
Abstract
This study aims to compare the clinical characteristics of children with general Mycoplasma pneumoniae pneumonia (GMPP) and refractory Mycoplasma pneumoniae pneumonia (RMPP), identify predictive factors for RMPP, and construct a predictive nomogram for early clinical prediction of RMPP. This retrospective study included 223 children with Mycoplasma pneumoniae pneumonia admitted to Lishui District People’s Hospital in Nanjing from June 2023 to February 2024. Children were divided into GMPP (171 cases) and RMPP (52 cases) based on treatment response. Baseline characteristics, laboratory findings, and imaging results were compared between groups. Multivariate logistic regression and receiver operating characteristic curve analysis were used to identify and evaluate predictive factors for RMPP. The RMPP group had higher incidence of dyspnea, lung consolidation, atelectasis, and pleural effusion, and longer hospital stays. Laboratory tests showed elevated C-reactive protein, interleukin-6 (IL-6), D-dimer, and lactate dehydrogenase (LDH) levels in RMPP compared with GMPP. Multivariate analysis identified LDH, IL-6, and D-dimer as significant predictive factors for RMPP. The combined model’s area under the curve was 0.946, indicating high prediction efficacy. Elevated levels of LDH, IL-6, and D-dimer are associated with RMPP. The predictive nomogram based on these markers improves RMPP risk assessment, providing a scientific basis for early recognition and personalized treatment.
Introduction
Mycoplasma pneumoniae (MP), known as an “atypical pathogen,” is one of the most common pathogens causing respiratory infections in children. 1 Unlike conventional bacteria, MP lacks a cell wall and therefore does not possess peptidoglycan, rendering it intrinsically resistant to β-lactam antibiotics—a defining structural feature that classifies it as an “atypical” pathogen. 2 Mycoplasma pneumoniae attaches to host respiratory epithelial cells via its specialized tip organelle, using adhesin proteins (primarily P1 and P30) to bind sialic acid receptors on ciliated cells, thereby initiating infection and impairing mucociliary clearance. 3 To evade host immunity, MP employs several strategies: intracellular survival, secretion of the community-acquired respiratory distress syndrome (CARDS) toxin and hydrogen peroxide that suppress ciliary function and induce epithelial injury, and molecular mimicry—whereby surface antigens resemble host tissue antigens, potentially triggering autoimmune responses that contribute to extrapulmonary complications. 4 Although asymptomatic carriers have been reported, 5 10% to 40% of children with MP respiratory tract infections eventually develop Mycoplasma pneumoniae pneumonia (MPP). 6 The majority of MPP patients improve rapidly with macrolide antibiotics, but some patients develop refractory Mycoplasma pneumoniae pneumonia (RMPP). 7 Currently, there is no universally accepted definition of RMPP. According to the latest Chinese guidelines for the diagnosis and treatment of MPP, 8 RMPP is defined as a severe type of MPP in which symptoms persist despite 7 days of standard macrolide treatment, characterized by continued fever, worsening lung imaging, or extrapulmonary complications. 9
In recent years, the incidence of RMPP has increased, often leading to longer fever duration, more complicated treatment processes, and higher medical costs. Beyond pulmonary manifestations, RMPP may involve multiple organ systems, giving rise to a spectrum of extrapulmonary complications. Neurological involvement includes encephalitis and aseptic meningitis; cardiovascular manifestations encompass myocarditis, pericarditis, and arrhythmias; dermatological findings range from erythema multiforme to Stevens-Johnson syndrome; and hematological complications such as hemolytic anemia and thrombocytopenia have also been reported. 10 On imaging, RMPP characteristically demonstrates large lobar or segmental consolidation, necrotizing pneumonia, bronchiolitis obliterans, pleural effusion, and—less commonly—pulmonary embolism. 