
Abstract
A large body of literature investigates whether increasing the number of women in legislative office translates into policies that benefit women in society. This research builds upon theories about descriptive and substantive representation. However, these theories may not travel well to authoritarian contexts, where we see some of the largest gains in women legislators in recent years. This article unpacks the link between women’s descriptive representation, healthcare spending, and health outcomes by regime type. Using a sample of 169 countries from 2000 to 2018, we find that the percentage of women legislators is associated with increased healthcare spending across all regimes. However, women’s health outcomes do not improve with women’s descriptive representation in closed autocracies. Meanwhile, the results for democracies and electoral autocracies are similar, suggesting that even limited vertical accountability through semi-competitive elections may facilitate substantive representation of women.
Introduction
It is no secret that women are underrepresented in political office. They account for around 50% of the global population but make up less than 25% of parliaments worldwide (IPU, 2022). Many argue that attaining descriptive representation, such as by increasing the percentage of women in the legislature, is important because it will bring about greater substantive representation through the adoption of policies that benefit women in society (Chattopadhyay & Duflo, 2004; Clayton & Zetterberg, 2018; Franceschet & Piscopo, 2008; Höhmann, 2019; Phillips, 1995; Westfall & Chantiles, 2016; Williams, 2000). While historically, “the concept and practice of representation have had little do to with democracy” (Pitkin, 1967, p. 2), the link between descriptive and substantive representation is based on assumptions of democratic accountability. Yet, research suggests that even in autocracies, women can successfully pursue their interests, at least to a certain degree, for example, by advancing women’s social and political rights (Donno et al., 2022) and through increased funding for policies that women prioritize to a greater extent than men (Forman-Rabinovici & Sommer, 2019). At the same time, the literature also finds that autocrats adopt redistributive policies for strategic reasons, such as to demonstrate power or to gather support before elections (Han, 2021; Robles, 2021). Thus, the adoption of policies that women prioritize could reflect efforts by authoritarian regimes to consolidate power rather than the substantive representation of women. As a result, such policies might not have the direct effect on citizens’ lives that theories about descriptive and substantive representation predict.
In this article, we unpack the link between women’s descriptive and substantive representation across regime types, focusing specifically on healthcare spending and health outcomes for women. We assess whether the effects of policies designed to benefit women travel through the chain of implantation to reach citizens on the ground and whether this relationship varies depending on regime type. We argue that autocracies increasingly adopt women-friendly policies as part of a cooptation and signaling game, and therefore, these policies have limited effects on citizens. Specifically, autocracies use “gender-washing” strategies, meaning they adopt policies that seemingly aim to improve the status of women to appear more progressive and democratic. The goal is to enhance the regime’s legitimacy and reputation, both at home and abroad (Bjarnegård & Zetterberg, 2022; Donno et al., 2022). For domestic audiences, “gender-washing” helps coopt the support of women, while for international audiences, it signals alignment with international norms, which can foster economic partnerships and attract foreign aid.
This has implications for the efficacy of women legislators once they attain office. The need for legitimacy is universal (Tannenberg et al., 2021). All politicians seek to maintain office, and one of the ways legislators can achieve this is through policy formulation. In authoritarian regimes, legislatures serve cooptation, powersharing, and information functions (Gandhi & Przeworski, 2007; Magaloni, 2008; Truex, 2016). To achieve these functions, legislators must be able to propose policies and amend government proposals. Research shows that even in closed autocracies, legislators are successful at affecting policy changes (e.g., Desposato, 2001; Krol, 2021). In addition, authoritarian governments may alter their spending to complement other seemingly pro-women policies. For this reason, we expect that increases in women legislators regardless of regime type should translate into concrete changes in government spending in the areas women tend to prioritize. Previous research suggests that women typically assign greater priority to healthcare spending when compared to men (Clayton et al., 2019; Funk & Philips, 2019; Gottlieb et al., 2018). Therefore, increases in women’s descriptive representation should lead to higher government healthcare budgets across all regimes.
However, we argue that the effects of descriptive representation on healthcare outcomes for women depend on the regime type. Electoral competition in democracies and electoral autocracies (even if the playing field is skewed in the latter) generates incentives for politicians to ensure that funding allocated by the government reaches their constituents. Otherwise, they risk losing the next election (Miller, 2015). By contrast, politicians in closed authoritarian regimes are accountable to a small ruling elite, which reduces the incentives for public goods over more clientelistic exchanges. For these reasons, closed autocracies are generally weaker in implementing social policies than regimes that hold multiparty elections. Further, women politicians are particularly limited in their freedom to change the status quo in closed autocracies where patronage systems tend to be dominated by men, and the women (s)elected to serve in office tend to be dependent on the regime (Bjarnegård et al., 2018; Clayton & Zetterberg, 2020; Nistotskaya & Stensöta, 2018). Combined, these factors lower the incentives and capacity for politicians in closed regimes to implement more complicated reforms required to ensure that social policies reach citizens, especially women, on the ground. As such, even if women are present in positions of power and the formal budget includes more resources for healthcare, we do not expect to find significant improvements in women’s health outcomes in closed autocracies.
We test the implications of our argument using a sample of 169 countries from 2000 to 2018. 1 We first assess whether increasing the number of women in authoritarian legislatures is associated with subsequent higher budgets for healthcare. Afterward, we investigate whether women’s descriptive representation and healthcare spending in autocracies leads to improved maternal mortality, a health outcome for women. In line with previous research (Forman-Rabinovici & Sommer, 2019), we find that women’s descriptive representation is associated with higher spending for healthcare across democracies and autocracies. However, the extent to which descriptive representation correlates with decreases in maternal mortality largely depends upon whether the regime allows electoral competition. In particular, our results show that closed autocracies are significantly worse at promoting women’s health. Increasing the number of women representatives in the legislature appears to have no significant effect on maternal mortality in closed autocracies. By contrast, in democratic regimes, an increased presence of women in the legislature is associated with lower maternal mortality rates. The effect of women’s representation in electoral autocracies is similar to that of democratic regimes across the dependent variables we examine, suggesting that multiparty competition may be the mechanism driving our results.
This article contributes to the literature on women’s representation in authoritarian regimes in several ways. While a growing body of literature examines the reasons why autocrats cater to women’s interests, this research mainly focuses on women’s political, economic, and social rights (Donno et al., 2022; Htun & Weldon, 2012, 2018) or the introduction of gender quotas (Edgell, 2017; Kang & Tripp, 2018; Krook & True, 2012). We know less about how these policies affect the everyday life of women in authoritarian contexts. We show that electoral competition matters for translating inputs like increased government spending on healthcare into concrete outcomes like maternal health. This suggests that even in non-democratic regimes, multiparty elections produce incentives for politicians to ensure that government resources reach their constituents. Our findings have important implications for future research on women in autocracies and policymakers, particularly development practitioners.
Theoretical Framework
Descriptive and Substantive Representation in the Literature
Advocates often argue that women’s access to decision-making is a human right and will lead to policies typically overlooked or ignored by men. This discussion largely centers on descriptive and substantive representation, two concepts introduced by Pitkin (1967). Descriptive representation refers to the representative’s characteristics rather than their actions. It comes from the idea that legislatures should mirror society by including individuals from diverse gender, racial, ethnic, religious, and other politically relevant backgrounds. By contrast, substantive representation refers to the actions, specifically “acting for” a specific group or individual. The expectation that descriptive representation will translate into substantive representation rests on three assumptions: (1) women have policy preferences that are distinct from men; (2) once elected to power, women politicians will stand for women’s interests as a group; and (3) women’s legislative efforts will lead to improved policy outcomes for women in society.
