
Abstract
The Coronavirus 2019 (COVID-19) pandemic has significantly impacted the volume and types of trauma patients encountered. We performed a retrospective analysis of pediatric trauma patients <17 years old presenting within a large US health care system from 2019 to 2021. Demographics, trauma volume, injury severity, mechanism of injury, and outcomes were compared. A total of 16 966 patients, from 88 hospitals over 18 states, were included in our analysis. Pediatric traumas decreased from 2019 to 2020 and 2021. The injury severity scores (ISSs) increased from 2019 to 2020 and 2019 to 2021. Compared with 2019, more gun-related traumas occurred in both 2020 and 2021, whereas motor vehicle collisions decreased. There were additional changes in bicycle, assault, auto versus pedestrian (AVP), playground, and sports injuries. The COVID-19 pandemic has impacted the volume, injury severity, and mechanism of injury of the pediatric trauma population.
Keywords
Key Take-Aways
During the COVID-19 pandemic, overall pediatric trauma volume decreased.
During the COVID-19 pandemic, injury severity increased in pediatric traumas.
During the COVID-19 pandemic, mechanism of injury in pediatric traumas changed.
Introduction
Trauma is the leading cause of death in people ages 0 to 18 years, and roughly 1 in 6 children require treatment of traumatic injuries in the United States every year. 1 Compared with adults, children sustain higher rates of blunt trauma as opposed to penetrating trauma. 2 Motor vehicle–related injuries are the most common cause of death in the pediatric population. 1 Other common mechanisms of pediatric death due to trauma include drowning, house fires, homicides, and falls. 1 Guns are the number one cause of homicides in children over 1 year of age. Falls account for the majority of non–lethal traumatic injuries in children. 1 It is estimated that $14 billion in medical and parental work loss costs occurred due to traumatic pediatric deaths in 2021. 3 Because of this extreme toll on individual families and society, a better understanding behind the causes and outcomes of pediatric trauma is necessary.
The COVID-19 pandemic has impacted trauma demographics. In adults, prior studies have found that the overall number of traumas decreased and major mechanisms of injury changed as compared with prepandemic times. 4 There was a decrease in motor vehicle–related traumas while the overall severity of injury increased.4,5 Limited studies of pediatric trauma showed similar results, with decreased overall traumas, increased motor vehicle–related traumas, and increased injury severity score (ISS) as compared with the prepandemic years.6,7,8 Despite this, there is still a relative lack of data demonstrating the impact of the COVID-19 pandemic on pediatric trauma. In this study, we sought to analyze the detailed injury mechanisms and evaluate the longitudinal effects of the COVID-19 pandemic on pediatric trauma in the United States.
Methods
This study was approved by our health care system’s Ethics Committee and Institutional Review Board. Data were collected from 88 hospitals from January 2019 to December 2020 and 87 hospitals from January 2021 to December 2021 from a large US health care system database. We identified 22 902 patients, age ≤17 years, for inclusion in the study. Patients with missing data on mechanism of injury (n = 315), sex (n = 37), ISS (n = 46), race (n = 121), overlapping admissions (n = 3501), and age >18 years (n = 1938) were excluded. A total of 16 966 patients (with 17 040 trauma admissions) were therefore included for final analysis. We compared prepandemic (January 2019 to December 2019) and pandemic (January 2020 to December 2020 and January 2021 to December 2021) times for the purposes of the study. Data on age sex, race/ethnicity, ISS, length of stay (LOS), and discharge information were extracted. Mechanism of injury was classified based on the International Classification of Diseases, Tenth Edition (ICD-10) codes. Categorical variables were reported as percentages and continuous variables reported as mean values with standard deviation. Analysis of variance (ANOVA) tests were used for continuous variables, and chi-square tests were used for categorical variables. Pairwise comparison tested with Turkey’s post hoc test for ANOVA and Bonferroni for chi-square tests. P value threshold of P < .05 was used for 2-tailed tests. Data analysis was performed using SAS 9.4 and R version 4.0.2.
