
Abstract

US medical providers have historically tried to prevent the harms of stigma by “normalizing” the sex of children with intersex variations/differences of sex development (I/DSD), 1 also called variations of sex characteristics (VSC).1,2 Meanwhile, adults with I/DSD have reported suffering resulting from even well-meaning pediatric protocols.1,3 -5 Revised care models, intended to be informed by bioethics, were designed with the intention to avoid this suffering. However, if clinical ethics cannot imagine a future in which sex diversity is accepted and affirmed, clinical care risks enacting the future it aims to avert: an adult struggling with trauma, shame, and internalized stigma. US intersex adults have reported poor general and mental health 6 and sexual well-being. 7 In a community survey of US adults with I/DSD, 61.7% screened positive for depressive symptoms, and 31.8% reported a lifetime suicide attempt, 6 markedly higher than the US lifetime prevalence of 4.6%. 8 In service of the Pediatric Endocrine Society’s goal to “support efforts to raise resilient individuals who have genital differences,” 9 a paradigm that radically destigmatizes I/DSD is overdue.
Fortunately, there is increasing recognition of the need to accept sex diversity. 10 Nonetheless, significant challenges hinder this shift. This article reviews how affirmation of sex diversity has been neglected when applying bioethical principles to I/DSD care. It then outlines an alternative paradigm that affirms sex diversity and accompanying psychosocial challenges. In the service of destigmatizing I/DSD, herein, we will predominantly use the terminology intersex/variations of sex characteristics (I/VSC), 2 while at times using I/DSD to reflect terminology in the referenced texts.
An international consensus statement defines I/DSD as “congenital conditions in which development of chromosomal, gonadal, or anatomic sex is atypical.” 11 Here, we focus on pediatric persons with I/VSC for whom medical care has commonly involved early interventions on primary sex traits (eg, genitoplasty, gonadectomy). This includes infants and children born with genital difference (“ambiguity”), gonads discordant with assigned gender, and/or dysgenetic gonads. Intervention refers to treatments, including surgeries, that can be safely deferred until the patient is older, not interventions that are urgently necessary to prevent imminent physical harm. Table 1 offers definitions of other key terms.
Definitions of Relevant Terms.

Recent Clinical Intersex/Variations of Sex Characteristics Care
Principlism upholds autonomy, beneficence, non-maleficence, and justice as primary moral principles in bioethics. 12 In pediatric clinical ethics, surrogate decision-makers (most often parents) serve as proxies for pre-autonomous patients. The American Medical Association’s Council on Ethical and Judicial Affairs found that surrogate decision-making with shared decision-making was the most ethical strategy for children with I/DSD. 13 Although a vast improvement over the doctor-driven 20th-century approach, this revised paradigm applies principlism through a medicalizing lens 14 shaped by cisnormative and heteronormative attitudes. Failure to critically evaluate the role of these biases, particularly in the analyses of beneficence and non-maleficence, may perpetuate stigma, shame, and trauma.
Consider a hypothetical child born with genital difference associated with 46, partial androgen insensitivity syndrome (PAIS) and assigned female at birth. To align anatomy with assigned sex, physicians offer genitoplasty to shorten the child’s clitoris and to create a vulva. Informed consent, including the risk-benefit discussion about the surgery, is grounded in medical information about protection from stigma and rates of reoperation, urinary or sexual dysfunction, fertility, and “gender incongruence.” 9 The unspoken background to the conversation is a set of normative assumptions about gender, sex, and sexuality, described in Table 2.4,14,15
Cisnormative, Heteronormative, and Medicalized Assumptions Embedded in the Traditional Model of I/DSD Care.
