, there is relatively little understanding of the factors shaping the views of politicians who craft or uphold such restrictive laws. This study examines the impact of a public health framing commonly employed by activists to persuade politicians to reform abortion laws. We provide evidence that politicians’ preferences toward abortion reforms are shaped by the intersection of gender and wealth. Drawing on a survey experiment conducted among more than 600 politicians in Zambia, we show that only women politicians from less wealthy backgrounds are more likely to support policy liberalization after being exposed to a public health framing. These findings underscore how economic inequalities can affect the substantive representation of women’s interests and provide a baseline for further research on the use of framing strategies in other developing country contexts.
Keywords
Women across the Global South face a public health crisis due to extensive restrictions on reproductive rights. Nearly half of all abortions carried out in developing countries are classified as unsafe: where a pregnancy is terminated by an unqualified individual or in conditions that do not conform to minimal medical standards (Ganatra et al., 2017). Such unsafe abortions are a leading contributor to maternal mortality, according to the World Health Organization, with nearly all of those deaths occurring in developing countries (Gerdts et al., 2015; Latt et al., 2019). Although women are as likely to seek an abortion where it is prohibited as where it is available upon request (Sedgh et al., 2016), abortion-related deaths are systematically higher in countries that legally restrict abortion access (Latt et al., 2019). Even when women survive unsafe abortions, they can go on to suffer long-term complications such as infertility, chronic gynecological problems, or other disabilities (Faúndes & Shah, 2015; Warriner, 2006).
Providing access to safe abortion involves medical and religious issues, but it is ultimately a political question. It is through the politics of elections, legislation, and regulation that abortion is made available to women, whether permitted without restriction, in exceptional cases of rape and incest, or only when required to save the life of a woman, if at all. Given the fundamental role of politicians in making abortion access legal and safe, we examine in this paper whether and how politicians adapt their policy preferences toward abortion liberalization.
Relatively little is known about the factors that influence politicians’ views of abortion policy. Although there has been extensive research on general attitudes toward abortion (Abramowitz, 1995; Cook, 2019; Jelen & Wilcox, 2003), nearly all of this work is based on average citizens, not those directly involved in policymaking. Moreover, there is no consensus in survey-based work on what underpins abortion policy preferences or causes them to change. Early findings regarding factors such as gender (Patel & Johns, 2009), religion (Jelen, 2014), and education (Jelen & Wilcox, 2003) have either been overturned over time or pared back considerably. This has resulted in an acute gap in our knowledge about the biases or heuristics that may play into abortion policymaking (Linde & Vis, 2017; Sheffer et al., 2018).
Focusing on how abortion is framed in public discourse offers one fruitful path for understanding potential shifts in politicians’ policy preferences. Noteworthy instances of abortion decriminalization around the world have often followed activists’ efforts to reframe abortion as a social justice issue that disproportionately affects the health of poor women. In Argentina, for example, activists were able to partner with legislators to bring about greater access to legal abortion after pivoting to emphasize the dangers that illicit abortions create for poor women in an unequal society (Anderson, 2022; Daby & Moseley, 2022; Lopreite, 2023). Activists have been able to promote similar reforms in countries as varied as Ethiopia (Holcombe & Kidanemariam Gebru, 2022), Mexico (Sánchez Fuentes et al., 2008), and Nepal (Shakya et al., 2004) by framing abortion as a public health issue that directly links the prevalence of maternal mortality among poor women to the legal restrictions that lead them to rely on clandestine, unsafe procedures. Yet, while the reframing of abortion as a public health issue appears to precede liberalizing reforms in many countries, it remains unclear to what extent such a framing strategy actually persuades politicians to change their policy positions. Can the provision of fact-based information about the toll of unsafe abortion cause politicians to support liberalizing reforms?
Framing abortion as a public health issue is likely to resonate with women politicians in particular. Women politicians frequently assume a leading role in advocating for the expansion of reproductive rights within legislatures in order to improve women’s overall wellbeing (Berkman & O’Connor, 1993; Levy et al., 2001; Sawer, 2012). The likelihood of abortion legalization is, in fact, correlated with the proportion of women elected to legislatures (Asal et al., 2008; Budde & Heichel, 2017). Yet, while there is a relationship between women’s descriptive representation in elected office and the expansion of reproductive rights, other demographic and sociological factors are likely to influence whether women politicians will support the adoption of abortion policies.
We argue that a woman politician’s personal wealth will affect her stance on abortion liberalization. Drawing on prior research showing that class distinctions affect women’s substantive representation (Blofield, 2008, 2013; Htun & Power, 2006; Htun & Weldon, 2010), we posit that a woman politician’s wealth will condition her receptivity to a public health framing emphasizing the risks associated with unsafe abortion. Such a framing may well persuade a woman politician from a middle-class or working-class background because she will intuitively understand how a lack of resources can limit family planning options. By contrast, a woman politician from a wealthy background may be less persuaded by a public health framing; the issue is simply less immediate for her because her family planning options are largely unconstrained by legal or medical restrictions. We have no such expectations for men politicians in this regard since they usually do not bear the same personal costs associated with pregnancy (e.g., childbirth risks).
To assess how politicians’ attitudes toward abortion liberalization might be influenced by a public health framing, we leverage a survey experiment conducted among more than 600 politicians who competed for national and local offices across Zambia. Abortion has been legal in Zambia under a range of conditions for several decades, but the law also required women to obtain the approval of three doctors—a requirement that few poor women could meet. Access to safe abortion in Zambia has therefore been extremely limited. We used a survey experiment to randomly expose half of our politician sample to the kind of public health framing employed by reform activists: politicians in the control group were asked if they would consider reducing the number of doctors required to approve a woman’s legal abortion in Zambia from three to one, while politicians in the treatment group were additionally presented with a framing that informed them that unsafe abortions account for 30 percent of maternal deaths in the country.
Our survey-based findings are consistent with earlier scholarship in showing that women politicians in Zambia are systematically more likely than men politicians to support liberalizing abortion policy even after accounting for factors such as education and religion. But the framing experiment further reveals that only a subset of women politicians liberalize their views on abortion policy after being informed of the public health costs in terms of maternal mortality. Women politicians who run for local office, though initially holding more conservative views on average, are the most likely to shift their policy preferences after being exposed to the public health framing. We provide suggestive evidence that local politicians are more likely to update their abortion policy preferences because they are economically distinct from their counterparts who compete for national office. Women politicians at the local level have significantly less personal wealth compared to women politicians at the national level. We interpret this economic distinction as a reflection of underlying differences in their relative abilities (or those of their constituents) to navigate alternative family planning options, such as access to private clinics that offer abortion services, along with the lived experiences associated with those options.
This study’s findings contribute to research on how public policies affect women’s well-being. While scholars have recognized the dearth of comparative studies focused on the gendered impact of policies (Tripp, 2006), our state of knowledge remains unrepresentative because we continue to draw inferences from studies drawn from a relatively small set of countries that tend to be established democracies or economically developed. In this respect, this study helps to expand understanding of how institutions (Beer, 2017; Stetson, 2001) and identities (Htun et al., 2013; Luna, 2017) can interact to shape policy outcomes critical to women’s health under more challenging conditions. Our findings, though drawn from the Zambian case, can be generalized to a number of African countries where women continue to face among the highest rates of maternal mortality in the world (Phiri et al., 2020) at the same time that they have the least access to safe abortion. 1 To our knowledge, this is the first empirical study in Africa that examines policymakers’ self-reported attitudes to gauge their willingness to adopt abortion policy reforms aimed at improving public health conditions for women.
Our study also contributes to the study of women’s substantive representation more generally (Beckwith & Cowell-Meyers, 2007; Celis et al., 2008; Childs & Krook, 2009). The fundamental experiences that women politicians share with other women in society often lead them to advocate for policies aimed at benefiting women’s interests (Cowell-Meyers & Langbein, 2009; Schwindt- Bayer, 2006; Taylor-Robinson & Heath, 2003; Wängnerud, 2009), though there is growing recognition that gender can intersect with other social cleavages to limit the scope for substantive representation (Blofield & Ewig, 2017; Luna & Luker, 2013). Our study complements earlier scholarship by providing nuanced empirical evidence that the economic background and work history (Kitschelt & Rehm, 2014) of elected representatives matters not only for explicitly economic policies but also potentially influences how they view public health policies. Given the continued underrepresentation of women in political power, particularly in the Global South, our findings are relevant for countries in which the few women who do attain office may not necessarily reflect the experiences of the majority of women. This demographic mismatch, in socioeconomic terms, may well have consequences for policymaking that have yet to be fully understood in societies that are becoming increasingly unequal (Carnes & Lupu, 2023).
What Factors Shape Politicians’ Abortion Policy Preferences?
The large literature on public attitudes toward abortion provides a starting point for identifying the relevant demographic factors that influence how politicians respond to distinct abortion policy framings. These demographic factors have the potential not only to shape politicians’ attitudes toward abortion policy but also how they might interpret new information about this issue area. We summarize the logic for specific attitudinal claims along with their testable hypotheses.
Gender
There is no consensus among the studies examining gender-based attitudes toward abortion policy (Patel & Johns, 2009). Some studies find that women are, as a group, more likely to support legalization (Barkan, 2014; Lizotte, 2015; Westfall, Kallail and Walling, 1991), others show that men tend to be more supportive (Moore & Stief, 1991; Wright & Rogers, 1987), and others find no relationship at all (Betzig & Lombardo, 1992; Szafran & Clagett, 1988). Given the documented role of women’s advocacy on behalf of legalization (Kreitzer, 2015), we expect women politicians to be more likely to support abortion liberalization. 2
Marriage
Attitudes toward abortion legalization may be conditioned by marital status. As an institution that has socio-cultural, religious, and legal elements, marriage may induce women to develop preferences connected to their roles as wives and mothers (Luker, 1984). Married women’s abortion policy preferences are therefore likely to be shaped by the fact that they must make joint decisions — and possibly disagree — with male partners over family planning, raising questions about the number of children to have (Chiappori et al., 1992; Miller & Valente, 2016). Empirically, married men typically prefer having more children than married women (Doepke & Tertilt, 2018; Westoff et al., 2010). 3 When disagreement over childbearing preferences arise within a marriage, actual fertility outcomes are likely to depend on the extent to which a woman can exercise bodily autonomy. In countries where women generally have fewer rights, for example, the number of children born to a couple tend to correlate with men’s childbearing preferences (Doepke & Tertilt, 2018). Given such dynamics, we generally expect married politicians to express less support for abortion liberalization.
Religion
Research shows that religious identities most consistently shape abortion policy preferences. Communities dominated by religious traditions that hold conservative Christian views on abortion tend to support restrictive regulations (e.g., Catholic and Evangelical) (McVeigh et al., 2017). Highly religious people tend to be especially opposed to abortion as a matter of principle (Jelen, 1993; Jelen & Wilcox, 2003; Lynxwiler, 1999; Minkenberg, 2002; Steensland et al., 2000), though there are differences across denominations. Active practitioners of their faiths tend to be the most opposed (Bartkowski et al., 2012; Hoffmann & Johnson, 2005). While studies of abortion attitudes generally distinguish the religious from the non-religious regardless of gender (Campbell et al., 2018; Lizotte, 2015), religious beliefs may differentially influence women’s policy views if they are, in fact, more religious than men (Cassese & Holman, 2016; Holman et al., 2020; Kaufmann & Petrocik, 1999). We expect politicians from conservative religious backgrounds to be less likely to support abortion liberalization.
Partisanship
Ideologically-driven partisanship can play a prominent role in shaping individual stances on abortion policy. Conservative or right-of-center parties often espouse anti-abortion positions through platforms emphasizing traditional family values. In the United States, for example, as the Republican Party came to rely on the support of outside religious interest groups from the 1980s onwards, its candidates and voters became increasingly opposed to abortion (Carmines et al., 2010; Karol & Thurston, 2020). By contrast, liberal or left-of-center parties typically advocate for abortion rights through platforms stressing equality of the sexes before the law. The likelihood of liberal parties consistently advocating for abortion liberalization has depended on whether they are aligned with feminist movements as well their degree of institutionalization (Blofield, 2008; Blofield & Ewig, 2017). However, while these partisan differences may consistently structure abortion politics in established democracies (Budde et al., 2018), parties in many late democratizing countries tend to lack the ideological roots required to activate abortion as a partisan cleavage (Elischer, 2013). Nevertheless, in general, we expect politicians from liberal or left-of-center parties to be more likely to support abortion liberalization.
Education
Higher education levels have long been associated with greater support for legalized abortion among both women and men (Patel & Johns, 2009; Wang & Buffalo, 2004). However, at least in the United States, the correlation between education and support for legal abortion has declined over time, particularly among conservative voters (Jelen & Wilcox, 2003). Beyond education, having knowledge about abortion procedures and regulations has been found to be significantly associated with greater support for access to legal abortion (Esposito & Basow, 1995). In some contexts, greater information about abortion, including its associated motivations and consequences, may not necessarily lead to increased support for liberalizing policy (Bernas & Stein, 2001; Hunt et al., 2022). Nevertheless, on net, we expect politicians with greater education to be more likely to support abortion liberalization.
