
Abstract
Objective
This study was performed to evaluate the effect of care bundles on the prevention of central venous catheter-related bloodstream infection (CRBSI) and improvement of patients’ experience.
Methods
In total, 212 patients with central venous catheter insertions were enrolled in this study. All patients were matched by sex, age, Acute Physiology and Chronic Health Evaluation II score, body mass index, department, and catheter insertion site and were randomly divided into case and control groups (n = 106 each). The control group was given conventional care, and the case group was given care bundles including nurse education, hand hygiene, maximal sterile barrier precautions, bedside observation, and evaluation. The anxiety scores, hospitalization days, CRBSI rate, and degree of satisfaction with hospitalization were compared between the two groups.
Results
The patients’ mean self-rating anxiety scale score and self-rating depression scale score after nursing intervention were significantly lower in the case group than in the control group. The mean number of hospitalization days and CRBSI rate were significantly lower and the satisfaction rate was significantly higher in the case group.
Conclusion
Care bundles are essential for preventing CRBSI. They can improve patients’ psychological state and hospitalization satisfaction and reduce the hospitalization days.
Keywords
Introduction
Catheter technology is becoming more complex with the development of medical technology. Various catheters have emerged as important tools with which to carry out hemodynamic monitoring, infusion, parenteral nutrition support, and other procedures. Central venous catheters (CVCs) are an important development in catheter technology and are widely used in intensive care units (ICUs) and for hemodialysis, parenteral nutrition support, renal replacement therapy, chemotherapy, interventional therapy, and various types of invasive monitoring.1,2 Despite the potential benefits of CVCs, these devices have a high risk of catheter-related complications including mechanical injury, infection, and thrombosis. 3 Among these complications, bloodstream infection [known as catheter-related bloodstream infection (CRBSI)] is a very important complication that can prolong the hospital stay and increase hospitalization costs and mortality.1,4,5 No nationwide survey on the prevalence of CRBSI in China has been performed. The incidence of CRBSI varies among different hospitals. Xinman et al. 6 reported that the incidence of CRBSI decreased from 7.9 per 1000 catheter days in 2012 to 6.4 per 1000 catheter days in 2015. In other studies, the incidence of CRBSI ranged from 4.52 to 8.10 per 1000 catheter days.7–10 However, Han et al. 11 found that the incidence of CRBSI was lower and that the incidence of central line-associated bloodstream infection (CLABSI) was 2.84 per 1000 catheter days in ICUs and 0.82 per 1000 catheter days in non-ICUs. Therefore, the importance of catheter management has been emphasized throughout the literature.
Additionally, several studies have shown that when patients are physically sick and treated in a hospital, they are more prone to develop anxiety and depression due to the direct or indirect stress from their illness.12–15 Therefore, hospitalized patients who undergo CVC insertion are likely to have an anxiety disorder or depression. Care bundles are likely to improve the psychological state of patients with CVCs.
This study was performed to evaluate the effect of care bundles on prevention of CRBSI and improvement of the patient experience among patients with CVCs.
Patients and Methods
Patients
Patients who underwent new CVC insertions in the ICU, general surgery ward, and emergency ward from June 2017 to May 2019 were enrolled in this study. The inclusion criteria were CVC insertion for infusion, parenteral nutrition support, or hemodynamic monitoring; the absence of infection; and a conscious state with agreement with the study protocol. The exclusion criteria were long-term use of antibiotics, glucocorticoids, and immunosuppressants and placement of a Swan–Ganz catheter. All patients were matched by sex, age, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, body mass index (BMI), department, and catheter insertion site. They were randomly divided into a case group and control group.
Methods
Patients with CVCs in the control group were given conventional nursing care during their hospital stay. They received the same treatment as the patients in the control group in addition to care bundles. The catheter management measures for patients with CVCs in the case and control groups are shown in Table 1.
Catheter management measures for patients with CVCs.
