
Abstract
Background.
People with Parkinson's disease (PwPD) experience increasing disability due to progressive motor and non-motor symptoms. Comprehensive rehabilitation approaches are needed to maximize their daily functioning. CO-OP targets daily functioning and has established efficacy in populations with similar symptom profiles.
Purpose.
To explore the potential of CO-OP for PwPD, a feasibility randomized controlled trial (RCT) was conducted.
Methods.
Consenting PwPD (n = 20) were recruited to a parallel group, assessor masked RCT. Following baseline assessment, participants were randomized to CO-OP (20 sessions:10-weeks) or a waitlist control (WLC; 0 sessions: 10 weeks). Goal attainment, functional and cognitive status, quality of life, self-efficacy, transfer, and maintenance were measured. Data were analyzed using descriptive statistics and multiple regression analysis.
Results.
Effort (M = 3.02/5) and enjoyment (M = 3.15/5) ratings; homework completion (M = 91%) and protocol adherence (M = 82%) indicate that CO-OP is feasible. CO-OP was superior to the WLC on Canadian Occupational Performance Measure (COPM) performance (p=<.001), COPM satisfaction (p=<.001), and Performance Quality Rating Scale (PQRS; p=<.001) but not the Goal Attainment Scale (GAS; p = .123).
Conclusions.
Addressing a critical gap in Parkinson's disease management, findings suggest that CO-OP is implementable, feasible, and potentially beneficial for PwPD. Further research is warranted to further establish efficacy.
Introduction
Parkinson's Disease (PD) is the world's fastest-growing progressive neurological disorder, with its prevalence expected to double by 2040 (Dorsey et al., 2018). PD's complex and highly individualized symptoms and variable rate of progression present significant treatment challenges (Bloem et al., 2015). While PD is characterized by well-known motor symptoms including tremor, rigidity, bradykinesia, and postural instability (Jankovic, 2008), it also involves a multitude of non-motor symptoms that significantly reduce quality of life (QoL), increase economic burden, and heighten risk of institutionalization (Biundo et al., 2017; Gaudet, 2002). Although management of non-motor symptoms has been declared an important area of unmet need (NICE, 2017), research indicates that difficulties in daily life arise from the complex interactions and cumulative impacts of PD symptoms that are observed across the course of the disease (Goetz & Pal, 2014; Seppi et al., 2019). This indicates that comprehensive, individualized interventions are needed to address the multifaceted impacts of PD.
Literature suggests that people with PD (PwPD) benefit from interventions that target physical skills and daily functioning through physical activity, environmental cueing, self-management and cognitive-behavioural strategies (Foster et al., 2014). However, most occupational therapy intervention research in PD has focused on physical performance skills, with interventions addressing cognitive or psychosocial performance skills so far understudied (Foster et al., 2014). This contrasts with other populations where occupation-based metacognitive interventions that target physical, cognitive and psychosocial performance are routinely implemented with positive effect (Cicerone et al., 2019). Metacognition refers to higher-order cognitive processes that involve planning, monitoring, and regulating one's own performance (Lai, 2011). Occupation refers to “the daily activities that people do to care for themselves, participate in family life, and contribute to broader society” (Crepeau, 2003, p. 28). Metacognitive strategy training (MST) addresses individual's awareness of their abilities and deficits, enabling them to employ effective problem-solving techniques and adaptive approaches to daily occupations and is recommended as a Practice Standard for brain injury rehabilitation (Cicerone et al., 2019). Importantly, literature suggests that PwPD have comparable cognitive symptom profiles and goals for rehabilitation to people with brain injuries (Vlagsma et al., 2016). Furthermore, the ability to use strategies to plan and problem-solve during complex task performance and monitor and evaluate ongoing performance is demonstrably impaired in PD (Sturkenboom et al., 2019). Therefore, MST interventions that target these performance problems may be effective in producing positive outcomes for PwPD. In recent years, MST targeting cognitive performance skills of PwPD have been trialled, with results indicating that MST may be effective in this population (Foster et al., 2018; Vlagsma et al., 2020). MST interventions comprehensively addressing the physical, cognitive and psychosocial performance problems experienced by PwPD have not yet been explored.
Cognitive Orientation to daily Occupational Performance (CO-OP) is “a client-centred, performance-based, problem-solving approach that enables skill acquisition through a process of strategy use and guided discovery” (Polatajko & Mandich, 2004, p. 2). CO-OP integrates functional skills practice and MST to address performance barriers that negatively affect participation and QoL. This is achieved in CO-OP by teaching problem-solving strategies to improve functional performance on client-chosen goals. CO-OP has demonstrated beneficial outcomes for adults with traumatic brain injuries (Dawson et al., 2009), stroke (McEwen, 2009), spina bifida, and cerebral palsy (Peny-Dahlstrand et al., 2020). Although there is growing evidence demonstrating positive outcomes using CO-OP with adult with neurological conditions (Saeidi Borujeni et al., 2019), the potential benefits for PwPD have not been explored. To investigate this potential, we conducted a feasibility randomized controlled trial (RCT) of the CO-OP approach for PwPD. We hypothesized that CO-OP would be feasible and that PwPD would experience improved performance on trained and untrained goals, improved perceived executive function, functional performance, self-efficacy, and QoL following CO-OP, which would be maintained at follow-up.
Method
Design and Setting
We conducted a parallel-group assessor-masked feasibility RCT in the homes of PwPD living in Greater Brisbane, Australia. Feasibility was explored using Bowen et al. (2009) framework. The detailed study procedures have previously been published (Davies et al., 2023). This research involved a person with PD as a consumer advisor to enhance the relevance and usefulness of the research to PwPD (Graham et al., 2018).
Participants
Participants were English-speaking adults with PD living independently in the community and able to participate in home-based intervention. Exclusion criteria included severe cognitive, psychiatric, or neurological disorders; significant sensory or communication impairments preventing study participation; complete dependence in personal care; and concurrent allied health intervention targeting the same goals.
Ethics and Registration
The study was approved by Research Ethics Committee of The University of Queensland (2020/HE002650) and registered in the Australian New Zealand Clinical Trials registry (ACTRN12621001483842).