Results
A total of 17 040 trauma admissions for 16 966 patients were identified from 88 hospitals over 18 states (Figure 1). The total volume of pediatric traumas decreased when comparing 2019 with both 2020 and 2021 with 6185 patients in 2019, 5493 in 2020, and 5362 in 2021. There was no significant difference in age, sex, or race/ethnicity (Table 1). The ISS increased from 2019 to 2020 (6.28 ± 7.10 vs 6.73 ± 7.25, P < .05) and 2019 to 2021 (6.28 ± 7.10 vs 6.69 ± 6.83, P < .05). Even though ISS significantly increased, the LOS was not significantly different between the prepandemic and pandemic groups (Table 1). Mortality rates between the 3 years were also not significantly different (1.46% vs 1.71% vs 1.64%, P = .52). The number of patients discharged home decreased when comparing 2019 to both 2020 (66.19% vs 62.86%, P < .05) and 2021 (66.19% vs 61.77%; P < .05), with increased patients discharged to another hospital (19.00% vs 22.37%, P < .05 and 19.00% vs 24.60%, P < .05) (Table 1). Gun-related trauma increased from 2019 to 2020 (3.56% vs 5.37%, P < .05) and 2021 (3.56% vs 5.22%, P < .05) whereas the number of motor vehicle collisions (MVCs) was decreased in 2020 (16.99% vs 15.35%, P < .05) and 2021 (16.99% vs 14.49%, P < .05) (Table 1).
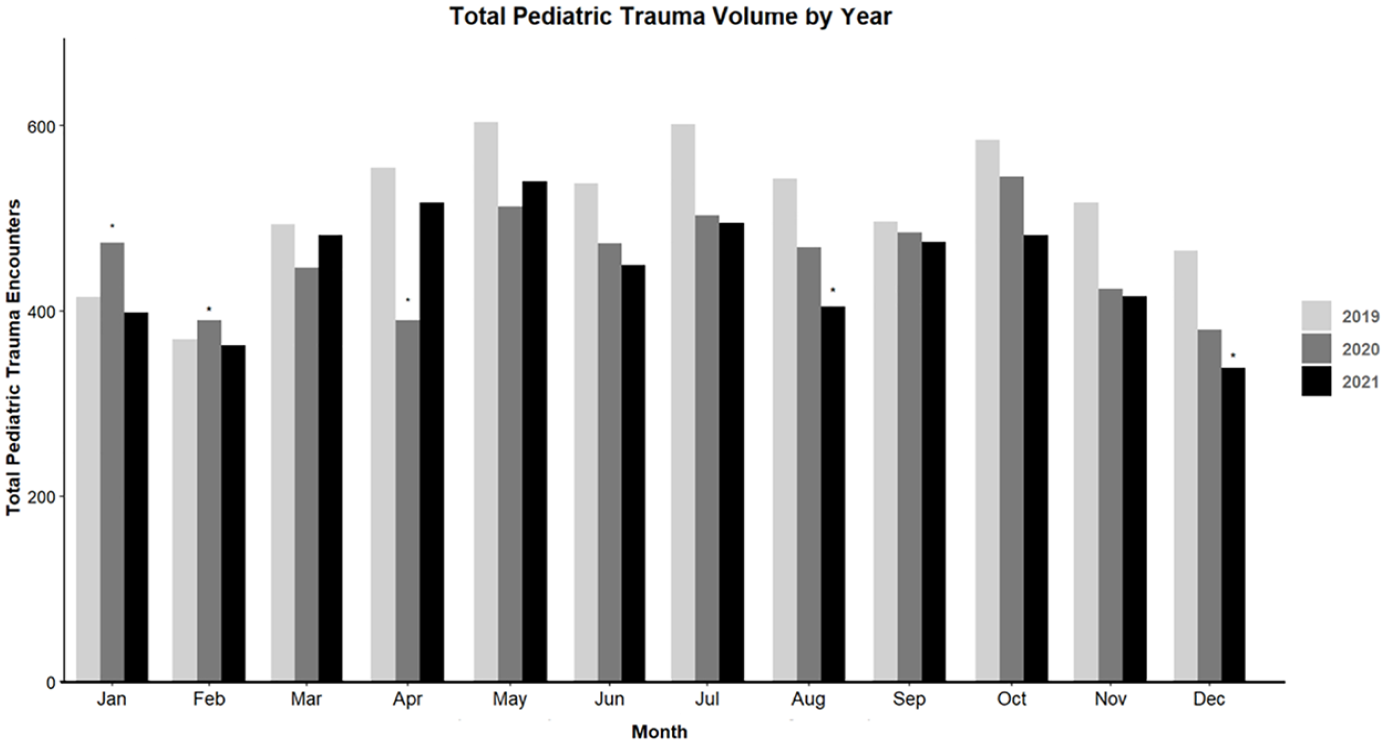
Trauma admissions by month comparing 2019, 2020, and 2021.