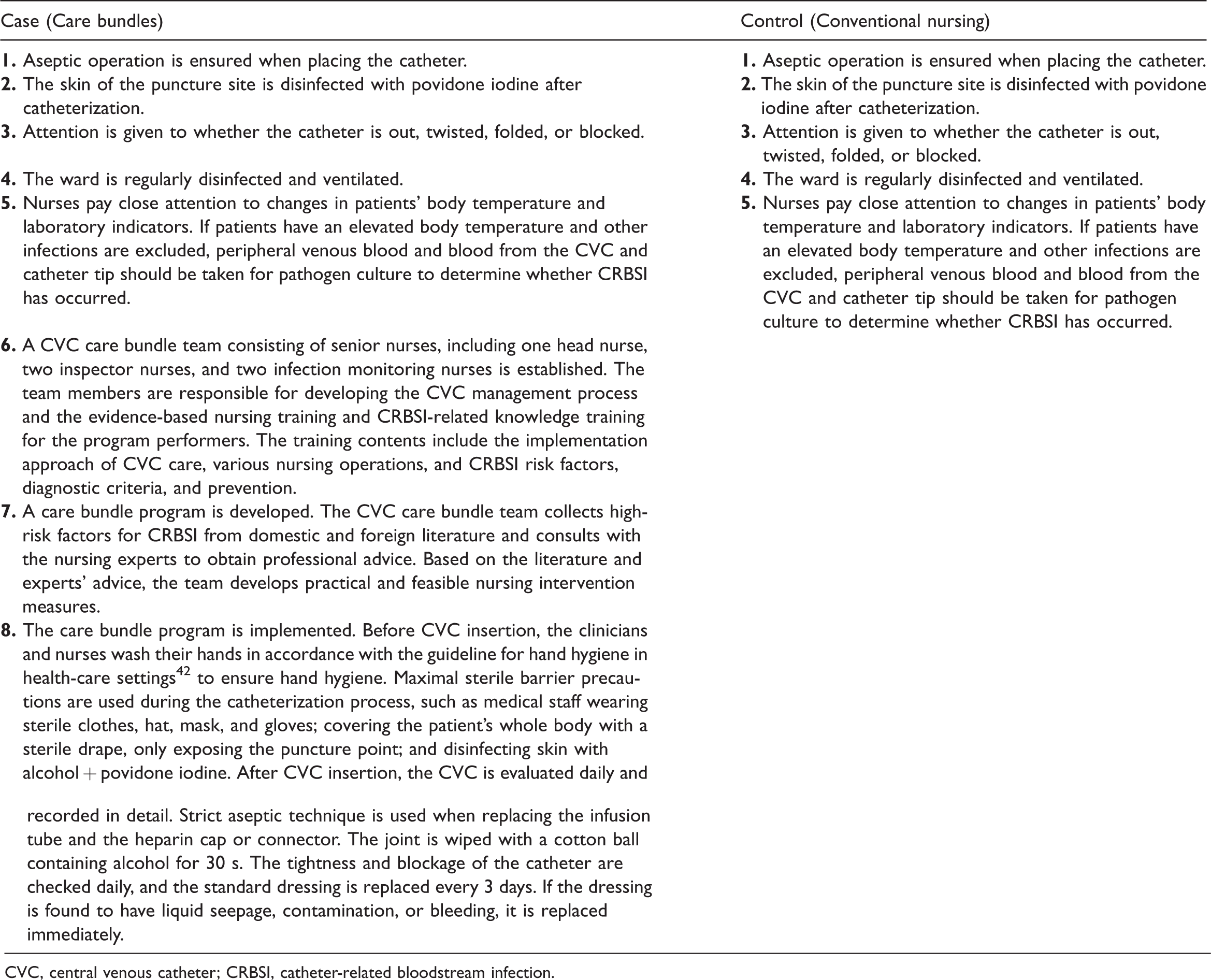
CVC, central venous catheter; CRBSI, catheter-related bloodstream infection.
This study was approved by the ethics committee of Beijing Shijitan Hospital (Institutional Review Board No. 2017036), and all patients provided written informed consent.
Diagnostic criteria for CRBSI16,17
Patients who met at least one of the following diagnostic criteria for CRBSI were defined as confirmed cases. (1) Positive semi-quantitative catheter culture (≥15 CFU per catheter segment) or positive quantitative catheter culture (≥1000 CFU per catheter segment) was obtained at least once, along with a positive peripheral venous blood culture with confirmation of the same offending organism as in the catheter culture. (2) The blood samples from the catheter and peripheral vein were quantitatively cultured at the same time, and the CFU ratio was ≥5:1 between the two samples. (3) The blood samples from the catheter and peripheral vein were qualitatively cultured at the same time, and the time to detection of the former was at least 2 hours earlier than that of the latter. (4) The same offending organisms were detected from the peripheral venous blood and pus at the outlet of the catheter.
Cases who met at least one of the following criteria were defined as clinically diagnosed cases: (1) The patient had clinical manifestations of severe infection, and the quantitative or semi-quantitative culture of the catheter tip or catheter segment was positive but the blood culture was negative. No source of infection other than the catheter could be found, and within 48 hours of removing the catheter, no new antibiotics were used and the symptoms of infection were improved. (2) The patient had clinical manifestations of fever, chills, and/or hypotension. Additionally, at least two blood cultures were positive (one of which was derived from peripheral venous blood), and the offending microorganisms from the two blood cultures were the same as the symbiotic microorganisms on the skin (such as diphtheroids, Bacillus, Propionibacterium, coagulase-negative Staphylococcus, Micrococcus, and Candida). However, the catheter segment culture was negative, and there were no other factors that could cause bloodstream infection.