First, it seems reasonable to expect that the marginalization of women has led to the construction of gendered political interests and preferences. In general, the social positioning of women is marginalized when compared to men. 2 In most societies, the public sphere (e.g., politics and economics) remains the preserve of men, while women are the primary caregivers in the private sphere, which includes responsibilities concerning the family and the home (Krook, 2017; Phillips, 1995). Women as a group, therefore, may have developed a different set of interests, which are then reflected in their expressed policy preferences (Beckwith, 2014; Celis & Childs, 2008; Wängnerud, 2000). There is robust empirical support for the argument that women and men develop different policy preferences. The literature typically categorizes these interests in three broad areas: expanding women’s political rights, increasing women’s autonomy related to care-taking obligations of others, and issues that have to do with women’s healthcare and reproductive rights (Beckwith, 2014). Survey evidence shows that women tend to prioritize wealth redistribution, poverty alleviation programs, healthcare, and access to water, while men focus on infrastructure and the economy (Alesina & Giuliano, 2011; Gottlieb et al., 2018; Khan, 2017; Poggione, 2004).
Second, while women may have similar policy interests on average, women politicians need to prioritize policies that serve those interests for the descriptive–substantive representation link to occur. Because of their shared experiences, women politicians may view other women as special constituents whose interests they should represent. For this reason, Phillips (1995) puts forward a theory of the “politics of presence,” arguing that it matters who representatives are, given their considerable autonomy in their everyday decision-making. While descriptive representation is not sufficient for ensuring the implementation of policies women prioritize, evidence suggests that having more women in public office increases the likelihood that policy and budget decisions will better reflect women’s priorities. For example, Mansbridge (2005, p. 622) famously writes that “descriptive representation by gender improves substantive outcomes for women in every polity for which we have a measure.” Thus, the evidence, on average, points to women being successful in acting on behalf of women by producing concrete policy outputs that alter the composition of budgets and content of laws, particularly those that focused on women’s rights (Clayton & Zetterberg, 2018; Ennser-Jedenastik, 2017; Franceschet et al., 2012; Funk & Philips, 2019; Schwindt-Bayer, 2006).
Third, the descriptive–substantive representation link requires that women’s legislative efforts not only translate into changes in policy but also outcomes for women in society. Increased spending on social welfare policies that never make it to women on the ground cannot be considered an example of successful substantive representation. Neither would the adoption of land reforms aimed at formalizing women’s property rights—such as in Kenya, Uganda, and Tanzania—if those reforms fail to address continued discrimination due to customary law, social norms, and legal literacy (Dancer, 2017; Andersson Djurfeldt, 2020). A much less developed strand of the literature focuses on policy outcomes (Reingold, 2008; Wängnerud, 2009). Some prominent examples show that increased representation of women in politics helps to improve outcomes that disproportionately affect women’s welfare, such as the provision of childhood health services in India (Bhalotra & Clots-Figueras, 2014) and improved childcare coverage in Norway (Bratton & Ray, 2002). In a cross-country study of 102 developing countries, Swiss et al., 2012 find that descriptive representation in the legislature is associated with increased infant and child survival.
The Effect of Regime Type on the Link Between Descriptive and Substantive Representation
The descriptive–substantive representation link draws heavily from democratic theory; yet, in recent years, some of the greatest gains in women’s descriptive representation have occurred in autocracies. Does descriptive representation translate into substantive representation in non-democratic settings? Or does it serve some other purpose? Recent studies suggest that the latter is more likely, with autocrats using policies like gender quotas to fast-track women’s descriptive representation for both domestic and international benefits (Bjarnegård & Zetterberg, 2022; Bush, 2011; Bush & Zetterberg, 2021; Donno et al., 2022; Donno & Kreft, 2019; Edgell, 2017; Tripp, 2019). This leaves open the question of whether women can be successful in advancing their priorities in autocratic regimes and whether this varies depending on the type of autocracy. We focus specifically on women’s descriptive representation in autocratic regimes to formulate some empirical expectations about how this may (or may not) contribute to substantive representation.
On the one hand, autocrats may promote gender equality to appeal to international audiences (Bush, 2011; Bush & Zetterberg, 2021; Donno et al., 2022; Edgell, 2017). Many authoritarian regimes are aid-dependent and, therefore, seek to appease international donors by appealing to international norms concerning women’s rights. Advances in gender equality act as a positive signal because the international community has bundled gender equality with both democracy and economic development. Autocrats put on “democratic clothes” in the form of gender quotas and other pro-women policies to boost their legitimacy and obscure authoritarian practices (Tripp, 2019) in a process known as “gender-washing” (Allan, 2019; Bjarnegård & Zetterberg, 2022). For example, Rwanda has received much acclaim for its women-majority parliament, and the United Arab Emirates recently joined the “parity club” by attaining 50% women in its Federal National Council. Yet, the parliaments in both countries have limited real power to implement policies. By promoting women’s access to public office, these regimes claimed credit for reforms widely seen as “progressive, liberal and democratic” despite making little progress in other areas (Bjarnegård & Zetterberg, 2022, p. 62).
On the other hand, the literature shows that authoritarian regimes introduce redistributive policies to demonstrate power and gather support domestically (Atilano Robles, 2020). For example, South Korea established its national healthcare program in 1977 under the dictatorship of President Park Chung-hee, and Cambodian Prime Minister Hun Sen created a social security scheme for civil servants in 2008. Both of these reforms happened immediately before elections as a way for leaders to secure electoral support (Han, 2021). Because women make up roughly half the population, autocrats have incentives to target them with specific policies as a mechanism of cooptation. Research suggests this is most likely in party-based regimes where autocrats attempt to buy women’s loyalty as part of the broader support coalition (Donno & Kreft, 2019). For example, in Uganda, President Yoweri Museveni has used extensive affirmative action policies to establish a strong women “voter bank” and a cadre of loyal elite women within government, both of which help him maintain power through flawed elections (Edgell, 2019; Goetz, 2002; Tamale, 1997).
Furthermore, traditionally strong areas of influence for women, such as healthcare, childcare, and education, tend to pose less risk to autocratic regimes. Given donors’ emphasis on these areas of human development, particularly for women and girls, there are also potentially large payoffs for the regime. Thus, women legislators in autocracies are more likely to produce changes in policy areas that are non-confrontational. For example, Forman-Rabinovici and Sommer (2019) find a positive correlation between women’s legislative representation and substantive representation in non- and partial democracies, specifically when measured with spending for healthcare and education, but also for the adoption of laws allowing abortion.
While it makes sense that autocrats want to signal that they are democratic and want to spend resources on redistributive policies, the literature also argues that authoritarian regimes might be worse at implementing those policies. Autocratic regimes tend to perform poorly in public service provision compared to democracies. And this poor performance can be directly traced to how representation, accountability, and selection work in autocracies (Besley & Kudamatsu, 2006). Thus, even if policies change due to women’s descriptive representation, this may not necessarily lead to tangible results for citizens.
Why Competition Matters
We expect that the descriptive–substantive representation link will hold for some, but not all, autocracies. In particular, multiparty elections should motivate leaders to deliver public goods to their citizens, thus allowing for substantive representation to appear even in autocratic settings. Multiparty elections, even flawed or semi-competitive ones, require a wider support base, encouraging leaders to respond to voter concerns about welfare and redistribution. As suffrage expands, the average income of the median voter falls, and demands for extensive social spending, including healthcare, increase (Acemoglu & Robinson, 2006). In democracies, when leaders fail to deliver policies that serve the majority’s interests, voters will hold them accountable through the ballot box (Gerring et al., 2012; Wang et al., 2019).
In electoral autocracies, leaders face a similar challenge, with the added complication of balancing efforts to maintain legitimacy while using a tilted playing field to minimize the possibility of losing the election (Schedler, 2002). Oftentimes, this means relying on clientelism, such as through vote-buying or patronage, which requires access to resources and local brokers; however, politicians in electoral autocracies also have incentives to deliver public goods. By claiming credit for healthcare, education, and infrastructure projects, electoral autocracies “pursue legitimation through social services” (Cassani, 2017, p. 348). To give an illustrative example, the Tanzanian government allocates more funding to competitive electoral districts, suggesting the ruling party tries to swing these areas through public goods provision (Rosenzweig, 2015). In Russia, elected mayors are more likely to invest in improved housing infrastructure when compared to centrally appointed mayors, suggesting that elections encourage public goods provision a the local level (Beazer & Reuter, 2022).