Outcome Measures
Screening Assessment
The Telephone-Montreal Cognitive Assessment (T-MoCA; Pendlebury et al., 2013) was used to screen cognition via telephone prior to participant enrolment in the trial. To exclude those with probable dementia, potential participants who scored 13 or below on the T-MoCA were excluded from the study as recommended in Benge and Kiselica (2021).
Demographic and Disease Data
Demographic and disease data including age, sex, education level, work status, and disease duration were collected at baseline via an online Qualtrics survey. Data collected in person during the baseline assessment included pre-morbid intelligence, neuropsychological status, and disease severity. The National Adult Reading Test (NART; Nelson & Willison, 1991) was used to estimate the premorbid intelligence levels of participants. The Addenbrooke's Cognitive Evaluation III (ACE-III; Mioshi et al., 2006) was used to stratify participants by their cognitive status for randomization. The stratification groups were ‘no cognitive impairment’ (ACE-III score 100-89) and ‘mild cognitive impairment’ (ACE-III score 88-77) (Senda et al., 2020). The Modified Hoehn and Yahr (H&Y) scale (Hoehn & Yahr, 2011) was used to measure disease severity/stage. The H&Y scale is a 7-point Likert scale (1 = unilateral involvement only to 5 = wheelchair bound or bedridden unless aided) focused on overall PD severity based on disability and features of objective impairment (Poewe, 2012).
Feasibility Assessments
Aligned with Bowen et al. (2009) framework, feasibility aspects of acceptability, demand, adaptation, and preliminary efficacy were evaluated. Acceptability related to participant perceptions their effort in, and enjoyment of CO-OP. Participants rated their levels of effort and enjoyment in each session on a 6-point response scale (0 = None, 1 = A little, 2 = Some, 3 = Much, 4 = Very much, 5 = Extreme) with the interventionist present (Mohlman et al., 2011).
Demand related to how much demand for CO-OP existed. Demand was evaluated through documentation of homework completion rates and logistical information. Each homework assignment was judged as complete, partially complete, or did not do and scored 1, 0.5, or 0 points, respectively. These scores were summed and divided by the total number of homework assignments to yield a homework completion rate for each participant. Scheduling and cancellation of sessions and recruitment trends using the Screened, Eligible, Approached, Randomized framework (SEAR; Wilson et al., 2018) were also recorded to explore demand characteristics.
Adaptation related to the extent that the protocol was able to be delivered as intended to PwPD. Adherence to the CO-OP intervention protocol was evaluated with the CO-OP fidelity checklist (Chui et al., 2017). The CO-OP fidelity checklist identified and operationalized observable behaviours associated with the essential elements of CO-OP. It measured fidelity across sessions (part A1), fidelity within sessions (part A2) and general fidelity (part B). The treatment session was more like CO-OP as the part A1 and A2 scores approached 5 and more like Standard occupational therapy as the part A1 and A2 scores approached 0. Part B scores approaching 5 indicated good general treatment quality.
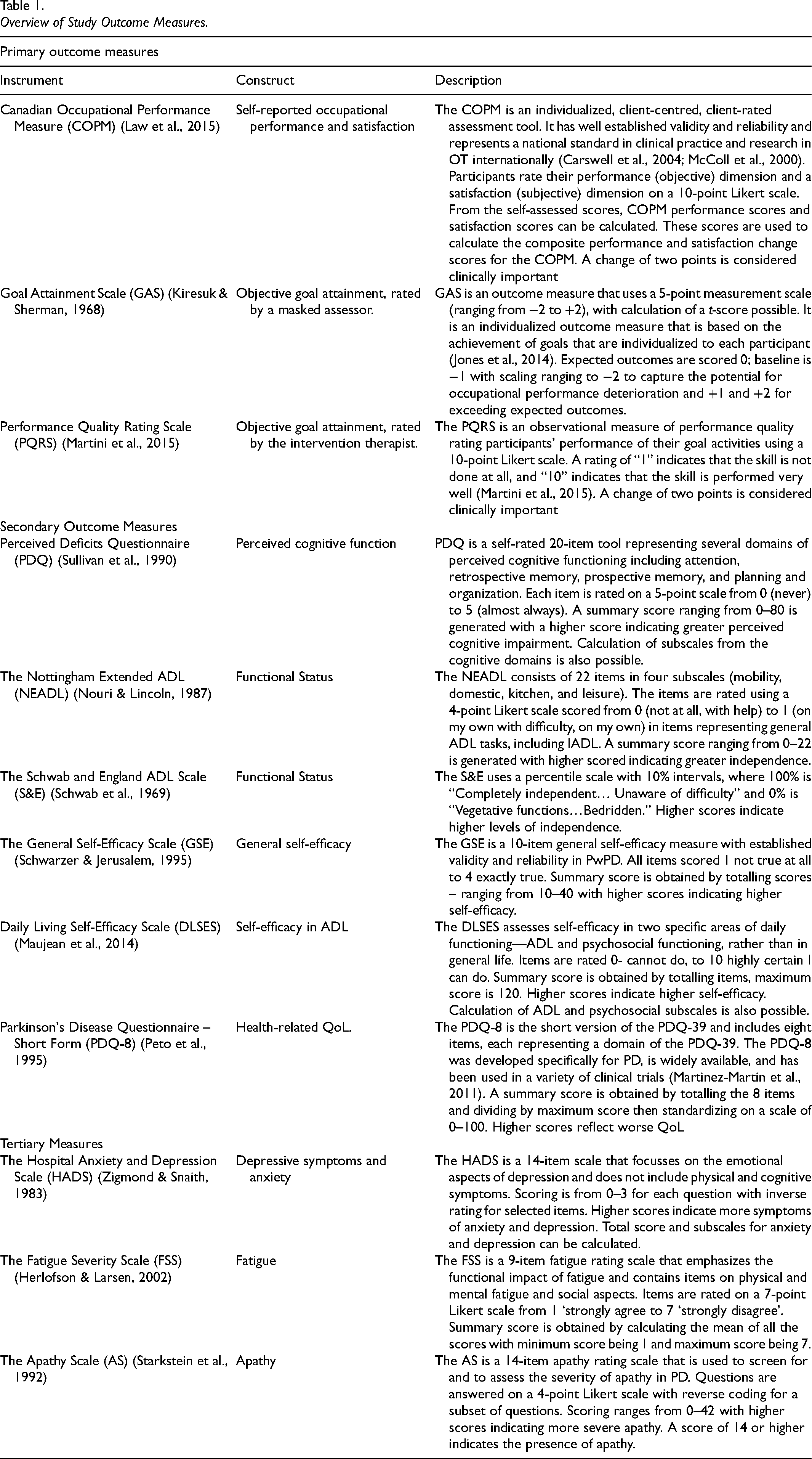
Preliminary efficacy testing was related to whether CO-OP demonstrated positive outcomes for PwPD in goal attainment, cognitive and functional status, QoL, self-efficacy, and transfer and maintenance of learned skills. Table 1 provides a full description of the primary, secondary and tertiary outcomes used in this study. The primary outcome measures related to goal attainment and measures included the Canadian Occupational Performance Measure (COPM; Law et al., 2015), Performance Quality Rating Scale (PQRS; Martini et al., 2015) and Goal Attainment Scale (GAS; Kiresuk & Sherman, 1968). The COPM and PQRS are linked to the scope of CO-OP (Kiriakou & Psychouli, 2024), the GAS was additionally included to enable standardized scoring and calculation of t-scores that allowed for statistical analysis (Kiresuk & Sherman, 1968). Secondary outcome measures related to cognitive and functional status, health-related quality of life (QoL), and self-efficacy. These constructs were measures with the Perceived Deficits Questionnaire (PDQ; Sullivan et al., 1990), Nottingham Extended Activities of Daily Living Scale (NEADL; Nouri & Lincoln, 1987), Schwab and England Scale (S&E; Schwab et al., 1969), General Self-efficacy Scale (GSE; Schwarzer & Jerusalem, 1995), Daily Living Self-efficacy Scale (DLSES; Maujean et al., 2014), Parkinson's Disease Questionnaire – Short Form (PDQ-8; Peto et al., 1995) and were administered at all timepoints via Qualtrics survey. Tertiary measures related to common symptoms of PD like apathy, fatigue, anxiety, and depression, and were included to explore their potential impact on the efficacy or feasibility of delivering the CO-OP approach and primary and secondary outcome attainment. They were administered at baseline via Qualtrics survey.
Overview of Study Outcome Measures.
Sample Size