11 Therefore, early and accurate diagnosis of RMPP is critical for formulating effective treatment strategies. Although traditional diagnostic methods, such as serological and polymerase chain reaction (PCR) testing, are useful for diagnosing MPP, they are insufficient in terms of sensitivity and specificity for early identification of RMPP. 12 Of note, PCR-based molecular testing offers an additional advantage beyond pathogen detection: it can identify macrolide resistance-associated mutations in the 23S ribosomal RNA gene, particularly at positions A2063G and A2064G, which are the predominant mutations conferring high-level macrolide resistance in MP strains circulating in China and East Asia.13,14 Early identification of these mutations via PCR can guide clinicians toward alternative antibiotic regimens—such as tetracyclines or fluoroquinolones—before clinical deterioration occurs, potentially preventing progression to RMPP. With advances in understanding the pathogenesis of RMPP, excessive host immune responses are now thought to be a key mechanism in its development. 15 It is important to clarify that RMPP does not arise from a “stronger” immune system per se, but rather from a dysregulated and unbalanced immune response. In susceptible individuals, the host immune system fails to appropriately modulate its reaction to MP infection: rather than mounting an effective, self-limiting response that clears the pathogen, the immune system enters a state of excessive and self-sustaining activation. This dysregulation—characterized by aberrant Th1/Th17 polarization, cytokine storm, and impaired regulatory T-cell function—results in paradoxical tissue destruction without superior pathogen clearance. 16 Therefore, monitoring inflammatory markers in MPP patients helps clinicians predict the onset of RMPP in advance, allowing for the timely initiation of individualized treatment. 17
This study retrospectively analyzed the clinical data of 223 children with MPP, aiming to explore the value of inflammatory markers such as C-reactive protein (CRP), lactate dehydrogenase (LDH), interleukin-6 (IL-6), and D-dimer in the early prediction of RMPP risk. The goal is to provide clinicians with more accurate tools for identifying children at risk of developing RMPP, enabling timely and personalized treatment strategies to improve patient prognosis.
Materials and Methods
Study Subjects
This study was a retrospective analysis that collected clinical data of 223 children diagnosed with MPP who were hospitalized at Lishui District People’s Hospital in Nanjing from June 2023 to February 2024. Inclusion criteria were (1) age between 6 months and 14 years; (2) confirmed Mycoplasma infection, established through detection of MPP nucleic acid by PCR in nasopharyngeal secretions—or, when PCR was negative, by serological criteria (paired sera) showing either (a) ≥4-fold rise in MP-IgG titer or (b) IgM seroconversion by chemiluminescent immunoassay—with single-serum IgM positivity alone not considered diagnostic; and (3) lung inflammation evident on chest x-ray or computed tomography. Exclusion criteria were (1) presence of other underlying conditions, such as immunodeficiency or congenital heart disease; (2) presence of other respiratory conditions, such as bronchopulmonary dysplasia, asthma, or pulmonary fibrosis; (3) incomplete data or loss to follow-up during treatment. This retrospective study was approved by the Ethics Committee of Lishui District People’s Hospital, Nanjing (No. 2024KY0802-01). The study was conducted in accordance with local legislation and institutional requirements. As this was a retrospective analysis of de-identified clinical data collected during routine medical care, written informed consent for participation was not required from the participants or their legal guardians/next of kin, in line with national legislation and institutional policies.
Patient Grouping
Patients were divided into 2 groups: GMPP and RMPP. The diagnostic criteria for RMPP included persistent symptoms after more than 7 days of standard macrolide antibiotic treatment, continued fever, worsening lung imaging, and extrapulmonary complications. A total of 52 patients met the criteria for RMPP, whereas the remaining 171 patients were classified into the GMPP group (Figure 1).
