
Abstract

Educational Objectives
Traumatic injuries, whether accidental or inflicted, might be a contributory cause of the onset of Streptococcus pneumoniae–associated hemolytic uremic syndrome.
Physical abuse must be considered in the differential diagnosis of any critically injured young child, especially if presentation is unusual or poorly explained.
Case Report
A 2-year-old girl was transferred to the pediatric intensive care unit of a tertiary care hospital following 3 days of abdominal discomfort, fever, and fatigue. Her past medical history was uneventful, and her immunization was up to date, including 4 doses of the 13-valent pneumococcal conjugate vaccine (PCV13) schedule. On arrival, vital signs were notable for fever (39.4 °C), tachypnea (48 rpm), tachycardia (180 bpm) with normal blood pressure (91/63 mm Hg), and oxygen saturation (99%). The patient presented labored breathing and a distended abdomen but had normal neurological and hemodynamic status. Extensive skin abrasions covering half the back and the left arm were noted. The initial laboratory investigation revealed pancytopenia (hemoglobin 80 g/L, white blood cell count 1.2 × 109/L and platelet count 43 × 109/L), acute renal failure (serum creatinine 145 μmol/L), normal urinalysis and elevated transaminases (ALT 985 U/L, AST 631 U/L). A chest x-ray showed opacification at the base of both lungs, and an abdomen ultrasound performed at the referral center identified a possible mass in the left upper quadrant. Sepsis and abdominal neoplasia were the initial diagnoses considered. However, schistocytes on a peripheral blood smear and the raised lactate dehydrogenase were consistent with microangiopathic hemolytic anemia. The diagnosis of Streptococcus pneumoniae-associated hemolytic uremic syndrome (Sp-HUS) was confirmed with the identification of Streptococcus pneumoniae (serotype 10A) in the blood culture, a serotype not covered by her previous PCV13 vaccination.
Hospital Course
Abdominal and thoracic computed tomography (CT) did not identify any signs of pneumonia or abdominal mass but, unexpectedly, revealed multiple posterior rib fractures (8th, 9th, and 10th left side and 10th right side), pulmonary contusions in both lower lobes and a small left hemothorax (see Figure 1).
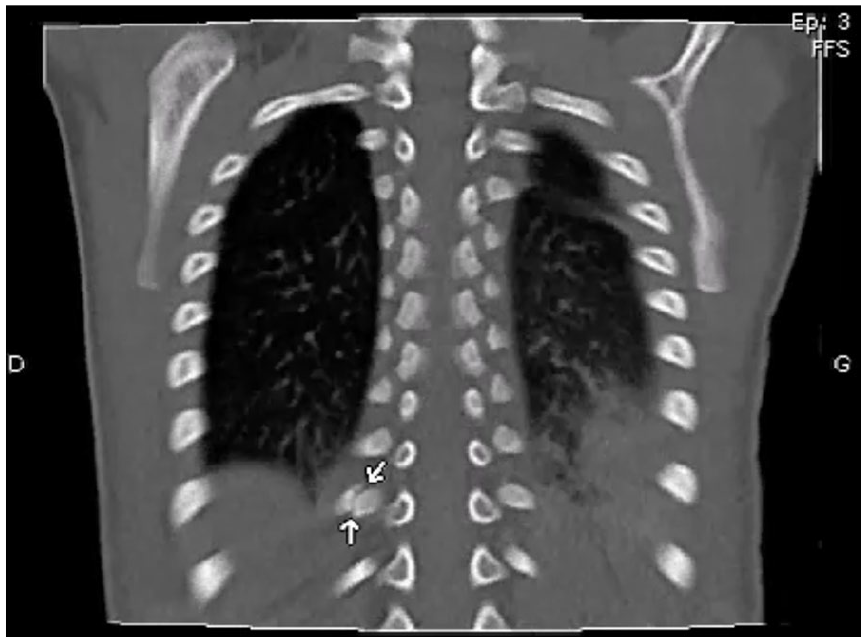
Chest computed tomography showing rib fracture (10th right side), pulmonary contusions in both lower lobes and left hemothorax.
