
Abstract
Return to driving is a highly valued goal for many following acquired brain injury (ABI) (Erler et al., 2018; Fleming et al., 2014; Novack et al., 2010). Occupational therapy driver assessments (OTDAs) explore the impact of a person's health and/or disability status on driving performance and can be used to ascertain capacity to resume driving post-ABI (Catchpole et al., 2019; Classen et al., 2009; Fields et al., 2019; Unsworth, 2007). One outcome that may arise following OTDA is a recommendation for on-road driving remediation (Bassingthwaighte et al., 2022; George et al., 2014; Ross et al., 2018; Unsworth & Baker, 2014). While evidence is emerging to support on-road remediation as an intervention to facilitate return to driving following ABI, little is known about whether skills acquired during driving remediation are maintained (Bassingthwaighte et al., 2021, 2024).
Independent driving post-ABI provides an opportunity for greater autonomy in accessing, initiating, and sustaining participation and engagement in community-based occupations. This often enables the resumption of occupations pivotal in fostering a positive self-identity and sense of well-being following traumatic brain injury (TBI) (Erler et al., 2018; Sanders et al., 2023) and stroke (Griffen et al., 2009; Liddle et al., 2009). In contrast, the inability to return to driving following ABI may limit participation in away-from-home occupations, increase dependence on others, diminish spontaneity and sense of self-control, and negatively impact upon psychosocial health (Bassingthwaighte et al., 2025; Sanders et al., 2023).
Although benefits to be gained from returning to driving post-ABI are substantial, many sequelae arising from brain injury can impact a person's capacity to competently negotiate the dynamic and demanding occupation of driving (Aufman et al., 2013; Classen et al., 2009). To mitigate the potential risk of health and/or performance concerns on driving safety, many driver license authorities require medical criteria to be met following ABI (Mountain et al., 2020; National Transport Commission, 2022). This process may involve participation in an OTDA to evaluate the capacity of the person to return to driving from an occupational performance perspective (National Transport Commission, 2022). In Australia, OTDAs are completed by occupational therapists with post-graduate qualifications in driver assessment and rehabilitation and occur after a medical practitioner has confirmed readiness to explore the potential to return to driving. These comprehensive assessments have been established as best practice in evaluating the influence of medical conditions on functional fitness to drive and consist of two main elements: an off-road evaluation and an on-road appraisal (Di Stefano & Macdonald, 2006; Fields et al., 2018). The off-road component seeks to appreciate the meaning of driving to the client and evaluates an array of person-related performance skills necessary for proficient and safe driving, such as visual acuity, strength and coordination, and attention. When indicated, progression to an on-road driving assessment provides an opportunity for an occupation analysis; a review of the client's capacity to operate the vehicle while navigating and negotiating the dynamic driving environment.
When driving performance and/or safety is noted to be compromised during OTDA, a recommendation for on-road driving remediation may result (Bassingthwaighte et al., 2022; Fields et al., 2018). However, there is currently insufficient robust evidence to determine the effectiveness of on-road driving remediation in achieving functional fitness to drive in general (Unsworth & Baker, 2014) or following stroke (George et al., 2014). Individualized on-road driving remediation programs devised by occupational therapists with qualifications in driver assessment and rehabilitation, and delivered by driving instructors, show promise in achieving a recommendation for return to driving following ABI (Bassingthwaighte et al., 2024; Ross et al., 2018). However, the increased risk of motor vehicle accidents following return to driving post-stroke (Perrier et al., 2010) and TBI (Bivona et al., 2012; Novack et al., 2023) raise concerns about whether driving skills developed during driving remediation are maintained.
The primary objective of this study was to investigate the driving performance and functional fitness to drive status of people experiencing ABI immediately after participation in on-road driving remediation and at six-month follow-up. This was to determine if skills acquired during on-road driving remediation were maintained. The secondary objective was to explore driving performance and person-related factor differences between those recommended as functionally fit to return to driving and those not functionally fit to drive at follow-up (hereinafter referred to as “fit” or “not fit” to drive). Exploring such differences may offer guidance when considering, developing, and/or assessing the outcome of driving remediation.
Methods
Study Design
The present study is a secondary analysis of a waitlisted randomized controlled trial with follow-up (Bassingthwaighte et al., 2024) conducted in accordance with the protocol registered with the Australian New Zealand Clinical Trials Registry ACTRN12620000057987. Sample size calculations and randomization procedures have been previously described (Bassingthwaighte et al., 2024). All participants received the intervention (immediately or following a six-week period of waiting), and this article reports a secondary analysis of the post-intervention and six-month follow-up data from all participants. Figure 1 illustrates participant flow and assessment points of the secondary analysis using a CONSORT diagram (Butcher et al., 2022). The study was approved by the appropriate health service (HREC/2019/QMS/57505) and university (GU2020/115) ethics committees.