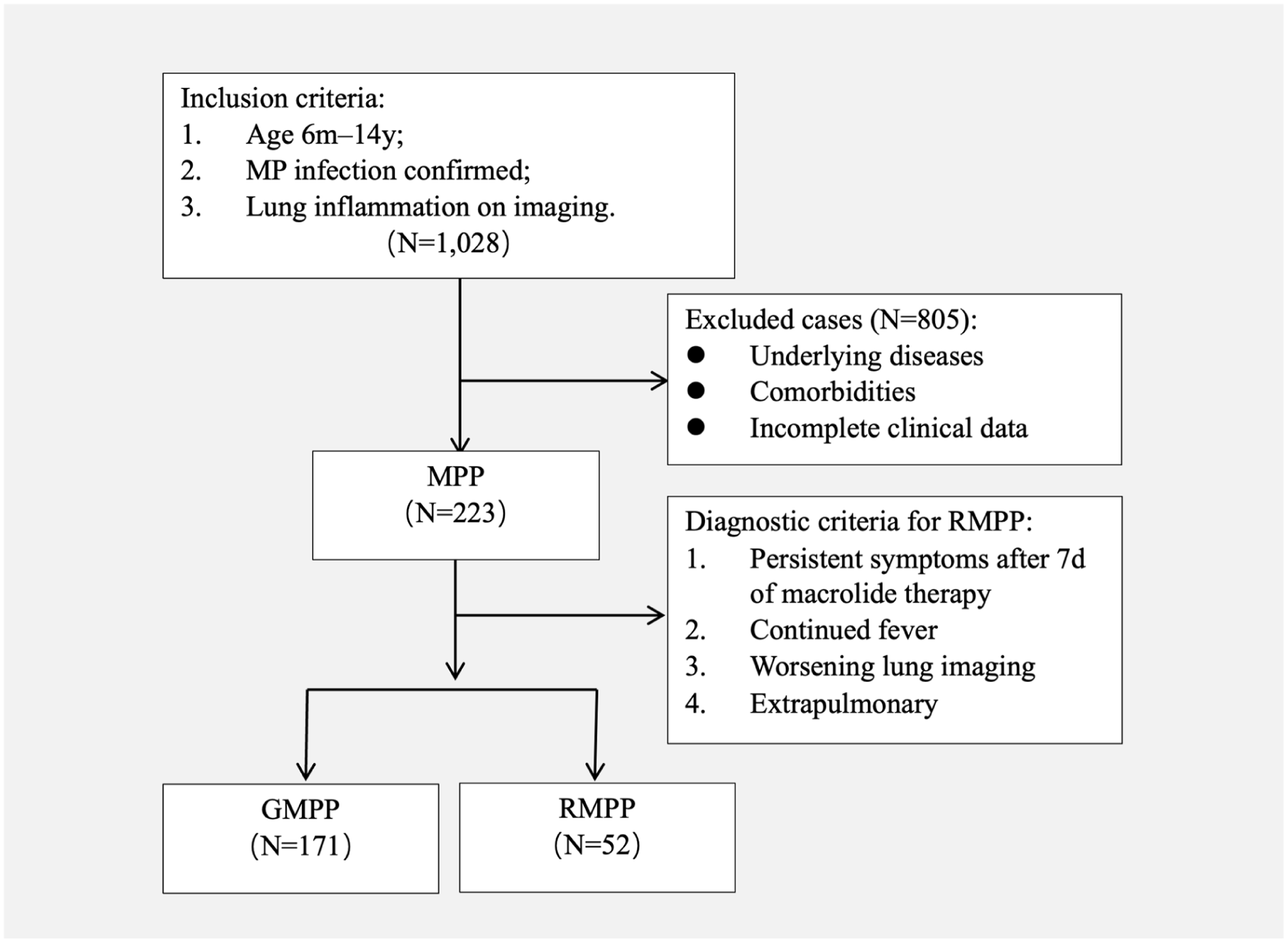
Study flowchart showing patient selection and group assignment.
Clinical Data
This retrospective study collected baseline characteristics, laboratory results, imaging findings, and treatment regimens for all patients. Baseline clinical characteristics included patient sex, age, clinical symptoms, and lung signs. Laboratory tests were conducted within 24 hours of admission and included PCR testing for respiratory pathogens such as adenovirus, respiratory syncytial virus, rhinovirus, influenza A and B viruses, and MP. Urinary antigen tests for Legionella and Streptococcus pneumoniae were not routinely performed, as the study focused on MP. Laboratory tests, including inflammatory markers (WBC, CRP, neutrophil percentage [NEP], procalcitonin [PCT], IL-6, D-dimer, and LDH), were conducted within 24 hours of hospital admission to capture early biomarkers that could predict RMPP risk. Imaging studies, including chest x-ray or computed tomography (CT) scans, were performed within 24 hours of hospital admission to confirm lung inflammation, as required for study inclusion. Findings such as lung consolidation, atelectasis, and pleural effusion were recorded based on these initial imaging studies. For patients diagnosed with RMPP, additional follow-up imaging was conducted as clinically indicated to assess disease progression, but only admission imaging data were used for comparative analyses in this study. Treatment regimens included antibiotics (macrolides as first-line therapy), glucocorticoids, immunoglobulins, tetracycline antibiotics, and bronchoalveolar lavage (BAL). All patients admitted were administered azithromycin (10 mg/kg/day) for anti-Mycoplasma therapy over a period of 5 to 7 days. In cases where persistent fever or deterioration of clinical symptoms was observed, corticosteroid treatment with methylprednisolone (2 mg/kg/day) was initiated. Immunoglobulin (1g/kg/dose) was administered to RMPP patients with severe inflammatory responses (eg, significantly elevated IL-6 or CRP) or clinical deterioration, such as persistent fever or worsening respiratory symptoms. Tetracycline antibiotics (doxycycline: 2 mg/kg/daily) were used in cases of suspected macrolide resistance, based on prolonged symptoms despite standard therapy, in accordance with Chinese guidelines. 8 Fluoroquinolones, a potential alternative for tetracycline-ineligible patients, were not administered in the present study given the predominant school-age population with no tetracycline contraindications.