Ethnicity
Ethnic identity could play a role in shaping abortion policy preferences in diverse societies. Early studies from the United States indicated that there were race-based differences with African Americans being less supportive of legal abortion (Craig & O’Brien, 1993; Secret, 1987). However, later research suggests a reversal in abortion attitudes among different groups with African Americans reporting greater support (Lynxwiler, 1999; Strickler & Danigelis, 2002). More recent studies have questioned race or ethnic-specific explanations for abortion attitudes, as such identities begin to disappear as consistent predictors by the late 1990s (Bolzendahl & Myers, 2004; Wilcox, 2000). In Ghana and Nigeria, for example, religiosity rather than ethnicity is a more powerful predictor of abortion attitudes (Adisah-Atta and Dim, 2019). We therefore remain agnostic as to whether ethnic identity conditions a politician’s support for abortion liberalization.
With the exception of gender, most of the explanations summarized above do not provide a sufficiently compelling account for why or how a politician might shift their policy position in response to abortion-related information that is either new or simply made salient. In the next section, we turn to examining why wealth is a particularly powerful demographic factor that filters how politicians interpret policy frames that stress the personal toll of abortion restrictions.
How Wealth Affects Politicians’ Responses to Abortion
Activists seeking to change abortion laws around the world have strategically experimented with varied policy framings to persuade politicians to change their positions on liberalizing access. In reframing the issue away from traditional debates over moral conceptions or religious principles (Burns, 2005; Ferree, 2002), activists have specifically employed rhetoric that emphasizes the life-threatening consequences of existing restrictions for women (Daby & Moseley, 2022; Encarnación, 2022; Lopreite, 2023). This reframing of abortion as a medical procedure that is disproportionately denied to poor women is meant to educate politicians about the realities faced by women with the aim of making them more amenable to supporting legislative reforms that might be described—less controversially—as protecting women’s welfare. Yet, it remains unclear to what extent a public health framing resonates among the politicians targeted for persuasion, or if only a distinct subset are likely to be receptive to such messaging.
While numerous factors might determine a politician’s receptiveness to a public health framing of abortion, particularly those reviewed in the previous section, we argue that a politician’s economic background plays a critical role in shaping whether and how they update their preferences in a policy context where their wealth may condition their personal experience. Prior scholarship shows that politicians from different economic backgrounds not only bring different preferences to office (Barnes et al., 2021; Carnes & Lupu, 2023), but those preferences also apply to a wide range of social welfare policies with politicians from white-collar backgrounds consistently holding more conservative views (Carnes & Lupu, 2015). Extending these insights, we contend that the personal wealth of politicians plays an outsized role in shaping their attitudes toward abortion policy. Because access to resources has a direct impact on whether women can secure safe reproductive services, especially in developing countries with high rates of socioeconomic inequality, we expect the views of women politicians toward abortion policy to be shaped by their own economic resources. Whether a woman politician responds to a public health framing will thus depend on her wealth.
In many countries of the Global South, where persistent economic inequalities are often normalized, women politicians from different socioeconomic strata can have parallel lives that offer completely different experiences with the structural obstacles limiting bodily autonomy. Women politicians from higher socioeconomic strata typically have independent access to resources and are therefore less constrained by legal regulations that might otherwise limit their reproductive choices (e.g., going to a private clinic that offers services that cannot be secured at a public hospital). By contrast, women who enter politics from lower socioeconomic strata are more likely to personally know, or have family or friends who know, what it is like for family planning options to be limited by financial constraints. In this respect, an abortion policy frame that stresses public health will tend to resonate with women politicians from lower socioeconomic strata because it speaks to a problem (i.e., maternal mortality) that is a part of everyday life among their constituents.
At the individual level, our theoretical intuition is consistent with studies of sexual negotiation showing that women are more likely to exercise autonomy when they control their own resources. A woman with her own income acquires greater bargaining power when negotiating over fertility. In Uganda, Wolff et al. (2000) find that women with access to cash-based work can feel more empowered to negotiate with their partners over sex. In Ghana, Tenkorang (2012) shows that wealthier women are more likely to report that they can ask husbands to use condoms or to refuse sexual intercourse. In South Africa, Hallman (2004) finds that wealth is a consistent predictor of sexual experience among young women: relative wealth decreases a woman’s odds of experiencing coerced sex, using a condom with her last partner, and, crucially, communicating about sensitive topics with most recent sexual partner. Poor women in Malawi are far less likely to report using modern contraception in comparison to wealthy women (Adebowale et al., 2014).
The available research further shows that resources directly influence a woman’s ability to choose a preferred contraceptive strategy. Women who can acquire and spend their own money are more likely to exercise a greater range of options for managing family planning, whether prior to the onset of pregnancy or afterward (Pop-Eleches, 2010). Wealth, in addition to increasing a women’s control over their bodily autonomy, provides access to alternative forms of contraception that allow for greater flexibility in family planning (Adebowale et al., 2014). Consider, for instance, that condom usage requires negotiation with sexual partners, but other forms of contraception can be used solely at the discretion of a woman who can afford them. In Nigeria, wealthier women are more likely to use injectable forms of birth control that are notable for their discretion and long-term effectiveness (Adebowale et al., 2016). Wealth specifically affects women’s ability to access safe abortions. In countries like Ghana (Sundaram et al., 2012) and Zambia (Leone et al., 2016), wealthier women are more likely to access safe abortion in comparison to poor women, who generally rely on unsafe abortion.
At a political level, our theoretical expectations are consistent with Htun (2003)’s study of abortion policy in Latin America, where elite reformers originally had little incentive to advocate for liberalization as long as middle-class women could access safe abortion in private clinics. In contrast to divorce — an issue area that cuts across class lines — she finds that abortion advocacy was largely conducted by feminist activists concerned with social justice for poor women. This class-based distinction can be generalized to a broader insight from Htun et al. (2013, p. 98): “When women act to promote women’s rights, it is because they are reacting to disadvantages, not because all women share the same interests.”
Blofield (2013)’s comparative study of Argentina, Chile, and Spain provides additional evidence by revealing how persistent social inequalities inhibit the emergence of the reformist coalitions needed to reframe abortion as a public health or women’s rights issue. Blofield (2013, p. 61) shows through her case studies how inequality can have “a corrosive effect” on cross-class mobilization. Middle-class women have little incentive to work with others toward reform as long as they can secure safe abortions through clandestine clinics. Abortion thus becomes the problem of poor women.
Similarly, Karol and Thurston (2020) show that the abortion policy attitudes of individual politicians in the United States can be shaped by personal background characteristics rather than partisan or constituency cues. In studying the mid-twentieth century voting records of California legislators, they find that politicians may default to their own personal views on an issue when they cannot readily ascertain those of their constituents. Politicians appear to give more weight to the views of constituents with whom they share identifiable traits, such as gender and class.
Drawing on such insights leads us to examine the following hypothesis: women politicians with less wealth should be more likely to support liberalizing access to safe abortion—after being informed of the human toll associated with unsafe abortion. We expect no such updating among men politicians because they do not have to consider the same risks as women, namely, unwanted pregnancy, the cost of legal abortion, or the risk of unsafe abortion.
Constrained Economic Access to Legal Abortion in Zambia
We focus empirically on Zambia to assess how politicians might respond to a reframing of abortion policy. Zambia is relevant to comparative research on abortion policy because the various legal restrictions imposed on accessing this medical procedure are comparable to those faced by women in countries across the Global South. As illustrated in Figure 1, whereas abortion tends to be available upon request in countries that are either established democracies or economically developed, there are a range of restrictions on abortion in most countries of Africa, Latin America, the Middle East, and South and Southeast Asia. In this respect, when politicians in Zambia deliberate over abortion policy, they do so under legal restrictions shared by many other countries. Abortion laws around the world.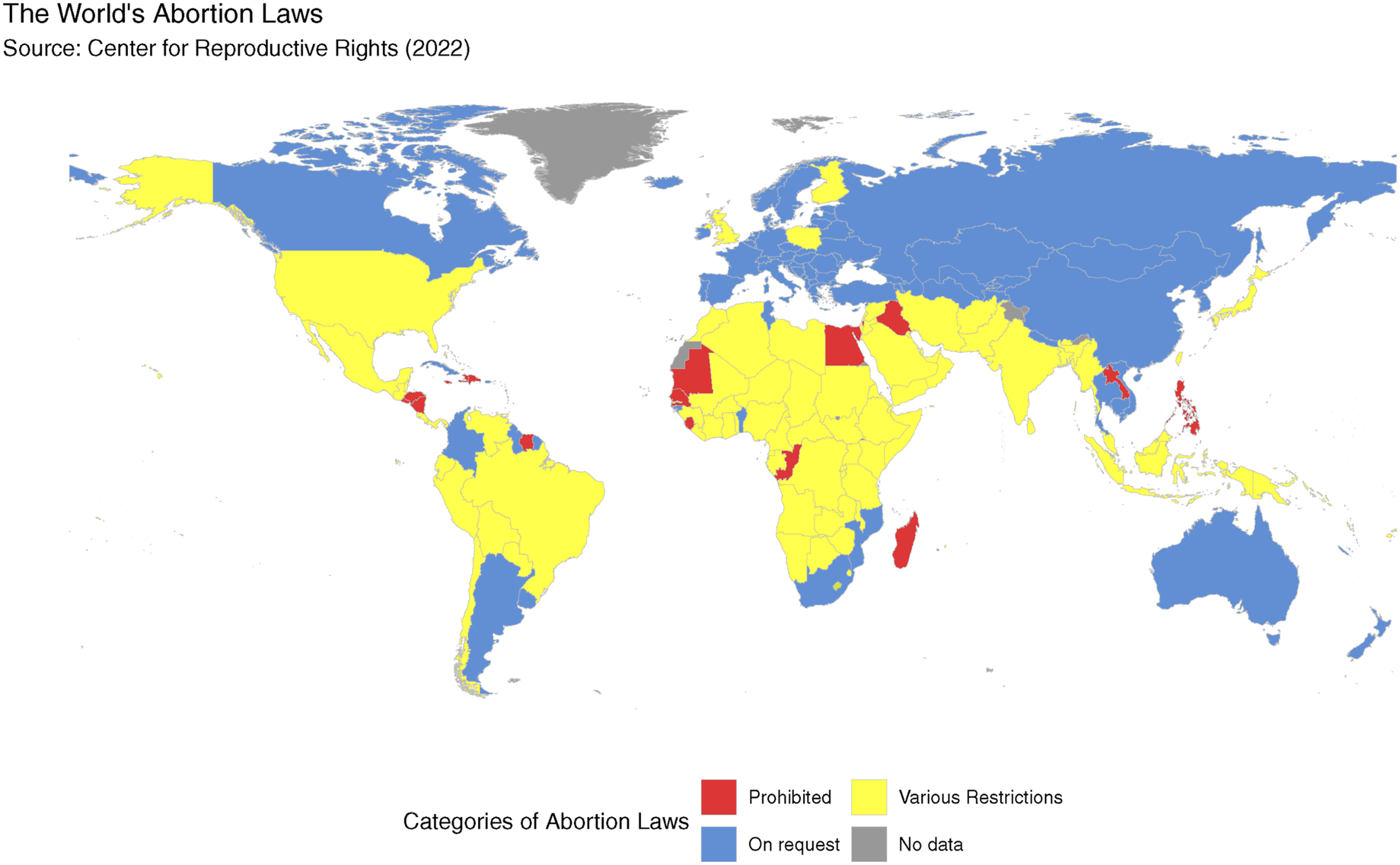
Zambia’s legal framework for abortion has historically been more constraining for women than what actually appears on paper. The Termination of Pregnancy Act (1972) ostensibly allows for abortions to be performed by registered medical practitioners when pregnancies involve a risk to the life of the woman, her physical or mental health, or to any of her existing children (Coast & Murray, 2016; Leone et al., 2016). 4 But access to safe abortion has historically been unattainable for most women in the country. Haaland et al. (2019) point out that the benefits of the 1972 law are offset by severe penalties: the criminal code imposes up to seven years in prison for those who illegally provide abortion services, and up to 14 years for women who procure illegal abortions or anyone who assists them.
The politics surrounding abortion in Zambia also make this country study comparable to many other countries in the Global South. The dominance of Christianity in Zambia’s public life—the country recognizes itself as a Christian nation in the constitution—limits how the issue is debated, particularly since the Catholic Church and Pentecostal churches actively oppose its legal status (Hinfelaar, 2011). While a proposed bill of rights that included a constitutional amendment stating that “life begins at conception” momentarily reignited political debate over abortion (Haaland et al., 2019), none of the country’s major parties is associated with a distinctive position on abortion rights. In this respect, Zambian parties are like many other parties across Africa and other late democratizing countries in that they lack ideological differences that translate into clear-cut partisan or programmatic cleavages (Elischer, 2013). In fact, we find no evidence of systematic party-level differences in Zambia regarding abortion. As shown in Appendix Figure A3, there are negligible differences in the average abortion policy preference between members of the country’s major parties. What this has meant, in terms of policymaking, is that activists in Zambia have lacked the institutionalized party ally required to place abortion reform on the agenda, mobilize popular support, and enact the necessary legislation (Blofield & Ewig, 2017).
Zambia’s legal framework, when combined with prevailing socioeconomic and political realities, makes access to safe abortion almost unattainable for women at lower income levels (Blystad et al., 2019; Munakampe, Zulu and Michelo, 2018). Women who wish to terminate a pregnancy, particularly poor women, frequently turn to unsafe methods or unqualified service providers (Macha et al., 2014; Owolabi et al., 2017). Treating the complications associated with unsafe abortion in Zambia costs approximately $ 1.4 million per year (Parmar et al., 2017). Official estimates from Zambia’s health authorities indicate that 30–50 percent of all acute gynecological admissions are due to abortion-related complications (Likwa et al., 2009). Some 6,000 Zambian women die of abortion complications each year due to unsafe procedures (Demographic, 2014). As a result, 30 percent of all maternal deaths in Zambia are related to unsafe abortion (Cresswell et al., 2016; of Health, 2011).