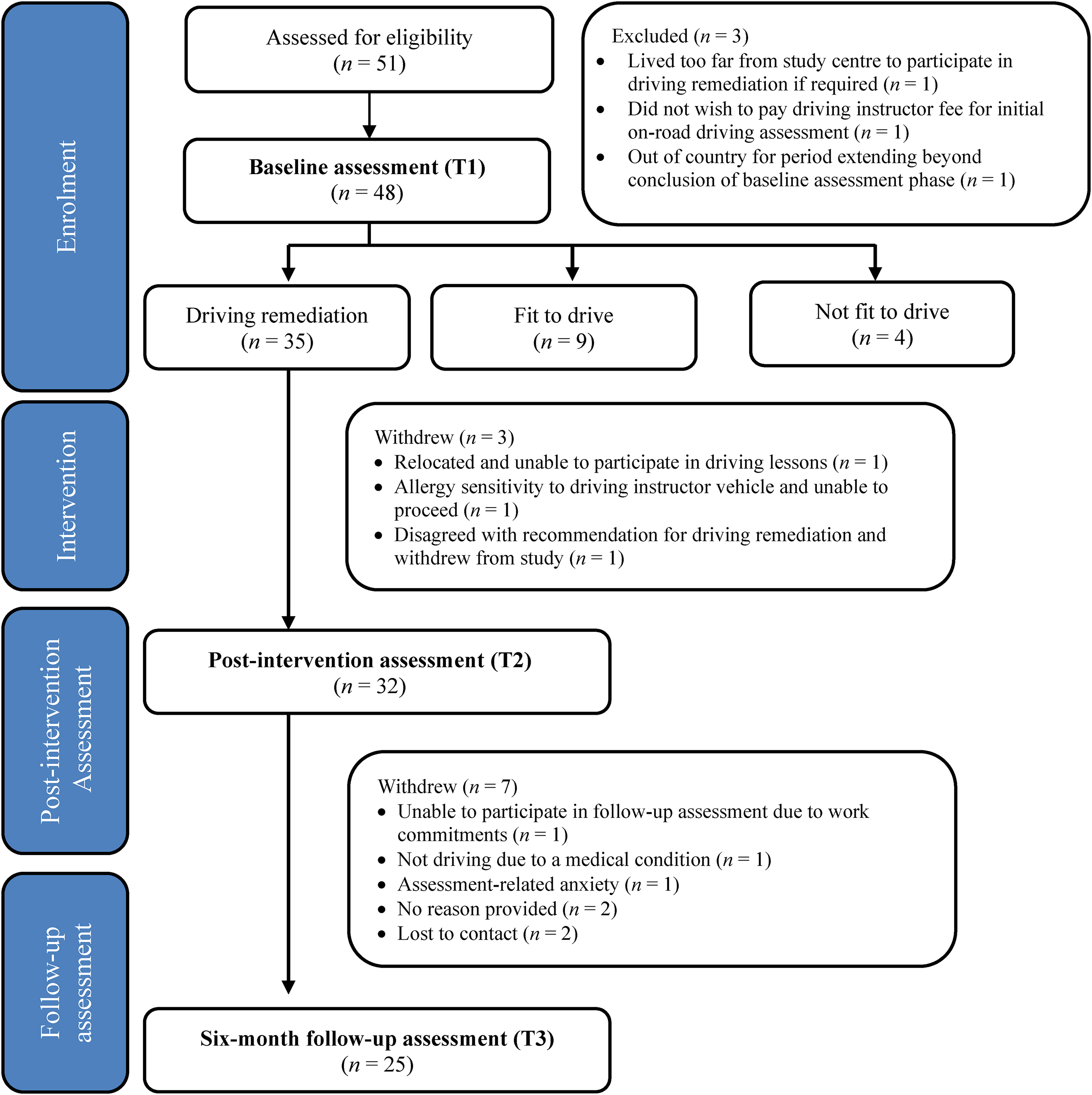
Consolidated standards of reporting trials (CONSORT) Participant flow and assessment points.
Participants and Study Setting
Adults with ABI referred to an Australian tertiary public hospital occupational therapy driving assessment and rehabilitation service for OTDA were recruited between May 2021 and January 2023, with the final six-month follow-up data collection concluding in July 2023. Inclusion criteria were (a) aged between 18 and 65 years inclusively; (b) medically stable and cleared by a doctor to participate in OTDA; (c) holder of a current and valid provisional or open drivers’ license; and (d) diagnosis of ABI. Potential participants were excluded if they were (a) a learner driver; or (b) had a previous neurological condition/incident.
Blinding
Table 1 provides an overview of personnel involved in data collection, assigned roles, and blinding status of randomized controlled trial group allocation (i.e., intervention group vs. waitlisted control group). All instructors and therapists were blinded to group allocation and were unaware as to whether participants had received on-road driving intervention at post-intervention review. To minimize inadvertent potential bias, participants were advised to not disclose their completion or otherwise of any driving lessons to outcome assessors.
Study Personnel, Role, and Blinding Status
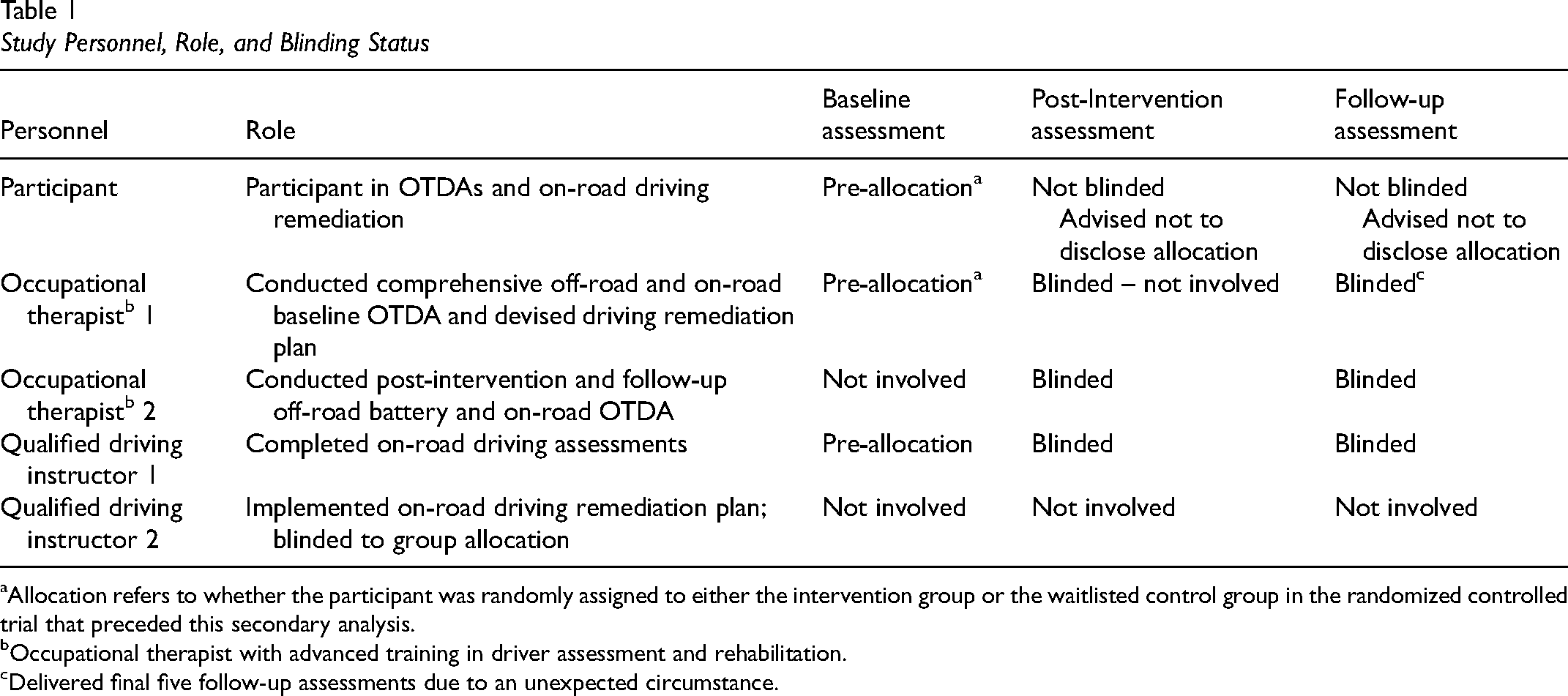
Allocation refers to whether the participant was randomly assigned to either the intervention group or the waitlisted control group in the randomized controlled trial that preceded this secondary analysis.