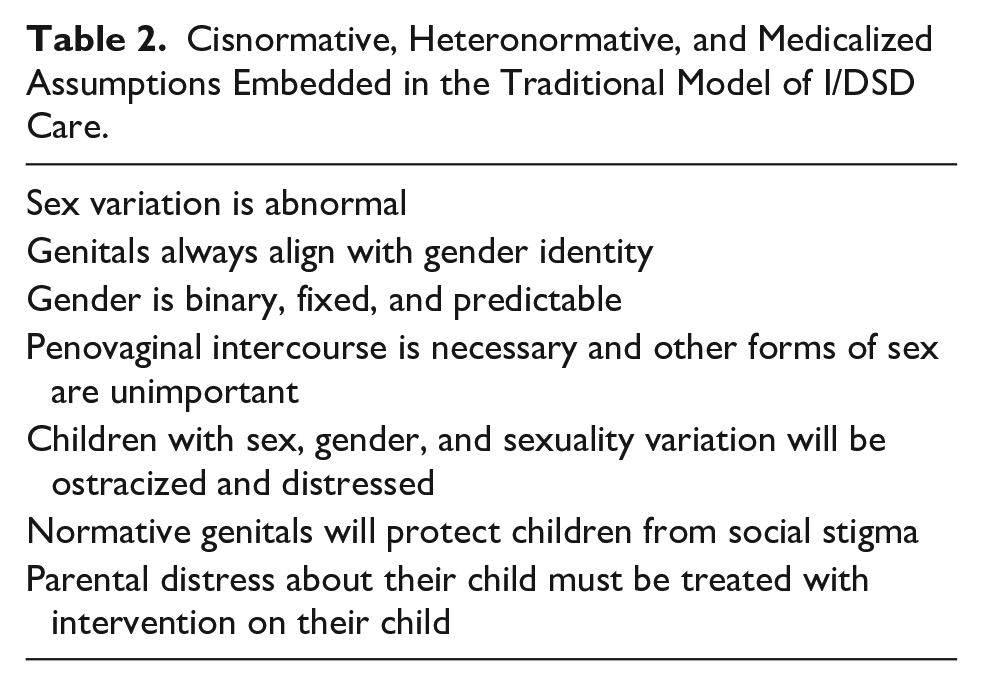
“Stigma” is thus shorthand for uncertainty about whether the child will meet criteria for “normal” and risk of social rejection. Compounding this uncertainty are unknowns regarding the child’s future gender and sexual development. Discomfort with these unknowns can exacerbate parental distress16,17 and create urgency to attempt to resolve, rather than accept, them.2,18 In this context, a natural conclusion is that it is in the child and family’s best interest to assign a binary sex and cisgender of rearing and to align the child’s genitals with that assignment. However well-intentioned, “correcting” a child‘s genitalia to avoid stigma has been identified as enactment of stigma in a medical context,15,19,20 lacks robust evidence of psychosocial benefit, 21 and may be a mechanism by which patients experience harm into adulthood.22,23 It is on this basis that early genital surgery, which presumes that sex diversity is a problem in need of treatment, has been likened to sexual orientation change efforts. 24 In other words, as has been detailed elsewhere,1,4,5 the medical community has treated “ambiguous genitalia” as a social emergency requiring urgent surgery, for which truly informed consent often has not been obtained, 5 when the reality is that surgeries that serve merely to alter sex features are elective and medically safe to defer until the concerned individual can participate in the decision.1,4,5
We do not dispute that stigma associated with I/VSC is real and harmful.16,25 -27 A goal of ethical intersex care should be to reduce the impact of stigma on a person’s life. However, the oft-cited rationale for recent care approaches of “avoid[ing] stigmatization related to atypical anatomy” 28 is dangerous and insufficient when cisnormativity and heteronormativity are foregrounded in the analyses of beneficence and non-maleficence. 15
Because cisnormative and heteronormative biases are part of the societal air we breathe, most clinicians and parents/guardians are influenced by these attitudes and are unaware of how they may impact clinical decision-making. Allaying stigma-related parental distress is a central goal of care.16,17 However, clinicians influence parents’ perceptions of stigma, including how parental views of children’s genitals,29,30 and understandings of what constitutes abnormal, normal, 31 and suffering.15,32 Difficulty processing information in the setting of distress can exacerbate this dynamic,18,33 and some parents have reported agreeing to surgery upon feeling pressure from clinicians. 4 This reveals how heavily the perception of a child’s best interest is influenced by the specter of stigma toward sex variation. In this way, the opportunity to reduce the impact of stigma is missed and iatrogenic stigma is introduced.