The apparent disconnect between the legal framework and the medical realities faced by Zambian women must be understood in light of a deficient national health system. With only about 60 obstetricians/gynecologists serving a population of 17 million (GRZ, 2017), access to reproductive health services is severely limited. The scarcity of qualified doctors and health facilities across the country, particularly in rural areas, is a structural barrier to women’s access to safe and legal abortion. This scarcity has been exacerbated over time by a legal requirement for three doctors’ signatures to authorize an abortion, including one signature from an obstetrician gynecologist. 5 This requirement was revised in 2017 to just one doctor (GRZ, 2017). Nevertheless, given the persistent lack of medical resources, many women have turned to unsafe alternatives despite abortion’s legal status (Halwiindi et al., 2016).
Estimated Costs for Abortion Services at Zambian Hospitals and Clinics.
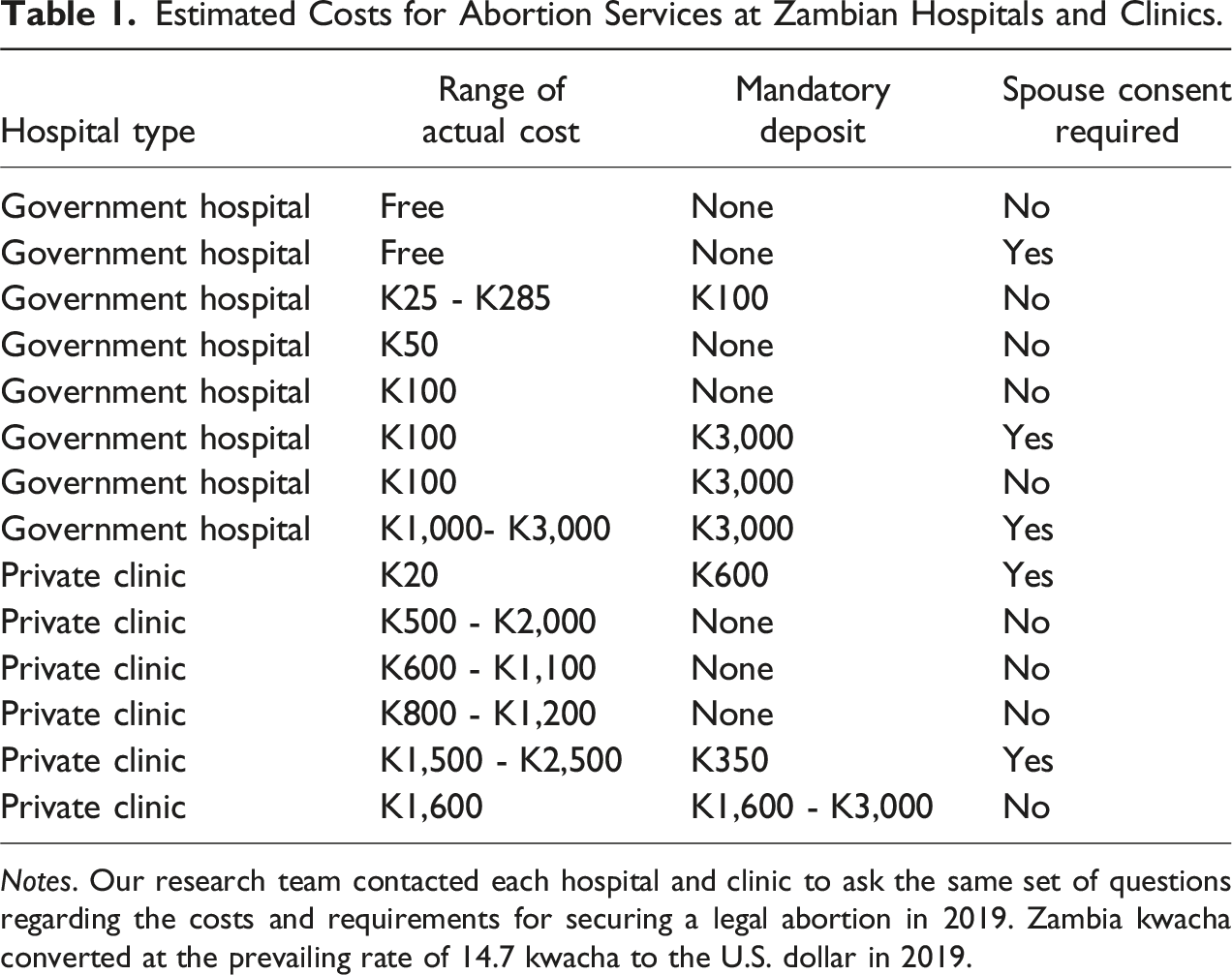
Notes. Our research team contacted each hospital and clinic to ask the same set of questions regarding the costs and requirements for securing a legal abortion in 2019. Zambia kwacha converted at the prevailing rate of 14.7 kwacha to the U.S. dollar in 2019.
The costs listed in Table 1 suggest that an abortion would pose a considerable economic hardship for the average Zambian woman. Among the eight government hospitals in our sample, the average minimum cost for securing an abortion would be K172 or almost $12. Such a cost would represent over 27 percent of monthly wages for a Zambian woman who is a domestic worker or about 16 percent of monthly wages for a woman who is a cleaner or general worker. 7 The average minimum cost is five times higher among the private clinics. For the hypothetical Zambian woman who is a domestic worker, the cost at a private clinic would amount to 132 percent of her monthly wages. The woman who is a general worker or cleaner would pay nearly 80 percent of her monthly wages. Table 1 further reveals that Zambian women must pay a cost to navigate a health system in which accurate information is difficult to come by. 8 While Zambian law does not require spousal consent for an abortion, the hospitals and clinics we contacted provided inconsistent information. Three of the eight government hospitals claimed that spousal consent was required, as did two of the six private clinics. Indeed, among the private clinics, the minimum average cost of accessing an abortion is more expensive at the clinics that do not require spousal consent (K875) than those requiring such consent (K760). In other instances, the medical personnel we reached provided inaccurate information by claiming that abortions could only be performed for limited medical reasons or rape. Consequently, a woman seeking to retain personal control over her fertility would potentially need to pay the cost associated with contacting multiple hospitals or clinics before arriving at one that might give her access to a legal procedure.
The question remains whether the abortion policy attitudes of Zambian politicians are affected by the economic realities described above. As in many other developing country contexts, it remains unknown whether those directly involved in policymaking are willing to support abortion liberalization when exposed to the human toll associated with the conditions of unsafe abortion.
Research Design
To assess how politicians might respond to a public health framing of abortion, we surveyed a sample of Zambian politicians who competed in the country’s 2016 general elections. Our sample includes candidates who competed for parliamentary seats in the National Assembly as well as ward councilor seats at the local level across the country. Parliamentary candidates are directly relevant to the study of abortion policymaking since they would be expected to vote on any national legislation pertaining to the existing abortion law or related portions of the criminal code. Ward councilor candidates are also relevant actors in policymaking because they are frequently local party leaders and members who hold offices within their partisan organizations, such as the chair of a district party branch. These local politicians inform the development of party platforms as well as the selection of parliamentary candidates. One measure of their influence can be seen in the fact that ward councilors control the first stage of parliamentary candidate selection, and parties typically field the candidates that their local-level selection committees initially endorse (Phillips, 2022).
We sampled parliamentary candidates across 156 single-member constituencies as well as ward councilor candidates in the districts encompassing Zambia’s ten provincial capitals. 9 Among parliamentary and councilor candidates, we sampled both winners and first losers. We included first-losers in the sample to ensure that our understanding of politician preferences over issues was not driven by their status as winners. The decision to include only first-losers was made based on our analysis of electoral data indicating that Zambian elections are predominantly two-person contests. Any candidate beyond the first loser typically receives only a small fraction of the vote share and is thus unlikely to be representative of the viable candidates who go on to become policymakers.
Our sample reflects the real distribution of candidates with respect to both gender and tier of office. Women are severely underrepresented in Zambian politics (Arriola, Phillips and Rakner, 2021): At the time of our study, women made up less than 10 percent of all ward councilor candidates and 20 percent of MP candidates. In 2016, only 25 women MPs were elected, constituting 16% of all MPs. Our sample—only around 12 percent of which are women for both tiers of office— thus reflects the under-representation of women in Zambian politics rather than a systematic undersampling of women from the population of political candidates. We believe inferences drawn on our sample should therefore be representative of the true distribution of policymakers’ abortion preferences as well as differences in these preferences across men and women. Moreover, since we sampled from the top-two vote-getters in national and local races, the women in our survey are likely to be truly representative of the type of woman who can compete in a male-dominated electoral arena. In this respect, attempting to over-sample women would have potentially introduced noise in our analysis by adding women who would not necessarily be representative of those who actually go on to become elected officials.
Descriptive Statistics.
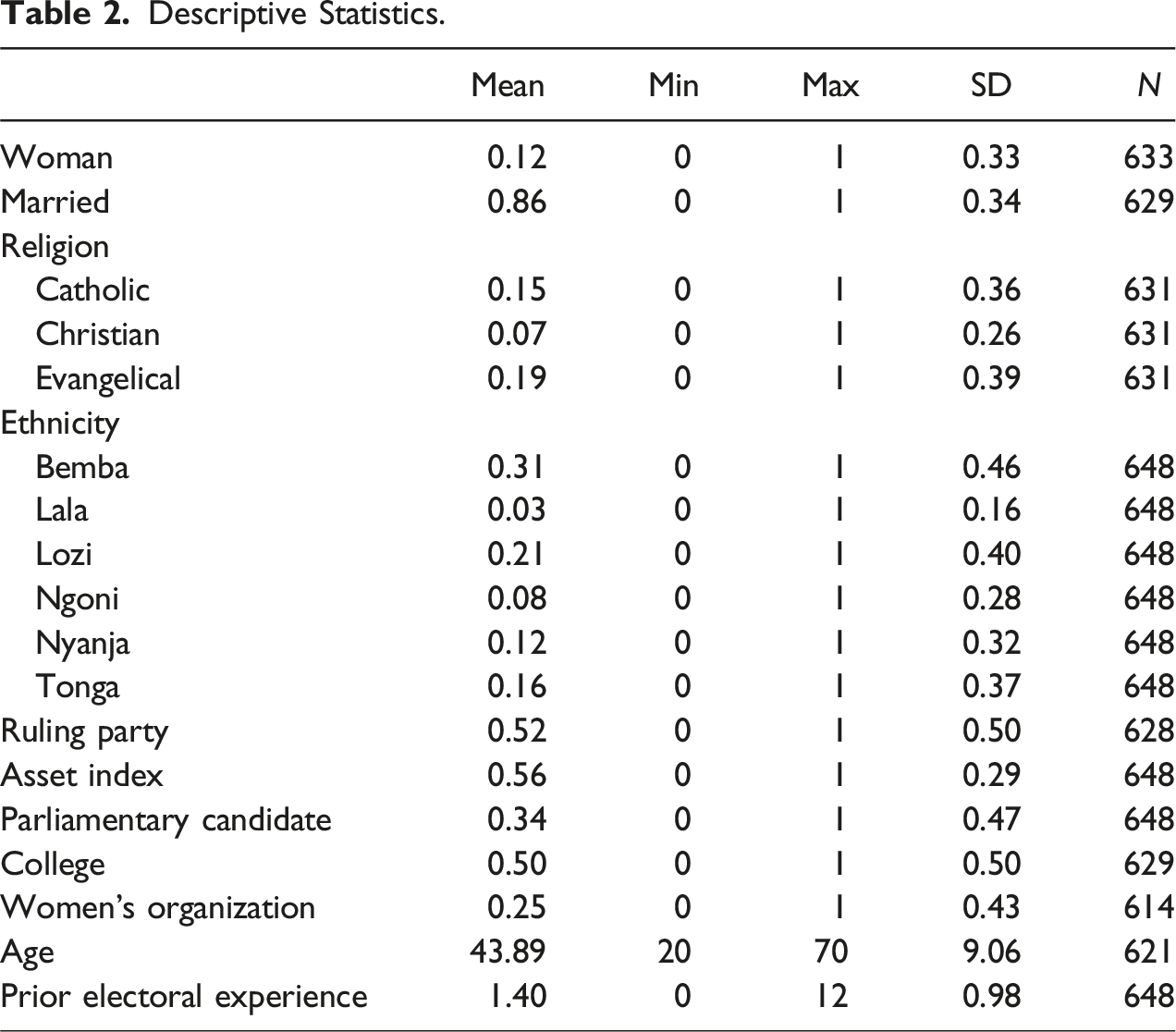
The majority of politicians in our sample are married (86 percent), and the most common religious affiliations are Evangelical (19 percent) and Catholic (15 percent). The sample includes the country’s main ethnic groups: Bemba (31 percent), Lozi (21 percent), Ngoni (9 percent), Nyanja (12 percent), and Tonga (17 percent). The sample is almost evenly split between ruling (52 percent) and opposition (48 percent) party members. About 34 percent were candidates for parliament, while the remaining 66 percent were candidates for ward councils. The average respondent’s previous electoral experience was running in 1.4 previous elections. Half the sample has a college degree and 24 percent claim membership in women’s organizations.