Occupational therapist with advanced training in driver assessment and rehabilitation.
Delivered final five follow-up assessments due to an unexpected circumstance.
Intervention
The intervention consisted of an individualized on-road driving remediation program to address driving performance concerns identified during baseline OTDA. Programs were devised by occupational therapist 1 (see Table 1), who conducted baseline OTDAs with input from driving instructor 1. Driving remediation goals outlined in Table 1 were classified according to the domains defined by Di Stefano and Macdonald (2006) and utilized by Ross et al. (2018) in their exploration of interventions for resuming driving after TBI: cognitive goals, physical goals, visual goals, addressing previously learned skills, and addressing psychological issues.
A qualified driving instructor experienced in working with people with medical conditions (driving instructor 2) delivered the program in a dual-control car. Completed at a frequency of one to two sessions/week over a period up to seven weeks, most sessions were of 60-minute duration, although five participants were prescribed 90-minute sessions for at least one of their driving lessons, and one participant a 120-minute lesson to address endurance issues (e.g., sustained concentration and fatigue management). Three phases of intervention described in-depth previously were adopted: (i) knowledge phase to enhance participant awareness of skills requiring address, (ii) on-road practice opportunities to learn and apply strategies to remediate and/or compensate for impaired driving performance, and (iii) facilitation of independent application of skills (Bassingthwaighte et al., 2021, 2024).
Measures
Demographic and Medical Conditions
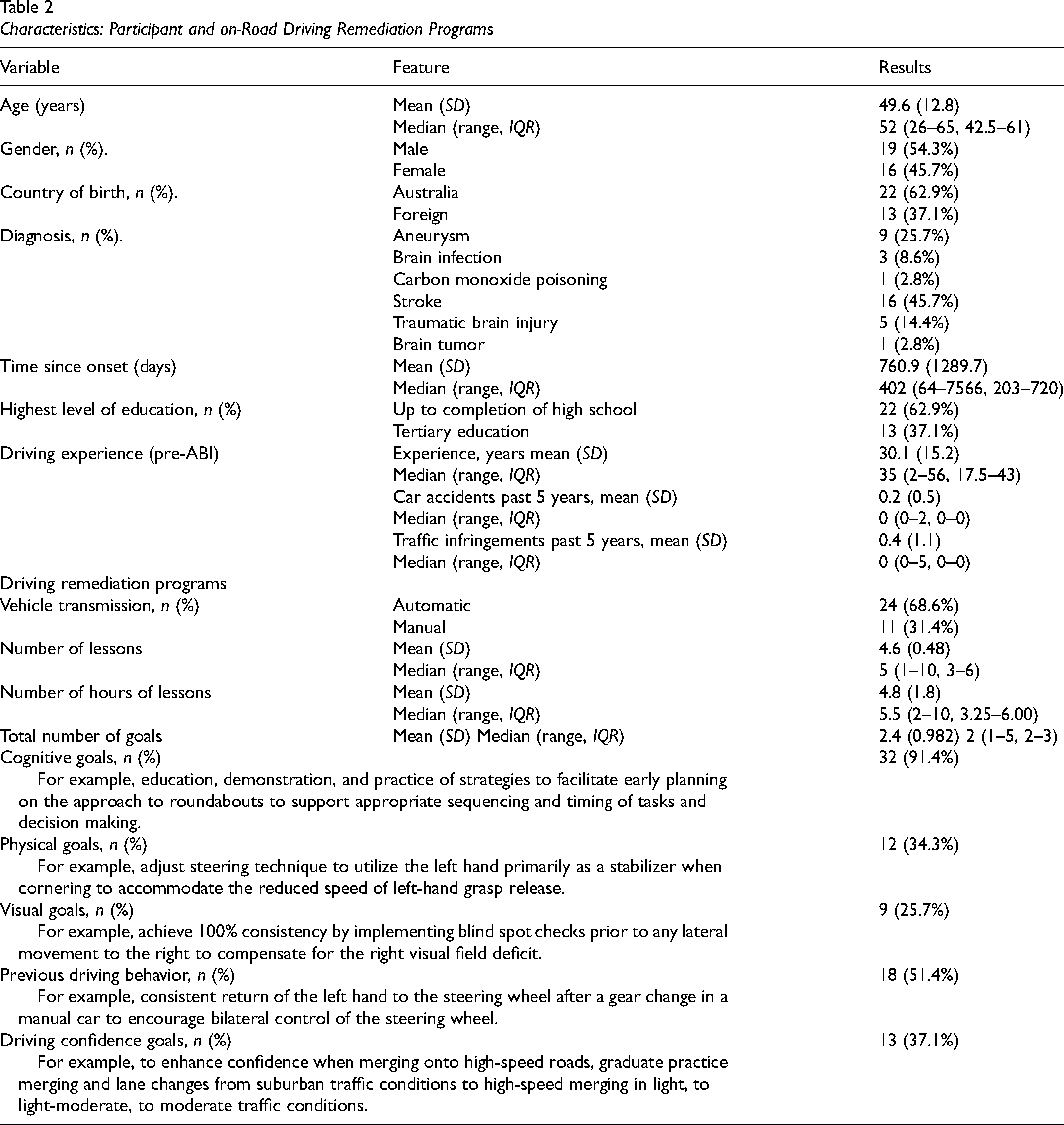
Demographic and condition-related information itemized in Table 2 were extracted from participants’ electronic medical records.