Sample size calculation indicated that a minimum of 52 participants were required to achieve power of .90 to detect a medium effect size at p = .01; f = .25 (G*Power3; Faul et al., 2007), which allowed for 26 participants per group. We aimed to recruit a total of 60 participants (up to 30 per group) to allow for potential attrition. This was based on a conservative attrition rate of <15% based on previous experience recruiting to neurorehabilitation clinical trials, which have demonstrated sufficient power to detect change within a small pilot sample (Gullo et al., 2019).
Procedures
Participants were recruited via convenience sampling through Parkinson's Queensland Incorporated and word of mouth from March 2021 to June 2022, with the final follow-up sessions occurring in March 2023. Potential participants were initially contacted via telephone for eligibility and cognitive screening. Eligible participants were then emailed a Qualtrics survey before the intervention therapist conducted a home visit to complete baseline assessments and establish the program goals. Prior to full baseline assessment, study procedures were fully explained and written informed consent was obtained.
The goal setting interview was facilitated by the COPM. Participants selected four goals which they ranked in order of importance. Participants top three goals were targeted in the intervention. The fourth goal, which was the lowest ranked goal, was an untrained goal to assess transfer of skills learned in CO-OP. GASs for all COPM goals were established at baseline to enable objective measurement by a masked assessor, according to the reported procedure for combined use of the COPM and GAS (Doig et al., 2010). This involved identifying goals and problem areas, defining specific goal behaviours, determining measurement methods, setting performance expectations, specifying performance levels, and weighting goals for t-score calculations for each goal. Participant self-ratings of baseline goal performance and satisfaction were captured on the COPM, the PQRS captured objective baseline performance and was rated by the intervention therapist. Depending on the nature of the goal, therapist field notes, written logs, photographs, and/or video-recorded performance was captured to enable rating of GASs by the masked assessor.
Following baseline assessment and goal setting participants were randomly allocated to CO-OP or a waitlist control (WLC) group. Participants were randomized with a blocked 1:1 allocation, stratified by scores on the ACE-III, by a computer-generated randomization schedule. An independent, senior member of the research team created a computer-generated randomization schedule with concealment then allocated participants in chronological order from date of written consent.
Participants in the CO-OP group commenced the 10-week intervention immediately post-randomization. Participants allocated to the WLC had a 10-week non-intervention period. Post-test assessment was conducted for both groups immediately following the 10-week period. The online survey was emailed to participants. A home visit was conducted to capture post-intervention/WLC goal performance on the COPM, PQRS and GAS. The CO-OP group were assessed a third time three-months post-intervention, using the same procedures as earlier time points. In line with the published protocol (Davies et al., 2023), the WLC group did not receive an assessment at the follow-up timepoint as the WLC group subsequently received the CO-OP intervention at a different intensity after their non-intervention period.
A qualified occupational therapist who was masked to treatment condition and was not involved in the delivery of the intervention assessed goal performance on the GAS. The masked assessor underwent training prior to completing the GAS ratings for the RCT by reviewing and rating GASs, using related measurement evidence (de-identified) from a prior study (Doig et al., 2010). The GAS inter-rater reliability was established following GAS training for a subset of study goals (n = 12, 15%). These goals were independently rated by the masked assessor and a senior member of the research team who is an experienced GAS user. Thereafter, the masked assessor proceeded with rating the remaining sample of GAS goals independently.
Intervention
The CO-OP intervention was carried out one-to-one by a CO-OP-certified occupational therapist in participants' home environments. The intervention group received 20 one-hour sessions over 10-weeks (2 sessions/week) based on the adapted intensive protocol (Dawson et al., 2017). The intervention focused on the three highest ranked goals identified by the participant during goal setting.
Influence of Coronavirus Disease of 2019 (COVID-19)
Australia implemented an elimination strategy to manage the COVID-19 pandemic (Stobart & Duckett, 2022). This included strict measures including lockdowns, mandatory mask-wearing, mandatory isolation periods for close contacts of infected persons or upon infection, and a vaccination program. This study was conducted during the pandemic, so all procedures followed strict infection control guidelines. These included health checks for participants and staff, including evidence of participant's vaccination status, protective equipment worn by the treating therapist (mask, eye protection, gloves and apron) during treatment sessions, and temporary cessation of research activities during periods of high community transmission. As a result, all participants experienced University-initiated research closures that caused interruptions or delays in their treatment plans or recruitment to the study.