Statistical Analysis
All data analyses were performed using SPSS 23.0 software. The distribution of continuous variables was tested for normality using the Shapiro-Wilk test. Normally distributed continuous variables were expressed as mean ± standard deviation (mean ± SD), and comparisons between groups were made using the independent sample t test. Non-normally distributed continuous variables were expressed as median (interquartile range), and comparisons were made using the Mann-Whitney U test. Categorical variables were expressed as frequencies and percentages (%), and comparisons were made using the chi-square test. When any expected frequency was less than 5, Fisher exact test was used. Laboratory indicators with significant differences in univariate analysis were further analyzed using multivariate logistic regression to assess their independent predictive value in diagnosing RMPP. The regression analysis results were expressed as odds ratio (OR) and 95% confidence interval (95% CI). Diagnostic performance was assessed by receiver operating characteristic (ROC) curves, calculating the area under the curve (AUC), sensitivity, and specificity. Nomograms and calibration curves were constructed using R software for quantitative prediction in clinical practice, assessing model fit and predictive accuracy. All statistical tests were 2-sided, and a P value < .05 was considered statistically significant.
Results
Comparison of Baseline Clinical Characteristics
In the GMPP group (171 cases), there were 84 male and 87 female patients, with an average age of 6.11 ± 3.11 years. In the RMPP group (52 cases), there were 19 male and 33 female patients, with an average age of 6.86 ± 3.37 years. No significant differences were found between the 2 groups in terms of gender distribution and average age (P > .05). Regarding clinical symptoms, all patients in the RMPP group presented with fever, and the proportion of dyspnea in this group was significantly higher than in the GMPP group (19.23% vs 7.77%, P < .01). The duration of symptoms (eg, fever or respiratory symptoms) before hospital admission was 4.77 ± 1.89 days in the GMPP group and 4.32 ± 2.03 days in the RMPP group, with no significant difference between the 2 groups (P > .05). There were no significant differences between the 2 groups in terms of cough, runny nose, gastrointestinal symptoms, or lung rales. Imaging findings showed that the incidence of bronchopneumonia was more prevalent in the GMPP group (61.04%) compared with the RMPP group (21.15%). whereas more severe radiographic findings were significantly more common in the RMPP group: lung consolidation (78.84% vs 38.95%, P < .01), atelectasis (11.53% vs 1.74%, P < .01), and pleural effusion (15.38% vs 1.74%, P < .01). Regarding treatment, all patients in the RMPP group received glucocorticoid therapy. Meanwhile, 23.07% of patients received immunoglobulin for severe inflammation or poor steroid response. A total of 30.77% of patients were switched to doxycycline due to suspected macrolide resistance or inadequate response, and 15.38% (8/52) of RMPP patients underwent BAL, mostly due to severe or persistent lung consolidation, atelectasis, or mucus plugging seen on imaging. BAL is not widely used because it is invasive and requires special equipment, so that it is used mainly in cases of significant airway blockage or when other treatments fail. These treatment options showed significant differences between the 2 groups (P < .01). Furthermore, the average length of hospital stay was significantly longer for the RMPP group compared with the GMPP group (12.16 ± 2.54 days vs 7.21 ± 3.06 days, P < .01) (Table 1).