The survey’s design allows us to take a two-pronged approach to analyzing abortion-related preferences among Zambian politicians. First, we conduct an observational analysis to investigate the correlates of baseline attitudes toward abortion policy. Second, we assess whether a simple treatment that highlights the consequences of unsafe abortions on maternal mortality can persuade politicians to support policies that make it easier for women to receive an abortion. 10
Observational Analysis of Baseline Attitudes
To provide a baseline understanding of the correlates of abortion-related attitudes, we employ ordered logistic regression analysis using a survey outcome that was asked to all politicians without (and prior to) experimental manipulation: Abortion is currently legal in Zambia when necessary to save a woman’s life or to protect the well-being of her children. Do you think it should be made more restricted, less restricted, or stay the same? Responses to this question were coded trichotomously: more restricted, stay the same, or less restricted. This outcome serves as the first dependent variable discussed in the empirical analysis.
Experimental Analysis of Public Health Framing
Experimental Treatment Script.
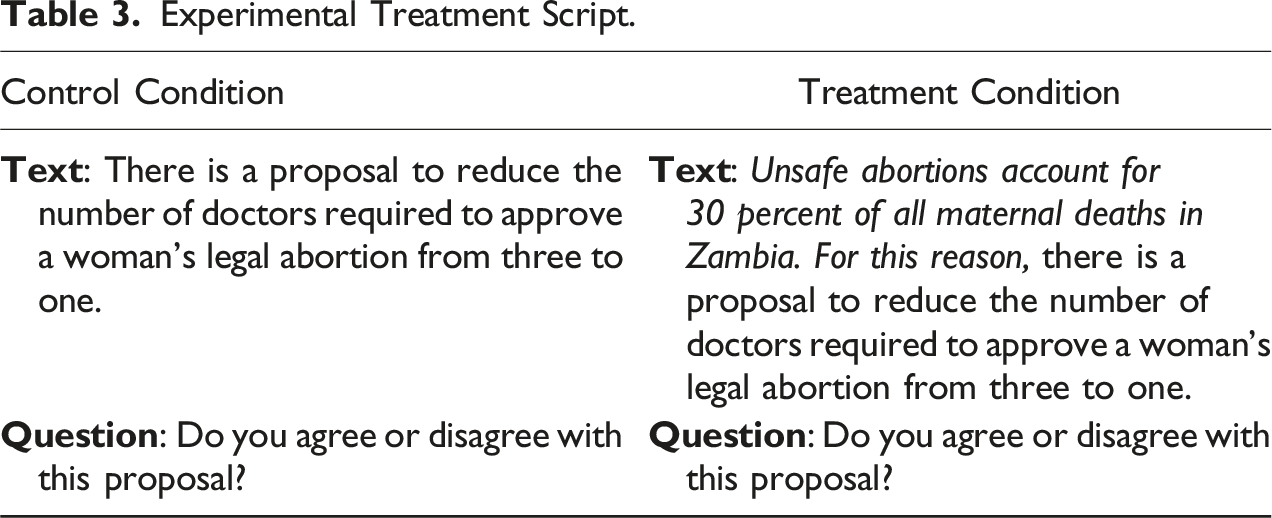
Immediately following the short treatment vignette, we asked policymakers whether they agreed or disagreed with the proposal using a 7-point Likert scale ranging from completely agree (7) to completely disagree (1). Our treatment and control group comparisons are conducted on this outcome using simple difference-in-means tests. Since we are interested in understanding how politicians’ demographic characteristics moderate the treatment effects, we present the treatment effects disaggregated by gender and other relevant factors. In providing tests of potential moderating mechanisms, we use variables included in the survey analysis such as marital status, education, tier of office contested, and an asset index. These are interacted with the treatment indicator in OLS regression models.
Balance diagnostics, presented in Table A1 in the appendix, lend credence to the inferences we can draw from the analysis of the survey experiment. Treated and control respondents are comparable across a wide range of demographic, political, and economic variables. Some minor exceptions include the proportion of politicians from the Tonga ethnic group (6 percentage points higher in the control group), the mean value of the asset index (0.5 higher in the control group), and the proportion of politicians who are members of women’s organizations (6 percentage points higher in the control group). To guard against the possibility that these imbalances are driving our results rather than the treatment itself, we present analyses with specifications that adjust for pre-treatment differences in addition to base specifications without any covariates.
Independent Variables
The survey captured a range of details about politician backgrounds that provide the necessary information to examine demographic correlates of abortion attitudes. Consistent with prior research, we expect women politicians will be more likely to support liberalizing abortion access when compared to their male counterparts. This variable is coded dichotomously.
We assess the relationship between abortion attitudes and economic resources in two ways. First, we treat the political office for which a candidate competes—member of parliament versus ward councilor—as an indirect measure of their access to economic resources. Candidates in our sample who run for national parliament or local ward councils are generally drawn from distinct socioeconomic strata. In Zambia, parties seek out wealthy individuals to run for parliament because they need to be self-financing to be electorally competitive (Arriola et al., 2022). For example, the average MP candidate spent over $20,000, most of it out of their own pocket, in the run-up to the 2016 elections (Arriola et al., 2021). By contrast, ward councilor candidates resemble the socioeconomic profile of the general population. Unlike their MP counterparts, these candidates for local office do not have the resources to fund campaigns; they depend either on the party or MP candidates to subsidize them. We therefore expect ward councilor candidates, who are relatively poorer than MP candidates, to be more supportive of liberalizing abortion access.
Additionally, we use a politician’s wealth as a direct measure of access to economic resources. Wealth is measured through an asset index that aggregates dichotomous responses to whether a candidate owns a vehicle, a house, a farm, a business, commercial property, or undeveloped land. We expect wealthier candidates to be more supportive of liberalizing abortion access.
Among other demographic factors, we control for marital status, which is coded dichotomously. We expect marital status to be correlated with less support for abortion liberalization. We also control for religious affiliation by coding respondents as Mainline Christian (e.g., Presbyterian or Methodist), Catholic, or Evangelical. We expect Catholics and Evangelicals in particular to be more likely to reject liberalization. While prior research suggests that ethnic identity could be correlated with abortion attitudes, we remain agnostic as to whether support for legalization varies significantly across Zambia’s larger ethnic groups (i.e., Bemba, Lozi, Ngoni, Nyanja, and Tonga).
To examine whether prior knowledge might affect how candidates respond to liberalizing abortion, we use two measures. We control for whether candidates are college graduates, and we control for whether candidates are members of women’s organizations. We expect both college graduates and members of women’s organizations to be more supportive of liberalizing abortion access. Additional controls include candidates’ birth year as well as political experience based on a count of their prior runs for office.
Analysis of Abortion Policy Preferences
We begin the empirical analysis by establishing a baseline for politicians’ attitudes toward abortion policy as it existed when the survey was conducted in Zambia. When asked if abortion policy should be made more restricted, less restricted, or stay the same, a majority of politician respondents prefer maintaining the status quo, regardless of gender. As the left panel of Figure 2 shows, 60 percent of women politicians and 58 percent of men politicians would choose to keep abortion policy as it stands in Zambia. Preferences on abortion policy change by electoral tier and gender: Women candidates prefer less restrictive abortion policy than men. Notes. The distribution of abortion policy preferences among men and women candidates by electoral tier. Darker (lighter) shades of color indicate preferences for more restrictive (less restrictive) policy change.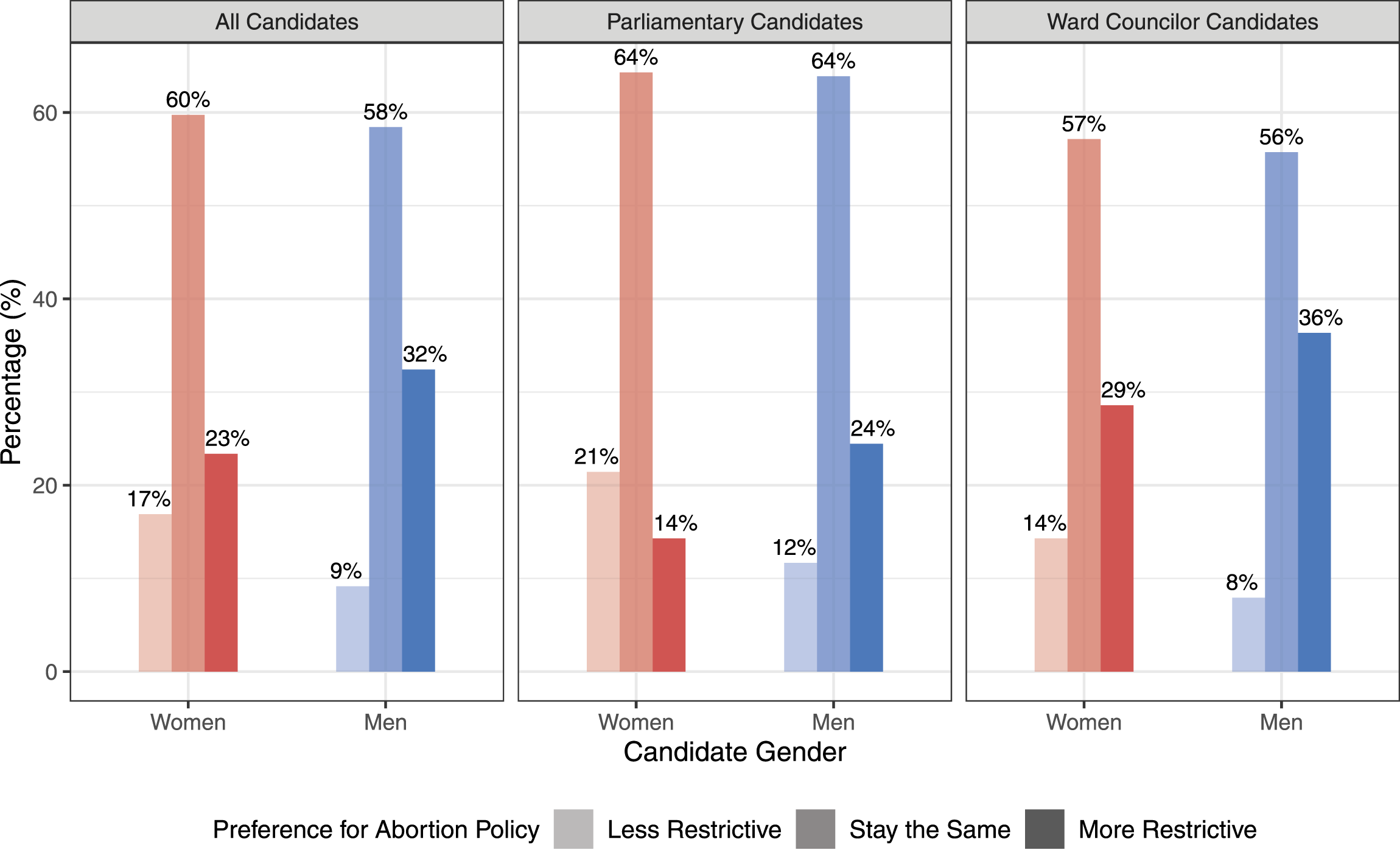
But there are significant gender differences when it comes to supporting policy change. A larger proportion of men politicians (32 percent) would prefer more restrictive abortion policy compared to women politicians (23 percent). Approximately 17 percent of women politicians indicate a preference for less restrictive abortion policy, but only 9 percent of men politicians state the same. Figure 2 further reveals that there are large differences between politicians who run at the national and local levels, even within gender. For example, while 24 percent of men parliamentary candidates would prefer more restrictive abortion policy, the rate rises to 36 percent among men ward councilor candidates. The differences among women are even wider: 14 percent of women parliamentary candidates prefer more restrictions, whereas 29 percent of women ward councilor candidates want the same.
Regression Analysis of Preferences on Abortion Policy Change.