Data Analysis
Feasibility data were extracted from therapist field notes to Microsoft Excel before being analyzed descriptively. Survey data were cleaned and checked for accuracy prior to conducting analysis using IBMStatistical Package for the Social Sciences (SPSS; Version 21; IBM Corporation, Armonk, NY). Normal distribution of the data was verified using the Shapiro–Wilk test (Shapiro & Wilk, 1965). Independent sample t-tests were conducted to investigate systematic differences in baseline characteristics between groups to identify potential co-variates for inclusion in the main analysis. Goal attainment data were extracted from the COPM, PQRS and GAS into SPSS. A series of 2 × 2 (Treatment × Time) mixed between-within analysis of variance tests (ANOVA) were planned based on the published protocol (Davies et al., 2023) to compare the CO-OP group with WLC to determine preliminary efficacy (Time: pre, post) on primary and secondary outcomes. Participants were analyzed according to intention to treat (Detry & Lewis, 2014). This analysis approach includes every subject who is randomized based on the treatment assignment regardless of non-compliance, protocol deviations, withdrawal, and anything that occurs after randomization.
To detect clinically important change on the COPM and PQRS composite scores were used for trained goals at all timepoints. Clinically important changes were defined as a change of two or more points in composite scores (Law et al., 2015; Martini et al., 2015). The scores for the fourth goal on the COPM and PQRS were used in analysis of the untrained goal. The GAS level of attainment (−2 to 2) for each participant was converted into t-scores using the published conversion equation (Turner-Stokes, 2009) and the t-score was used in the statistical analysis. With only one goal in the untrained goal GAS analysis, there was no intercorrelation between goals or weighting of goals so a simplified GAS formula [GAS = 50 + (10x)] was used, where x is the GAS raw score. This method for analyzing one-goal GAS has been demonstrated to be responsive to change (McGarrigle et al., 2019). Goal attainment outcomes were also descriptively analyzed using independent t-tests that compared means for both groups. The COPM and PQRS composite scores for trained goals and individual scores for untrained goals were subsequently tabulated by frequency of clinically important change.
Results
Participants
The final sample comprised 20 PwPD. Table 2 displays participant characteristics. There were no significant differences detected between groups on key characteristics of age (p = .50), disease duration (p = .61), cognitive status (p = .71), functional status on the NEADL (p = .66), pre-morbid intelligence (p = .33), or disease severity (p = .93) at baseline. Participants in both groups met the criteria for severe fatigue (CO-OP M = 4.68; SD = 0.98; WLC M = 4.51; SD = 1.23) (Nordin et al., 2016) and apathy (CO-OP M = 16.77; SD = 3.49; WLC M = 14.61; SD = 4.40) (Starkstein et al., 1992) at baseline. Thirty percent of participants were H&Y stage three, indicating “mild to moderate bilateral disease; some postural instability; physically independent.”
Participant Characteristics.
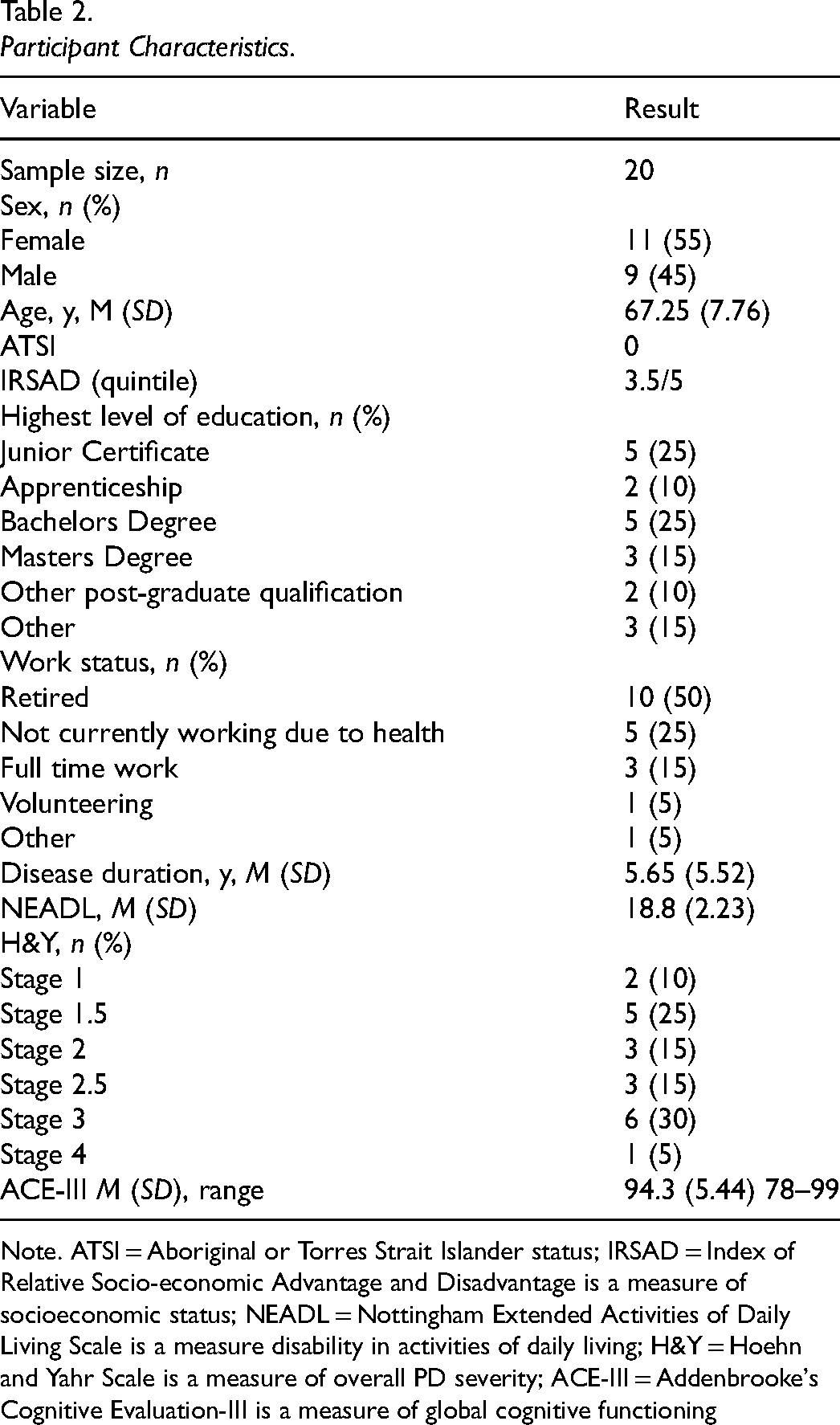
Note. ATSI = Aboriginal or Torres Strait Islander status; IRSAD = Index of Relative Socio-economic Advantage and Disadvantage is a measure of socioeconomic status; NEADL = Nottingham Extended Activities of Daily Living Scale is a measure disability in activities of daily living; H&Y = Hoehn and Yahr Scale is a measure of overall PD severity; ACE-III = Addenbrooke's Cognitive Evaluation-III is a measure of global cognitive functioning
Feasibility
Acceptability
The mean effort and enjoyment ratings were 3.02/5 and 3.15/5, respectively, which equated to ‘much’ effort, and also ‘much’ enjoyment on the Likert scale. Approximately 71% of effort ratings were ≥3/5, and 75% of enjoyment ratings were ≥3/5.