Comparison of Clinical Characteristics, Imaging, and Treatment Between General Mycoplasma pneumoniae Pneumonia (GMPP) Group and Refractory Mycoplasma pneumoniae Pneumonia (RMPP) Group.

Laboratory Test Results
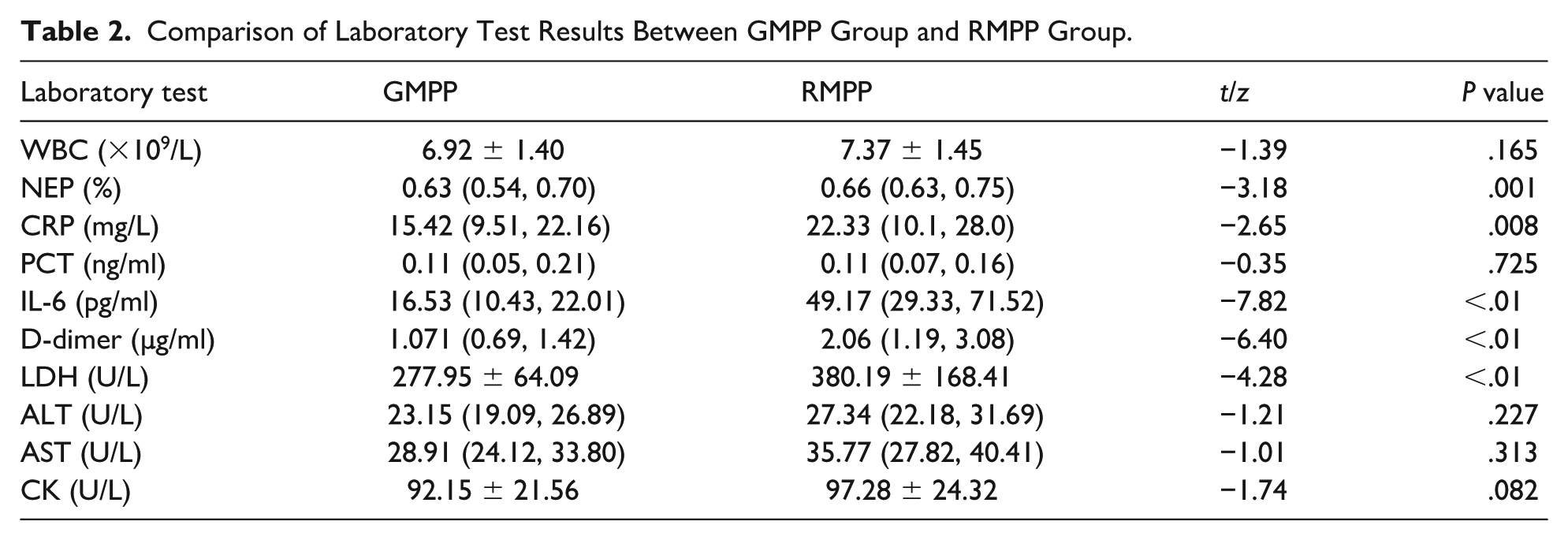
As shown in Table 2, serum CRP, D-dimer, IL-6, and LDH levels were significantly elevated in the RMPP group compared with the GMPP group (P < .01), suggesting that these inflammation and damage-related markers were more pronounced in the RMPP group. In contrast, no significant differences were found between the 2 groups in terms of WBC count, NEP, PCT, alanine aminotransferase (ALT), aspartate aminotransferase (AST), and CK (P > .01).
Comparison of Laboratory Test Results Between GMPP Group and RMPP Group.
Multivariate Logistic Regression Analysis of RMPP Risk Factors
Laboratory markers that showed significant differences in univariate analysis (CRP, IL-6, D-dimer, and LDH) were included in a multivariate logistic regression model. The results indicated that LDH (OR = 1.109, 95% CI: 1.003-1.115), IL-6 (OR = 1.141, 95% CI: 1.078-1.187), and D-dimer (OR = 8.27, 95% CI: 3.00-22.797) were important predictive factors for the occurrence of RMPP (Table 3).
Multivariate Logistic Regression Analysis of Predictive Factors for RMPP.