In summary, the early 21st-century treatment approach is built on an assumption that “accurate” sex assignment and surgery eradicate stigma and prevent suffering. Affirmation of sex diversity has been missing from the application of the principlist paradigm. Yet, major shifts in I/VSC care in the early 2000s,11,34 and increasing general acceptance of sex and gender diversity, 21 suggest that sex diversity need not be forever de facto stigmatized by clinicians.
Emerging Alternative Approach
Affirmation of sex diversity demands a radical reimagination of I/VSC medical care. Providers must examine and reduce the influences of heteronormativity, cisnormativity, and medicalization on their upbringing recommendations and surgical counseling. This aligns with the 2020 position statement of the Pediatric Endocrine Society, which “advocates for advances in acceptance by the broader society of individuals with physical differences and/or non-binary gender expression.” 9
Creating an Open Future
To illustrate this alternative, let us revisit the hypothetical infant with 46,XY PAIS and apply an affirming model, delineated in Table 3. The clinicians characterize genital difference as one aspect of the spectrum of human variations,35,36 explaining that all genitals vary37 -39 and that genitals do not single-handedly define well-being or gender identity. Absent urgent physical health need, the clinicians observe that there is little advantage to altering the child’s genitals in early childhood.
Comparison of the Traditional and Affirming Models.
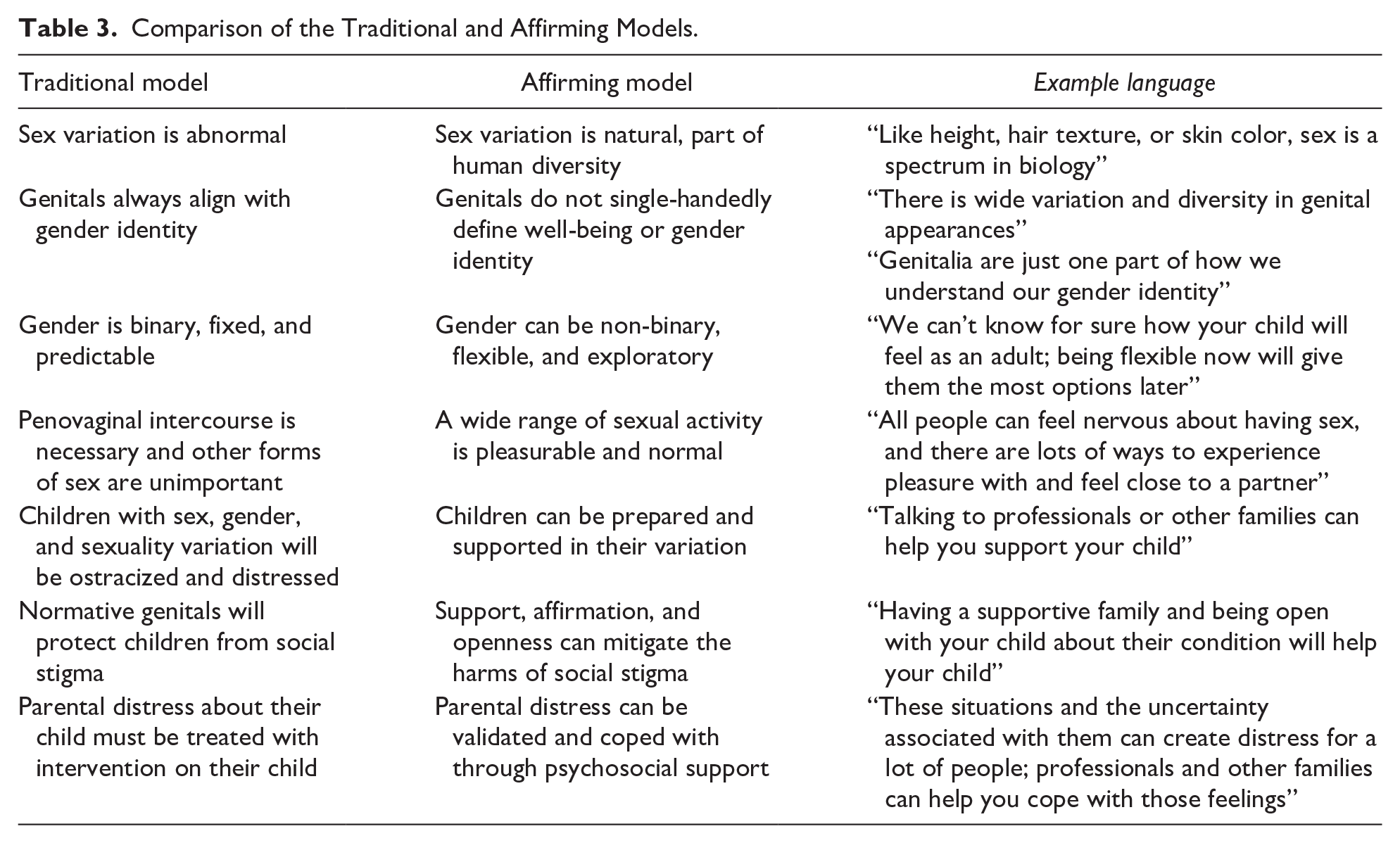
The clinicians may encourage a non-binary—or at least flexible—social gender of upbringing in support of an open future. 40 They emphasize the inability to predict the child’s eventual gender identity or sexuality. The parents are encouraged to avoid assumptions that may turn out to be false, allowing the child to be free to explore gender, and eventually sexuality, on their own terms.
The clinicians do not ignore negative impacts of societal stigma. In fact, the clinical team acknowledges and validates the potentially distressing uncertainties of raising a child with genital difference. 