By contrast, incentives to deliver public goods are lower in closed autocracies where leaders depend on a much smaller group of elite insiders for survival. Because vertical accountability is severely limited, politicians in closed autocracies prioritize particularistic and club goods over public services (De Mesquita et al., 2005). Furthermore, the selection of public officials in closed autocracies is often based on loyalty and personal gain rather than merit. As a result, bureaucratic corruption and incompetence further reduce the efficiency of public services, even if the regime has allocated resources for them (Besley & Kudamatsu, 2006). This explains why, for example, appointed mayors in Russia have allowed Soviet-era public housing infrastructure to become dilapidated and unsafe so long as they can secure electoral victories for the ruling party (Beazer & Reuter, 2022). Several studies support this argument, showing that electoral autocracies invest more in social services like health and education than closed autocracies (Cassani, 2017; Fails, 2020), and perhaps on similar levels to democracies (Miller, 2015). This translates into better development outcomes, including lower infant mortality, higher literacy, and gender balance in schooling for electoral autocracies compared to closed regimes (Miller, 2015). 3
What does this mean for theories about women’s descriptive and substantive representation in authoritarian regimes? As discussed above, a core assumption underlying the descriptive–substantive representation link is that women politicians have a special relationship with women voters through their shared experiences, encouraging them to advance policies addressing women’s interests (Phillips, 1995). This is especially true where women voters can exert more pressure on women politicians (Mechkova & Carlitz, 2021) and where women’s organizations can effectively influence policy-making (Htun & Weldon, 2012; Kang & Tripp, 2018). Thus, in electoral autocracies, we might expect to find a similar link between descriptive and substantive representation because women politicians will have stronger incentives to redistribute benefits to women constituents through social services.
In closed autocracies, however, politicians answer to a small elite, which might not depend on a well-functioning public system. Thus, in these regimes, the expansion of the social system might not be a specific “women’s interest” in the eyes of the constituents to which women politicians will be held accountable. Furthermore, in closed autocracies, politicians face greater informational constraints due to the lack of multiparty elections, limitations on civil society, and media restrictions. This makes it more difficult for citizens to communicate their preferences to legislators (Dahlum et al., 2022). In practice, this means that politicians in closed autocracies have limited knowledge about the specific needs of their constituents and fewer incentives or opportunities to act upon them.
While closed autocracies are generally weaker in terms of implementing social policy (Gerring et al., 2022), we argue that the success of policy implementation has important gendered dimensions. Research suggests that women politicians are less effective in more corrupt settings because clientelistic networks tend to be dominated by men and because women bring fewer financial resources and have smaller support networks (Bjarnegård et al., 2018; Clayton & Zetterberg, 2020; Nistotskaya & Stensöta, 2018). This makes women politicians more vulnerable and dependent on the ruling party in closed autocracies where loyalty and patronage are the main drivers for access to public office (Arriola & Johnson, 2014). Under these conditions, women politicians tend to be tightly associated with the regime (Bjarnegård et al., 2018; Nistotskaya & Stensöta, 2018). As a result, in closed autocracies, the ability of women parliamentarians to implement substantive changes in line with their priorities is more limited due to extensive corruption and patronage (Mechkova et al., 2022).
Morocco acts as an illustrative example. It is a closed regime where recruitment to party positions is highly centralized and based on patrimonial linkages (Sater, 2007). The introduction of a gender quota in 2002 did not result in substantive changes for women citizens as those who top the party lists for women tend to be wives or close relatives to party leaders (parachutées as activists call them). Thus, they have strong family and ethnic links to patrons rather than constituents. Due to limited financial resources and strong gender biases, women political aspirants are rarely successful without the support of established political parties.
Empirical Implications for Healthcare Spending and Maternal Mortality Rates
Because previous research shows that women tend to prioritize healthcare more than men, we focus on healthcare spending and maternal mortality as indicators of women’s substantive representation. We argue that substantive representation requires not just policy change in the form of greater healthcare spending but also requires that resources translate into healthcare outcomes for women in society, namely, through decreased maternal mortality rates. 4 We focus on maternal mortality because it is a health outcome that directly affects the female sex and only indirectly affects men through, for example, partner loss. 5 These outcomes also act as a “most likely” case for seeing a link between women’s descriptive and substantive representation in autocracies because health is a policy area that poses little risk to the regime (Forman-Rabinovici & Sommer, 2019). Therefore, our decision to focus on health provides a robust test of the scope conditions. If our theory fails to hold in this particular policy area, it will raise serious concerns about its validity in other policy areas as well.
What are the successful strategies to reduce maternal mortality, and can we reasonably expect that women’s descriptive representation in the legislature helps to reduce these numbers? Thanks to advancements in medicine and concentrated political efforts to address the issue, global rates in maternal mortality have declined substantially in recent decades with a decrease of 44% from 1990 until 2013 (Callister & Edwards, 2017). However, maternal deaths are still high, as eight hundred women die from pregnancy-related reasons worldwide every day (one woman every 2 seconds). Importantly, most of these deaths are preventable with simple interventions. Countries that managed to cut maternal deaths significantly did so by increasing public awareness of the magnitude of the problem. This includes mobilization and education of professionals and communities about maternal health and well-being (De Brouwere et al., 1998). Even in developing countries, where poverty and poor access to healthcare services pose substantial barriers to maternal health, interventions designed to improve knowledge for professionals and communities have successfully reduced maternal death rates (Callister & Edwards, 2017).
This suggests that the greatest barriers to maternal health—knowledge and behavior change—can be addressed relatively quickly through policy interventions (De Brouwere et al., 1998). However, increased spending and policy prescriptions are not always enough. For example, a recent review of Uganda’s maternal health policy from 2000 to 2015 questioned whether the interventions were “designed to fail” given their piecemeal approach and lack of attention to shortcomings in healthcare facilities and medical personnel (Mukuru et al., 2022). This suggests that spending and policy are insufficient for realizing outcomes on the ground absent political will to improve capacity through a comprehensive approach.
We anticipate that the regime type, particularly the degree to which it allows for electoral competition, influences the likelihood that women’s descriptive representation translates into reduced maternal mortality rates. In short, we expect that as part of the cooptation and signaling game, women politicians might be able to make gains in some visible and easy-to-achieve policies that address women’s interests (relative to men’s), such as allocating greater resources for healthcare. However, the extent to which those resources reach citizens on the ground varies depending on the regime. Compared to regimes with some electoral competition, closed autocracies will have weaker incentives and capacity to deliver redistributive public goods like healthcare. This has implications for the link between descriptive and substantive representation. Even if the “playing field” is skewed in electoral autocracies (Schedler, 2002), some competition exists, which could encourage women politicians to represent women’s interests in similar ways to democracies. By contrast, closed autocracies have the weakest incentives and capability to implement comprehensive redistributive policies that reach citizens on the ground. The generally weaker position of women politicians in closed autocracies, where a small elite built upon corruption and patronage networks dominates decision-making, means that resources for healthcare will not translate into improved health outcomes for women in society.
Based on the theoretical discussion we developed so far, we formulate the following hypotheses:
Women’s descriptive representation will be positively associated with government spending on healthcare regardless of regime type.
Women’s descriptive representation will be positively associated with healthcare outcomes for women in electoral autocracies and democracies, but not in closed autocracies.
Data and Empirical Approach
We take a two-step approach to assess whether women’s descriptive representation in authoritarian legislatures translates into substantive improvements in women’s health outcomes. First, we test whether regimes with a higher percentage of women in the national legislature (single or lower chamber) spend more on healthcare. Afterward, we investigate whether women’s descriptive representation also affects maternal mortality risk, an indicator of women’s health, while controlling for health expenditures.