Pediatric Trauma Admissions, 2019 to 2021.
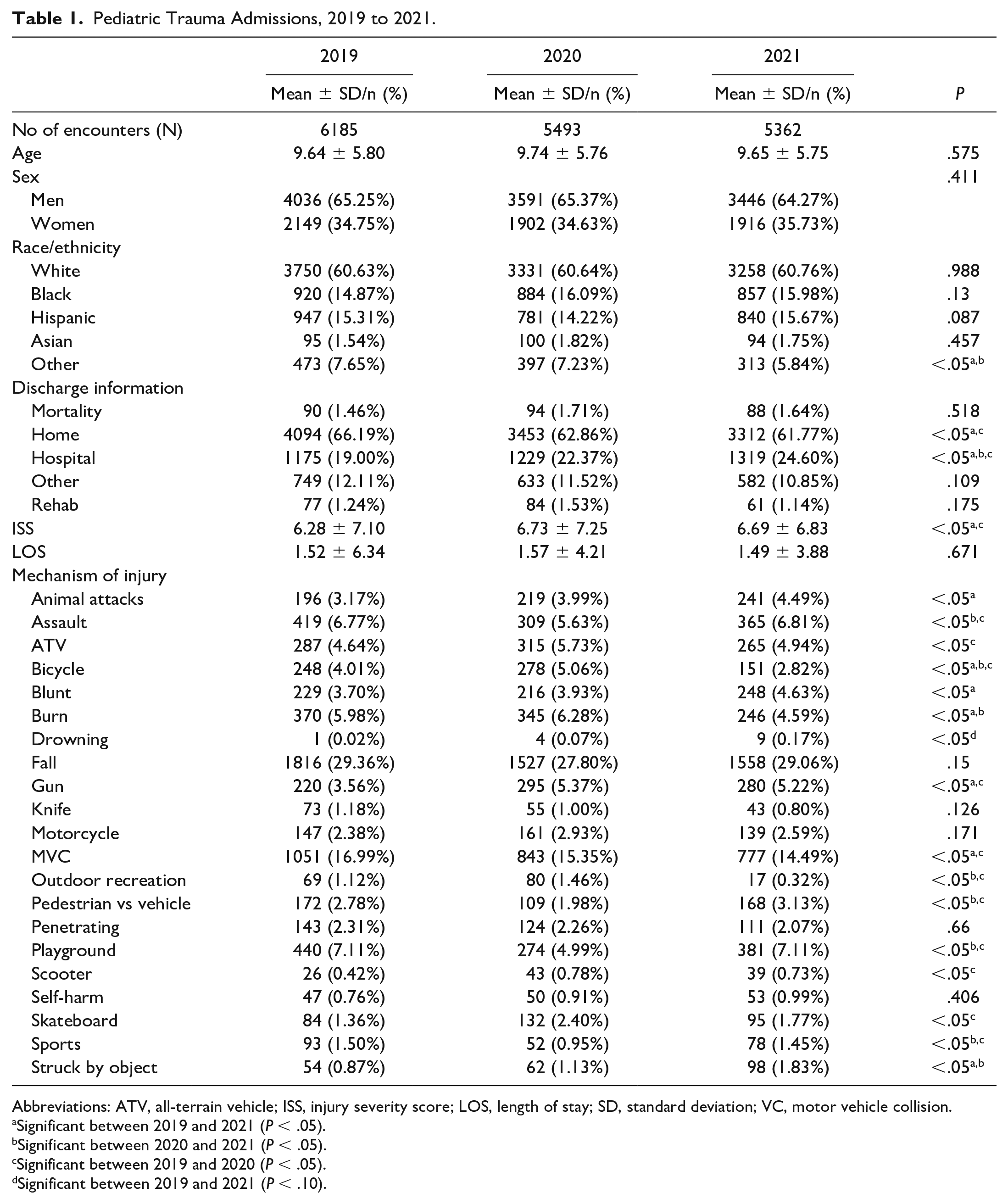
Abbreviations: ATV, all-terrain vehicle; ISS, injury severity score; LOS, length of stay; SD, standard deviation; VC, motor vehicle collision.