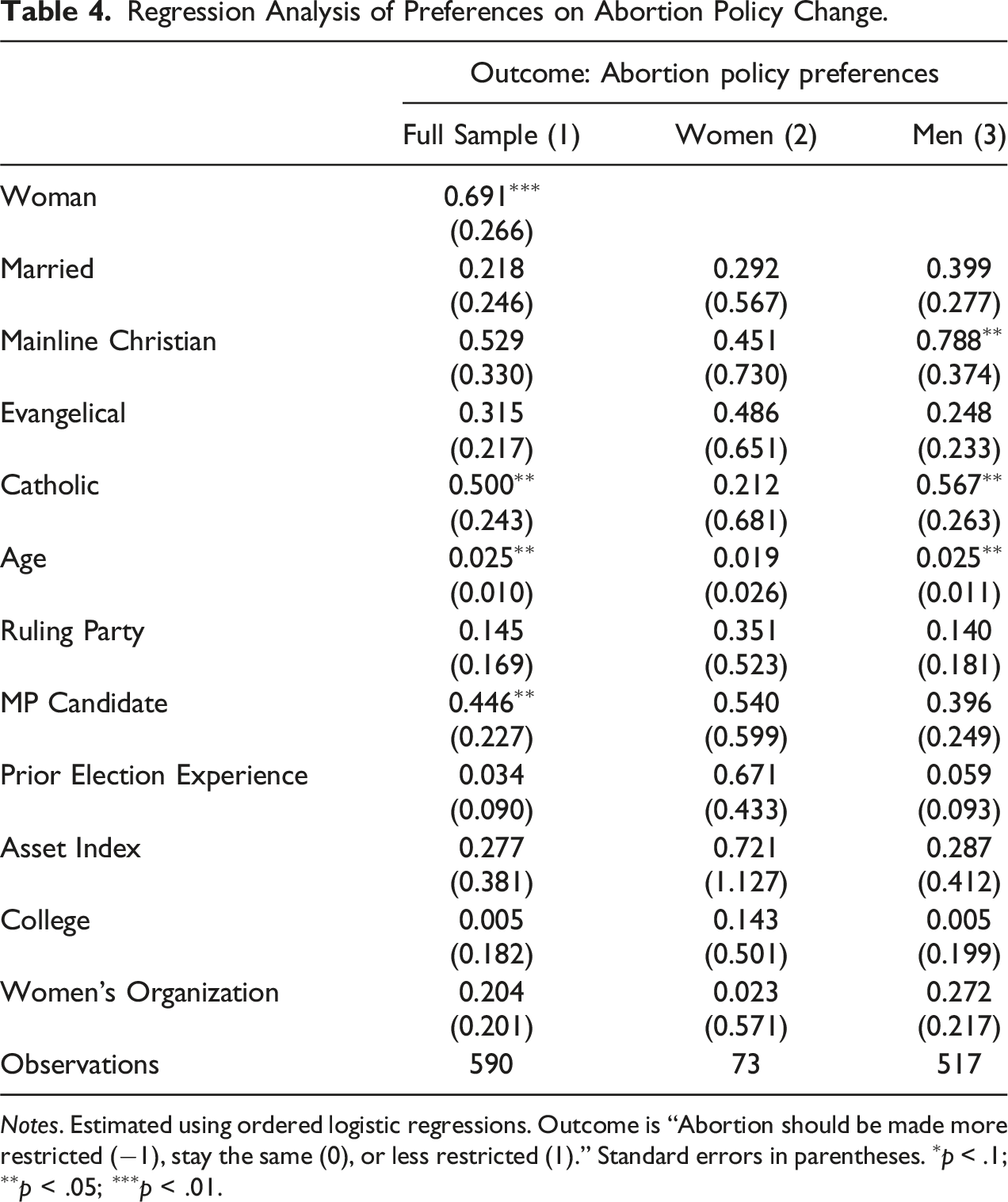
Notes. Estimated using ordered logistic regressions. Outcome is “Abortion should be made more restricted (−1), stay the same (0), or less restricted (1).” Standard errors in parentheses. ∗p < .1; ∗∗p < .05; ∗∗∗p < .01.
MP candidates appear to be more liberal in their attitudes toward abortion when compared to ward candidates. The positive coefficient indicates that MP candidates are more likely to support liberalizing abortion restrictions. This result is statistically significant at the 0.05 level in the pooled analysis, but fails to retain statistical significance in the subgroup analysis for women.
We observe that older candidates hold more liberal abortion policy preferences, as shown in the pooled analysis and the men subgroup analyses. But other demographic variables in Table 4 appear to have no systematic relationship with abortion policy preferences. The coefficients on marriage, religion, and education mostly fail to attain statistical significance. Male candidates that are mainline Christians appear to be marginally more supportive of liberalization, though this relationship does not hold in the women’s subgroup analysis. In the women’s subgroup analysis, Catholic women are less supportive of liberalization, an effect that does not hold among men. Membership in a women’s organization, a possible proxy for information and even revealed preference over reproductive rights, is uncorrelated with abortion policy preference. Neither electoral experience nor ruling party membership are associated with abortion policy preferences.
We now turn to discussing the experimental results. Recall that politicians in our sample, after expressing their initial preferences, were subsequently asked whether they would support the then-pending proposal to reduce the number of doctors’ signatures required for a woman to secure medical approval for a legal abortion. Before being posed this question, politicians in the treatment condition were informed about the prevailing mortality rate linked to unsafe abortions in the country. Politicians in our sample were thus effectively asked if they would support liberalizing legal access to the medical service in light of the negative health effects associated with existing restrictions.
The top panel of Figure 3 shows that the treatment on the consequences of unsafe abortion had no effect when examined among the full sample. However, when disaggregated by gender, it becomes clear that women politicians are significantly more likely to respond to the treatment regarding maternal mortality by increasing their support for the liberalizing proposal. The treatment effect is close to zero and fails to attain statistical significance in the sample restricted only to men politicians. Treatment effects by candidate electoral tier and gender: Women candidates respond more strongly to the experimental treatment regarding maternal mortality. Notes. Treatment effects from the experiment by candidate electoral tier and gender. Points represent average treatment effects estimated using linear regression while thick and thin lines represent 90% and 95% confidence intervals. Tabular presentation of results are found in Appendix Table A3.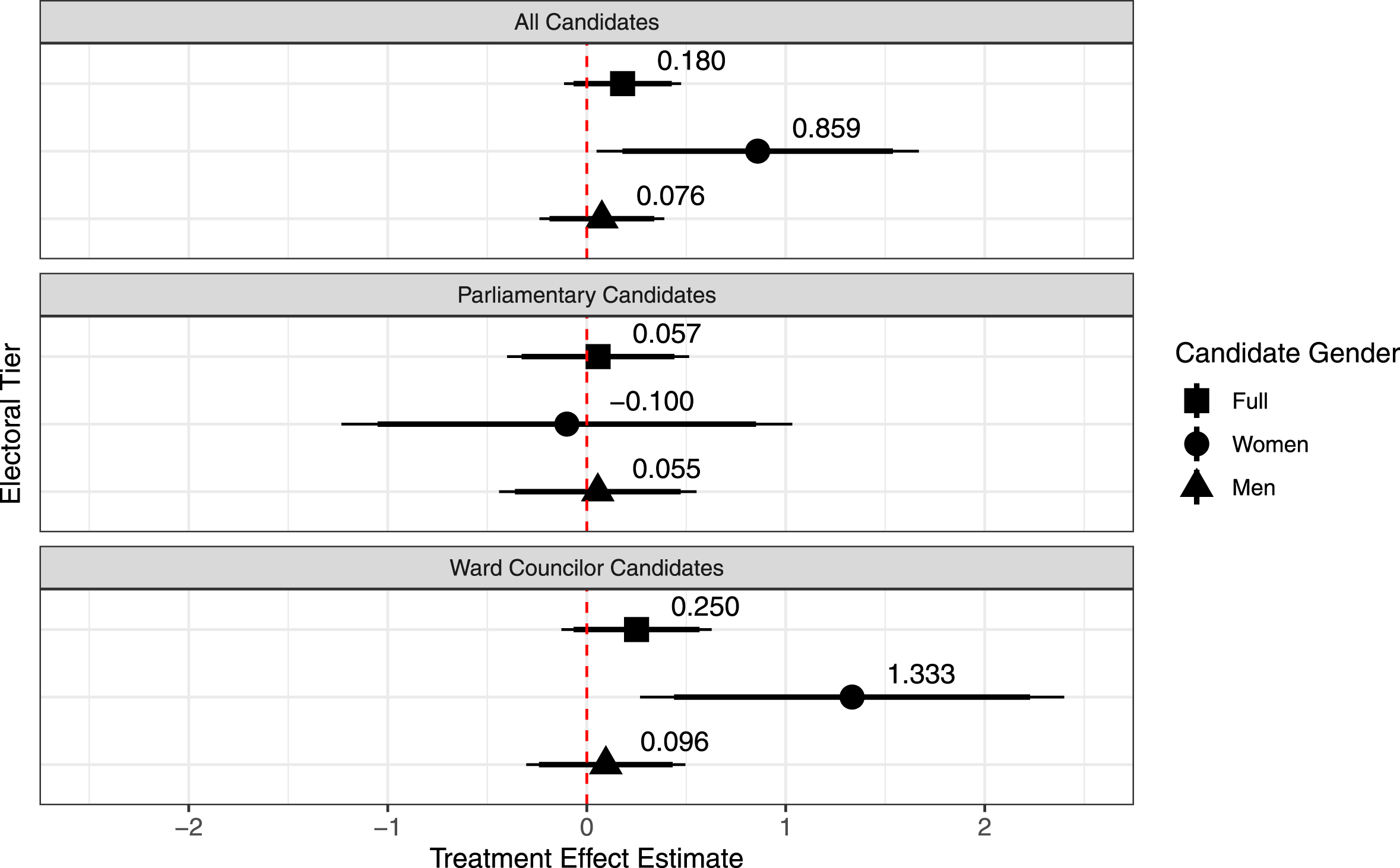
The middle and bottom panels in Figure 3 reveal the potential interaction between gender and other factors correlated with candidacy. We find that not all women politicians respond to the treatment in the same way. The treatment effect for women politicians in the middle panel is statistically indistinguishable from zero, suggesting that women who seek to become MPs in Zambia’s national parliament were unaffected by the additional information on maternal mortality. By contrast, in the bottom panel, the treatment effect for women is positive and statistically significant at the 0.05 level, indicating that women who run to become local ward councilors are updating their policy preferences when exposed to public health information. The treatment effect in the bottom panel suggests that this information alone can increase a woman ward candidate’s support for liberalizing abortion policy by nearly 19 percent (1.3 points on the 7-point scale). We further show in supplementary analyses presented in the appendix that these effects hold even when controlling for the candidates’ prior abortion policy preferences (see Appendix Table A4) or the full set of pre-treatment controls (see Appendix Tables A5 and A6). Finally, as expected, we find that men politicians remain unaffected by the public health treatment, regardless of whether they are running as MP or ward candidates.
Figure 4 provides greater clarity on the differences across candidate type and gender. MP candidates hold, on average, more liberal attitudes toward abortion policy when compared to ward councilor candidates. In the control condition, women MP candidates hold the most liberal positions (4.50), while women ward councilor candidates are the most conservative (3.52). Yet, when exposed to the information on maternal mortality in the treatment condition, it is the women ward councilor candidates who exhibit the largest shift toward liberalizing abortion. Notably, men ward councilor candidates, who hold similarly conservative positions in the control condition, show no such updating. Average responses on the experimental outcome by candidate electoral tier and gender treatment condition: Treatment effects among women candidates are driven primarily by women ward councilor candidates. Notes. Subgroup analysis of the treatment effects by candidate type and gender. Outcome is “Agree to reduce the number of doctors required” (7-point scale). Bars represent means for the treated and control conditions for each candidate category. The error bars present 95% confidence intervals for the means. The connecting lines are from two-tailed difference-in-means tests. ∗p < .1, ∗∗p < .05, ∗∗∗p < .01.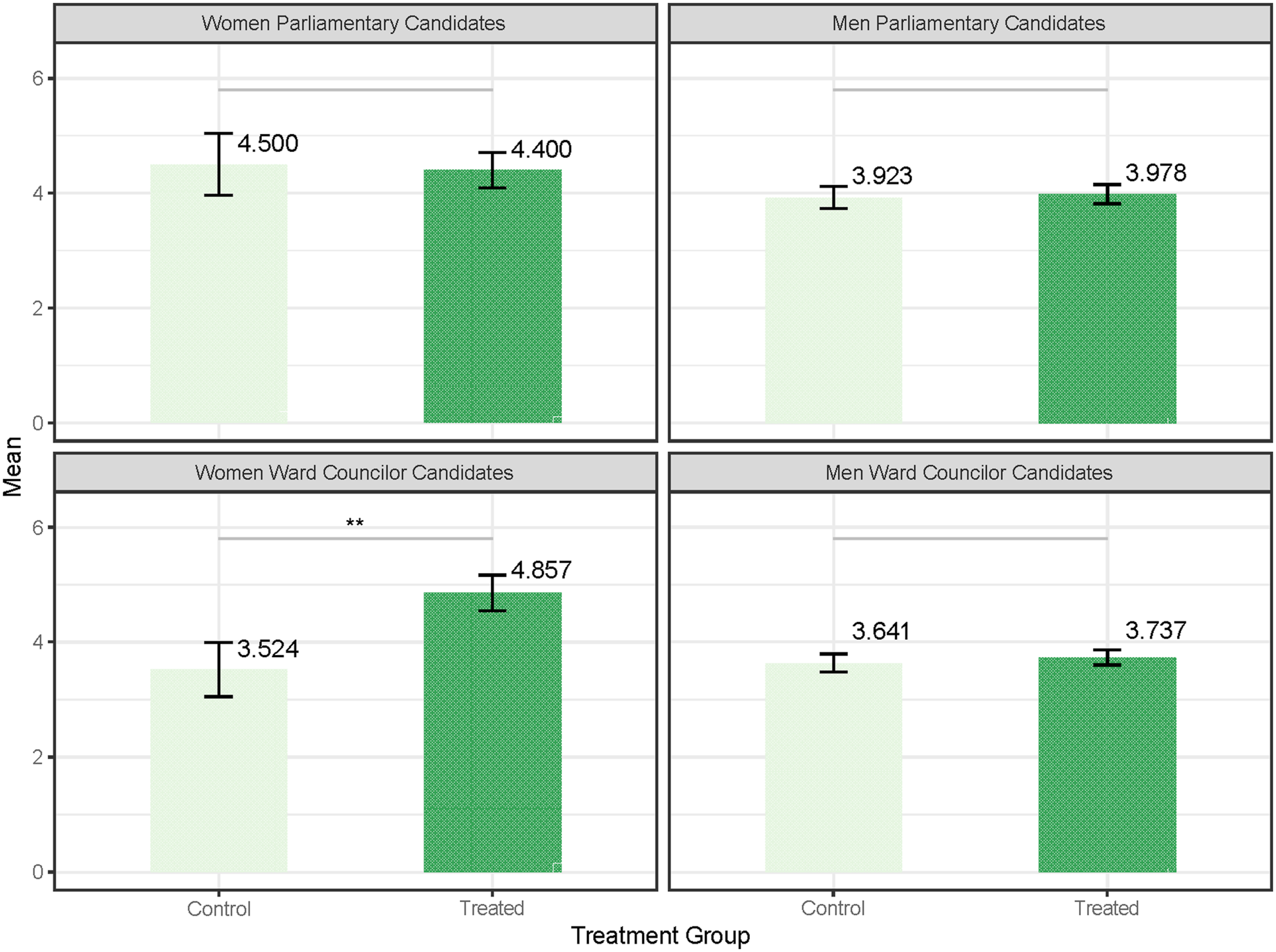