Characteristics: Participant and on-Road Driving Remediation Programs
Driving Performance Measures
Functional Fitness to Drive
The primary outcome measure was functional fitness to drive as measured by the outcome of a standardized 18 km on-road OTDA led by occupational therapists with advanced training in driver assessment and rehabilitation, with a qualified driving instructor delivering scripted instructions in a dual-controlled vehicle (see Table 1). Specific testing of the validity and reliability of the primary and secondary on-road assessment routes was not undertaken. Rather, the design of the assessment protocol was informed by previous studies, which confirmed on-road occupational therapy driver assessments as a valid indicator of driving performance capable of identifying types and locations of driving errors (Mallon & Wood, 2004; r = .76, p < .001). Measures to enhance construct and content validity of the outcome measure included compliance of the assessment protocol and on-road route with Australian Competency Standards for Occupational Therapy Driver Assessors (Fields et al., 2018), VicRoads Occupational Therapy Driving Test: Assessment Manual (Catchpole & Di Stefano, 2018; Di Stefano & Ross, 2018), and Mallon and Bewert (2011). Inter-rater reliability was enhanced through a series of theoretical workshops and practical sessions attended by all therapists and instructors involved in the program of research. Sessions were designed to facilitate consistent application of the assessment protocol, “critical error” definition, and clinical reasoning processes. This included a practice on-road driving assessment where the qualified driving instructor tasked with completing the assessments delivered the scripted instructions, and all occupational therapists involved in the program of research evaluated driver performance. Reflective and discussion activities aimed to further hone reliability. Details about the assessment routes and core elements, timing, and conduct of all on-road assessments, and risk mitigation strategies were comprehensively described in the randomized controlled trial (Bassingthwaighte et al., 2024).
Secondary Driving Performance Measures
Two secondary outcome measures adopted in the randomized controlled trial were used to explore driver performance (Bassingthwaighte et al., 2024). Firstly, critical error frequency was recorded. Any incident requiring driving instructor verbal or physical intervention or the requirement for another road user to take evasive action to maintain the safety of the assessment vehicle, its occupants, or other road user/s, was defined as a critical error (Di Stefano & Ross, 2018) and tallied. Secondly, the percentage of correctly performed maneuvers was calculated. For each maneuver (e.g., negotiating a roundabout or turning left at a non-traffic light controlled intersection), participant performance was rated as appropriate or not on a range of parameters: observation; awareness and attention to the driving environment; vehicle control (brake, accelerator, and steering); use of accessories; vehicle position; speed control; planning and judgement; and road law (see Supplemental Material). Failure to appropriately attend to any parameter resulted in that item being rated as an incorrect maneuver. There was no expectation that participants perform all maneuvers without error, and it is recognized that not all errors are equivalent. It is possible for multiple non-critical errors to occur in the context of safe driving performance, while a single critical error is sufficient to result in a not fit to drive recommendation. The exploratory nature of these calculations meant there was no criterion of proportion of correct maneuvers to indicate fit to drive, not fit to driving or driving remediation outcomes.
The total percentage of correct maneuvers reflected the combination of two navigation-based calculations. Firstly, the percentage of correct maneuvers when driving under the direction of the driving instructor (i.e., driving instructor-directed navigation). Secondly, the percentage of correct maneuvers whilst self-navigating using road signs and markings (i.e., self-directed navigation). At the conclusion of the session, the therapist calculated percentage of correct maneuvers, tallied critical errors, rated the drivers performance on ten domains (observation, awareness of driving environment, attention, steering control, use of accessories, control of pedals and gears, vehicle positioning, speed control, planning and judgement and self-navigation) as “functional” or “not competent” and then and through a process of consensus with the driving instructor, rated overall driving performance as (i) fit to drive, (ii) not fit to drive, or (iii) on-road driving remediation indicated.
Person-Factor Measures
The off-road assessment battery was completed prior to the on-road assessment and comprised measures designed to evaluate person-related factors associated with driving a motor vehicle and included: visual screening (Owsley et al., 2015), Rapid Pace Walk Test (RPWT) (Ball et al., 2006), Trails Tests A and B (Abeare et al., 2019; Marshall et al., 2007), Adelaide Driving Self-Efficacy Scale (ADSES) (George et al., 2007), Patient Awareness Questionnaire (Sherer et al., 2003), Depression, Anxiety and Stress Scale (DASS-21) (Lovibond & Lovibond, 1996), and Lifespace Mobility Assessment-Composite (LSMA-C) (Peel et al., 2005).
Procedure
All eligible participants completed a comprehensive baseline OTDA conducted by occupational therapist 1 and driving instructor 1 (see Table 1). The results of the baseline OTDA formed the pre-intervention results, and only participants recommended for on-road driving remediation progressed. The on-road driving remediation plan was devised by occupational therapist 1 following the conduct of the baseline assessment and implemented by driving instructor 2. Post-intervention OTDA was conducted within one week of completing the driving remediation program. Follow-up OTDA was completed six months after the post-intervention assessment. Both post-intervention and follow-up assessments were conducted by occupational therapist 2 and driving instructor 1. These assessors were blinded to group allocation and were not aware whether the intervention had been received or otherwise. There was a variation to this protocol due to the unexpected unavailability of occupational therapist 2 for the final five follow-up assessments. These were conducted by occupational therapist 1, who was blinded to the outcome of driving remediation.