Significant between 2019 and 2021 (P < .05).
Significant between 2020 and 2021 (P < .05).
Significant between 2019 and 2020 (P < .05).
Significant between 2019 and 2021 (P < .10).
Bicycle-related traumas initially increased when comparing 2019 and 2020 (4.01% vs 5.06%, P < .05) but subsequently decreased between 2019 and 2021 (4.01% vs 2.82%, P < .05). Assaults, auto versus pedestrians (AVPs), playground-related traumas, and sports-related trauma all decreased between 2019 and 2020 and subsequently increased comparing 2020 and 2021, whereas there was no significant difference between 2019 and 2021. There was no significant difference in burn injuries from 2019 to 2020, yet a significant decrease from 2020 to 2021 (6.28% vs 4.59%, P < .05) was identified. A similar trend was seen for outdoor recreational traumas with no significant difference between 2019 and 2020, yet a significant decrease from 2020 to 2021 (1.46% vs 0.32%, P < .05). Regarding animal attacks, there was a significant increase between 2019 and 2021 (3.17% vs 4.49%, P < .05). Skateboard-related injuries increased from 2019 to 2020 (1.36% vs 2.40%, P < .05). Injuries related to children being struck by objects significantly increased between 2019 and 2021 vs 2020 and 2021 (0.87% vs 1.83 and 1.13% vs 1.83%, P < .05).
Discussion
The COVID-19 pandemic had a significant impact on society in general, and on trauma specifically in volume, injury severity, and injury mechanisms. The overall volume of pediatric trauma activations and admissions decreased in both 2020 and 2021 as compared with 2019 in our multi-institutional study. Sanford et al 6 found a decrease in the number of pediatric trauma encounters in 2020 compared with the mean number of encounters in previous years (460 vs 392). Bessoff et al 8 found similar results with roughly a 13% reduction in pediatric trauma volume in 2020 compared with the previous 3 years. One study stood alone in that they found no difference in pediatric traumas during the pandemic year compared with years prior, which could largely be due to its region-specific design. 9 This downward trend seen in our and other studies is likely partially attributable to the overall decrease in travel, both locally and nationally, in 2020 and 2021. 10 Nationwide stay-at-home orders and school closures were enacted in the early months of 2020. Overall non–COVID-related hospital admissions were previously reported as decreased in 2020 compared with previous years, which could be attributed to the fear of hospitals and the potential contraction of COVID pneumonia.11,12 This might help to partially explain the decreased number of trauma admissions, leading to a potential delay in care of pediatric patients.
Although the number of trauma admissions decreased in the pandemic year, there was also an unexpected increase in the severity of injuries. In our study, the ISS increased significantly between 2019 and 2020 and between 2019 and 2021. This finding is similarly reflected in other studies. In evaluating injury severity during the pandemic, Wells et al 13 divided 2020 into 3 periods for comparison: early, middle, and late, with severe injury defined as an ISS >16. Their study found an increase in severe injury in each period, as compared with the previous 3 years. 13 Another study, which categorized severe injury as ISS ≥25, found an increased median ISS after implementation of the stay-at-home orders. 8 Conversely, a review, with over 3000 patients, found that the average ISS was not significantly different comparing 2018 and 2019 to 2020. 14 Even though ISS was increased in our study, we did not identify a significant difference in mortality, which is consistent with previous pediatric trauma studies.6,14,15 Despite differences between prior studies in how severe injury was defined, our study was consistent with the overall finding that ISS of pediatric patients treated during the pandemic was higher compared with the prepandemic patients.
