
Abstract
It is unclear if socioeconomic status (SES) factors influence severity of illness of patients hospitalized with bronchiolitis. This study was conducted to identify SES factors including the Center for Disease Control and Prevention’s Social Vulnerability Composite Index (SVI), estimated income, proportion of minority, proportion of living below poverty, insurance status, and number of household members associated with length of stay (LOS) and intensive care unit admission. Infants hospitalized at a tertiary care urban center for bronchiolitis were identified using International Classification of Diseases codes. Federal information processing system codes were identified from home address and paired with SVI and 2018 census tract. Other measures of SES were obtained from the Federal Financial Institutions Examination Council. Number of household members, insurance, age, sex, and history of prematurity were recorded from patient chart. Length of stay was modeled with mixed effects negative binomial regression and pediatric intensive care unit (PICU) admission with mixed effects logistic regression with random intercept at the census tract and adjustment for clinical factors. A total of 417 infants had median age of 144 days (interquartile range (IQR): 61, 357) and 136 (33%) were born premature. Median LOS was 62 hours (24, 136) with 97 (23%) patients admitted to the PICU. Median household members were 4 (4, 5). For each increase in household member, there was 7% increase in LOS (incidence rate ratio 1.07, 95% confidence interval: 1-1.14, P = .038). Social Vulnerability Composite Index, subcategories, insurance status, estimated income, percent of minority, and percent of poverty did not show any associations with length of hospitalization or PICU admission. Increasing number of household members may be associated with increased bronchiolitis hospital LOS. We find no associations with other SES measures.
Introduction
Bronchiolitis is the most common reason for hospital admission for infants with over 100 000 hospitalizations each year in the United States.1,2 There are known clinical factors such as young age and history of prematurity that are associated with increased severity of illness requiring increased length of hospitalization or admission to the pediatric intensive care unit (PICU).3-6 It is also thought that non-clinical factors such as socioeconomic status (SES) may also influence bronchiolitis illness. Previous studies have shown that patients from lower socioeconomic conditions were more likely to present to the emergency room and be hospitalized.7-10 However, it is unclear once hospitalized whether patients from lower SES also have more severe illnesses compared to other hospitalized infants. This question is important as predicting the course of illness in bronchiolitis is challenging. Some patients are hospitalized for observation and nasal suctioning, while some infants are intubated and hospitalized for mechanical ventilation. Identifying factors associated with severe illness can help with efficient triaging, resource management, and improved clinical care.
There are numerous measures of SES utilized in pediatric health research. 11 Types of SES range widely from education level, income status, and insurance status. Measurements of SES can be from Zone Improvement Plan (ZIP) code level, census tract level, block group level, or individual level. We aim to evaluate various measures of SES using individual-level metrics, number of household members, and insurance status, as well as a variety of census tract level factors using the Center for Disease Control and Prevention’s (CDC) Social Vulnerability Composite Index (SVI), estimated household income, proportion of minority living in census tract, proportion of living below poverty in tract. We aim to find any associations with these SES factors with hospital severity outcomes of increased length of stay (LOS) and PICU admission. We hypothesize that infants from lower SES areas will have increased severity outcomes as they may have increased barriers in seeking timely care or evaluation.
Methods
Population and Measures of SES
All infants less than 23 months old hospitalized with a primary diagnosis of bronchiolitis over a 2-year period from 2015 to 2016 at an urban tertiary care children’s hospital were identified using International Classification of Diseases 9 and 10 diagnosis codes (466.x, J21.x). Patient’s age, sex, and history of prematurity were extracted from the electronic medical record (EMR).
Patient’s home address was used to identify federal information processing system codes that corresponded to the patient’s census tract. The CDC’s SVI was obtained for each patient’s 2018 census tract. The SVI is a composite index made up of 15 social factors grouped into 4 related themes—SES, household composition and disability, minority status and language, and housing type and transportation. 12 The composite score ranges from 0 to 100 with higher numbers representing a more vulnerable population. Additional measures of SES were obtained from the Federal Financial Institutions Examination Council (FFIEC) Web site including estimated median income, proportion of minority living in tract, and proportion of living below poverty in tract. 13 The FFIEC defines tract percent minority as the percentage of the tract’s total population minus the white alone population divided by the total tract population. The number of household members was extracted from the admission history and physical documentation. Insurance status was extracted from the EMR and was categorized as public, private, and self-pay. Public insurance was defined as any insurance that fell within the Medicaid financial class. To facilitate interpretation and given the low number of self-pay patients, regression models dichotomized insurance to public + self-pay versus private.