To ensure maximum comparability across our models, we use a standard set of controls and estimation strategy. Summary statistics for all variables used in the main models are reported in Table A1. Because we cannot control for all country-specific variation, we include country-fixed effects and robust country-clustered standard errors. As such, our main results focus on within-country effects rather than between-country comparisons. To mitigate potential reverse causality and endogeneity, we lag all independent variables based on a reasonable lag structure and present several alternatives as robustness checks. We also provide alternative model specifications in the appendix, including two-way country-year fixed effects and Prais–Winsten models with panel-corrected standard errors. Given the observational nature of our data, these attempts may not mitigate all confounding or potential for endogeneity; therefore, we interpret our results as associations rather than strictly causal effects.
Dependent Variables
Health Expenditures
We measure health spending based on government health expenditures as a percentage of gross domestic product (GDP). The World Health Organization (WHO) collects this data based on official reports from its member states (WHO, 2022). We use the version from the Quality of Government dataset (Teorell et al., 2022), as reported in the World Bank World Development Indicators (World Bank, 2022b). Between 2000 and 2018, government health expenditures ranged from .06% (D.R. Congo in 2000) to 11.57% (Cuba in 2015) of GDP, with a mean of around 3.11% (similar to Russia in 2015). For the health expenditure models, we apply one year lag, as this is a fast-changing variable (see Figure A3 in the online appendix). On average, countries saw an increase of .03 per year in their government spending on health as a percentage of GDP with a range of −6.5 to 5.9. The average absolute value of these annual changes is .25, which is quite large, considering that the overall mean is 3.11. Therefore, it is reasonable to assume that changes in women’s representation will affect government spending fairly quickly. Adopting a one-year lag also helps us avoid conflating the effects of one legislative term on the outcomes of another while ensuring that changes in women’s representation preceded changes in government spending. We find similar results with a two-year lag, as reported in Table A14 and Figure A23 of the online appendix.
Because expenditure data are official government statistics, they have several limitations. First, temporal coverage is limited to the 21st century. While the WHO produced data before this period (see Clayton & Zetterberg, 2018), they introduced a new classification system in 2011 that improves comparability across countries (WHO, 2011). As a result, data on government health expenditures collected under the older definition are incompatible with the newer series. They are no longer included in the World Bank development indicators (World Bank, 2022b). Second, official government statistics are prone to errors or strategic manipulation. States with less capacity may fail to provide data or report inaccurate statistics. More importantly, autocratic regimes may over (under) report certain statistics to benefit the state’s reputation (Carlitz & McLellan, 2021; Magee & Doces, 2015; Sandefur & Glassman, 2015). Thus, we cautiously interpret our results in light of these limitations, given that these are the best available data. In the online appendix, we also report results using an alternative measure of government healthcare expenditures provided by the Institute for Health Metrics and Evaluation (IHME, Chang et al., 2019), which covers the period 1995 to 2019. 6 The IHME estimates of government health expenditures are moderately correlated with the WHO estimates, with a Pearson’s coefficient of .54.
Maternal Mortality
To measure maternal mortality, we use lifetime risk of maternal death (LRMD). This indicator assesses the probability (as a percentage) that a 15-year-old girl living in the country will die within their lifetime from a maternal cause, keeping constant present levels of fertility and general mortality. These data come from the Trends in Maternal Mortality: 2000 to 2017, produced by the WHO, UNICEF, UNFPA, World Bank, and the United Nations Population Division (WHO, 2019). We take these data from the most recent QoG dataset (Teorell et al., 2022), but they are also available through the World Development Indicators (World Bank, 2022b).
As with health spending, data on LRMD only cover 2000 to 2017 because the WHO has updated its estimation strategies to improve the data reliability and comparability, making the older series incompatible with newer estimates. 7 To deal with the short time series for the official WHO data, we report alternative results in the online appendix using estimates of LRMD from 1990 to 2019 from the Global Maternal Health Model (GMHM, Ward et al., 2023). The WHO and GMHM data are highly correlated, with a Pearson’s correlation coefficient of .93.
Working with data on maternal mortality presents several other challenges. Thanks to advancements in medicine and concentrated efforts to address the issue, global rates in maternal mortality have declined substantively, particularly in the last few decades (Callister & Edwards, 2017). By 2000, most countries had achieved a very low probability of the mother dying during childbirth, even in developing countries. As a result, the LRMD is heavily right-skewed (see Figure A4). It ranges from .002 (Italy in 2017) to 10.96% (Sierra Leone in 2003), but the average value is .95% (similar to Bangladesh in 2006). Indeed, 73% of our sample has less than one percent LRMD. In line with the literature, we take the natural log of LRMD to deal with this extreme skew in the data, as illustrated in Figure A4 and Figure A6.
Yet, important variation in LRMD across countries persists, with most deaths happening in developing countries (Kassebaum et al., 2014). In particular, sub-Saharan Africa’s average LRMD—2.82%—is disproportionately higher than in other regions. At the extreme, it was more than ten percent in Sierra Leone and Chad in the early 2000s. This contrasts with Western Europe and North America where LRMD is .03% or less throughout our sample time period (see Figure A5 in the online appendix). For our purposes, this matters most because it suggests that there may be important differences in maternal mortality by regime type. As shown in Figure A6, liberal democracies generally tend to have lower LRMD, with little variation among these regimes.
Our concerns about reporting bias for health expenditures also carry over to our measure of maternal mortality, namely, under-reporting due to state capacity or reputation concerns. The World Bank cautions, “Maternal mortality ratios are generally of unknown reliability, as are many other cause-specific mortality indicators. The probability cannot be assumed to provide an exact estimate of risk of maternal death (World Bank, 2022a).” Therefore, we are cautious in our interpretation of the results. Predictions from our models should be taken as illustrative in relative rather than absolute terms for comparative purposes only.
Given that it takes time to design and implement policies that will reduce mortality, we assume that increases in women’s descriptive representation should have an observable effect on maternal mortality within five years. In our benchmark models, we use five-year lags of LRMD, but in the online appendix, we find similar results with alternative lag structures (Table A10 and Figure A18). 8
As a robustness test, we use data on the maternal mortality ratio provided by the World Bank (World Bank, 2022b). This ratio captures the number of women who die from pregnancy-related causes while pregnant or within 42 days of pregnancy termination per 100,000 live births. Finally, we also replicate our main models with life expectancy for women as the dependent variable (also see Westfall & Chantiles, 2016), which is taken from the World Bank data (World Bank, 2022b). This variable is broader in nature compared to our main variable of choice, which focuses only on maternal deaths. Thus, with this robustness check, we test whether government policies are able to increase the lifespan of all women on average.
Independent Variables
Our key independent variables of interest are women’s descriptive representation and regime type. We measure descriptive representation as the percentage of women in the single or lower chamber of the national legislature from the latest version of the Varieties of Democracy (V-Dem) dataset (Coppedge et al., 2022). For the time period under investigation, these data primarily come from the Inter-Parliamentary Union (IPU, 2022). During our observation period, women’s representation averaged 17.46% (similar to Tajikistan 2005–2009), with a range of zero (e.g., Vanuatu and Yemen in 2017) to 63.75% (Rwanda 2013–2015).
For regime type, we use the Regimes of the World measure (Lührmann et al., 2018) from the V-Dem dataset (Coppedge et al., 2022). This variable takes a four-fold typology of regimes based on Schedler (2002). Closed autocracies (e.g., Saudi Arabia) do not hold elections at all or fail to achieve minimal competition in elections. Electoral autocracies (e.g., Belarus) allow some electoral competition for the executive and legislature, but there are significant electoral irregularities and repression of civil liberties. Democracies are all regimes that guarantee a certain level of fairness when holding elections. Electoral democracies (e.g., Paraguay) differ from liberal democracies (e.g., Sweden) to the extent that they provide protections of civil liberties and the rule of law. Thus, the Regimes of the World allows us to distinguish between democracies and autocracies, as well as between closed autocracies and electoral autocracies.
We estimate models with a simple dichotomous variable for autocracy/democracy and then differentiate closed from electoral autocracies with all democracies as the reference category. In the online appendix (Table A13), we also report results differentiating liberal and electoral democracies. Generally, we see no differences in the results by type of democracy (also see Figures A21 and A22). To assess differences in the effects of women’s representation across regime types, we interact regime type with the share of women in the legislature.