An abdominal ultrasound was repeated by a pediatric radiologist and revealed a hyperechoic lesion on hepatic segment VII suggestive of hematoma, which was not visible on the CT, probably due to technical limitations. This finding was consistent with elevated liver transaminases which remained high for 2 weeks. Frank hematuria occurred and persisted for a month. It was attributed to HUS rather than trauma to the urinary tract and kidneys. Given the patient‘s precarious condition, bedside ultrasounds were favored subsequently, with no progression of the hepatic lesion and no signs of peritonitis. With no history of significant or high-velocity accidental trauma, child protective services were involved, and a forensic evaluation was completed. Cerebral magnetic resonance imaging was normal and fundoscopic examination directed by an ophthalmologist showed no retinal hemorrhages. Three additional subacute fractures (4th and 7th left rib and scapula) were identified when skeletal survey (21 films) became feasible 3 weeks after the patient’s admission to the hospital. This could not be conducted earlier in the child’s medical course because of significant instability. No medical conditions predisposing to bony injuries or bleeding diathesis were found.
Social history revealed that the patient lived alone with her mother. Prior to the onset of symptoms, the patient spent the weekend at family members‘ home. When her mother returned, she noticed swollen and lacerated lips as well as abrasions on her back and left arm. Grandparents reported that the child had fallen forward while running outside.
After the rib fractures were identified, the child abuse pediatrician became involved. On detailed physical examination, significant lip swelling was noted with crusted lesions on the upper lip, but no other oral injuries (including normal frenulum). There were also extensive abrasions covering the lower middle third of the back. There was no identified bruising or patterned injuries. Specifically, there were no skin findings overlying the rib fractures. Skin examination may have been impacted by the dark skin tone of the patient. In the absence of a history of plausible significant accidental trauma, the appearance, severity and location of the skin findings were suggestive of inflicted trauma. Skin biopsy showed hypodermic necrosis, but no evidence of purpura that might be associated with the low platelet count associated with the HUS.
The patient‘s condition significantly deteriorated over the first 24 hours after admission. Antibiotics were initiated (intravenous piperacillin/tazobactam) as blood cultures grew S. pneumoniae serotype 10A sensitive to penicillin. Eculizumab was initiated as first-line treatment for atypical HUS. Nonetheless, renal failure progressed, and peritoneal dialysis was required for 7 days. The patient remained critically ill despite blood transfusions and developed multiple organ failure. Cardiac arrest occurred and resuscitation was performed with epinephrine administration and chest compressions. Pericardial effusion developed afterward, requiring pericardiocentesis and continued drainage.
After 4 weeks in the Intensive Care Unit and 6 weeks in the pediatric ward, the patient recovered fully with no residual renal dysfunction or neurological deficit. She was discharged to her mother‘s care with the authorization of child welfare services. No additional information in relation to potential mechanisms was brought forward following social and police investigations. The mother provided consent for the dissemination of this case report.
Discussion
Hemolytic uremic syndrome (HUS) is a rare but severe condition in children characterized by a classic triad of acute hemolytic anemia, thrombocytopenia, and acute kidney injury. 1 While this condition is mainly associated with Shiga toxin-producing E. coli (STEC), the association with Streptococcus pneumonia accounts for 5% of all childhood HUS. 2 The majority of patients with Streptococcus pneumoniae-associated hemolytic uremic syndrome (Sp-HUS) present with pneumonia with or without pleural effusion (72% of patients), and meningitis accounts for most of the remaining cases (29%). 3 Compared with the typical form, patients with Sp-HUS have a more severely acute course of renal, hematologic, and neurologic diseases and higher mortality (between 2% and 12%). 4
While the pathomechanisms of Shiga toxin-mediated microangiopathy in patients with STEC-related HUS are well described, those involving Sp-HUS remain to be clarified. In the absence of the more common initial clinical presentations of Sp-HUS, mainly pneumonia and meningitis, we hypothesized that traumatic injuries were contributory to the development of the disease in our patient. Recent cohort studies indicated that Sp-HUS tends to develop in patients with loculated infected fluid collections such as parapneumonic empyema and subdural hematoma. 5 Our patient‘s hemothorax and pulmonary contusions could have led to a significant bacterial load, one of the main physiopathology hypotheses for Sp-HUS. 6 Moreover, the visceral injuries could have been a contributing factor to the disease, as the blunt trauma to the abdomen might have caused direct endothelial cell lesions in the microvasculature of the kidney, a common feature of all forms of hemolytic uremic syndrome.1-3 These arguments support our assumption that significant traumatic injuries might have created a favorable environment for S. pneumoniae to proliferate and that direct endothelial cell damage to the kidneys and liver may have facilitated the onset of HUS within the context of circulating S. pneumoniae.