Outcomes and Analysis
Descriptive statistics were used to describe patient characteristics with median (interquartile range) and number (percentage) used for continuous and categorical variables, respectively. Length of hospital stay was measured in hours and defined as the duration of time from arrival to the hospital room to departure from the hospital room as recorded in the EMR. Length of stay was treated as a count and analyzed using a negative binomial regression adjusted for age, sex, and history of prematurity. Pediatric intensive care unit admission was defined as utilization of a PICU bed at any point during the patient’s admission. This was treated as a binary outcome and analyzed using multiple logistic regression adjusting for age, sex, and history of prematurity. Each measure of SES was analyzed independently from each other given the high correlation between measures (Supplement 1). Initially, penalized ridge regression was used to identify top predictors to include in multivariate regression; however, ultimately a simplified regression model with one SES predictor was used after finding insignificant differences between the 2 models. All regression models used mixed effects with random intercept at the census tract to account for variation in outcomes due to unmeasured census tract characteristics.
In exploratory analysis in describing the relationship between household size and severity outcomes, a household with a large number of members was defined as a binary variable for number of members greater than the 75th percentile of our cohort. Differences between groups in level of respiratory support were analyzed using independent proportions tests. Independent sample t-test was used to analyze differences in lag time to discharge (defined as the duration of time from when the discharge order was placed and when the patient was recorded as discharged from the EMR). Spearman correlation coefficients were calculated to compare relationships of household size with other measures of SES.