During the COVID-19 pandemic, the mechanisms of injury leading to trauma changed significantly in the pediatric population in our study. Although motor vehicle trauma remains the leading cause of death in the United States, our study found that the incidence of MVCs decreased during the COVID-19 pandemic from 16.9% in 2019 to 15.4% in 2020 and 14.5% in 2021. We also saw an initial decrease in AVP injuries from 2.8% in 2019 to 1.9% in 2020; however, this increased in 2021 back to 3.1%. Sanford et al 6 similarly described a decrease from an average of 53.2 MVCs per year to 27 when comparing 2015 to 2019 with 2020; similarly, AVP decreased from 50 per year to 14 per year. Another study at a level 1 Pediatric Trauma Center found a decrease in MVCs from 2017 to 2019 compared with 2020. 16 Contrary to our findings, 1 pediatric multicenter study found no change in MVCs from 2019 to 2020 and a decrease in AVPs, whereas another pediatric multicenter study in the same region actually reported an increase in MVCs.9,17 These differences could be attributed to the particular region in which the studies occurred. In general, the reported decreases in trauma due to MVCs and AVP during the pandemic are likely due to stay-at-home orders, which in turn made for less vehicle traffic and therefore fewer accidents. 18
Guns are the number one cause of homicide in children greater than 1 year of age in the United States. 1 Multiple studies have demonstrated an increase in gun-related traumas during the COVID-19 pandemic.8,10,9 Our study showed an increase in gun-related trauma in both 2020 (5.4%) and 2021 (5.2%) as compared with 2019 (3.6%). A multistate study found an increase in pediatric gunshot wounds from 1.8% to 3.3% from the 3 years prior to the pandemic compared with during the pandemic. 8 The authors of that article suggested this was due to an increase in community violence regarding the stay-at-home orders, especially in disadvantaged communities. 8 Chaudhari et al 9 demonstrated an increase in pediatric gun–related injuries from 7.5% to 10.5% in the pandemic era. A Colorado study specifically looking at gun-related traumas in pediatrics found an increase from an average of 5.18 per 100 trauma encounters in 2018 and 2019 to 8.61 per 100 trauma encounters in 2020. 15 On the contrary, Yeates et al 17 found no difference in pediatric gun–related traumas between 2019 and 2020. Gun violence remains a significant issue in the United States. Although prior data are somewhat mixed on the effect of the COVID-19 pandemic on the incidence of gun violence, our study found that the overall incidence was increased. This could certainly be an area of further study regarding violence prevention due to gun-related trauma, particularly in areas that demonstrated increased incidence as a result of the pandemic.
School closures along with closures of public playgrounds may have led children to activities that did not require social distancing, such as outdoor recreation and bicycling. Our study found a decrease in playground-related injuries from 2019 to 2020, with a subsequent return to prepandemic levels in 2021, likely due to pandemic-related closures of playgrounds and other public spaces in 2020 with subsequent re-opening in 2021. We also found an increase in bicycle-related injuries in 2020 as compared with 2019 with an unexpected sharp decline in 2021. Multiple other studies have demonstrated similar trends with decreased playground-related injuries and increased bicycle-related injuries during the pandemic.6,19 Malige et al 20 found results coinciding with previous evidence demonstrating a decrease in injuries occurring at sporting areas, parks, and pools. Even though that study did not explicitly incorporate playgrounds into their findings, it showed changing child behavior during the pandemic leading to new patterns of injury. 20 Further knowledge relating to the particular mechanisms of injury could help to potentially prevent injuries in the vulnerable pediatric population during future societal events.
We are limited by the retrospective nature of this study. We lack certain granularity regarding injury mechanisms and the specific injuries sustained. Although this was a multicenter study, our results could potentially be biased based on the particular locations included, as some states were affected differently throughout the COVID-19 pandemic with varying public mandates on lockdowns as well as different disease burdens. Furthermore, despite the fact that this is a multicenter study, it may not be representative of the pediatric population as a whole in the United States.
Conclusions
The COVID-19 pandemic resulted in a decrease in overall pediatric trauma volume across the United States. Despite this decrease in volume, there was an increase in injury severity in the pediatric population prepandemic and postpandemic. We also identified significant differences in the injury mechanisms prepandemic and postpandemic, with decreased numbers of MVCs and a troubling increase in gun-related injuries during the pandemic. Further studies are needed to fully understand the pandemic’s impact on pediatric trauma as well as potential injury prevention mechanisms if we were to find ourselves in a similar situation again in the future.
Author Contributions
All authors conceptualized and designed the study along with collection and analysis of data. The authors also drafted, reviewed, and revised the initial manuscript. All authors approved the final manuscript and are agreeable to be accountable for all portions of the work.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported (in whole or in part) by the HCA Healthcare and/or an HCA Healthcare–affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Ethical Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of HCA (no. 4291) on February 26, 2020 with an exemption from informed consent. No specific consent is needed for statistical analyses of aggregated de-identified data. For this study, the raw data were extracted, and patients’ identities, including names, screening IDs, patient IDs, and mobile phone numbers, were de-identified.