Demand
A Consolidated Standards of Reporting Trials (CONSORT; Bennett, 2005) diagram depicts participant flow through the study (Figure 1). A total of 20 adults (11 females and 9 males) were randomized, once randomzsed and the intervention was commenced, no participants from either group were lost from the study.
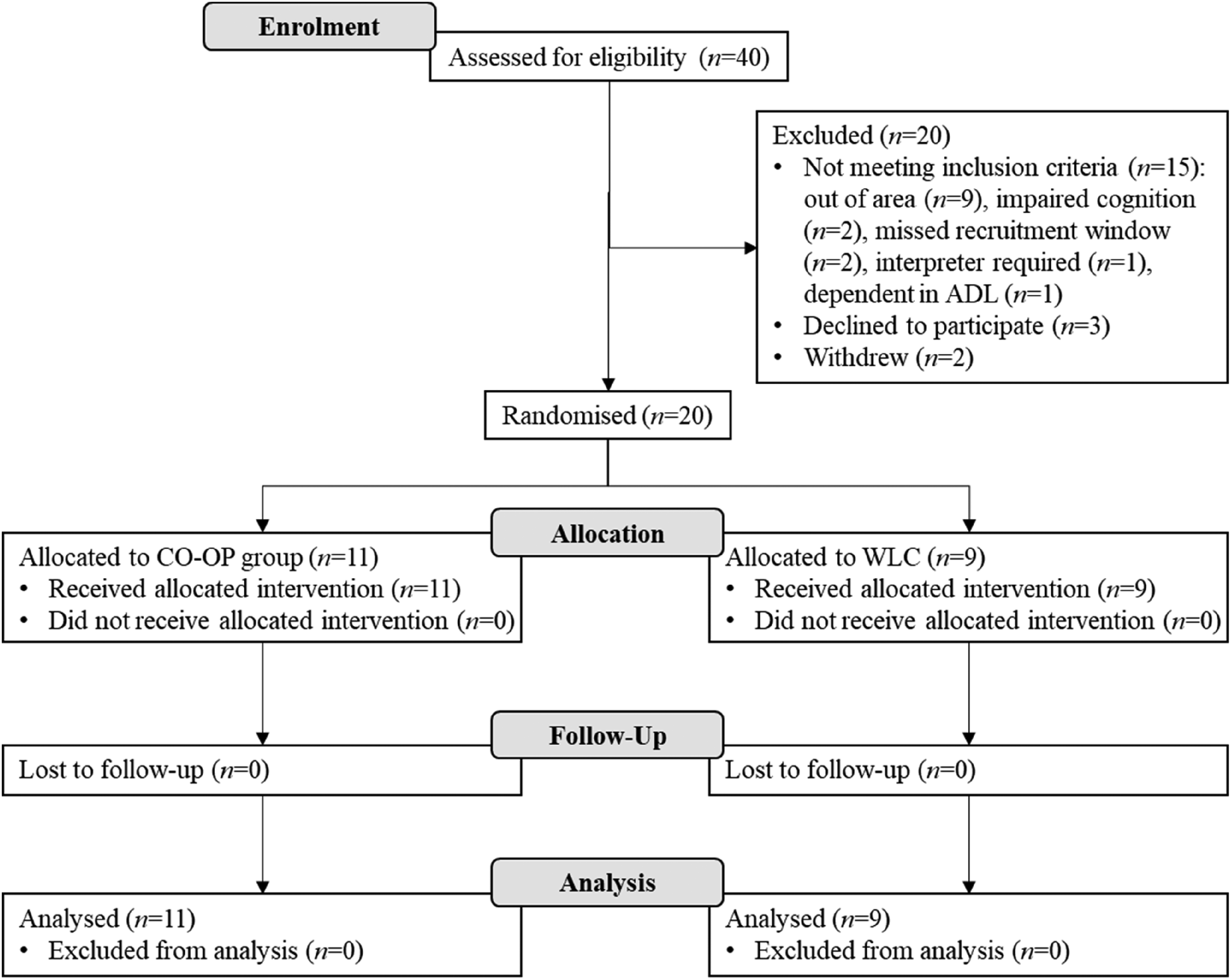
CONSORT flowchart of participants.
Homework completion rates ranged from 50% to 100% (M = 91%, SD = 15%). The percentage of prescribed CO-OP sessions that were fully completed ranged between 55% (11/20 sessions) and 100% (20/20 sessions), (M = 82%, SD = 14%). All non-completions were due to illness, COVID-19 lockdowns, pre-planned holidays, bereavement, and/or natural disasters.
Adaptation
The mean scores for parts A1, A2 and B on the CO-OP fidelity checklist were 5/5 indicating that the sessions had excellent adherence and compliance to the CO-OP approach within and across sessions and high general fidelity with the CO-OP approach.