P values less than .05 were considered significant, and all analyses were conducted using Stata v15. Geospatial mapping was performed using qGIS Version 3.16.14. The TIGER/Line Shapefile released in 2018 was used which corresponded to the 2010 census. The study was approved by the local institutional review board with waiver of individual consent.
Results
A total of 417 infants from 297 unique census tracts were identified. The median age was approximately 5 months, with 56% male and 33% with history of premature birth. The median number of people living in the household was 4 (4, 5). Unadjusted outcomes included a median LOS of 62 hours, and 23% of our cohort were admitted to the PICU (Table 1).
Patient Demographic and Unadjusted Outcome Descriptions.
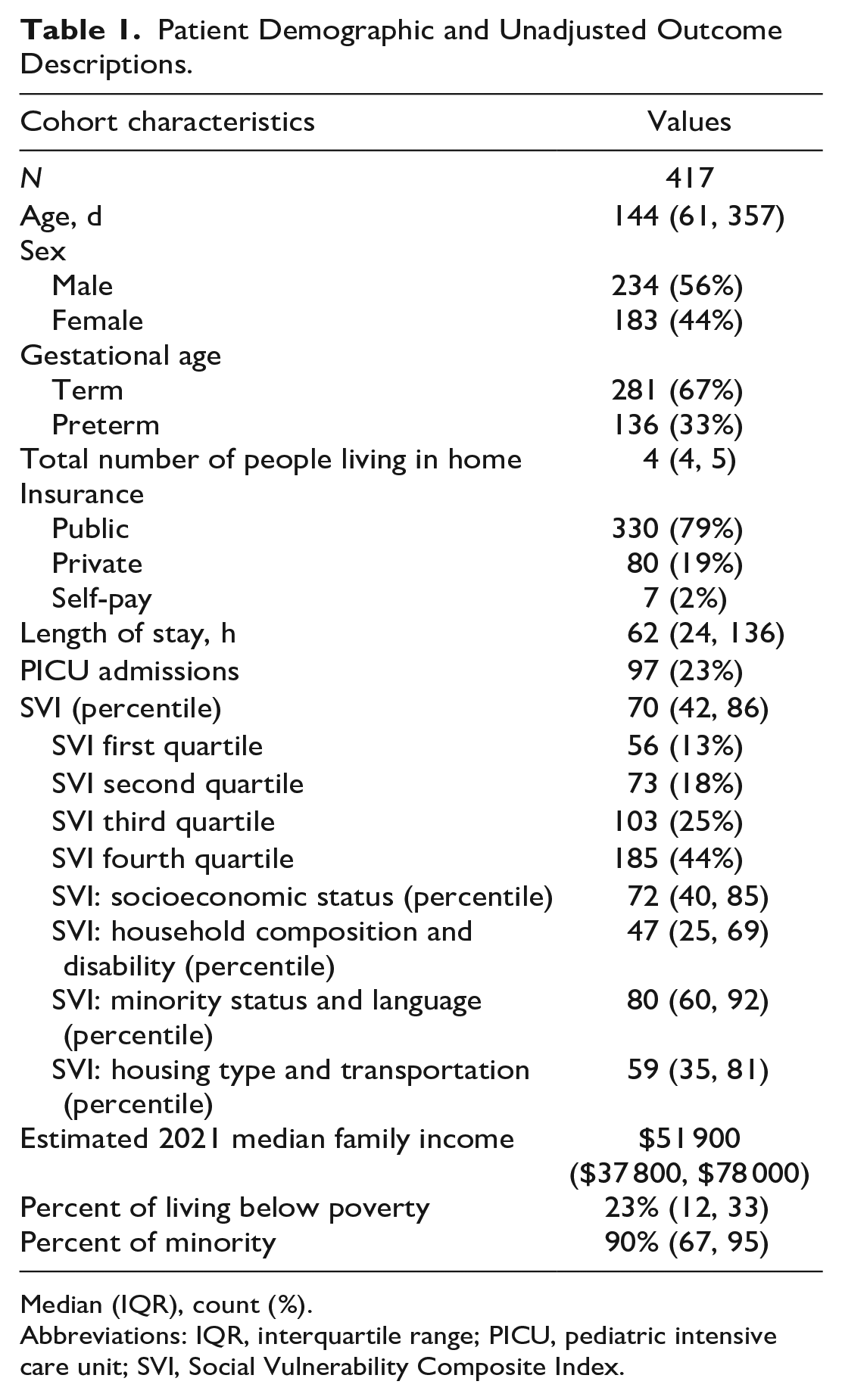
Median (IQR), count (%).
Abbreviations: IQR, interquartile range; PICU, pediatric intensive care unit; SVI, Social Vulnerability Composite Index.
Our cohort had a SVI score of 70 (42, 86). There was a statistically significant difference in cohort proportion between SVI quartiles. Patients from census tracts of the least vulnerable quartile (first) made up 13% of our hospitalized population, whereas patients from census tracts of the most vulnerable quartile (fourth) made up 44% of our cohort. This is visualized graphically in Figure 1 which displays the census tracts color coded by SVI quartiles with cross hatches representing census tracts of patients from our cohort. Descriptions of other SES factors are listed in Table 1.
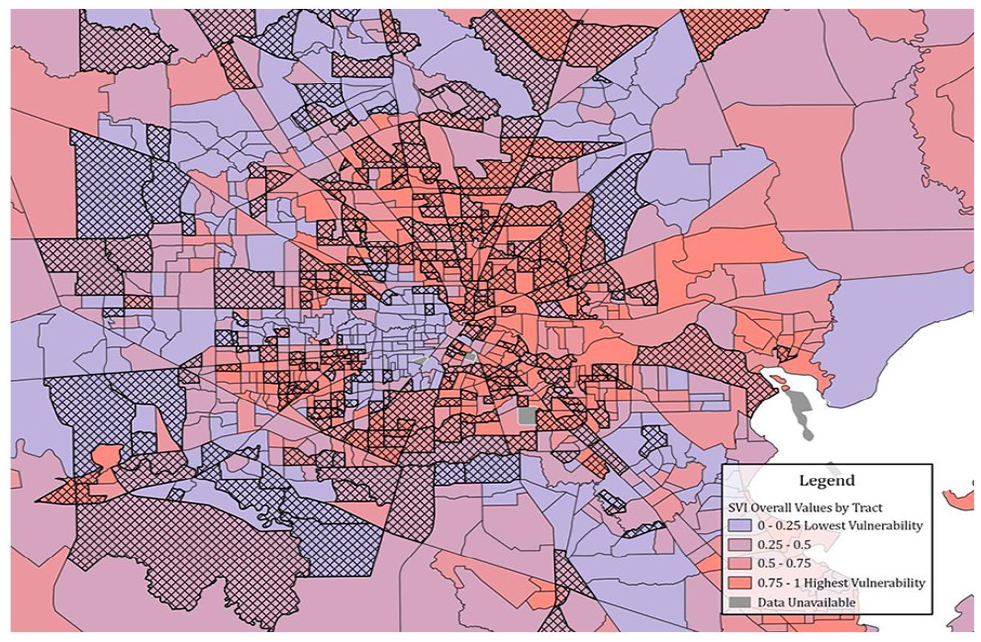
Map of census tracts of the greater Houston area color coded by SVI quartile. Cross hatches represent census tracts with patients in our cohort.