Predictive Value of Serum IL-6, D-dimer, and LDH for RMPP
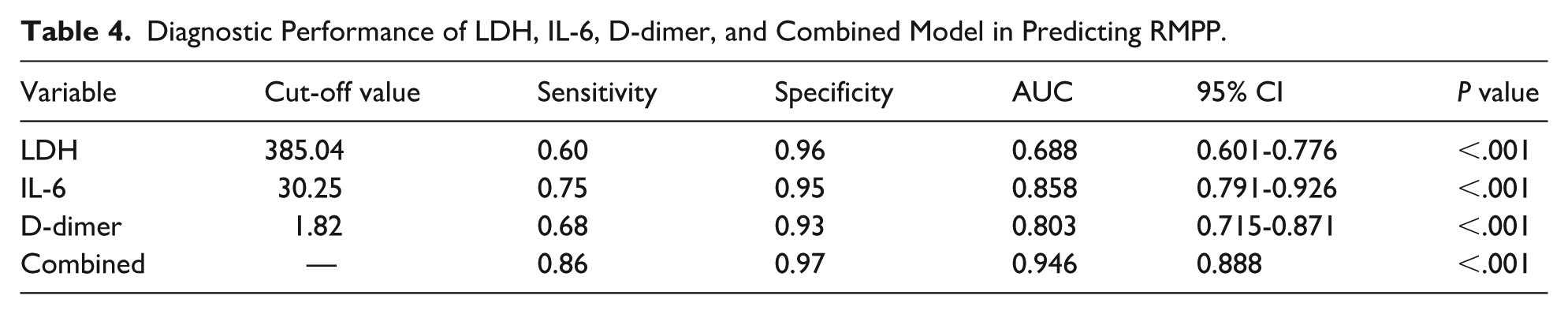
Based on logistic regression analysis results, ROC curves were plotted and AUC values were calculated to further explore the predictive value of serum IL-6, D-dimer, and LDH levels for RMPP. The ROC curve analysis showed that each of these markers had good diagnostic performance for predicting RMPP: the AUC for IL-6 was 0.858 (95% CI: 0.791-0.926), with an optimal cut-off value of 30.25 pg/ml, sensitivity of 0.75, and specificity of 0.95; the AUC for D-dimer was 0.803 (95% CI: 0.715-0.871), with an optimal cut-off value of 1.82 µg/ml, sensitivity of 0.68, and specificity of 0.93; and the AUC for LDH was 0.688 (95% CI: 0.601-0.776), with an optimal cut-off value of 385.04 U/L, sensitivity of 0.60, and specificity of 0.96. These results indicate that IL-6 and D-dimer have higher diagnostic accuracy, whereas LDH, though with a lower AUC, still provides some reference for predicting RMPP. Finally, a combined detection model incorporating IL-6, D-dimer, and LDH was constructed. The ROC curve analysis showed that the combined model had an AUC of 0.946, significantly improving diagnostic sensitivity and specificity (Table 4, Figure 2). A bootstrap interpolation method with 1000 resampling iterations was used to assess the model’s calibration curve and ROC curve. Figure 2 shows that the mean absolute error (MAE) between the predicted probability and the actual probability was 0.02, indicating that the model has good predictive ability (Figure 3) .
Diagnostic Performance of LDH, IL-6, D-dimer, and Combined Model in Predicting RMPP.

ROC curves of LDH, IL-6, D-dimer, and combined model for predicting RMPP.

Calibration curve of the model.
Construction of the Nomogram for Predicting RMPP
Using the 3 independent factors (IL-6, D-dimer, LDH), a nomogram was constructed to identify RMPP (Figure 4). For example, a child with MPP, with LDH of 230 U/L, IL-6 of 76.15 pg/ml, and D-dimer of 1.90 µg/ml, had a total score of approximately 92 (10 + 24 + 58), corresponding to a risk of 0.51.

Nomogram for predicting RMPP.