Controls
Because of our short time series, we are judicious with control variables and use country-fixed effects to control for time-invariant confounders. All of our controls come from the the V-Dem dataset (Coppedge et al., 2022).
First, we control for gender quotas and women executives. Gender quotas have become increasingly common, especially after the mid-1990s, as a way to “fast-track” women’s legislative representation. Prior research suggests that gender quotas are associated with increased health spending and improved health outcomes for women (Chen, 2010; Clayton & Zetterberg, 2018; Westfall & Chantiles, 2016). By contrast, we expect quotas will not have an independent effect on our outcomes of interest and only benefit spending and health outcomes through higher women’s representation. Nevertheless, because autocracies may jointly adopt quotas and other policies benefiting women for strategic reasons (Bjarnegård & Zetterberg, 2022; Donno et al., 2022; Donno & Kreft, 2019; Edgell, 2019; Tripp, 2019), we include quotas as a control. This variable was originally coded in the QAROT dataset and has been updated by V-Dem (Coppedge et al., 2022; Hughes et al., 2019). About 26% of the country-years in our sample had a legal gender quota policy. While our primary interest here is in women’s representation in legislatures, we also control for whether the head of state or head of government was a woman, anticipating that women executives may have an independent influence on health spending priorities and outcomes. This measure is coded by V-Dem using a variety of sources (Coppedge et al., 2022). Only about 10% of the country-years in the sample have a woman executive.
We include several development and demographic controls as well. Wealthier countries are likely to have more health spending and better maternal health outcomes all else equal. Therefore, we include a measure of GDP per capita (Fariss et al., 2022), which ranges from .55 (D.R. Congo in 2003) to 100.86 (Qatar in 2012), with an average value of 15.25 (similar to Turkey in 2006). Larger countries may face greater challenges that require more health spending and, perhaps, experience higher maternal mortality. Therefore, we also control for logged population (Fariss et al., 2022). In its level form, this variable ranges from 87,560 (Seychelles in 2000) to 1.47 billion (China in 2017), with an average of 43.2 million (similar to Tanzania in 2007). Further, we control for the overall equality within the health system using a measure coded by the V-Dem country experts (Sigman & Lindberg, 2015). This measure captures the degree to which there is equality in access to basic high-quality healthcare. It ranges from −2.28 (Sudan 2013–2015) to 3.31 (France 2001–2015), with an average of .67 (similar to Rwanda 2001–2004). We also control for the level of corruption in a country as previous research shows that corruption affects both the extent to which women are elected in a country (Sundström & Wängnerud, 2016), and success in improving human development in general (Holmberg et al., 2009). However, because research connects the election of women with reduced levels of corruption (Bauhr & Charron, 2021; Bauhr et al., 2019; Swamy et al., 2001), this variable may introduce issues with post-treatment bias. Therefore, we only include corruption as a control variable in the robustness checks.