When looking at SES factors associated with increased LOS, we found a significant association with number of household members. Each additional member in the household was associated with a 7% increase in LOS. Other markers of SES were not associated with hospital LOS (Table 2). When looking at associations with PICU admission, we find that none of the SES factors, including household members, were associated with PICU admission (Table 3). The intraclass correlation at the census tract level was mildly positive: 0.24 for the LOS model and 0.32 for the PICU model.
Associations of Socioeconomic Factors on Hospital Length of Stay (Hours).
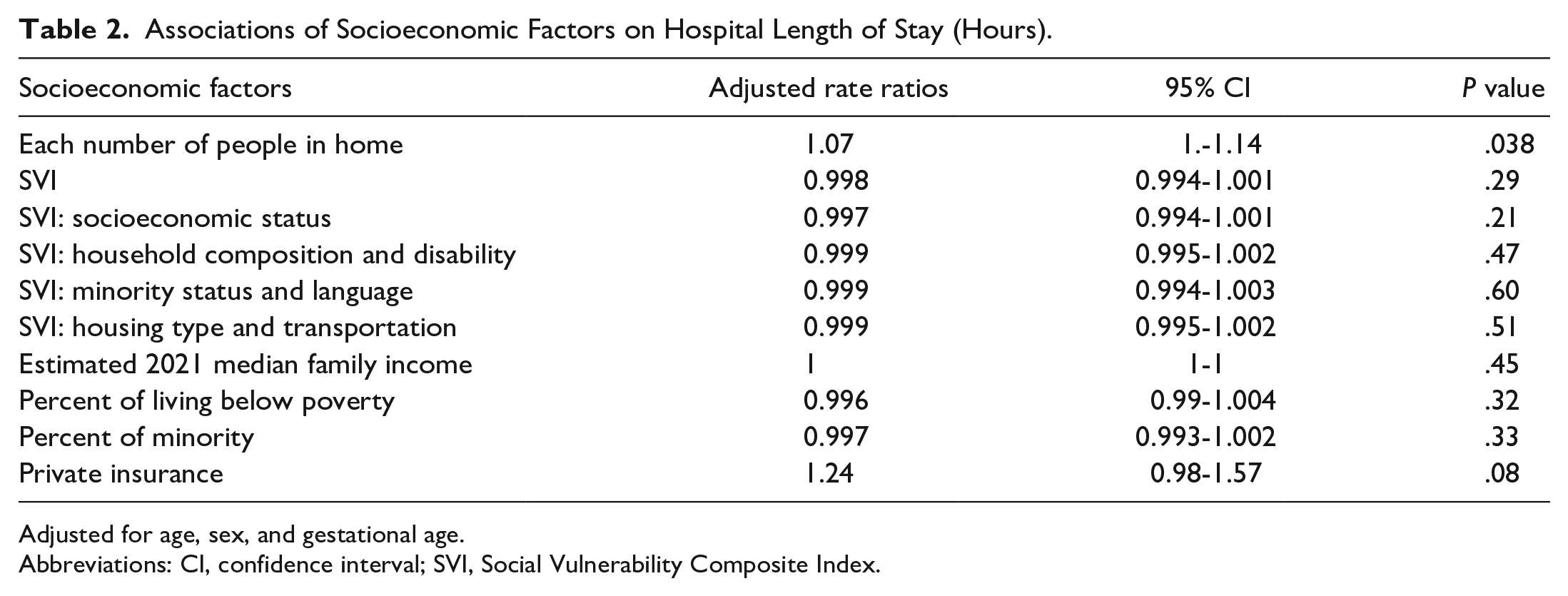
Adjusted for age, sex, and gestational age.
Abbreviations: CI, confidence interval; SVI, Social Vulnerability Composite Index.
Association of Socioeconomic Factors on PICU Admission.