Discussion
This study conducted a retrospective analysis of the clinical characteristics of 52 patients with RMPP and compared them to those with GMPP. The results demonstrated that RMPP patients had significantly more severe clinical manifestations, including a 19.23% incidence of dyspnea and markedly higher rates of lung consolidation (78.84%), atelectasis (11.53%), and pleural effusion (15.38%) compared with the GMPP group—findings consistent with those from previous clinical studies.18,19 The clinical differences between the 2 groups suggest that lung lesions in RMPP are more extensive and complex, with a higher risk of complications such as atelectasis, necrotizing pneumonia, and bronchiolitis obliterans. Given that RMPP patients had a higher incidence of severe radiological abnormalities (lung consolidation, atelectasis, pleural effusion) at admission, early imaging might help identify RMPP-prone patients, enhancing the predictive power of inflammatory markers. The imaging spectrum of RMPP differs substantially from that of GMPP: GMPP typically presents with diffuse bronchopneumonia or bilateral ground-glass opacities on chest x-ray or CT, whereas RMPP is characterized by large lobar or segmental consolidation—often involving an entire lobe—along with mucus plugging, atelectasis, necrotizing pneumonia, and pleural effusion. In severe cases, CT may reveal cavitation or early features of bronchiolitis obliterans. These distinct radiological patterns, when integrated with clinical and laboratory data, can further support the early stratification of patients at risk for RMPP. These complications notably increase hospitalization duration and healthcare burden. 20 All RMPP patients received corticosteroid treatment, underscoring the critical role of glucocorticoids in RMPP management. 21 In addition, 23.07% of patients required immunoglobulin, 30.77% received tetracycline antibiotics, and 15.38% underwent alveolar lavage, reflecting the complexity and individualized needs of RMPP treatment. 16 In contrast, the treatment strategy for GMPP patients was relatively simpler, highlighting the necessity for more comprehensive therapeutic approaches for RMPP patients.
Therefore, early and accurate identification of RMPP is crucial for implementing effective treatment measures and improving patient outcomes. However, current diagnostic methods for MP, such as serological testing, PCR testing, and imaging, primarily confirm infection without effectively distinguishing between GMPP and RMPP. 22 The limitations of these traditional diagnostic tools hinder the timely identification of potential RMPP cases, resulting in delays in optimal treatment. Hence, there is a pressing need in clinical practice for auxiliary tools that can distinguish RMPP early and evaluate disease severity. While GMPP patients generally respond well to antibiotic therapy, the condition of RMPP patients is considerably more complex. In the early stages of Mycoplasma infection, the pathogen infiltrates the lower respiratory tract through the airways and adheres to the ciliated epithelial cells of the respiratory mucosa, causing direct damage via secreted toxins such as CARDS toxin and hydrogen peroxide. 23 Concurrently, the host’s innate immune system is activated, triggering immune responses from monocytes, macrophages, and dendritic cells. 24 The adaptive immune response, mediated by T cells, also unfolds in response to the infection. 25 The host immune response is a double-edged sword; an appropriate response, including cytokine secretion and lymphocyte activation, is essential for clearing MP and alleviating disease symptoms. 26 However, in RMPP patients, dysregulation of immune response leads to an excessively activated inflammatory reaction. 27 Research has shown that Th1 and Th17 cells are significantly increased in RMPP patients, releasing a large amount of pro-inflammatory cytokines such as IL-6, tumor necrosis factor-α, and interferon-γ. These persistently elevated cytokines exacerbate lung inflammation and tissue damage. 28 With lung tissue damage, the integrity of cellular membranes is compromised, leading to the release of cellular contents like LDH into the bloodstream. 29 Elevated serum LDH often indicates the need for higher doses of corticosteroids during clinical treatment to manage intense pulmonary inflammation. 30 Dysregulation of the fibrinolytic system is also an important mechanism in the pathogenesis of RMPP. 31 The fibrinolytic system regulates thrombosis and dissolution, and Mycoplasma infection activates this system, causing a significant increase in fibrinolytic markers such as D-dimer. 32 The interaction between the fibrinolytic system and the immune response intensifies lung tissue damage and may lead to thrombosis and extrapulmonary organ injury. 33 A retrospective study by Hang C demonstrated that children with elevated D-dimer levels and MP infection often exhibited more severe imaging findings and a propensity for vascular embolism. 34 Against this backdrop, the importance of inflammatory biomarkers has become increasingly apparent. Early detection of inflammatory biomarkers offers a new approach for early recognition and precise treatment of RMPP. By tracking changes in these markers, clinicians can better assess disease progression, adjust treatment promptly, and prevent severe complications.