Influence of COVID-19
The study was impacted by the COVID-19 pandemic and Australia's management, including local and national lockdowns and restricted travel (Stobart & Duckett, 2022). The conduct of research adhered to hospital directives to mitigate COVID-19 transmission, which included screening for symptoms of viral illness pre-assessment and the closure of service during times of increased community transmission. Post-intervention assessment was delayed up to one week for three participants. Six participants completed the six-month follow-up between seven and eight months due to COVID-related delays (five) or assessor ill-health (one).
Data Analysis
Data were analyzed using IBM SPSS Statistics version 30. Summary statistics of baseline participant characteristics are presented depending on the nature of the variable and its contribution. Categorical variables were described using frequencies and proportions. Continuous variables were described using mean, median, standard deviation, range, and interquartile range. Inferential statistics were used to determine if a significant change in driver status, driving performance, and/or person-related factors was observed between post-intervention and follow-up (McNemar test and Wilcoxon signed-rank test) and to explore relationships between driving performance and person-related factors and driver status at follow-up (Fisher's exact test and Mann-Whitney U-test). Effect size was calculated using partial eta squared (
Results
Participants
Figure 1 illustrates participant flow through the project. This secondary analysis concerned 35 participants recommended to receive an on-road driving intervention. Three participants withdrew from the study and did not complete the intervention or subsequent assessments, resulting in 32 (91.4%) completing on-road driving remediation and post-intervention assessment. Table 2 outlines participant and driving remediation characteristics, including the number of lessons, hours of on-road driving, and remediation goals. On average, participants (n = 32) received 4.6 lessons (range: 1–10) and 4.9 hr (range: 2–10) of on-road driving remediation during their program. Post-intervention, 23 participants (71.8%) achieved a fit to drive outcome, two (6.2%) were deemed not fit to drive, and seven (21.2%) were not fit but recommended to participate in further driving remediation. A recommendation for further driving remediation intervention between post-intervention and follow-up was not encountered in the preceding feasibility study. Consequently, this study was not designed to include a multi-phase program. While capturing this data comprehensively or not exposing some participants to remediation between post-intervention and follow-up assessments would have been preferred, the research team held the view that withholding further remediation would have been unethical and not in the participants’ best interest. Therefore, participants who elected to pursue further remediation did so external to the study, with detailed data concerning such programs not available. For transparency, the number of participants who did complete further remediation and what is known about their driving status at follow-up is reported.
Twenty-five (78.1%) participants progressed to follow-up. Ninety-five percent of the 19 participants deemed fit to drive and 50% of the six participants assessed as not fit to drive post-intervention, retained that status at follow-up. Four participants (16%) experienced a change in driver status at follow-up, with one changing from fit to not fit to drive and three from not fit to fit to drive. The seven participants recommended to progress further driving remediation after post-intervention assessment, were fit to drive (n = 3), not fit to drive (n = 1), lost to contact (n = 2), or withdrew from the study (n = 2) at follow-up. No participants reported involvement in a motor vehicle accident or any driving infringements (e.g., speeding fines) between return to driving post-ABI and follow-up. There was no missing data for any variable of interest for those participants who remained in the study.
Post-Intervention to Follow-up
Comparisons between post-intervention and follow-up outcomes in terms of functional fitness to drive status, on-road driving performance, and person-related elements revealed no statistical significance difference for any factor. Table 3 details the post-intervention to follow-up findings, and Figure 2 illustrates the driver status at the same time periods.
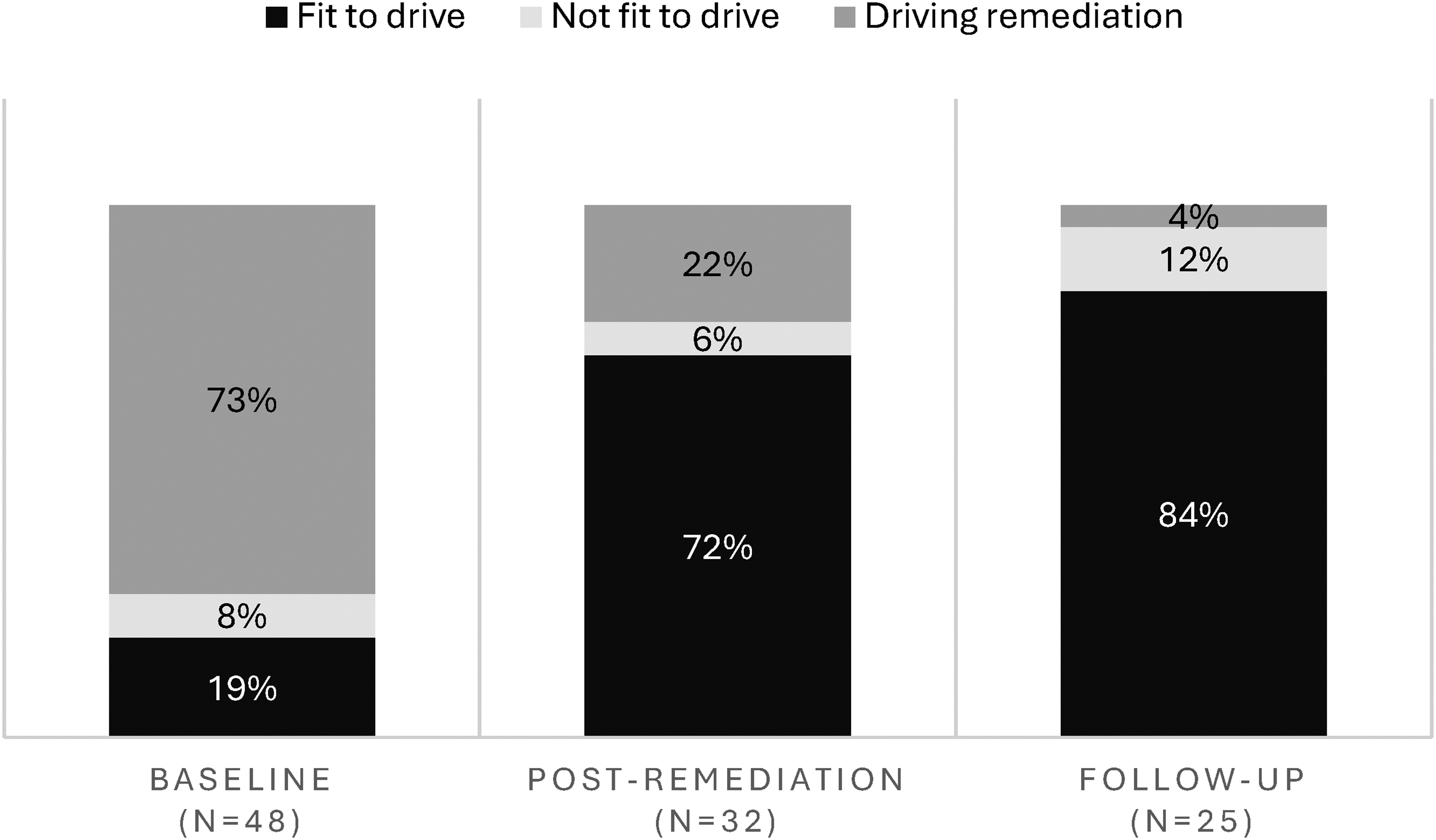
Fitness to drive at baseline, post-intervention, and at follow-up.