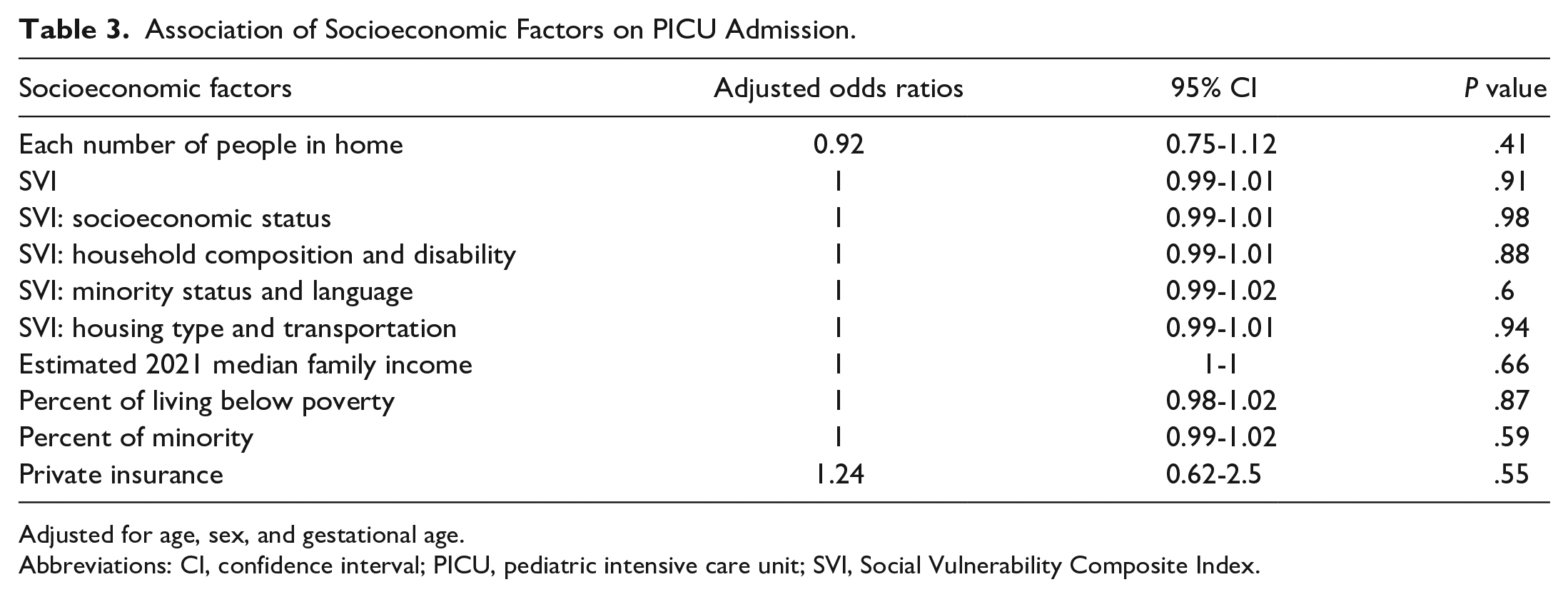
Adjusted for age, sex, and gestational age.
Abbreviations: CI, confidence interval; PICU, pediatric intensive care unit; SVI, Social Vulnerability Composite Index.
To further explore the relationship between large households and length of hospitalization, we looked at differences in levels of respiratory support between the 2 groups. While not statistically significant, we find greater proportions of more intensive therapies such as mechanical ventilation, continuous positive airway pressure, and high-flow nasal cannula in patients from large households, and greater proportions of patients on room air, or simple nasal cannula from other households (Table 4).
Highest Level of Respiratory Support Based on Household Size.