Figure 5 further shows that the framing treatment moved the very women who originally reported having the most conservative abortion policy preferences. Using the pre-treatment measure of preference for abortion policy (used as the outcome for analyses in Table 4) to examine subgroup heterogeneity in treatment effects, women ward candidates who said they would prefer abortion to be more restricted appear to be most responsive to the public health treatment, moving from an average of 2.33 among control to 5.25 among treated (2.92 change on a 7 point scale, p < .001). The magnitude of the treatment effects was slightly smaller among women ward candidates who said that they would like abortion policy to stay the same prior to treatment (1.28 on a 7-point scale, p < .05). In contrast, the treatment seems to have little effect among women ward candidates who had already reported that they would prefer abortion policy to become less restrictive; the difference between the treated and control groups is −0.25 points and is statistically indistinguishable from zero at conventional levels. Heterogeneity in treatment effects among women ward candidates by pre-treatment abortion policy preferences: Treatment effects are largest for women ward candidates that reported having the most conservative pre-treatment abortion policy preferences. Notes. Subgroup analysis of treatment effects by pre-treatment preference for abortion policy change among women ward candidates. The outcome is “Agree to reduce the number of doctors required” (7-point scale). Bars represent means for the treated and control conditions for each level of the pre-treatment policy preference. The error bars present 95% confidence intervals for the means. The connecting lines are from two-tailed difference-in-means tests. ∗p < .1, ∗∗p < .05, ∗∗∗p < .01.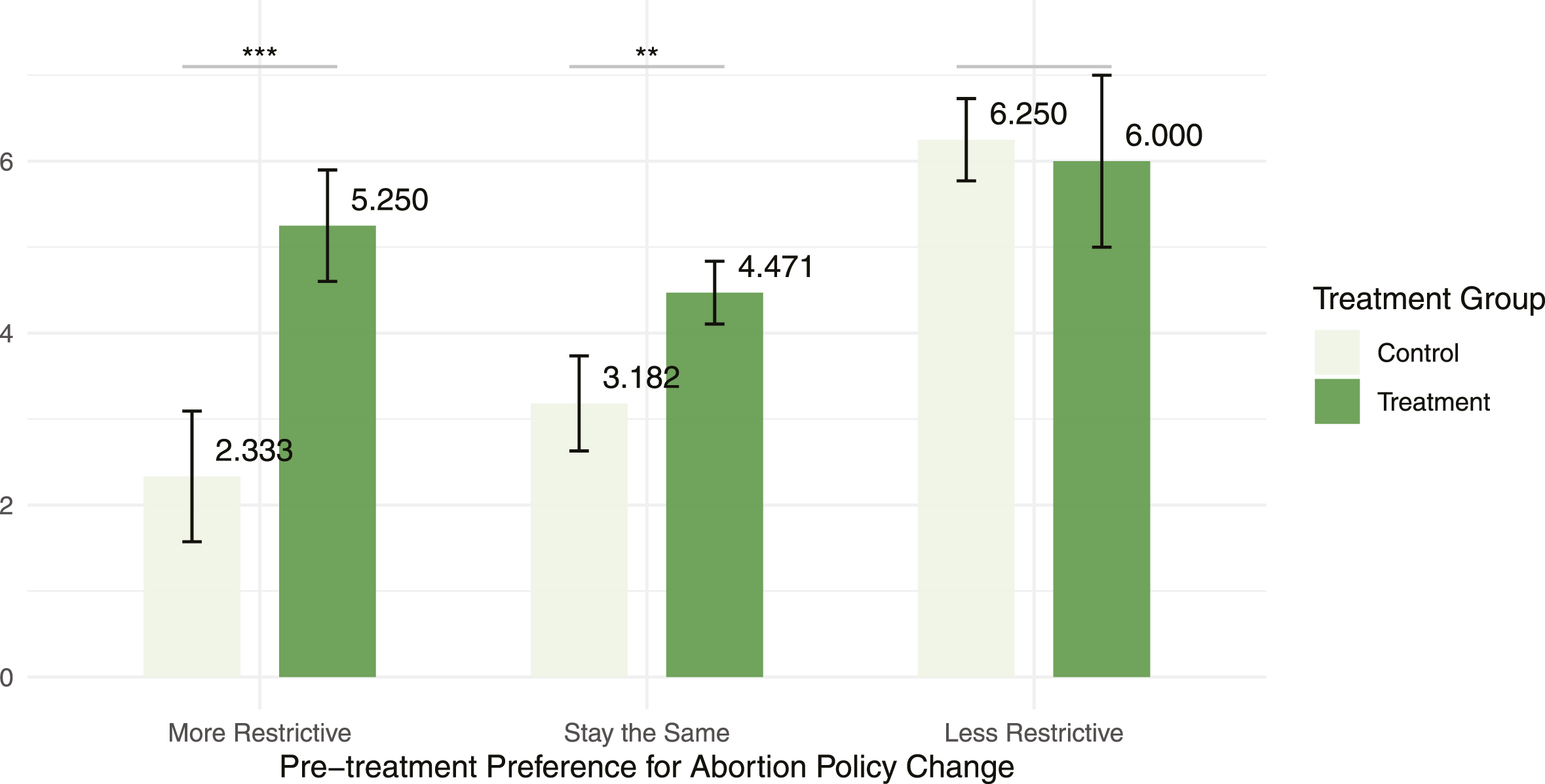
Assessing the Mechanisms for Policy Preference Change
The findings in the previous section indicate that the gender effect in updating abortion policy preferences is driven largely by the subset of women politicians competing to become ward councilors (local politicians) rather than MPs (national politicians). To account for this apparent divergence, we suggest that focusing on the intersection of gender and wealth can help illuminate why women involved in local—rather than national—politics might be more amenable to changing their positions on abortion policy after being exposed to a public health framing on maternal mortality in Zambia.
Wealth as the Mechanism for Policy Preference Change
Why are women politicians with fewer financial resources more likely to be moved by a treatment regarding the human cost associated with unsafe abortion? In Zambia, women who enter local politics are typically from lower socioeconomic strata. Like the average Zambian woman, these local politicians have relatively few resources to circumvent the multiple legal and medical obstacles to managing their fertility. Consequently, when the health risks linked to existing abortion conditions are made salient to them, women politicians competing for local offices are more likely to understand that they themselves—or women they know—may have to pay the costs, financially and physically, if policy remains unchanged. By contrast, women who run for parliament in Zambia are from wealthier backgrounds, enabling them to afford the high costs of personally paying for election expenses (Arriola et al., 2021). 12 For these women, their greater wealth affords them greater freedom from the legal regulations that might otherwise limit their choices across a range of domains. Existing abortion policy simply poses less of an obstacle to their exercise of reproductive rights. Women MP candidates are therefore unlikely to have been negatively affected by financial constraints in accessing reproductive healthcare. For these politicians, family planning services can be readily secured through private clinics, which are less likely to require spousal consent, but at a relatively higher financial cost.
To corroborate our expectations regarding the interaction between gender and wealth among women candidates, we first confirm that women seeking to become local ward councilors have, as a group, lower average wealth than women pursuing national parliamentary seats. Figure 6 shows that women ward candidates do, in fact, possess relatively fewer assets (i.e., business, commercial property, land, farm, house, vehicle) than women MP candidates. While women MP candidates possess over 75 percent of those assets on average, women ward candidates hold just over 50 percent of such assets on average. Asset index for women parliamentary and ward councilor candidates: Ward candidates have lower average wealth than parliamentary candidates. Notes. Figure shows mean values of the asset index (business, commercial property, land, farm, house, vehicle) for women MPs and ward councilors. The bars reflect the means with 95 percent confidence intervals. The connecting line is from a two-tailed difference-in-means test. ∗p < .1, ∗∗p < .05, ∗∗∗p < .01.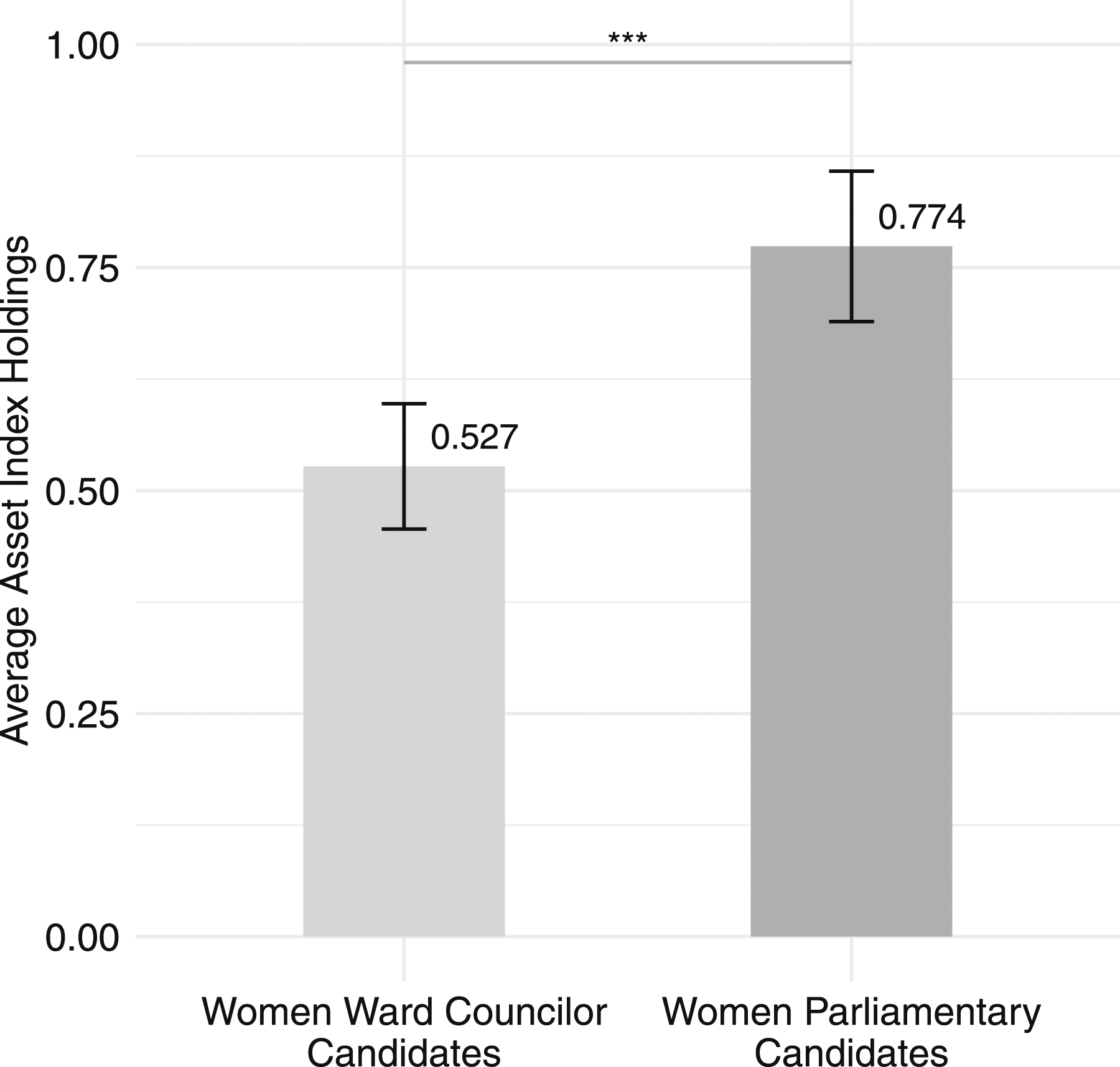