This study retrospectively evaluated commonly used inflammatory biomarkers, including IL-6, D-dimer, and lactate dehydrogenase (LDH), in the early prediction and identification of RMPP in children. Analyzing clinical data from 223 children diagnosed with MPP, we found that individual biomarkers showed certain sensitivity and specificity in RMPP prediction, with AUCs of 0.858, 0.803, and 0.688 for IL-6, D-dimer, and LDH, respectively. This study further investigated the effect of combined detection of IL-6, D-dimer, and LDH. A combined predictive model was constructed using logistic regression analysis, and the results showed that the combined model’s AUC increased to 0.946. Internal validation revealed good alignment between the calibration curve and the standard curve, indicating improved detection efficacy. Compared with individual biomarkers, combined detection provides a more comprehensive assessment of disease severity, reflecting the complex inflammatory response and tissue damage in patients, thereby enhancing early diagnostic accuracy, particularly in the early stages when clinical symptoms are not yet pronounced. Other studies have found that variables such as fever duration and hospitalization length, while important factors in RMPP incidence,35,36 are often delayed in early prediction of RMPP. In contrast, laboratory inflammatory biomarkers can provide earlier insights into disease progression. This study presented predictive results for IL-6, D-dimer, and LDH through a nomogram, offering clinicians a digital tool to enable timely personalized treatment interventions (such as corticosteroids, immunoglobulin, and tetracycline antibiotics), thereby reducing disease progression and complication risks. Our findings suggest that a combined detection model based on IL-6, D-dimer, and LDH provides an effective tool for the early identification and precise treatment of RMPP. Future studies could further explore the combined effects of additional inflammatory markers to expand early detection methods for RMPP.
Study Limitations
Despite valuable findings in early identification and prediction of RMPP, this study has limitations. First, as a single-center retrospective study, the relatively small sample size may affect the stability of statistical analyses and the generalizability of the results. Second, the completeness and accuracy of data in retrospective studies may be limited. This study relied on previous clinical records and laboratory results, which may have gaps or incomplete data. To minimize these issues, data integrity and accuracy were ensured during data collection and analysis, but potential biases cannot be entirely excluded. Finally, this study did not delve into the specific roles of these inflammatory biomarkers in the pathogenesis of RMPP. Although a significant association between biomarker levels and disease severity was found, the underlying biological mechanisms remain unclear. Future basic research should further clarify how these biomarkers influence Mycoplasma infection and the host’s inflammatory response to provide theoretical support for clinical applications. In addition, this study measured inflammatory markers only at hospital admission and did not assess their kinetic patterns over the course of MPP infection. Future studies with serial measurements could provide further insights into how these markers evolve and persist in relation to RMPP development.
Conclusion
Interleukin-6, D-dimer, and LDH serve as critical inflammatory biomarkers for the early prediction of RMPP, offering enhanced disease assessment and facilitating timely, targeted therapeutic interventions that improve clinical outcomes. Proper utilization of these biomarkers can significantly enhance the management of RMPP patients, reducing mortality and the incidence of complications.
Author Contributions
Yang Yu (first author) contributed to the study design, data collection, and analysis, and was responsible for writing the manuscript. He also revised the manuscript critically for important intellectual content. Yu Xia (corresponding author, second author) assisted in the study design, supervised the data analysis, and provided critical revisions to the manuscript. He is responsible for correspondence regarding the manuscript and ensured the overall quality of the research. Rufeng Ji (Co-corresponding authors) participated in the data collection process and contributed to the interpretation of results. She also provided significant support in the literature review and manuscript writing.
Footnotes
Acknowledgements
The authors have acknowledged Professor Qiao Lixing and Dr Wei Hongjuan for their guidance and statistical support in the study.
Ethics Approval
This study was approved by the ethics committee of Lishui District People’s Hospital, Nanjing (No. 2024KY0802-01).
Consent to Participate
Informed consent was obtained from the parents or legal guardians of all participants included in this retorspective study.
Patient Consent for Publication
This article does not contain any personal data or images requiring patient consent for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Nanjing Science and Technology Project (Project No. 201803074).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
We confirm that the data used in this study are available upon request.