Preliminary Efficacy Testing
Data was missing from the sample due to unit non-response in survey data. Baseline demographic information and goal attainment data collected in person was not affected. Little's Missing Completely at Random (MCAR) test (Little, 1988) was conducted on the cleaned datafile prepared for analysis and found to be non-significant (CO-OP versus WLC efficacy χ 2 [44] = 19.21, p > .99) indicating data was missing completely at random. Multiple imputations approach recommended by Rubin (1976) was applied, the gold standard to handling missing data (Graham, 2009), and pooled results from twenty imputations were used as the basis of further analysis. Independent t-tests were conducted on baseline measures of apathy, fatigue, anxiety, and depression to check if any needed to be included as co-variates in the main analysis. Significant between group differences were seen in baseline anxiety scores as measured on the HADS Anxiety Subscale (p = .0158).
Intended repeated measures analysis using ANOVA were unable to be conducted as this approach cannot be implemented in SPSS when missing data has been addressed with multiple imputation due to a lack of pooled effects (van Ginkel & Kroonenberg, 2014). A modified approach involving a series of multiple regression analyses controlling for baseline performance at timepoint one to test whether the CO-OP treatment group predicted differential change on key measures was employed (van Ginkel & Kroonenberg, 2014). Anxiety was subsequently included in the multiple regression analysis to control for differences at baseline. The GAS inter-rater reliability kappa score was 0.788 (p = .001) indicating large effect (Twisk, 2014).
Primary Outcomes
Regression analysis detected significant between group differences in COPM performance, COPM satisfaction and PQRS scores as presented in Table 3. This may indicate that CO-OP was superior to the WLC for achievement of trained goals. For untrained goals, significant between group differences were detected on COPM satisfaction and PQRS. No significant differences were observed for trained or untrained goals according to the masked assessor rated GAS.
Regression Analysis of Treatment Group Predicting Post-Test Scores for Primary Outcomes.
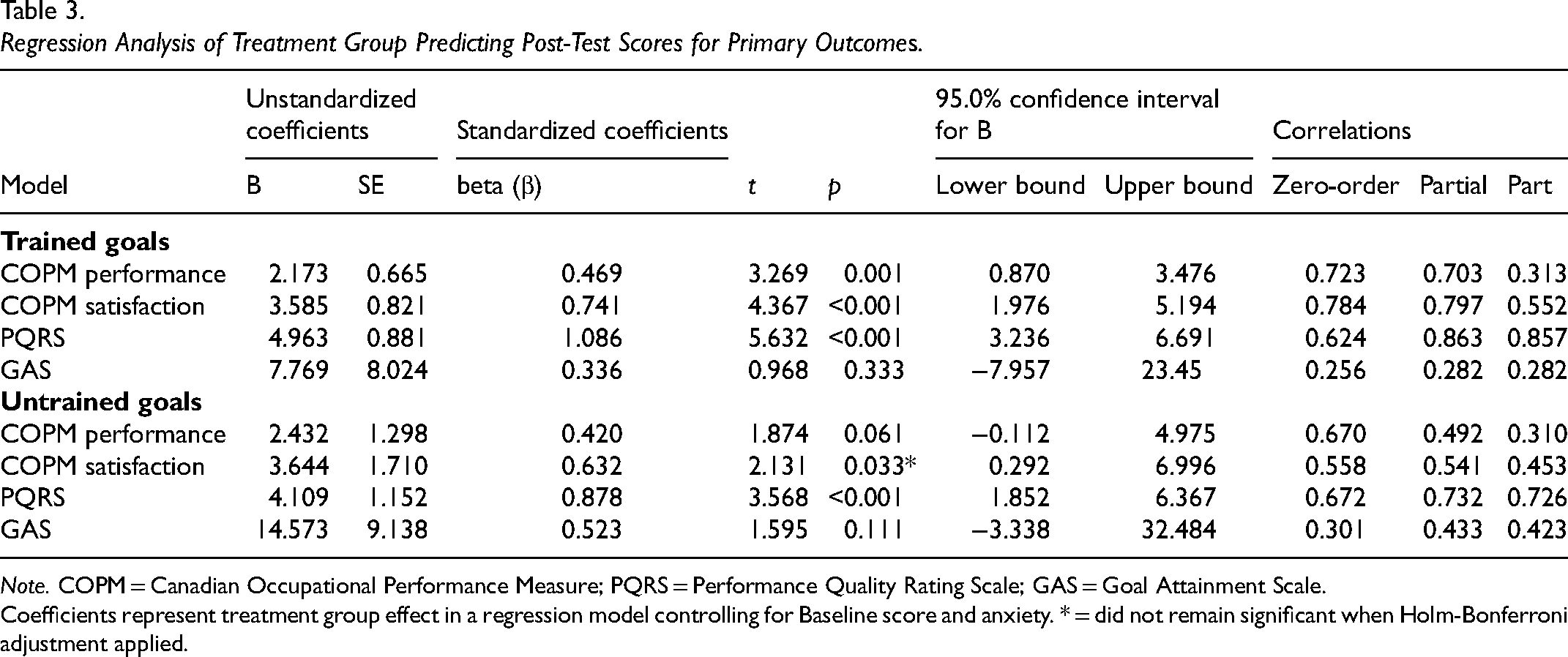
Note. COPM = Canadian Occupational Performance Measure; PQRS = Performance Quality Rating Scale; GAS = Goal Attainment Scale.
Coefficients represent treatment group effect in a regression model controlling for Baseline score and anxiety. * = did not remain significant when Holm-Bonferroni adjustment applied.
The mean change scores and level of clinically important goal achievement for the CO-OP and WLC groups, and the mean change scores and level of clinically important achievement for the CO-OP group from pre-intervention to the follow-up timepoint are presented in Table 4.
Mean Change Scores on Primary Outcomes and Comparison Level of Attainment Within Groups Post-Test and at Follow-up.