Recognition of child abuse by practitioners can be challenging, even more so with severely ill patients in the intensive care setting. In this case, maltreatment concerns were raised following investigations, even if it had not been included in our initial differential diagnosis. In situations of elevated hepatic transaminases (> 80 IU/L), abdominal injury should always be considered and imaging must be performed—preferably CT which is normally more accurate in detecting this kind of injury. 7 Rib fractures have a strong association with inflicted injury in the absence of high-velocity trauma. Specificity is increased when the rib fractures they are multiple, bilateral and posterior.8,9 A scapula fracture is another highly specific finding of child maltreatment. 8 These fractures associated with unexplained underlying pulmonary contusions, hemothorax and liver hematoma suggest violent blows to, or compression of the chest. Unwitnessed injury, delay in seeking medical attention and presence of highly suspicious oral and skin injuries on the torso of a young child are other red flags for inflicted trauma that were also present in our patient’s case.10,11
Interestingly, a case report published in 1996 by Sajjanhar et al 12 presented a 13-month-old boy with Sp-HUS and subdural hematoma. Despite the well-documented link between subdural hematoma and child abuse, the authors rejected the diagnosis of non-accidental injury on the basis of absence of bruising and retinal hemorrhage. No skeletal survey was reported to have been performed at that time. Consequently, occult fractures could have been missed. This heightens the importance of considering maltreatment in the differential diagnosis of any critically injured young child, especially if presentation is unusual or poorly explained.
Final Diagnosis
The patient was diagnosed with Streptococcus pneumoniae-associated hemolytic uremic syndrome (Sp-HUS) in the setting of multiple posterior rib fractures, bilateral lung contusions, left hemothorax, and liver hematoma injuries with no history of high-velocity trauma. Despite broad-spectrum antibiotics, eculizumab, and peritoneal dialysis, the patient developed multiple organ dysfunction syndrome. She eventually recovered with no persistent renal dysfunction or neurological deficit. Ultimately, the identification of injuries highly suggestive of maltreatment combined with an extensive social evaluation by child protective services led the Youth Court to retain the diagnosis of physical abuse for this child.
Conclusion
To our knowledge, this is the first report of pneumococcal hemolytic uremic syndrome related to traumatic injuries in the context of child abuse. This case provides additional information about the pathogenesis of the disease by supporting the hypothesis that polytrauma, whether accidental or inflicted, might be a contributory cause of the onset of Sp-HUS through thoracic fluid collections and direct endothelial cell damage to kidney. Given the severity of diagnosis and potential for morbidity and mortality, timely recognition and appropriate management of both HUS and child abuse are of paramount importance. For a rare and severe disease such as Sp-HUS, clinicians should maintain a high level of suspicion for abusive injuries in the absence of the classic presentation of pneumonia or meningitis. For child abuse consultants, it emphasizes the relevance of a dedicated medical evaluation of any suspicious lesions, including in critically ill patients.
Author Contributions
Footnotes
Acknowledgements
Thank you to Dre Clara Low, Dr Tremblay-Roy, Dr Frédéric Dallaire, and Dr Claude Cyr for their review of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval to report this case was obtained from Centre hospitalier universitaire de Sherbrooke Institutional Review Board (approval # 2021-4185) on July 21, 2021 (renewed July 21, 2023). Written informed consent was obtained from the patient’s legal guardian (mother) for the publication of this case report.