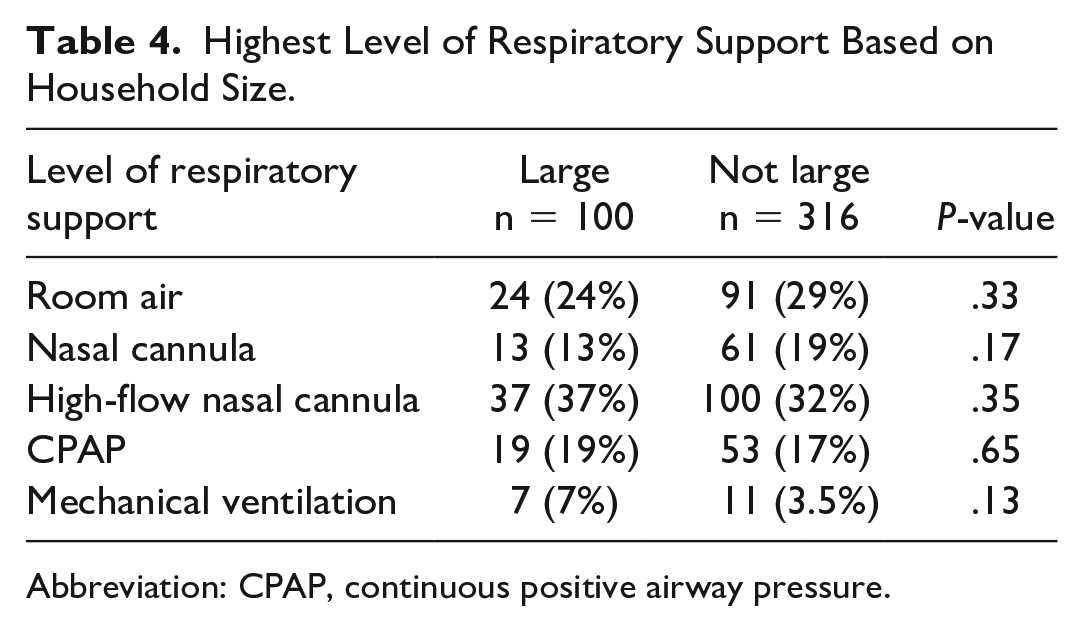
Abbreviation: CPAP, continuous positive airway pressure.
We also evaluated if there were any differences in delays in discharge that may have artificially inflated the differences in LOSs. We find no differences in lag time to discharge. Patients from large households had a lag time of 1.87 hours (standard deviation (SD) 1.2), and patients from other households had a lag time of 1.84 hours (SD 1.2).
We also find a lack of correlation between household size and other measures of SES with all Spearman’s coefficients ranging between −0.05 and 0.14 (Supplement 1).
Discussion
We find an association with number of household members with increased lengths of hospitalization in infants with bronchiolitis after adjusting for age, sex, and history of prematurity. Other measures of SES including the SVI, its subcategories, estimated median income, insurance status, proportion of minority in census tract, and proportion of living below poverty level in census tract were not associated with length of hospitalization of PICU admission.
Previous studies have shown higher rates of hospitalizations and emergency room visits for patients with bronchiolitis from low SES tracts compared to high SES tracts.7-9 Our study also supports this finding with 44% of our hospitalized cohort coming from the most vulnerable quartile compared to only 13% of our cohort from the least vulnerable quartile. While there is consistent evidence that patients from lower SES environments are more likely to visit the emergency room and subsequently admitted, there is conflicting evidence on how SES relates to the severity of the bronchiolitis illness. In one prospective multicenter cohort study (Multicenter Airway Research Collaboration, MARC), estimated median income from patient ZIP code was not associated with PICU admission. 14 In a subsequent prospective study of the same MARC network, estimated median household income from ZIP code was most strongly associated with PICU admission. Perhaps counterintuitively, patients with high estimated median household income had twice the odds of an intensive care unit (ICU) admission compared to patients in the intermediate estimated household income (adjusted odds ratio: 2.05, 95% CI: 1.19-3.53). Other factors of SES such as parent-reported household income, number of adult and children in household, and insurance type were not associated with PICU admission. 15 In another study with a broader population of respiratory failure encompassing patients 2 weeks to 17 years old presenting to the ICU, estimated median income from a census tract level was not associated with illness severity upon PICU admission. 11 In our study we find no association with estimated income with PICU admission or hospital LOS.
Our study differs from previous studies evaluating the influence of SES on bronchiolitis severity in that we tried to capture a comprehensive list of socioeconomic factors using the CDC’s SVI. Socioeconomic status is a complex entity with multiple factors influencing a patient’s overall vulnerability. While income is an important factor that relates to many other aspects of SES, specifically evaluating different components such as household composition, minority status, and housing type and transportation can help tease out driving factors for increased illness severity. Regardless, our study somewhat surprisingly showed no associations with SVI or any of its components with bronchiolitis severity.