Results
Government Health Expenditures (%GDP).
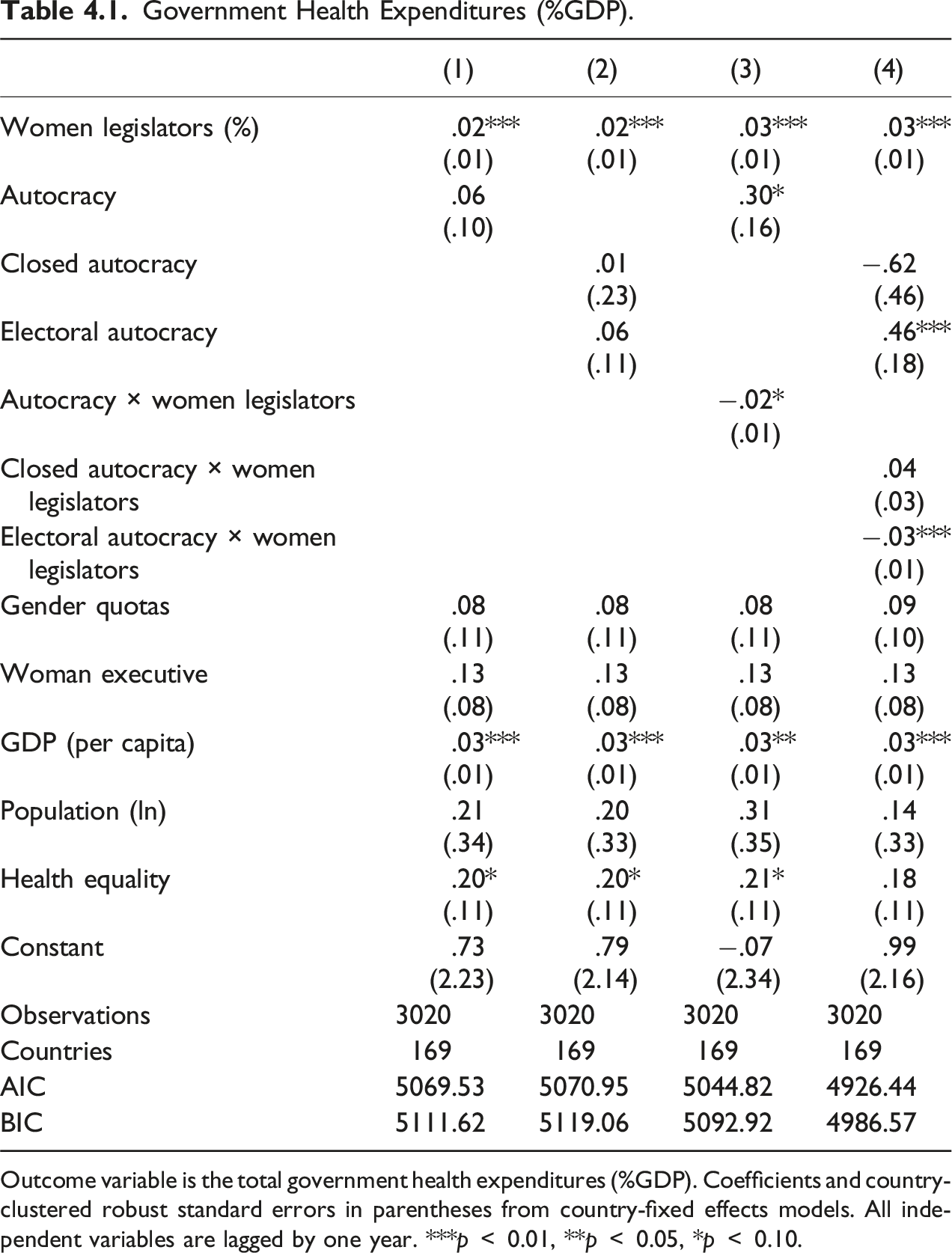
Outcome variable is the total government health expenditures (%GDP). Coefficients and country-clustered robust standard errors in parentheses from country-fixed effects models. All independent variables are lagged by one year. ***p
In Model 4, we assess the extent to which political competition affects the observed relationship between women’s representation and government spending on healthcare in autocracies. Figure 4.1 illustrates these interactive effects. As shown in panel (a), a one percentage point increase in women’s descriptive representation is associated with a substantial increase in government health spending in closed autocracies. On average, the estimated effect in closed autocracies is not significantly different from democracies. As shown in panel (b), government spending on healthcare in closed autocracies and democracies is not significantly different across a range of reasonable values for women’s descriptive representation. Thus, contrary to expectations, the results suggest that women lawmakers in closed autocracies are able to influence government healthcare spending similarly to democracies. Marginal effects of women’s representation on health spending by regime type. Based on estimates from Model 4 in Table 4.1. (a) Average marginal effects of women’s descriptive representation on government health spending (%GDP) and (b) estimated difference in government health spending (%GDP) versus democracies.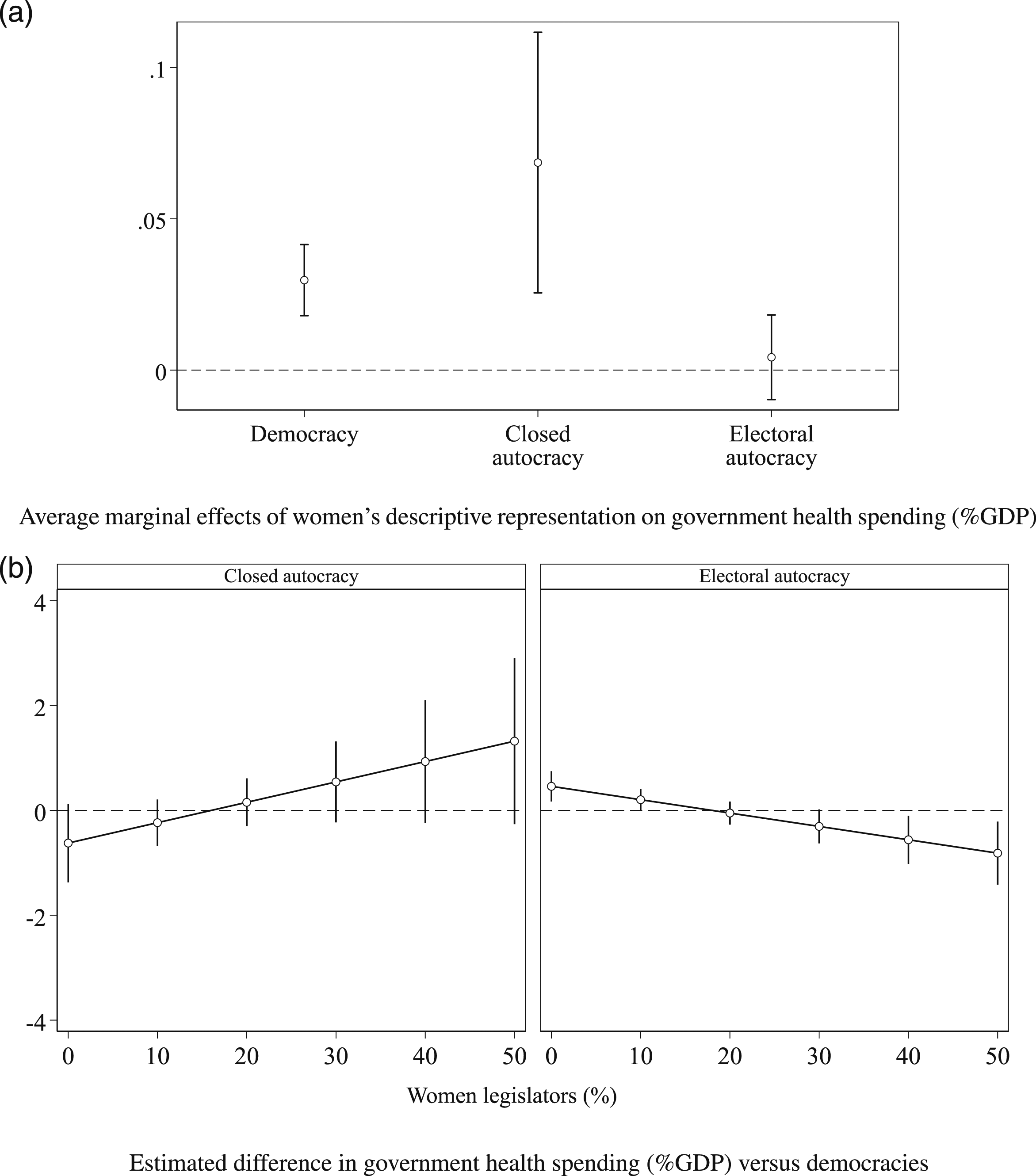
For electoral autocracies, however, the average marginal effect is smaller and the 90% confidence interval crosses zero. As shown in Figure 4.1 panel (b), electoral autocracies appear to spend more on healthcare than democracies when women’s representation is low (10% or less). Nevertheless, once women lawmakers achieve about 30%, democracies spend significantly more on healthcare than electoral autocracies. Thus, contrary to expectations, the results suggest that women lawmakers in electoral autocracies have less influence on government healthcare spending than in democracies and closed autocracies.
Lifetime Risk of Maternal Death (%, Logged).
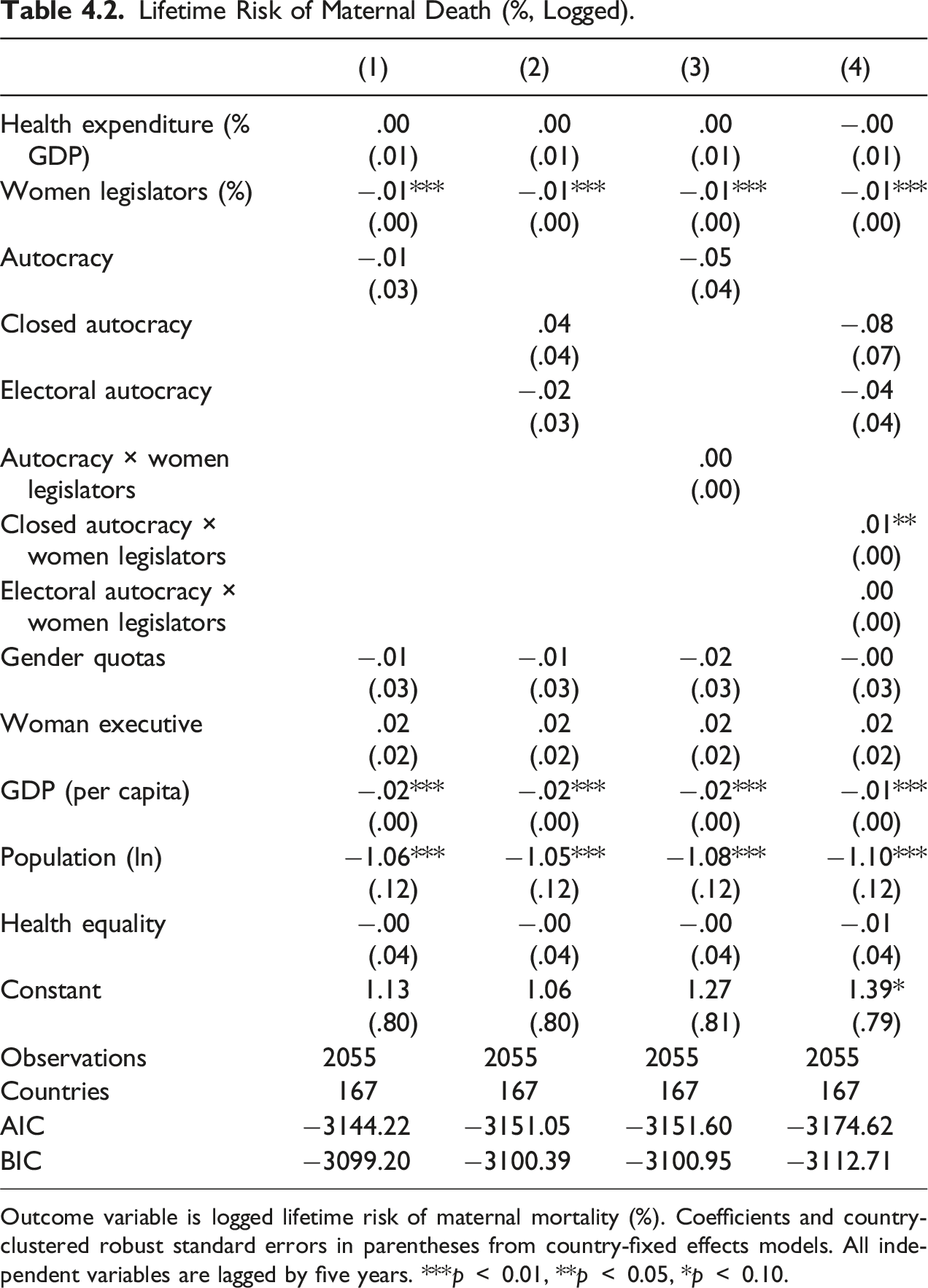
Outcome variable is logged lifetime risk of maternal mortality (%). Coefficients and country-clustered robust standard errors in parentheses from country-fixed effects models. All independent variables are lagged by five years. ***p
However, when we account for political competition in Model 4, we find that the interaction term for closed autocracy is statistically significant and positive. To illustrate this relationship, panel (a) of Figure 4.2 shows average marginal effects for democracies, closed autocracies, and electoral autocracies.