The asset index maps on to real distinctions among women candidates. Illustrating candidate type differences across each asset category, Figure 7 shows that women MP candidates are more likely than women ward candidates to own assets in five of the index’s six categories. Consider, for example, that 82 percent of the women among MP candidates own a business, but only 49 percent of the ward candidates do so, a statistically significant difference (p = .004). Similarly, women MP candidates are more than twice as likely to own commercial property compared to women ward candidates (43 percent versus 20 percent, p = .036), they are more likely to own land (71 percent of MP candidates versus 41 percent of ward candidates, p = .010), and they are more likely to own a farm (79 percent of MP candidates versus 49 percent of ward candidates, p = .011). Women MP candidates are also more likely to own a vehicle compared to women ward candidates (93 percent versus 65 percent, p = .007). Owning a home is the single category in which there is no statistically significant difference among women candidates. Individual assets among women parliamentary and ward councilor candidates. Notes. Figure shows the proportion of women MPs and ward councilors owning individual types of assets. The bars reflect the means with 95 percent confidence intervals. The connecting lines are from two-tailed difference-in-means tests. ∗p < .1, ∗∗p < .05, ∗∗∗p < .01.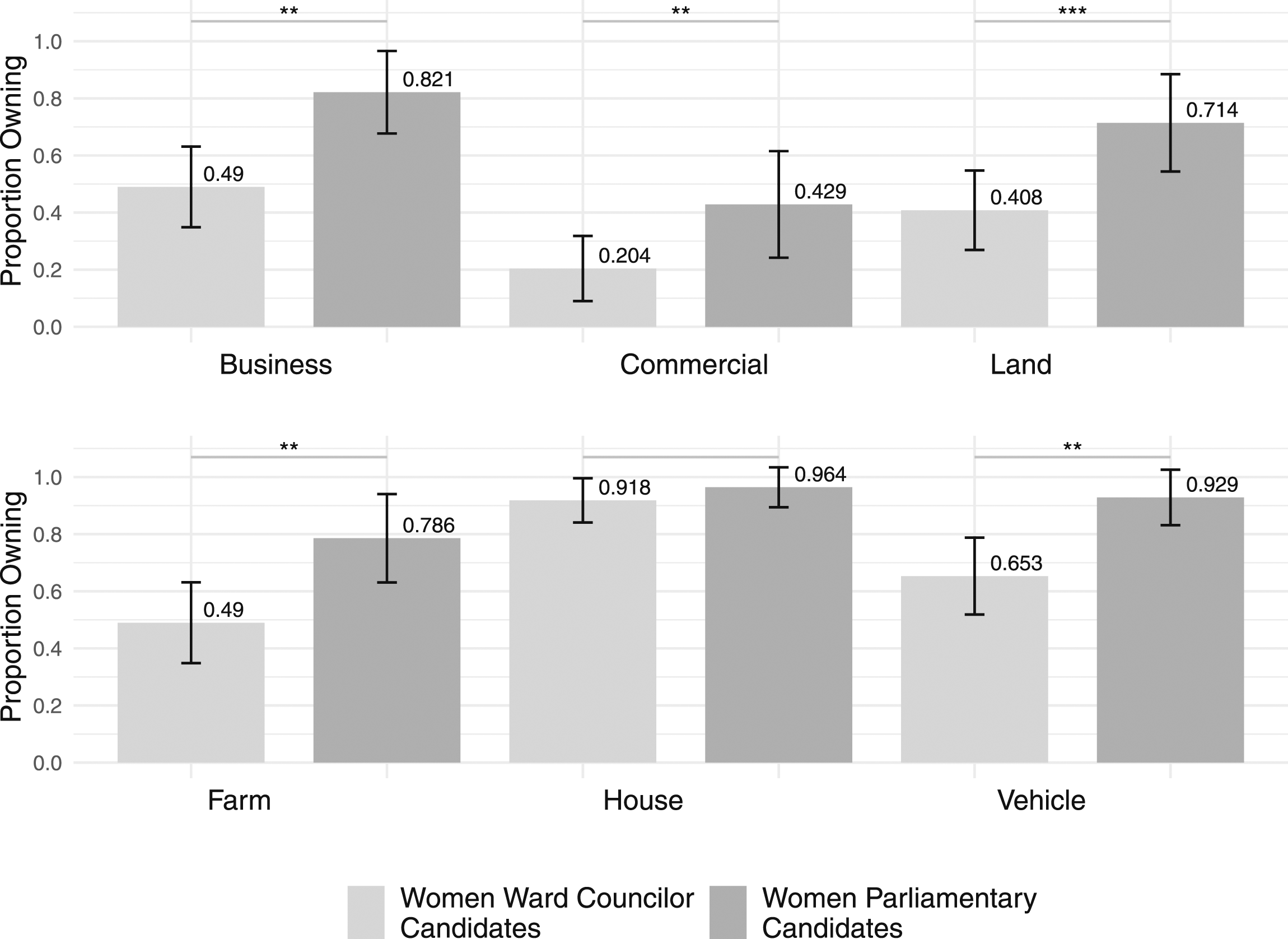
We find that the effects of the public health framing among women politicians are conditioned by wealth. Figure 8 shows that women candidates with lower wealth are systematically more likely to be moved by the treatment. Appendix Table A7 presents the associated tests. By interacting the treatment variable with the asset index, we find a negative interaction effect that is statistically significant at conventional levels for both specifications with and without the full set of pre-treatment controls for women candidates only, as shown in subfigure (b). The negative sign on the interaction term suggests that women with less wealth are systematically more likely to be affected by the treatment. These women are far more likely to support the liberalizing proposal (i.e., reducing the number of required doctor signatures) after being informed of the human cost associated with unsafe abortion. Conversely, women candidates with more wealth are less likely to be moved by the treatment in support of the liberalizing proposal. For example, at the 25th percentile of the asset index (0.33 on the 0 to 1 index), being exposed to the treatment leads to approximately a 2.06 average increase (on the 7-point scale) in a woman’s support for the liberalizing proposal. However, at the 75th percentile of the asset index (0.83 on the 0 to 1 index), exposure to the same treatment only leads to a 0.30 average increase for the proposal. In line with our intuition, we observe no such effect among men candidates as shown in subfigure (a). Treatment and wealth interaction: Treatment increases support for abortion liberalization among less wealthy women candidates (a) Men Candidates (b) Women Candidates. Notes. Figure reports heterogeneity in treatment effects by candidate wealth. The points represent the treatment effect estimate while the lines represent the 95 percent confidence intervals. Regression models from which the plot is generated are reported in columns (6) and (4) in Appendix Table A7.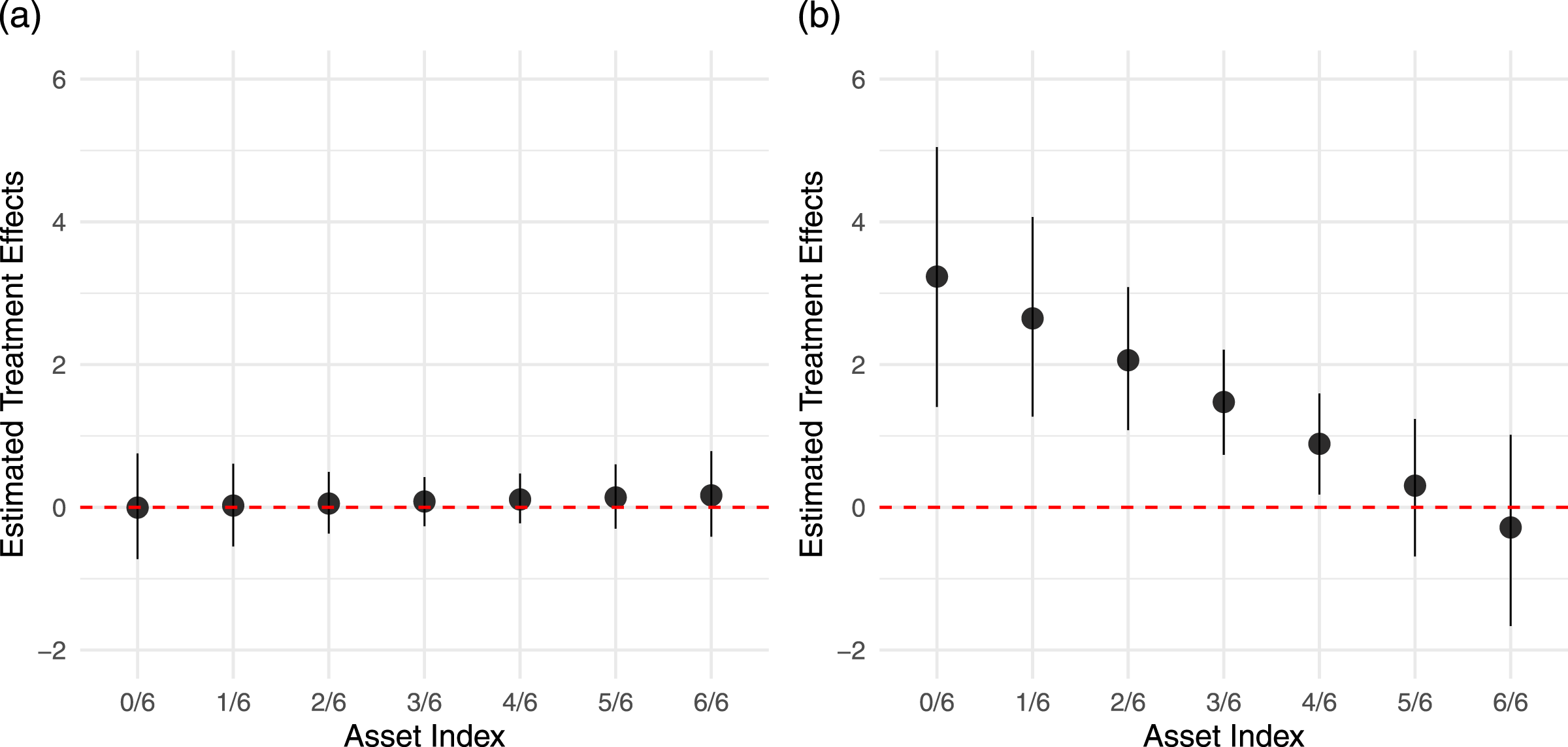
We further probe the plausibility of our claim by replicating the analysis among the women who ran to become ward councilors. In Figure 9, which is drawn from Appendix Table A9, we again find that the treatment alone has a statistically significant and positive effect on women ward candidates’ support for the liberalizing proposal. We also replicate the significant negative interaction between the treatment and the asset index among women ward candidates. Women politicians with less wealth are far more likely to support the liberalizing proposal after being exposed to the treatment. Consider once more a woman ward candidate at the 25th percentile of the asset index: when compared to the control condition, exposing her to the treatment leads to a 2.71 average increase (on the 7-point scale) in support of the liberalizing proposal. By contrast, at the 75th percentile of the asset index, there is effectively no difference between a woman candidate in the treatment or control conditions; the average difference between them is −0.13 on the 7-point scale. Treatment and wealth interaction: Treatment increases support for abortion liberalization among less wealthy women ward candidates (a) Women MP Candidates (b) Women Ward Candidates. Notes. Figure reports heterogeneity in treatment effects by candidate wealth. The points represent the treatment effect estimate while the lines represent the 95 percent confidence intervals. Regression models from which the plot is generated are reported in columns (4) and (2) in Appendix Table A9.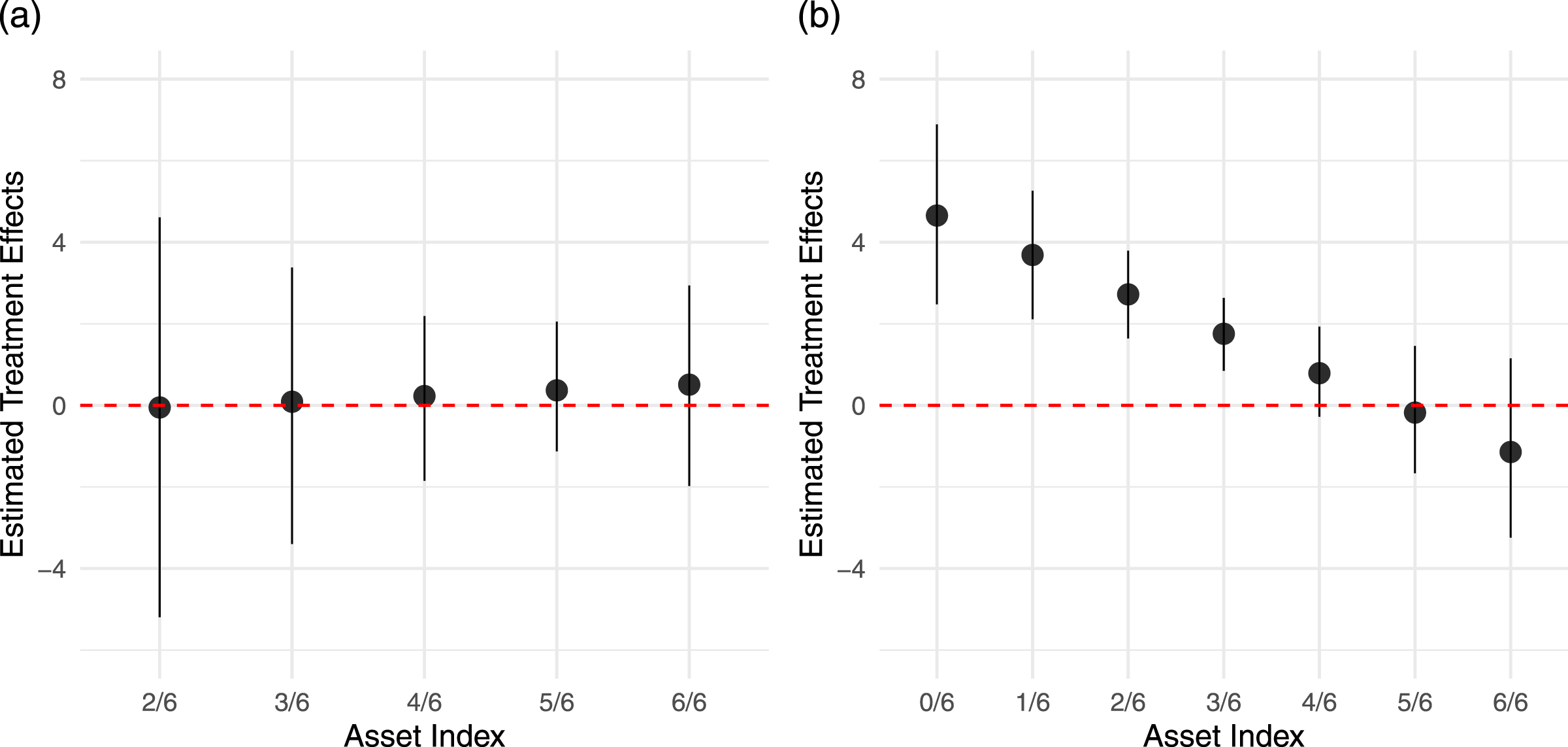
It is important to acknowledge that the preceding analyses of heterogeneity in politician wealth are conducted on small samples (N = 75 for all women candidates, N = 49 for women ward councilor candidates). To address concerns over the validity of inferences based on small sample sizes, we conduct randomization inference that tests against the null of constant effects (i.e. no heterogeneity in candidate wealth) equal to the estimated ATE. We present these results in Appendix Figures A1 and A2 as well as Tables A10 and A11. We are able to reject the null hypothesis of constant effects, reinforcing the validity of the findings reported in Figures 8 and 9.