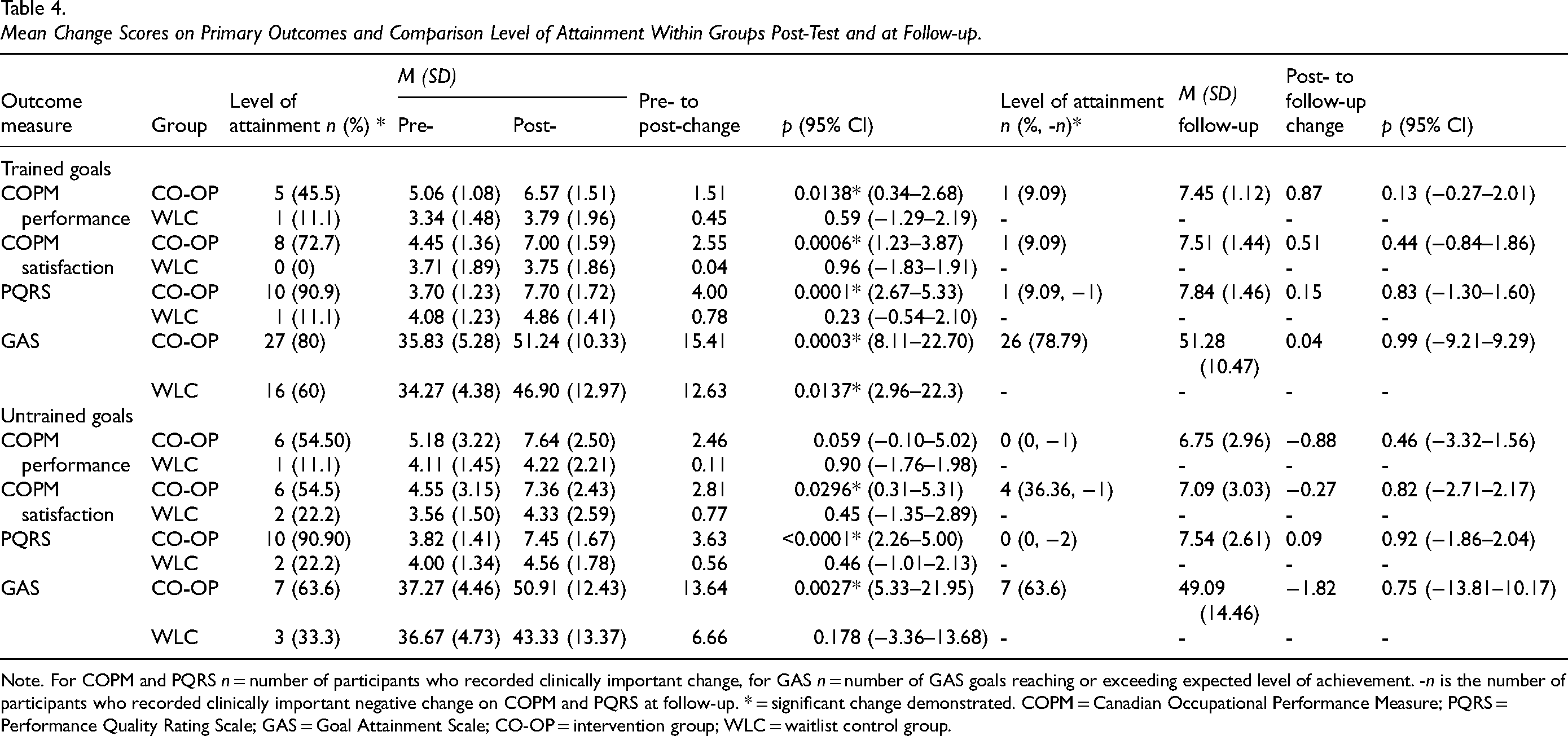
Note. For COPM and PQRS n = number of participants who recorded clinically important change, for GAS n = number of GAS goals reaching or exceeding expected level of achievement. -n is the number of participants who recorded clinically important negative change on COPM and PQRS at follow-up. * = significant change demonstrated. COPM = Canadian Occupational Performance Measure; PQRS = Performance Quality Rating Scale; GAS = Goal Attainment Scale; CO-OP = intervention group; WLC = waitlist control group.
Significant increases in mean scores were detected in the within group analysis on the COPM, PQRS and GAS for trained goals from pre- to post-intervention in the CO-OP group. On the GAS, the WLC group also demonstrated significant change from pre- to post-intervention for trained goals. For untrained goals, the CO-OP group demonstrated significant improvements on the COPM satisfaction, PQRS and GAS but not COPM performance. At follow-up, the CO-OP group COPM and PQRS scores indicated that goal achievement had been maintained for trained goals. For untrained goals at follow-up, results indicated that there was a non-significant reduction in COPM, PQRS, and GAS mean scores.
Secondary Outcomes
The regression analysis predicting post-intervention differences between groups for secondary outcomes did not reach significance in measures of cognitive (p = .693) and functional (NEADL p = .441; S&E p = .750) status, QoL (p = .163), or self-efficacy (GSE p = .317; DLSES p = .867). Within group analysis also indicated that change was not significant for any of the secondary outcomes. A mean minimally important change >0.37 points was detected on the GSE for the CO-OP group (M = 1.86) which may indicate clinically important improvements in self-efficacy following CO-OP (Ohno et al., 2017). The mean change score on the PDQ-8 was 5.07 in the CO-OP group post-intervention. A change ≥ 4.9 points indicated clinically important worsening of QoL on this measure (Horváth et al., 2017).
Discussion
This was the first RCT investigating the use of CO-OP for PwPD. Supporting our hypothesis, we found that CO-OP was a feasible and potentially beneficial approach as evidenced by improved performance on trained and untrained goals, which was maintained for the CO-OP group at follow-up. Functional and cognitive status and QoL results did not support our hypothesis that these outcomes would be improved following CO-OP. However, self-efficacy results indicated improved self-efficacy following CO-OP.
Previous research supports the feasibility of MST in PD (Alzahrani & Venneri, 2018; Foster et al., 2018; Vlagsma et al., 2020). Our findings similarly indicate that CO-OP was a feasible approach. Unlike prior studies focused on cognitive performance skills, this research took broad rehabilitation focus to explore the potential of CO-OP to holistically meet the diverse needs of PwPD. We found participants identified mainly activity and participation level goals across a broad range of occupational domains (Davies et al., 2024a). This study build on those findings by exploring CO-OP's preliminary efficacy in this population. We have also reported on participants perspectives of the CO-OP intervention (Davies et al., 2024b). This research suggested that CO-OP was perceived by PwPD as a positive experience that improved their management of daily life, self-awareness, and self-efficacy. Our qualitative results supported CO-OP as an implementable, acceptable, and potentially beneficial intervention for people with PD, in keeping with the quantitative findings presented here. (Davies et al., 2024b)
Demand for the CO-OP intervention was high, as indicated by recruitment and retention rates, and high rates of homework and appointment completion. The COVID-19 pandemic impacted on recruitment and intervention delivery so rates of appointment completion should be interpreted in this context. Participant reported high levels of effort and enjoyment during CO-OP, alongside their high homework completion rates. Engagement is positively associated with functional outcomes (Foster et al., 2018; Rees et al., 2005), these findings suggest engagement with CO-OP was sufficient to produce positive outcomes if CO-OP is truly effective. Conversely, apathy and fatigue are negatively associated with participation and engagement (O'Brien et al., 2016) and were prevalent in this sample. Despite this, CO-OP had high levels of acceptability and demand. This suggests that CO-OP was feasible even in the presence of these common PD symptoms. It is possible that structural features of CO-OP may have enhanced engagement for PwPD experiencing apathy and fatigue. Protocol adherence was confirmed with high fidelity ratings, suggesting that it is possible to deliver the CO-OP intervention in this population, even in the presence of symptoms that may influence engagement.