18 Rather than offering a surgical solution to a psychosocial problem, the clinicians facilitate professional and peer psychosocial support and emphasize prioritizing the child’s well-being over societal expectations. The clinicians draw from queer and disability ethics-informed practices that affirm differences rather than erase or “fix” them.41,42 Clinicians use evidence from sexual and gender minority populations that stigma-related problems are mitigated by social acceptance and support 21 to frame affirming psychosocial support as a tool to promote well-being. Indeed, condition openness and peer support have been shown to improve well-being19,43 and further normalize sex and gender diversity.2,44 -46 Peer support includes connecting patient and families with community groups (eg, interACT, InterConnect, and Beautiful Your MRKH Foundation) which parents and patients report as being uniquely beneficial.2,23
As the child grows, their clinicians orient interventions toward affirming bodily diversity and promoting autonomy in a way that is conscious of—but not driven by—societal stigma. They educate the child about their anatomy on the spectrum of genital diversity seen among all people.37 -39 Psychosocial interventions expose the child to language, relationships, and role models that affirm difference and empower the child to navigate social stigma. Adolescent anxiety about sexual experiences is buffered by having grown up in an environment of positivity around body, sexual, and gender diversity, and is explicitly normalized by teaching that all people have apprehensions about sex. 47 Anxieties about infertility could also be addressed in adolescence to build future resilience. 46 Perhaps, our adolescent even feels prepared to decide about interventions that are in the service of their own gender, sexual, and fertility goals, rather than in response to what they think is “normal.”
Shifting to a New Intersex/Variations of Sex Characteristics Clinical Care Paradigm
This hypothetical scenario illustrates how affirmation of sex diversity can actively reject reproduction of stigma. Within this model, decisions on sex and gender identity, and surgery are driven by the individual with I/VSC, rather than proxy decision-makers, which more fully respects the future autonomy of pediatric individuals with I/VSC and counters stigma.
Counterarguments and Anticipated Challenges
Critics might rightly point out the lack of research supporting this approach. Perhaps as an artifact of stigma, I/VSC care has primarily focused on early surgeries, although there is emerging work on implementation and outcomes of other approaches.21,48,49 We acknowledge this limitation, and suggest that absence of evidence is not evidence of absence of benefit.