Post-Intervention to Follow-Up Comparison
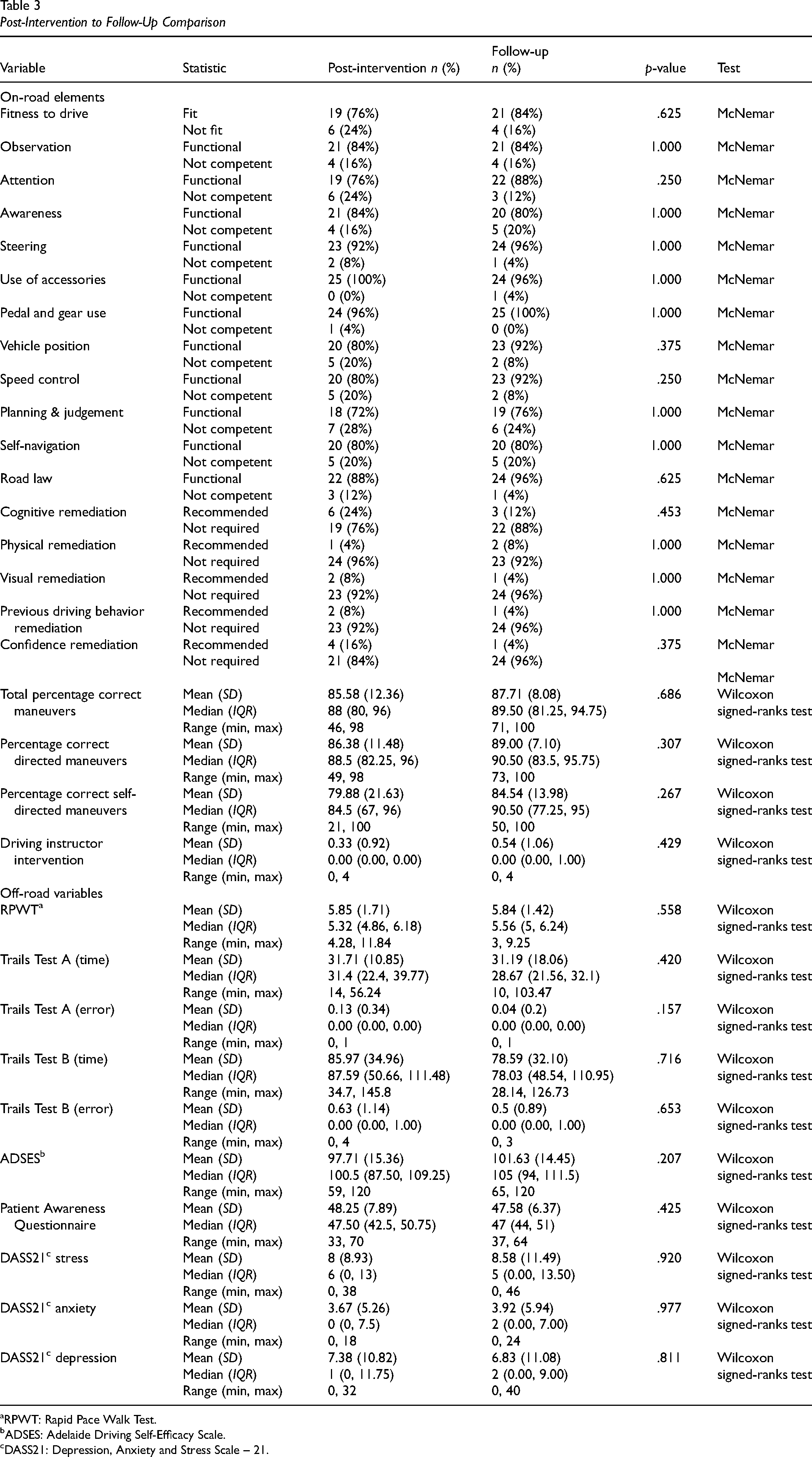
RPWT: Rapid Pace Walk Test.
ADSES: Adelaide Driving Self-Efficacy Scale.
DASS21: Depression, Anxiety and Stress Scale – 21.
Relationship With Driver Status at Follow-Up
The relationships between driving performance, person factors, and driver status at follow-up are presented in Table 4. Statistically significant differences with large effect sizes were observed between those rated as fit to drive and not fit to drive at follow-up in relation to self-awareness (p = .03,
Factors According to Driver Status at Follow-Up.

ADSES: Adelaide Driving Self-Efficacy Scale.