9
The 90% confidence interval for closed autocracies crosses zero, suggesting that women’s descriptive representation is not significantly associated with logged LRMD in these regimes. By contrast, we find similar marginal effects for democracies and electoral autocracies. Marginal effects of women’s representation on LRMD (%, logged). Based on estimates from Model 4 in Table 4.2. (a) Average marginal effects of women’s descriptive representation on LRMD (%, logged) and (b) estimated difference in LRMD (%, logged) versus democracies.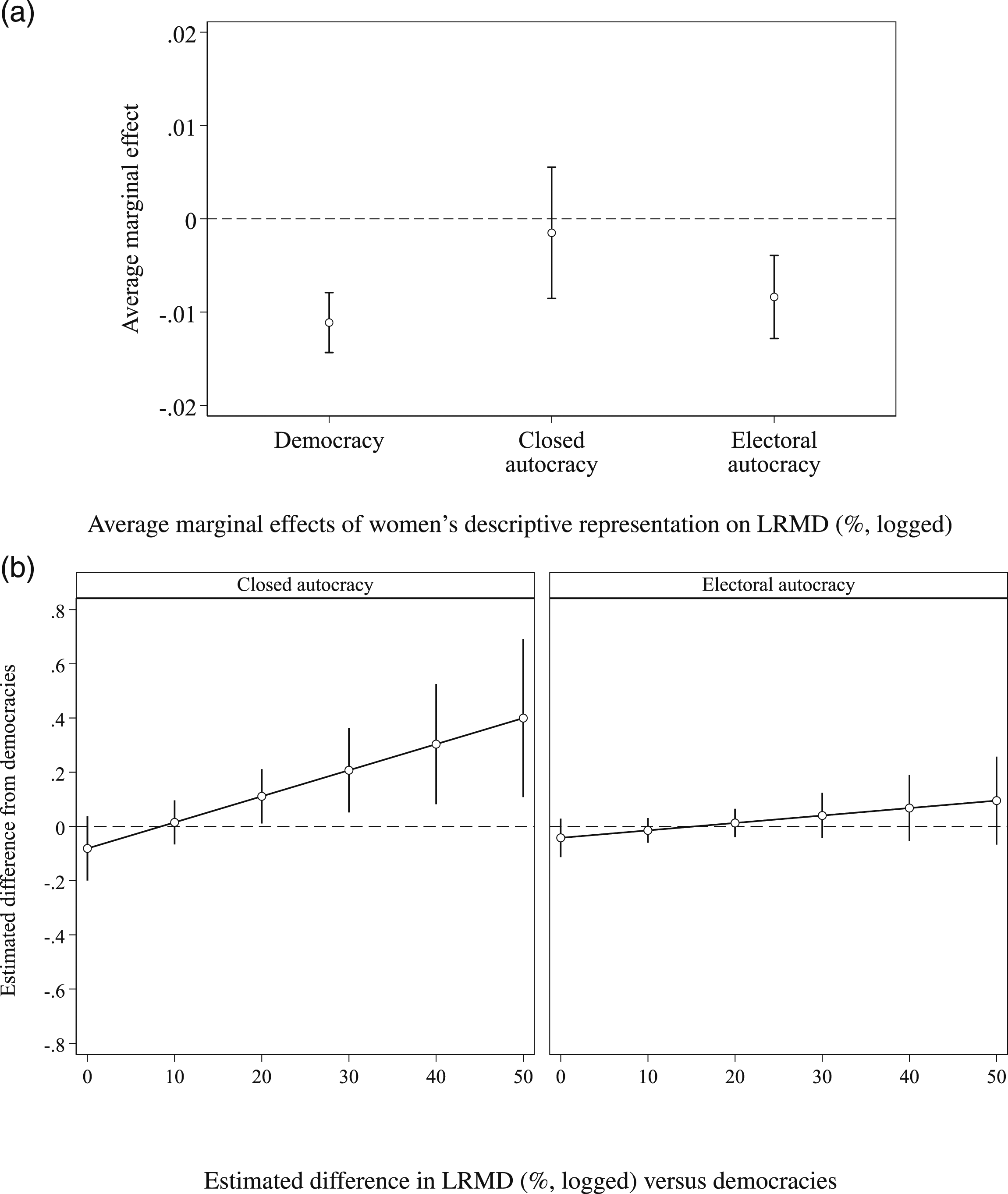
In panel (b) of Figure A9, we illustrate the estimated difference in logged LRMD for closed and electoral autocracies, compared to democratic regimes. We find that logged LRMD is significantly higher for closed autocracies than democracies as women achieve 20% or more of the seats in the legislature. In other words, once countries reach a critical mass of women’s representation, democracies outperform closed autocracies on maternal health outcomes. By contrast, the right-hand side of the panel shows that logged LRMD in electoral autocracies is not significantly different from democracies as women’s representation increases from zero to 50%.
In short, the findings in Tables 4.1 and 4.2 provide support for our theory that multiparty competition provides incentives and opportunities for women lawmakers in autocracies to engage in substantive representation as their numbers increase. While women in closed autocracies appear to be able to influence the spending priorities of the regime, we find little evidence that this translates into substantive health outcomes for women. By contrast, we find that women lawmakers in electoral autocracies may have less influence over the health budget, but they nevertheless are associated with improved substantive health outcomes for women, like maternal mortality.