Evaluation of patients’ psychological state
The patients’ psychological state was scored using the self-rating depression scale (SDS) 18 and self-rating anxiety scale (SAS). 19 The SDS and SAS were designed by Zung18,19 and are two widely used self-report measures in the area of depression and anxiety. Both are 20-item Likert scales in which psychological and physiological symptoms are rated by the respondents according to how each symptom applied to them within the past week. The SDS and SAS use a 4-point scale ranging from 1 (none or a little of the time) to 4 (most or all of the time). The SDS items are based on factor analytic studies of depression symptoms, 18 whereas the SAS items are affective symptoms based on diagnostic criteria listed in the major American psychiatry literature. 19 The total score for both the SDS and SAS ranges from 20 to 80. A higher score indicates more severe anxiety or depression.
Evaluation of patients’ satisfaction with hospitalization
On the day of discharge, the patients were asked to complete our self-made questionnaire on the satisfaction of medical services for inpatients, which was based on the content of the patient satisfaction survey prescribed by the former Ministry of Health 20 and reflected the inputs of medical staff and management experts of our hospital. The hospitalization satisfaction scores were divided into excellent (>90%), good (70%–89%), and poor (<70%) according to the ratio of the score for each questionnaire form to the total score. 21 The satisfaction rate was defined as the proportion of questionnaire forms with an “excellent” or “good” result.
Definitions
The number of catheter days was calculated as the number of days from catheter insertion to removal, and the CRBSI rate was calculated as the number of CRBSI episodes per 1000 catheter days (episodes of CRBSI/total sum of catheter days × 1000).
Data collection
Study data were collected from the medical records and entered into an Excel spreadsheet. The variables examined were sex, age, medical unit, BMI, APACHE II score, catheter insertion site, admission date, discharge date, catheter insertion date, catheter removal date, SAS score, SDS score, hospitalization satisfaction score, and number of CRBSI episodes.
Statistical analyses
Data are presented as mean ± standard deviation (range) or n (%) and were analyzed using SPSS 20.0 statistical software (IBM Corp., Armonk, NY, USA). Student’s t-test was used to compare quantitative data between the two groups, and the χ2 test was used to compare categorical data between the two groups. A P-value of <0.05 was considered statistically significant.
Results
Patients
In total, 212 patients were included in this study (case group, n = 106; control group, n = 106). There were no significant differences in sex, age, APACHE II score, BMI, department, or catheter insertion site between the two groups (Table 2).
Characteristics of patients in case and control groups.

Data are presented as mean ± standard deviation or n (%).
BMI, body mass index; APACHE II, Acute Physiology and Chronic Health Evaluation II; ICU, intensive care unit.
SAS and SDS scores before and after nursing in both groups
Although the SAS and SDS scores of the patients in the case and control groups were both significantly lower after than before the nursing intervention (P < 0.05), both the SAS and SDS scores were lower in the case group than control group after the intervention (P < 0.05) (Table 3).
Comparison of SAS and SDS scores before and after nursing in both groups.
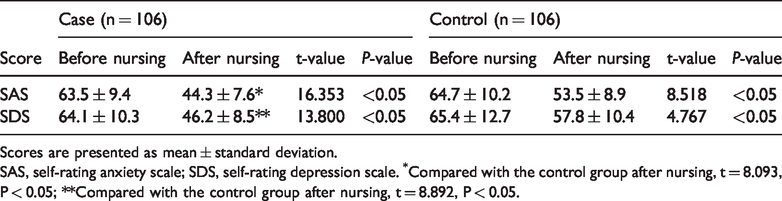
Scores are presented as mean ± standard deviation.
SAS, self-rating anxiety scale; SDS, self-rating depression scale. *Compared with the control group after nursing, t = 8.093, P < 0.05; **Compared with the control group after nursing, t = 8.892, P < 0.05.
Hospitalization days and CRBSI rate in both groups
After the care bundle intervention, the number of hospitalization days and the CRBSI rate were significantly lower in the case group than control group (P < 0.05 for both) (Table 4).
Comparison of hospitalization days and CRBSI rate in both groups.
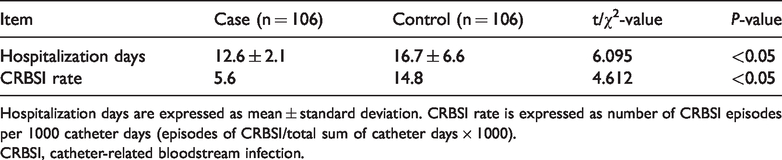
Hospitalization days are expressed as mean ± standard deviation. CRBSI rate is expressed as number of CRBSI episodes per 1000 catheter days (episodes of CRBSI/total sum of catheter days × 1000).
CRBSI, catheter-related bloodstream infection.