Lifespace: Lifespace Mobility Assessment-Composite.
DASS-21: Depression, Anxiety and Stress Scale − 21.
RPWT: Rapid Pace Walk Test. * p < 0.05; ** p <0.001.
Discussion
The findings from the previous randomized controlled trial, which informed the present secondary analysis, confirmed the association between participation in comprehensive OTDA and individualized on-road driving remediation and achieving a fit to drive recommendation for adults who were drivers pre-ABI onset (Bassingthwaighte et al., 2024). This secondary analysis observed no significant change between post-intervention assessment and six-month follow-up in terms of driver status (i.e., recommendation of fit or not fit to drive), on-road driving performance, or off-road measures. These findings confirm the retention of driver status and driving performance skills developed during on-road driving remediation following ABI six-months post-intervention.
In support of the usefulness of on-road driving remediation following ABI, 95% of participants achieving a fit-to-drive recommendation post-intervention maintained that status at follow-up. Furthermore, no participants reported any involvement in a motor vehicle accident, nor did they record any driving infringements (e.g., speeding fines) between return to driving and follow-up. It appears that in the short to medium term post-intervention, skills developed during on-road driving remediation and the safe driving practices demonstrated at assessment are successfully sustained. This is consistent with more recent crash risk data following return to driving following stroke (Naredo Turrado et al., 2021) and contemporary evidence associating a lower crash risk with less time since resuming driving following TBI (Novack et al., 2023). Yet findings are at odds with longer-term elevated crash risk following stroke (Perrier et al., 2010) and TBI (Neyens & Boyle, 2012; Novack et al., 2023). Factors beyond driving remediation may also influence post-RTD accident rate. Deterioration in function over time has been established following moderate to severe TBI (Forslund et al., 2019). Potentially, debilitating effects arising from chronic ABI may influence driving performance over the longer term, challenging the capacity to maintain driving competency.
Three participants deemed not fit to drive following on-road driving remediation later demonstrated competent driving performance at follow-up. Each of these participants engaged in further on-road driving remediation, outside the scope of this study, to continue the gains made during their initial program. Findings may indicate that for some, successful return to driving may be achieved via more lengthy or multi-phase programs such as those described by Ross et al. (2018), who delivered on average 7 hr of driving remediation and 2.5 assessments for drivers who had sustained TBI. In gauging potential for further on-road remediation, particular consideration of driving performance factors associated with a functional fit to drive recommendation at follow-up (i.e., observation and awareness of driving environment, speed control, planning and judgement, and self-navigation) and capacity to respond to tuition concerning these factors, are indicated.
Differences between participants deemed fit or not fit to drive at follow-up were explored. Evidence concerning factors predicting successful or otherwise, return to driving outcome remains unclear. Retrospective studies have identified inconsistent associations between return to driving post-ABI and person-related factors such as age (Chua et al., 2012; Novack et al., 2010), cognitive status (Aufman et al., 2013; Marshall et al., 2007; McKay et al., 2016), and pre-ABI onset driving experience (Marshall et al., 2007), as well as diagnostic characteristics including years since TBI onset (Chua et al., 2012; Coleman et al., 2002) and injury severity (McKay et al., 2016; Novack et al., 2021; Ross et al., 2015). Apart from awareness at follow-up, this study observed no associations between any person or diagnostic-related factors and returning to driving following on-road driving remediation after ABI. This may partially reflect the diverse diagnostic groups represented in the sample and the inability to explore injury severity due to small numbers in subgroups. Previous studies exploring predictive factors for return to driving do not consistently report the manner of return to driving post-ABI. For example, some describe participation in a form of driver evaluation (e.g., OTDA, medical screening, and licensing authority examination) as a precursor to return to driving post-ABI, and others report on return to driving irrespective of the pathway (e.g., self-determined readiness to return to driving). It is proposed that the two-tier screening process preceding on-road driving remediation in this study (i.e., [1] medical clearance indicating readiness to return to driving and [2] comprehensive OTDA excluding those for whom on-road driving remediation is deemed inappropriate) assisted with screening out those for whom diagnostic and person-related factors may influence capacity to respond to on-road driving remediation after ABI.
This study highlights the importance of demonstrating competent observation, awareness, speed control, planning, judgement, and self-navigation driving performance skills in achieving a fit to drive recommendation at follow-up after on-road driving remediation. This partially aligns with findings concerning on-road driving performance following TBI, which found that those who failed the assessment demonstrated errors with observation, speed control, and gap selection (a component of planning and judgement), although links with lane positioning and car control were not evident in this cohort (Stolwyk et al., 2019). Clinical application of these findings may guide practice in two ways. Firstly, consideration of the noted performance elements may increase confidence in fitness to drive judgments during post-driving remediation assessment. Findings may reinforce readiness, or otherwise, to return to driving, should competent or incompetent performance be displayed across the key areas.
Secondly, careful monitoring of the development and application of these skills (in addition to specific individual driving remediation goals) during on-road driving remediation may guide decision making about further on-road intervention and the timing of re-assessment. For example, for participants unable to sufficiently progress key driving performance skills within their defined driving rehabilitation plan, discontinuation of driving remediation may be indicated. Alternatively, for those making good progress but are not yet competent with key driving performance skills, discussions between the driving instructor, occupational therapist, and client may explore the option of extending on-road remediation prior to undertaking on-road re-assessment. This process may alleviate psychological distress associated with ill-timed driving re-assessment (Leung et al., 2009) and reduce the financial burden associated with unnecessary repeated mid-driving remediation (Bassingthwaighte et al., 2024; Ross et al., 2018).