Preliminary efficacy testing indicated that CO-OP produced positive change in trained and untrained goals, with broader effects seen for trained goals. Whilst person-centred goal setting was implemented and CO-OP includes structural features to promote generalization and transfer, it is possible that the lower rank of the untrained goal may have influenced participant's motivation in working towards these goals (Smit et al., 2019) and the consequent attainment of untrained goals. Positive changes were seen in subjective and objective goal performance measures along with masked assessor rated goal attainment outcomes, adding reliability to the findings (Kiriakou & Psychouli, 2024). Our results suggested that the CO-OP group showed greater statistical and clinical achievement of program goals as measured by the COPM and PQRS than the WLC group. The GAS results are more complex to interpret given that statistically significant results were only seen in the mean changes scores within groups. This is likely because participants in the WLC demonstrated significant mean changes scores on the GAS in the absence of the intervention. The therapeutic contribution of goal setting and monitoring goals (Harkin et al., 2016) has been discussed in previous literature and comparable results in goal attainment between intervention and non-intervention groups measured using GAS have been reported (Herdman et al., 2019). It is possible that the procedures for goal setting and monitoring of goals produced those results in the WLC group, but the difference between the WLC group and the CO-OP group is attributable to the CO-OP intervention. This highlights the importance of control groups in rehabilitation research along with evaluation of clinically important changes and triangulation of findings with subjective and objective assessment of primary outcomes. Employing multiple measures of goal attainment was considered a strength of this research as it allowed participant, therapist and masked assessor ratings of goal attainment. We decided to use multiple measures because we anticipated that various sources of evidence would be needed to evaluate goal-related performance and were concerned that the COPM and PQRS alone would not enable evaluation for all goal types. Particularly as the psychometric properties of PQRS for participation, time management, and organization goals relying on log and photo-based evidence for their rating by a masked assessor have not yet been established. This is why we incorporated the GAS, as it provided a means of having masked, objective assessment, overcoming limitations of the potential bias of determining outcomes using patient self-ratings and ratings of the therapist who delivered the intervention (and was unmasked to allocation) alone. However, using the GAS was time consuming, didn’t allow recognition of partially achieved goals, and was impacted by external factors such as cessation leisure activities during the Christmas period. The PQRS and COPM weren’t affected by these factors which increases the feasibility of using these measures in future research. Establishing the psychometric properties of the PQRS for novel goal types, using novel sources of evidence may also be warranted.
Previous Reviews Have Suggested That CO-OP Appears to Have a Positive Impact on activity performance, cognitive strategy use, and generalization and transfer (Cantin et al., 2024; Jacob et al., 2020; Kiriakou & Psychouli, 2024; Madieu et al., 2023; Roostaei et al., 2022). Each of the reviews concluded that there is still a need for large scale trials, with homogenous comparison groups and adequate power. While preliminary efficacy of CO-OP for PwPD showed similarly promising results, these findings are based on small numbers and are consequently interpreted in this light. Even though we only recruited one-third of the participants we originally planned, considering the challenges we faced due to COVID-19 lockdowns, disruptions to the intervention, and increased anxiety among potential participants (Soilemezi et al., 2023), our recruitment and retention rate is still a good sign. It suggests that we could successfully recruit a larger number of participants for a bigger trial in the future.
Unfortunately, significant between groups differences were not observed for secondary outcomes related to cognitive or functional status, QoL, or self-efficacy. Baseline scores on the functional status measures were already very high, likely because of the study inclusion criteria, which may have produced a ceiling effect. The improvement in self-efficacy alongside a reduction in QoL is paradoxical but is interpreted cautiously due to small study numbers. The COVID-19 pandemic's negative impact on global QoL (Violato et al., 2023) might explain a general decline in this study. However, the specific worsening in the CO-OP group suggests another factor. Increased self- and disease-awareness following the intervention, which has been associated to lower QoL in other chronic illnesses (Venkataraman et al., 2014), could be a potential explanation.
Limitations
While an RCT format was utilized, the reduced power of this feasibility study limits our ability to draw broader conclusions regarding efficacy of CO-OP for PwPD. The study also included a small, culturally homogeneous sample of community-dwelling individuals who were independent in activities of daily living and had high education levels. Therefore, the findings may be less representative of a broader population of PwPD or people with more severe PD. Due to missing data in self-report measures it is recommended that future studies have suitable support to reduce the likelihood of missing data from occurring.
Conclusion
As the first RCT focused on CO-OP for PwPD, exploring feasibility of the approach is an important initial phase potentially laying the foundation for future large-scale trials. We have shown that CO-OP is feasible to implement, acceptable to PwPD, and promising in terms of its preliminary efficacy for attainment of personally meaningful goals. The potential long-term impact of this work is an implementable intervention approach that comprehensively addresses the daily performance challenges experienced by PwPD across a broad range of performance domains.
Key Messages
This research has demonstrated that CO-OP is a feasible, acceptable and implementable approach for people with Parkinson's disease (PwPD) that may result in improved performance in trained and untrained goals. Further research is required to further establish the efficacy of CO-OP for PwPD, including the impact of the approach on self-efficacy and quality of life outcomes.
Footnotes
Authors’ Note
The views expressed in the submitted article are the authors’ own and not an official position of the institutions or funders.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an Australian Government Research training Program (RtP) scholarship and by Parkinson’s Queensland Incorporated through a PhD award.