Raising a child without a binary gender may be admittedly challenging in a society defined by binary gender roles and language. 50 However, many cultures have seen increasing acceptance of non-binary genders over time.51,52,53 In the United States, large segments of the population have generally become more accepting of steering children toward activities stereotypically not associated with their gender, 53 of LGBT (lesbian, gay, bisexual, transgender) individuals, 21 and of non-binary gender identities, 54 and there are rising levels of youth openly identifying as trans and non-binary. 21 In addition, the US federal government allows passports to carry an unspecified gender marker, 55 and many have argued for alternatives sex designations for state-level vital statistics.56 -58
Perhaps, the greatest challenge to this approach is stigma-related clinical knowledge and skills deficits. Most clinicians were taught to think of sex as binary, lack practice in communicating positively about bodily, sex, and gender differences, and learn little—if at all—about sex variation.18,59 -61 Medical education trains clinicians to prioritize patient deficits relative to an ideal of healthy and “normal.” In I/VSC care, this manifests as training in sex disorders, rather than sex variation, in which a perspective of pathological differences is reinforced by heteronormative and cisnormative biases. 2 However, unlearning societal norms and stigma can be done. Recent work in I/VSC care has explored surgical delay and non-binary gender/sex recommendations,48,49 aligning with medical trends toward affirmation of LGBTQ+ (lesbian, gay, bisexual, transgender, queer) experiences, 41 as well as rejection of race-based medicine. 62
To counter these challenges, advocates and clinicians must work together to support necessary shifts in mindset and culture toward humility and acceptance of the unknown.2,15,23 Clinicians can access extant resources developed by intersex activists to assist in this work.63 -65 Clinicians can take advantage of published narratives by individuals who have overcome stigma and shame66,67 and support efforts to expand the evidence base. Close collaboration between clinicians and individuals with I/VSC can uncover and challenge false assumptions, work that may also benefit any patient who has anxieties about their body. 68 For example, clinicians can challenge parental assumption that clitoromegaly is undesirable and makes one “less female” by affirming that genital variation is natural and that individuals who identify as female have a diversity of genitalia, while patient narratives can illustrate positive experiences with clitoromegaly. 3
Clinicians may question the ability of this approach to work cross-culturally, especially within communities that have more rigid constructions of or taboos around sex, gender, and sexuality. Clinicians may even wonder whether this approach is cultural imperialism. We observe that the wish to protect a child from harm is universal, and that culturally responsive strategies can help clinicians elicit a family’s concerns and develop a solution that suits the family’s culture. For example, a devoutly religious family may find reassurance in a narrative that their child’s body was created by God and is sacred.2,69 For families from cultures with rigid gender binaries, a binary, yet flexible gender of upbringing may be an adaptive solution.
Conclusion
To achieve the goals of promoting well-being and reducing the impact of stigma on health in I/VSC care, clinicians must embrace the complexity of sex diversity, even despite ones’ stigmatizing cultural and medical training. A model of care that affirms sex diversity and dismantles stigma is slowly emerging, but faces barriers. This model necessitates actively rejecting (1) dominant narratives that restrict the human body to sex binaries and (2) cisgender and heterosexual views of human identities and desires. In the clinic, this can be achieved by normalizing bodily, sexual, and gender diversity and avoiding assumptions. This approach respects the future autonomy of pediatric individuals with I/VSC and resists reproduction of internalized stigma and shame.
Author Contributions
CK conceptualized the piece with significant input from KBD. CK drafted the initial manuscript which was heavily revised by KBD. CK and KBD reviewed and revised the manuscript to achieve its final form.
Footnotes
Acknowledgements
The authors acknowledge the significant input from Lance Walhert in the early stages of conceptualizing and drafting this manuscript and thank him for his guidance and insights.
Data Availability
Data availability is not applicable to this article as no data sets were generated or analyzed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CK was supported by the NIH grant T32 DK063688 from the National Institute of Diabetes and Digestive and Kidney Diseases while working on this manuscript. The NIH had no role in the (1) design, (2) the collection, analysis, and interpretation of data, (3) the writing of the report, and (4) the decision to submit the paper for publication.