It was not surprising that achieving a higher percentage of correct maneuvers was related to a fit-to-drive OTDA outcome. It makes sense that less driving errors be associated with a fit to drive recommendation. This was not universally observed with the two sub-components of the measure—driving instructor-directed navigation and self-directed navigation. Though a strong association was illustrated between being fit to drive and percentage of correct self-directed maneuvers (p = .003, η2 = 0.49), no relationship was observed for percentage of driving instructor-directed maneuvers (p = .081). This aligns with previous findings demonstrating that more errors (proportionally) are observed during self-directed compared to instructor-directed navigation for healthy adults and older adults with and without early visual impairment (Mallon & Wood, 2004), reflecting the more complex demands experienced when required to self-navigate. It also reinforces the recommendation for self-navigation to be included in driving remediation programs following TBI (Ross et al., 2018) and when clinically indicated during OTDA (Fields et al., 2018), extending the recommendation to the broader ABI population.
In this study, lifespace (p = .047, η2 = 0.16) was associated with fitness to drive at follow-up. Lifespace refers to the geographical space within which a person conducts their life (Peel et al., 2005). It reflects the frequency, extent, and level of support required to access domains within the home and community (Kuspinar et al., 2023). Significant differences in lifespace scores were evident between participants recommended as fit to drive (M = 75.95) and those not fit to drive (M = 53.75) at follow-up. This study extends the significant association identified between lifespace and the ability to drive a car in older adults (Hashimoto et al., 2021) and the significant decline in lifespace described following driving cessation for community-dwelling older adults (Huisingh et al., 2017) to include those experiencing ABI. Participants deemed not fit to drive following on-road driving remediation experienced a restricted lifespace score of less than 60 (Phillips et al., 2019). This may signal unsuccessful on-road driving remediation post-ABI as a time when additional supports may be required to facilitate adjustment to unfulfilled return to driving goals identified as necessary to increase uptake of alternate community access options required for community-based occupational participation (George et al., 2022; Liddle et al., 2011).
The relationship identified between higher levels of awareness and a fit to drive recommendation in this study are similar to previous studies linking lower self-awareness scores with failed on-road driver assessment post-TBI (Gooden et al., 2017). The higher awareness scores associated with fit to drive recommendation at follow-up may reinforce the importance of effective error monitoring performance in achieving competent driving following ABI (Robertson & Schmitter-Edgecombe, 2015). Conversely, over-estimation of driving performance may restrict capacity to adjust driving behavior, leading to inadequate response to the driving environment at a tactical level (Lundqvist & Alinder, 2007). The inclusion of strategies to build accurate awareness of driving performance may be indicated during on-road driving remediation following ABI.
There are limitations to acknowledge with this study. Firstly, as a single-center study, findings may partially reflect local practices such as driving instructor tuition style, occupational therapist professional reasoning, or the complexity of the assessment course. Future studies could include multiple sites to enhance confidence in the generalization of the intervention. Secondly, this study explored the influence of a single-phase on-road driving remediation program and did not account for subsequent driving remediation undertaken external to this study between post-intervention assessment and follow-up. Given that some participants were able to achieve a fit to drive recommendation at follow-up after pursuing a multi-phase remediation program, future investigations may consider an approach that accounts for all on-road driving remediation undertaken to achieve a fit to drive recommendation. Findings may further illuminate understanding of queries such as who may benefit from multi-phase driving remediation and how many phases might be considered sufficient. Finally, consideration is required of the heterogeneity in diagnoses, injury severity, and pre-ABI driving experience, as well as the middle-aged sample recruited to this study. Findings may not apply to all people seeking a return to driving following ABI.
Opportunities for further investigation are apparent. Longitudinal exploration of driving performance following ABI with extended follow-up periods (e.g., 5–10 years) may provide greater insight as to whether and/or when driving performance may begin to decline and whether on-road interventions to refresh driving performance at that time is viable to manage elevated crash risk reported following ABI and support people to safely drive longer. Additionally, this study focused on participants who were drivers prior to the onset of their ABI. Exploration of the learn to drive process and outcomes for people who acquire a brain injury prior to achieving driving competency requires investigation.
Conclusion
Following comprehensive OTDA, on-road driving remediation designed by an occupational therapist with post-graduate qualifications in driver assessment and rehabilitation and delivered by a qualified driving instructor, can be effective in achieving and maintaining competent driving performance following ABI.
Key Messages
On-road driving remediation programs may be effective in achieving and maintaining a fit to drive recommendation following ABI. Multi-phase on-road driving remediation may be indicated for some. For those not fit to drive post-OTDA and on-road rehabilitation, exploration of alternate ways to access community are indicated to facilitate participation in community-based occupations.
Plain-Language Summary
Many people want to return to driving after an ABI. Occupational therapy driver assessments check how a person's injury and overall health affect their ability to drive. Some people may need on-road driving lessons to improve their skills and become safe, confident drivers. The assessment and lesson process can be expensive and take time. Little is known about whether skills gained during lessons truly help people return to driving. This study found that the skills gained through on-road driving lessons remained strong six months later. This suggests driving lessons can be a valuable part of rehabilitation, helping people living with ABI return to driving. These findings are important for people living with ABI, occupational therapists, and funding bodies. We can be more confident in on-road driving rehabilitation as a way to regain and keep competent driving after ABI.
Supplemental Material
sj-docx-1-cjo-10.1177_00084174261427989 - Supplemental material for On-Road Driving Remediation After Acquired Brain Injury: Driving Performance at Follow-Up
Supplemental material, sj-docx-1-cjo-10.1177_00084174261427989 for On-Road Driving Remediation After Acquired Brain Injury: Driving Performance at Follow-Up by Louise Bassingthwaighte, Louise Gustafsson, Matthew Molineux, William Pinzon Perez, Ryan Bell and Darshan Shah in Canadian Journal of Occupational Therapy
Footnotes
Acknowledgments
Our gratitude is extended to participants in this study for sharing their experiences. We acknowledge the support of the Princess Alexandra Hospital Occupational Therapy Department in enabling the implementation of this research initiative, including Mary Whitehead, Nicole Weir, Penny Whitelaw, and Janelle Griffin. We appreciate the contributions made by driving instructors during the assessment and remediation phases of the program.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Hopkins Centre, MetroSouth Health (grant number Seed Grant, RSS_2020_013).
Supplemental Material
Supplemental material for this article is available online.
ORCID iDs
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.