Hospitalization satisfaction scores in both groups
The hospitalization satisfaction score was significantly higher in the case group than control group (97.2% vs. 85.8%, respectively; χ 2 = 10.071, P < 0.05) (Table 5).
Comparison of scores of hospitalization satisfaction in both groups.

Data are presented as n (%).
Discussion
Care bundles are series of structured packages of evidence-based practices and interrelated interventions. They are used to develop nursing procedures for managing difficult clinical diseases and aim to improve nursing processes and patient outcomes.22,23 The nursing protocol generally consists of three to five simple, clear, and achievable evidence-based measures, the joint implementation of which is better than any single approach in improving patient outcomes. 21 Care bundles can greatly increase patients’ access to the required nursing care and enable effective implementation of every step of CRBSI prevention. A meta-analysis of the incidence of CLABSI in adult ICUs, neonatal ICUs, and pediatric ICUs showed that care bundles can significantly reduce the incidence of CLABSI across all age ranges. 24 Another meta-analysis of CLABSIs in neonatal units also showed a significant reduction in the incidence of CLABSI following the implementation of care bundles. 22 However, another meta-analysis of the effects of care bundles on patient outcomes suggested that the effect of care bundles is uncertain. 25
In the present study, we built a CVC care bundle team. The team assessed the risk factors for CRBSI and identified the weak links in nurses’ daily work (such as a lack of work experience in CVC nursing, delayed and inaccurate assessment of CVCs, and lack of system training and related operation standardization procedures). In response to these risk factors and weak links, the team provided targeted theoretical knowledge and operational training to the medical staff and developed a set of CVC catheterization nursing procedures including protocols of hand hygiene, catheterization site selection, catheterization nursing and routine maintenance, and other measures. The team also regularly evaluated the implementation of CVC operations and routine CVC maintenance and constantly optimized the nursing process and improved the quality of nursing.
The present study suggests that care bundles can improve patients’ psychological state and hospitalization satisfaction and reduce the number of hospitalization days; care bundles were also found to be associated with a significant reduction in the incidence of CRBSI. This seems to be supported by previous studies of CLABSIs.26–28 Development of the CVC management process and training of nurses in CRBSI-related knowledge are critical to ensure accurate implementation of other components in care bundles. The trained nurses can provide effective nursing measures and proper advice to patients and reduce the uncertainty and diffidence in dealing with clinical problems.29,30 Training of nurses can also dramatically improve the patients’ degree of satisfaction and alleviate their anxiety during hospitalization. These beneficial effects may be explained by the fact that uniform training can make nurses’ operations more standardized and give nurses adequate knowledge on CVC nursing, thus allowing them to provide detailed answers to patients’ questions and carry out all components of the care bundles during catheterization. These active interventions can reduce patients’ feelings of helplessness.
Other components of care bundles, such as hand hygiene, maximal sterile barrier precautions (MBPs), and bedside observation and evaluation by nurses, are also very important to prevent CRBSI. Although some studies have shown that CRBSI rates were reduced by partial compliance with the care bundles,28,31 one study revealed that the incidence of CRBSI for cases in which all elements of the care bundles were not perfectly performed was twice as high that for cases in which all elements of the care bundles were perfectly performed. 26 Therefore, physicians and nurses should implement all elements of the care bundles completely and without exception. The catheter insertion site may also affect the incidence of CLABSI; previous studies have revealed that femoral vein catheterization is associated with a higher risk of CRBSI than is subclavian or internal jugular vein catheterization.32–35 In this study, the differences in the proportions of catheter insertion sites between the case and control groups were not statistically significant, and the proportion of the femoral vein approach was lowest in both groups (around 10%) (Table 2). Thus, the use of the femoral insertion site had less negative impacts on care bundles in this study.
The use of MBPs is also a good way to prevent CRBSI; however, failure to use a full drape, which is an individual component of MBPs, could lead to a very high risk of CRBSI. 25 Therefore, some studies have suggested that MBPs, especially a full sterile drape, should always be used when inserting a CVC.36–38 In addition, some studies have shown that an alcohol + povidone iodine skin preparation is effective for preventing CRBSI,39,40 and the use of different types of dressings may affect the CRBSI rate. One study suggested that the use of chlorhexidine gluconate-impregnated sponge dressings in the ICU could reduce the incidence of CRBSI, and reducing the frequency of changing unsoiled adherent dressings from every 3 days to every 7 days modestly reduces the total number of dressing changes and appears to be safe. 41 In the present study, the standard dressing was used, and the frequency of changing dressings was every 3 days. Whether more frequent standard dressing changes, such as every 3 days, can significantly reduce the CRBSI rate should be investigated in future studies.
In conclusion, care bundles were found to be effective in decreasing the incidence of CLABSI, improving patients’ psychological state and hospitalization satisfaction, and reducing the hospitalization days. Therefore, care bundles should be performed as a routine protocol.