Robustness checks
Recognizing that our results are limited due to the observational nature of the data as well as the time frame and country coverage, we engage in several robustness checks reported here and in the online appendix. We summarize the key results of these robustness tests in Figure 5.1. Summary of main findings from robustness checks. Full results are available in the online appendix. (a) Government healthcare spending and (b) maternal health outcomes.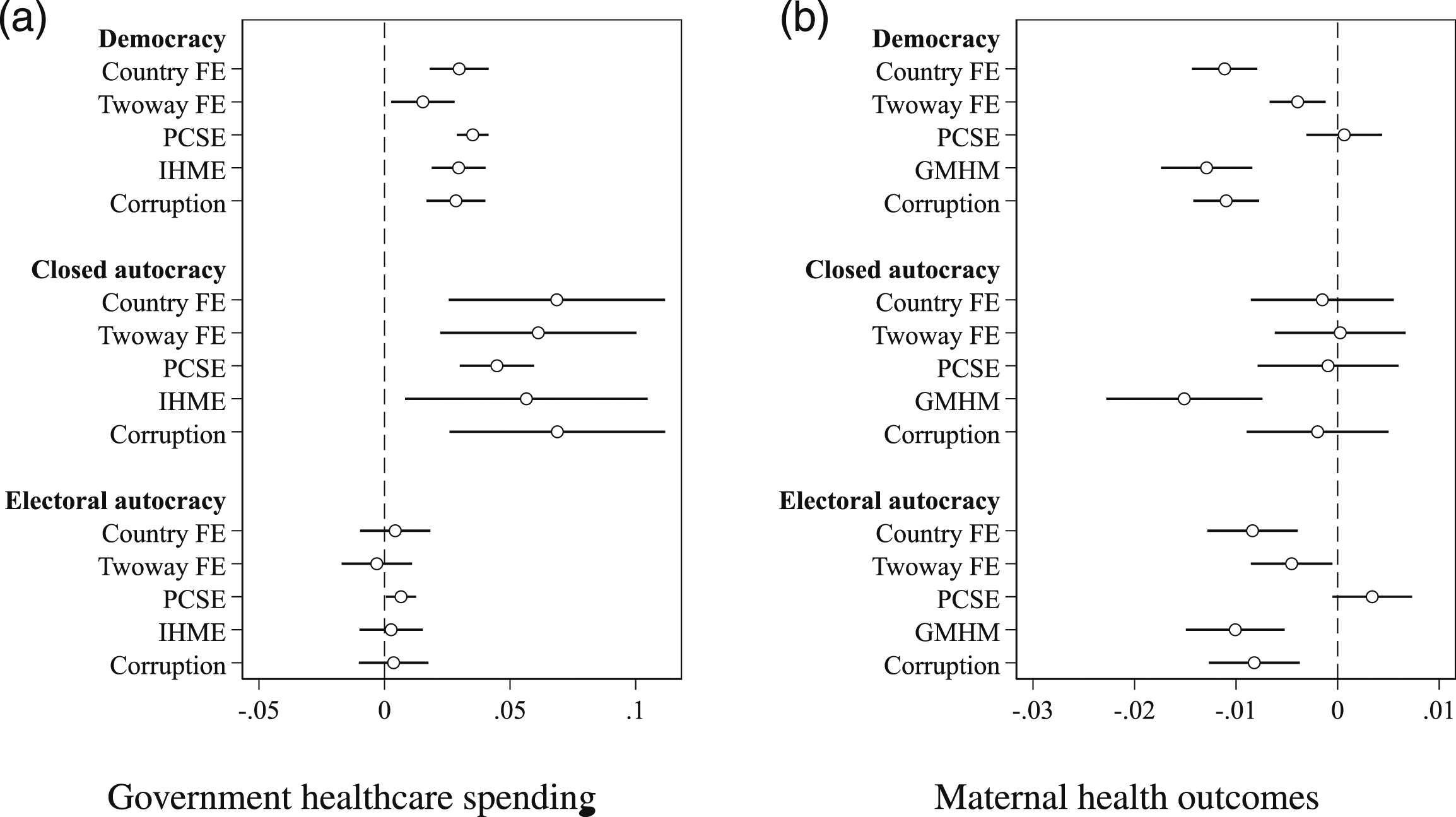
We compare our results using country-fixed effects to two alternative estimation strategies. Generally, the findings are similar when using two-way country and year fixed effects (two-way FE); although, the magnitude of the coefficients decreases for both government health spending and logged LRMD (see Tables A2 and A3 in the appendix). We also ran Prais–Winsten regression models with panel-corrected standard errors for an AR(1) process (PCSE). These results differ from the fixed effects approach, which we attribute to the fact that the PCSE model estimates between- rather than within-country effects. Between countries, we find that the relationship between women’s representation and government healthcare spending is similar (Table A4); however, we do not find evidence of a significant association for logged LRMD regardless of regime type when using a PSCE model (Table A5). We are cautious about these between-country results given the data limitations and our inability to control for many possible confounders.
As discussed above, the official data offer a limited time series because of changes in how the WHO calculates government healthcare spending and maternal mortality statistics. To account for this, we run additional models using new simulated data estimating government health spending from IHME (Chang et al., 2019) and maternal mortality from GMHM (Ward et al., 2023). These data allow us to extend the time series to 1995 and 1990, respectively. Regarding government health spending, we find similar patterns using the IHME data (Table A6). By contrast, the GMHM data suggest that women’s representation has a significant negative association with logged LRMD across all regimes (Table A7). This divergent finding for closed autocracies, in particular, appears to be driven by differences in how GMHM calculates LRMD. 10
Finally, Figure 5.1 reports results when we introduce corruption as an additional control variable (see Tables A8 and A9). Evidence suggests that corruption may undermine public spending and the efficacy of public services. In addition, corruption may limit the ability of women to engage effectively in policy adoption and implementation processes because typically women have fewer resources and connections to clientelistic networks (Bjarnegård et al., 2018; Clayton & Zetterberg, 2020; Nistotskaya & Stensöta, 2018). We use the V-Dem political corruption index, which captures six distinct forms of corruption in the public sector, executive, judiciary, and legislature (Coppedge et al., 2022). According to our estimates, however, corruption is not significantly associated with health spending nor with logged LRMD. Our main results concerning the descriptive–substantive representation link in autocracies also hold when this control is included.
In addition to the robustness checks summarized in Figure 5.1, our online appendix reports the results for three other alternative specifications of maternal health outcomes. First, we estimated models with logged LRMD lagged by one year, rather than the five years reported in our main models (Table A10). Second, we replicate our findings using the logged maternal mortality ratio, which captures the number of women who die from pregnancy-related causes while pregnant or within 42 days of pregnancy termination per 100,000 live births (Table A11). Third, we run the analysis with female life expectancy as the outcome, which allows us to test whether government policies are able to increase the lifespan of all women on average not just mothers (Table A12). In general, our main findings hold across these alternative specifications. We find that electoral autocracies and democracies consistently see improvements in women’s health as women’s descriptive representation increases, while closed autocracies show little evidence of the descriptive–substantive representation link for women’s health.
Conclusion
While activists and policymakers alike often argue that having more women in public office is important to ensure that women’s policy preferences are adequately addressed through public goods and spending, the link between descriptive and substantive representation remains tenuous. This is particularly true for non-democracies, where legislatures (and the policies they produce) may be used as a tool of cooptation to support existing patriarchal elite structures rather than a genuine vehicle for representation.
In this article, we examine whether women’s descriptive representation is associated with public health spending and women’s health outcomes. In particular, we focus on government expenditures and the lifetime risk of maternal death. In general, we find that women’s descriptive representation is positively associated with health spending and health outcomes for women. However, we also find evidence that electoral competition matters for establishing a link between descriptive and substantive representation for women. In electoral autocracies, women’s descriptive representation is associated with improved maternal health outcomes, similar to those observed in democracies. We expect that competition in electoral autocracies (even if it is restricted) creates incentives to improve public goods delivery and also permits women lawmakers to influence policy adoption and implementation, particularly around elections. By contrast, due to the small selectorate in closed autocracies, we argue that there are minimal incentives and opportunities to actually implement policies that improve the lives of women. This explains why we only see increases in health budgets and not health outcomes as women take up more legislative seats in closed autocracies. The simultaneous increase in women lawmakers and health budgets may reflect “signaling” or “autocratic gender-washing” rather than genuine investments by the regime in political and health equality (Allan, 2019; Bjarnegård & Zetterberg, 2022).
Our findings speak directly to the growing literature on representation in autocratic regimes (Allan, 2019; Bjarnegård & Zetterberg, 2022; Donno et al., 2022; Edgell, 2019; Forman-Rabinovici & Sommer, 2019; Tripp, 2019). We contribute to the ongoing discussion on autocratic politics by studying the effects of increasing the number of women in politics directly on the quality of life for women. The implications of our findings are that while women in parliaments have the potential to promote policies that address the specific interests of women, the conditions under which this happens matter. At least part of this variation can be explained by electoral competition. Future research could help to better illuminate the causal processes and mechanisms behind substantive representation in autocracies.
Finally, we have chosen health outcomes as most likely case to investigate the link between descriptive and substantive representation in authoritarian regimes. Repeated studies show that women tend to place a higher premium on healthcare spending than men. In addition, health represents a policy area where autocracies can engage in redistribution with minimal risk and high possible rewards for the regime. Because our models are supportive of the main argument, we have greater confidence in our theory. However, whether we could reasonably expect our findings to travel to other policy areas women prioritize largely depends on the degree to which those policies threaten the regime. Regardless, we anticipate that in closed autocracies tangible change for citizens will be hardest to achieve due to the limited nature of accountability. A promising avenue for future research would be to investigate other policy areas of greater priority for women such as access to water and education for girls to assess whether our findings also travel to these outcomes.
Supplemental Material
Supplemental Material - Substantive Representation, Women’s Health, and Regime Type
Supplemental Material for Substantive Representation, Women’s Health, and Regime Type by Valeriya Mechkova, and Amanda B. Edgell in Comparative Political Studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by the Swedish Research Council, Consolidator Grant with Principal Investigator Johannes Lindvall (2016– 00783).
Data Availability Statement
Data and replication materials for this article can be found at Mechkova and Edgell (2023). ![]() .
.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.