We found infants from larger households to be associated with increased length of hospitalization. While large number of people living in a household would intuitively increase risk of transmission of a viral illness, 16 it is unclear how it would potentially lead to increased severity of illness. Recent studies with COVID-19 have found similar associations with crowding and severe illness.17-19 In a prospective cohort of COVID cases and their household members, households with secondary transmission had index cases with a median viral load that was 1.4 log10 higher than those households without secondary transmission. 20 Perhaps infants in larger households who likely are getting infected through secondary household transmission are having higher viral loads leading to higher severity compared to infants becoming infected from non-household transmission. An alternate hypothesis may be that infants from larger households have greater passive immunity due to greater exposure to viral illness from siblings and household members in utero and after birth. Therefore, a viral illness that ultimately hospitalizes this infant may be more severe than one that hospitalizes a more naïve infant immune system. Further research is needed to solidify the relationship between the number of household members and illness severity.
It is important to note that the number of household members may not correlate directly with SES. For example, a 5-member household with 4 working adults and 1 child versus a single parent with 4 children likely have significant differences in SES, yet the same number of household members. In our data collection we did not collect specifics such as age of the members, birth order of the patient, or presence of multifamily units which would have been informative. Furthermore, it may be that our results of increased severity of illness with larger household numbers are independent of actual SES. This is supported by the lack of correlation found between household size and other established measures of SES like the SVI and estimated income, in addition to the lack of associations found between all other SES measures with LOS and PICU admission.
Our results should be interpreted in the context of some of our limitations. All of our measures of SES excluding number of household members were from a census tract level. While census tracts provide more uniform description of a population than ZIP codes, it is still an estimation of a patient’s SES rather than truly reflective of an individual’s SES. Furthermore, our study sample had a low number of patients per census tract which makes distinguishing census tract effects from individual patient effects difficult. We also had inconsistencies in the data for census years. Our cohort was obtained from the years 2015 to 2016, while SVI data were pulled from the 2018 census tract, and shapefiles corresponded to the 2010 census. We do not believe that this affected our analysis and results in a meaningful way. In addition, while we would have liked to include patient race and ethnicity data into our analysis, we found that the documentation in the EMR for this field was inconsistent, inaccurate, and unreliable. While both the SVI minority status and language subgroup and the proportion of minority of a census tract indirectly account for this, our low number of patient per census tract makes it to correlate the true proportion of race and ethnicity without the patient-level data. Further research on individual-level socioeconomic factors and bronchiolitis severity is needed.
We also included length of hospitalization as an important severity measure for bronchiolitis to consider along with PICU admission which previous studies in this area have not. While need for ICU-level care is an important measure of severity, it may not fully capture significant severity of illness. Need for PICU admission can be clinician dependent and the level of care provided in an ICU is institution dependent. At our institution, for instance, high-flow nasal cannula is an intervention that can be started outside the ICU while for other hospitals this is a therapy given in the ICU. By utilizing length of hospitalization and assuming that more severe illness leads to longer hospitalizations, we are able to more completely capture severe bronchiolitis illness. However, we do realize that LOS is also limited in that decision to discharge may also be clinician dependent, and that LOS may be influenced by other factors outside of inherent bronchiolitis illness. While we did look at lag times to discharge, it may not reflect delays in actual placement of the discharge order by the clinician.
Finally, as a single-center study in an urban environment our findings may not be generalizable to all settings. As mentioned previously our outcomes of PICU admission and LOS may be reflective of our own clinical practices. Furthermore, the distribution of patients’ SES admitted to our hospital and thus our cohort may be reflective of our hospital’s capture area rather than reflective of the true distribution of patients’ SES requiring hospital admission for bronchiolitis.
Conclusion
In this retrospective cohort of bronchiolitis patients admitted to our hospital, only the number of household members was associated with increased LOS and prolonged hospitalization. No other measures of SES from a census tract level were related to LOS or PICU admission. Further studies are needed that evaluate the impact of individual-level socioeconomic factors and their association with severe bronchiolitis illness.
Author Contributions
RP-C: Conceptualized and designed the study; collected data; analyzed the data; drafted the initial manuscript; and reviewed and revised the manuscript.
ZH: Collected the data; analyzed the data; and critically reviewed and revised the manuscript.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of work.
Supplemental Material
sj-docx-1-cpj-10.1177_00099228231200393 – Supplemental material for Association of Socioeconomic Factors and Severity of Bronchiolitis Hospitalizations
Supplemental material, sj-docx-1-cpj-10.1177_00099228231200393 for Association of Socioeconomic Factors and Severity of Bronchiolitis Hospitalizations by Raymond Parlar-Chun and Zoabe Hafeez in Clinical Pediatrics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Study was approved by the UT Houston IRB—Approval number HSC-MS-18-0867.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.