Addressing Alternative Explanations
Treatment and Marriage/Identity Interactions: Gendered Effects on Abortion Liberalization Preferences Are Unlikely to Be Driven by Marital Status or Religious Identity.
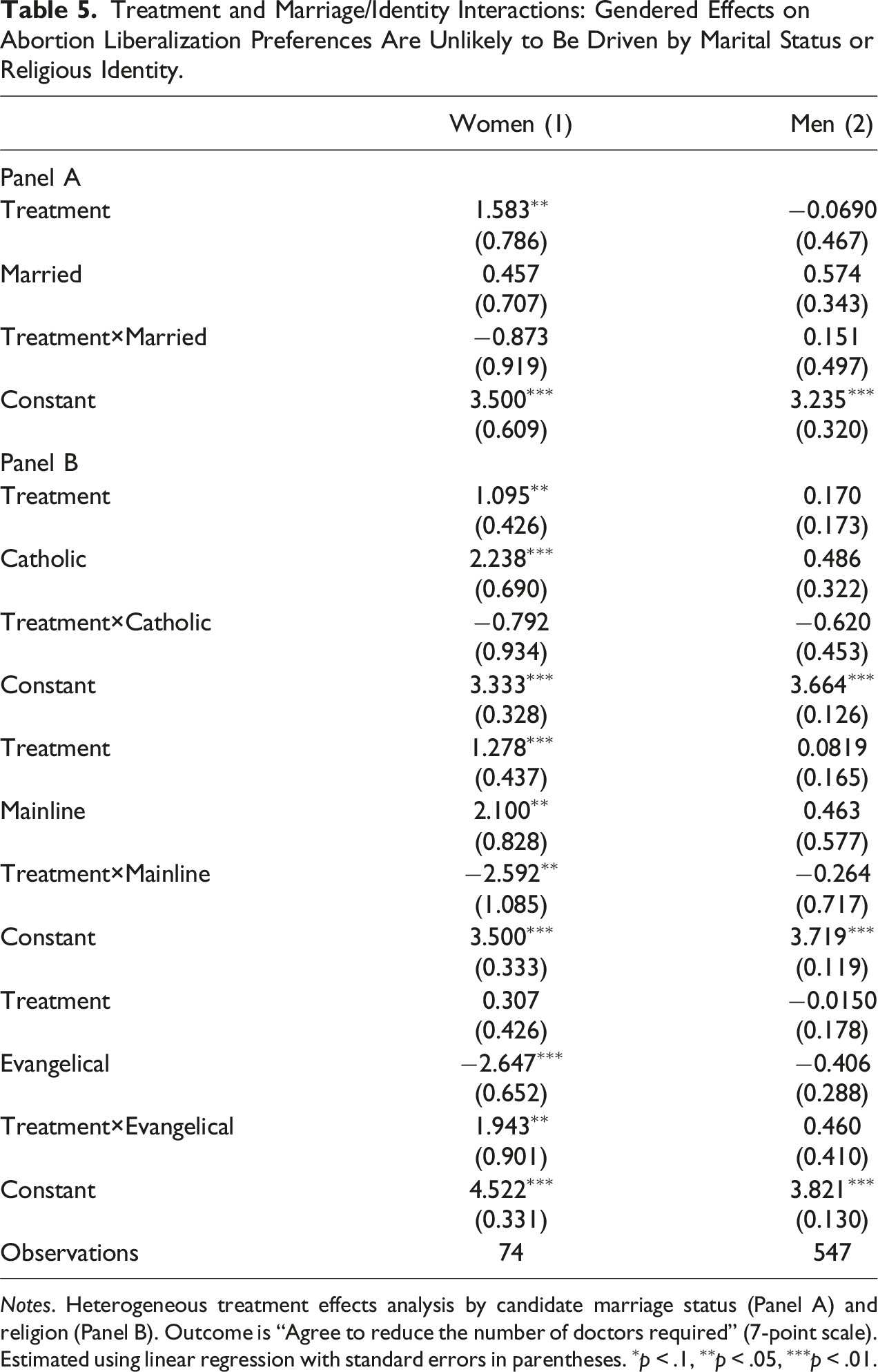
Notes. Heterogeneous treatment effects analysis by candidate marriage status (Panel A) and religion (Panel B). Outcome is “Agree to reduce the number of doctors required” (7-point scale). Estimated using linear regression with standard errors in parentheses. ∗p < .1, ∗∗p < .05, ∗∗∗p < .01.
Religious affiliation has been previously found to be a significant predictor of more conservative abortion attitudes. In Panel B of Table 5 and Appendix Table A14, we find that the information treatment is not systematically conditioned by religious adherence among Catholics, whether men or women. The effects move in opposite directions for different religious groups. Whereas women candidates who belong to Mainline Christian denominations are more likely to liberalize their views after being exposed to the information treatment, women candidates who are in Evangelical faith traditions are more likely to hold onto conservative positions. Again, as with previous findings, these particular denominational effects are gendered; they do not hold among men candidates.
Ethnicity also does not seem to play a consistent role in driving women candidates’ responses to the treatment. Both women and men candidates in our sample are ethnically diverse. In Appendix Table A15, we report that women candidates who identify as Ngoni are less likely to support the liberalizing proposal. The same is true for men who identify as Bemba. Furthermore, when examining treatment-ethnicity interactions, we find very little evidence that the treatment resulted in heterogeneous treatment effects across ethnic groups (see Appendix Table A16).
Treatment and Knowledge Interaction: Gendered Effects on Abortion Liberalization Preferences Are Unlikely to Be Driven by Knowledge.
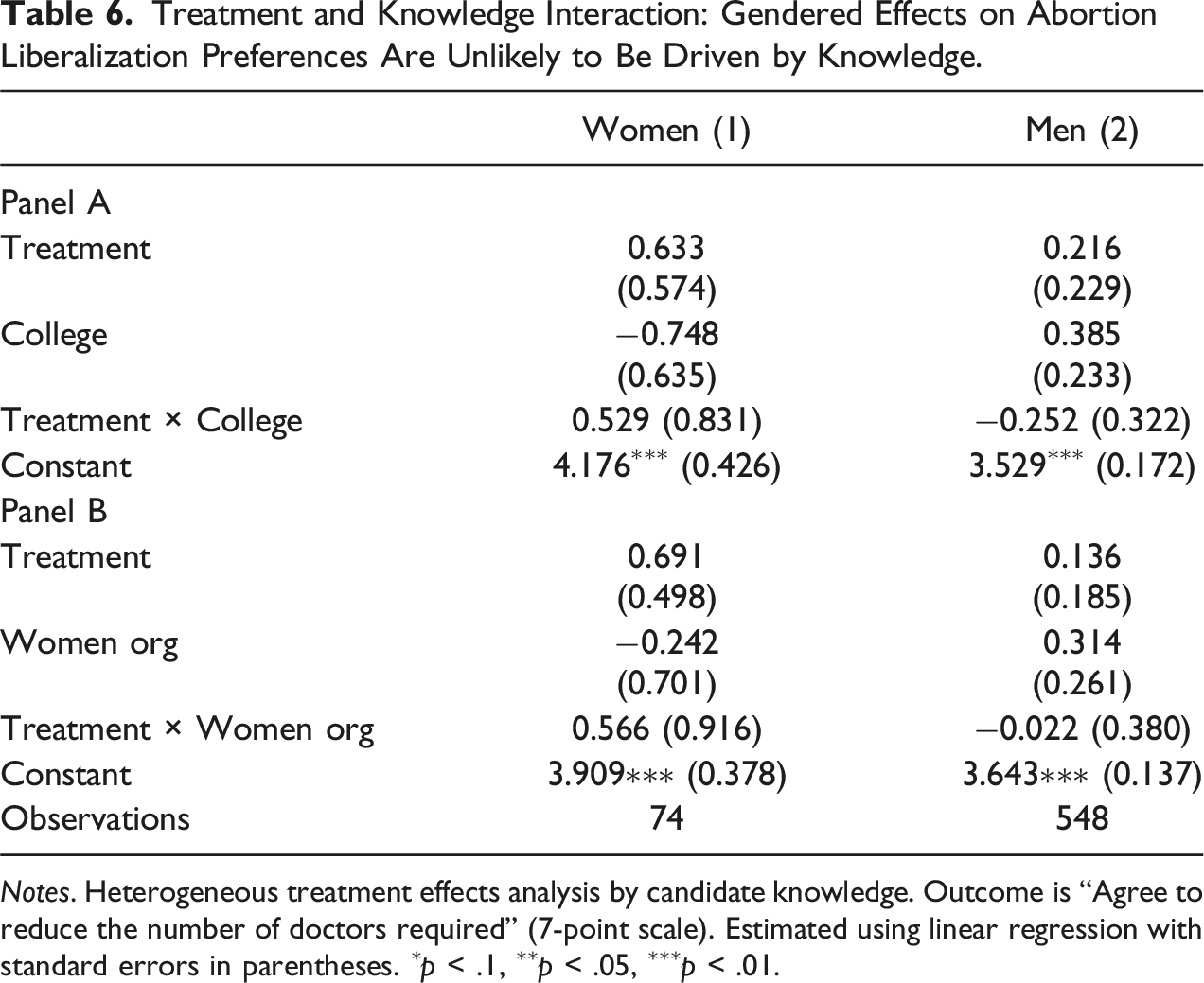
Notes. Heterogeneous treatment effects analysis by candidate knowledge. Outcome is “Agree to reduce the number of doctors required” (7-point scale). Estimated using linear regression with standard errors in parentheses. ∗p < .1, ∗∗p < .05, ∗∗∗p < .01.
Conclusion
While the human cost associated with restrictive abortion policies have been documented by researchers in medical and other scientific disciplines, social scientists have yet to accumulate the insights necessary to understand the conditions in which elected politicians might be willing to use such information to implement reforms aimed at improving the health and wellbeing of women and their families. In investigating how candidates for office respond to public health treatments regarding the impact of abortion policy on maternal mortality—namely, emphasizing the importance of saving women’s lives—we find that such a framing only produces a response from a subset of women candidates and none from men candidates. We find that women candidates are more likely to support liberalizing abortion access mainly when they come from lower economic strata.
Our findings help to nuance the literature on substantive representation by detailing how — beyond critical mass or institutional context — the varied socioeconomic realities of women shape their actions as political representatives, particularly in countries of the Global South. We provide suggestive evidence that a key mechanism affecting their support for liberalizing reform is economic rather than identity or information-based. Further research is needed to corroborate this finding and establish to what extent women candidates see themselves as representatives of their gender when their lives are as likely to be conditioned by other salient inequalities in their societies. In this respect, our work provides a baseline for future research to assess the impact of the different types of framings employed by social movements to influence policymakers. Additional research would also consider how partisanship—while not as pertinent in the Zambian case, but important elsewhere—may also shape abortion liberality across the globe.
The findings presented here also help illuminate why the heterogeneity among women politicians should be examined more systematically, particularly in understanding how they might shift their policy preferences on sensitive or controversial issues. Since arguments for policy reform are unlikely to be based or justified solely on an individual’s gender identity, we must understand how claims for changing policy might be used to activate other socioeconomic cleavages that structure women’s lives, whether based on class, race, ethnicity, or religion. Understanding how alternate framings influence women politicians will enable researchers to better account for consequential policy shifts—or the lack thereof—as women increasingly participate in governance around the world.
Supplemental Material
Supplemental Material - Policymakers’ Abortion Preferences: Understanding the Intersection of Gender and Wealth
Supplemental Material for Policymakers’ Abortion Preferences: Understanding the Intersection of Gender and Wealth by Leonardo R. Arriola, Donghyun Danny Choi, Justine M. Davis, Melanie L. Phillips, and Lise Rakner in Comparative Political Studies.
Footnotes
Acknowledgments
We thank survey enumerators Bwale Chungu, Chichi Davison, Francine Chiluba, Grace Kyungupengu, Mildred Bwalanda, Charity Mills, Kawide Nakasamum, Amon Phiri, Fortune B. Kanyembo, Kalonde Siulapwa, Patrick Chilumbwa, Stephen Emmanuel Mwale. Additionally, we thank our project coordinator Beverly Shicilenge.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research funding was kindly provided by the Peder Sather Center for Advanced Study at UC Berkeley and the project on “Political Determinants of Sexual and Reproductive Health: Criminalization, Health Impacts and Game Changers” sponsored by the Norwegian Research Council (project number 248159). This research was approved by the UC Berkeley Office for the Protection of Human Subjects under protocol number 2015-12-8222.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.