
Abstract
Introduction
Engaging in age-appropriate, enjoyable physical activity, limiting sedentary screen time, and attaining an adequate amount of sleep have been associated with positive physical, socio-emotional, and cognitive development among preschool-aged children (Carson et al., 2017; Chaput et al., 2017; Poitras et al., 2017). The Canadian 24-Hour Movement Guidelines for the Early Years (herein referred to as the 24-Hour Movement Guidelines; Canadian Society for Exercise Physiology [CSEP], 2017) suggest that preschool-aged children (3–4 years) should accumulate 180 min of physical activity (including 60 min of energetic play); not be restrained for more than 1 hr at a time; limit sedentary screen time to less than 1 hr; and, get 10–13 hr of sleep (including naps) each day (Tremblay et al., 2017).
The Canadian Society for Exercise Physiology (CSEP) has indicated that the 24-Hour Movement Guidelines can be used for children with disabilities under the advisement of a healthcare professional (CSEP, 2017); however, research indicates that children with disabilities are less likely to meet these recommendations than their peers without disabilities due to physical, social, and environmental barriers (Arbour-Nicitopoulos et al., 2021; Healy et al., 2020). In a qualitative study by Handler et al. (2019), mothers (n = 15) of children with disabilities discussed the Canadian 24-Hour Movement Guidelines for Children and Youth (aged 5–17 years), which builds on the recommendations for preschoolers. These mothers noted that they generally valued the movement guidelines and had no issue with the recommendation doses (i.e., frequency, intensity, time, type); however, they felt the guidelines failed to provide clear information and to acknowledge/accommodate inter-individual and inter-disability needs and differences. While more research is required before specific recommendations for preschool-aged children with disabilities can be developed (Taylor et al., 2023b), occupational therapists (OTs), could play an important role in adapting the current 24-Hour Movement Guidelines to better suit the needs of children with disabilities.
Healthcare professionals, including OTs, have been identified as key disseminators of the 24-Hour Movement Guidelines and crucial for supporting their clients’ movement behaviours (Faulkner et al., 2016; Latimer-Cheung et al., 2016). This includes supporting movement behaviours through assessment, counselling behaviour change, prescribing, and referring (Fowles et al., 2018). Moreover, parents have reported healthcare practitioners are trustworthy sources for communicating the guidelines (Riazi et al., 2017). OTs are well-positioned to support the implementation of these guidelines given their focus on participation and engagement for young children with disabilities. Specifically, a critical aspect of the work of pediatric OTs is to support the participation of children with disabilities in important childhood occupations such as movement-based play and sleep (Case-Smith, 2013). At an individual child level, OTs can use adaptation and graded activity participation to support the engagement of preschoolers with disabilities in these meaningful occupations. This can include addressing barriers to participation and modifying the recommendations to support diverse abilities, which could help to address concerns with implementing the 24-Hour Movement Guidelines (D’Arrigo et al., 2020; Handler et al., 2019). Although some OTs have reported using movement behaviours in their clinical practice (Hill et al., 2022; Taylor et al., 2023a), Handcock and Tattersall (2012) note that many may lack the expertise to interpret, explain, modify, and employ the recommendations. Therefore, supporting the capacity of OTs to implement the 24-Hour Movement Guidelines is critical (Latimer-Cheung et al., 2016).
Despite the role OTs could play in supporting the integration of the 24-Hour Movement Guidelines, it is unclear whether OTs working with young children with developmental disabilities are aware of the guidelines, and if their knowledge, agreement, and external factors align with implementation in practice. The Knowledge, Attitudes, Behaviour Framework is well accepted in the scientific literature as an approach to understanding and addressing perceived barriers for healthcare practitioners to implement clinical guidelines (Cabana et al., 1999; Fischer et al., 2016). This framework suggests that behaviour (i.e., implementation of guidelines) is shaped by internal factors of the healthcare practitioner and external factors in their environment
The primary purpose of this study was to describe the internal and external factors influencing the incorporation of the 24-Hour Movement Guidelines in practice by pediatric OTs when working with young children (aged 3–4 years) with developmental disabilities (e.g., a variety of conditions that, in combination with environmental factors, can impair physical, cognitive, language, behaviour and/or learning functions; Zablotsky et al., 2019). The secondary purpose was to explore the impact of OT education level and years of practice on perceived internal and external factors influencing the implementation of the 24-Hour Movement Guidelines in practice. The aim of this line of inquiry is to increase our understanding of the factors influencing the ability of OTs to implement the movement behaviour recommendations and support future dissemination and intervention activities to incorporate the 24-Hour Movement Guidelines in occupational therapy.
Method
All procedures for this cross-sectional, exploratory study were approved by Western University's Health Sciences Research Ethics Board (REB #121341) and informed consent was obtained from all participants prior to data collection.
Recruitment and Participants
OTs in Canada were recruited via emails circulated by the Canadian Association of Occupational Therapists (CAOT) and provincial regulatory bodies to registered OTs. The study was also shared on CAOT's research listing website, on social media, with professional networks, and via occupational therapy special interest group leaders in Canada. Interested OTs were required to email the research team and provide their registration number, which was verified in the college directories. OTs were eligible to participate if they: (1) were currently registered with a Canadian occupational therapy regulatory body and able to practice in Canada; (2) had self-reported experience working with children aged 3–4 years with developmental disabilities; (3) were able to read and write in English or French; and (4) had access to the internet.
Data Collection
Data collection took place via a single online survey administered on Qualtrics. Eligible participants were sent a survey link and a password and were able to self-select their preferred language (English or French). Participants provided demographic information and data pertaining to their personal movement behaviours. Participants were then asked to review the 24-Hour Movement Guidelines before completing the remainder of the online survey.
Measures
Participant Demographics
Participants reported their location of practice (province), education (degree type), and years of experience as an OT. Participants were also asked to provide their gender and race, given their known correlations with physical activity (e.g., Choi et al., 2017).
Clinical attitudes toward physical activity implementation in practice have been associated with health professionals’ own physical activity participation (Lobelo et al., 2009). Therefore, the International Physical Activity Questionnaire-Short Form (IPAQ-SF; 7 items) was used to determine participants’ self-reported adherence to the Canadian 24-Hour Movement Guidelines for Adults (150 min of moderate to vigorous physical activity per week, limiting sedentary behaviour to 8 hr per day or less, with no more than 3 hr of recreational screen time, and 7–9 hr of sleep per night; CSEP, 2020; Ross et al., 2020). The IPAQ-SF is a valid and reliable measure of physical activity (types and intensity) and sitting time (average/day) that people do as part of their daily lives (Craig et al., 2003). The section evaluated participants’ self-reported physical activity and sedentary time, with one question added to collect sleep duration (i.e., During the last 7 days, how many hours did you spend sleeping per night on average?).
Internal and External Guidelines Implementation Factors
The Clinician Guideline Determinants Questionnaire (n = 51 items), a validated tool that investigates internal (knowledge, n = 4; attitudes, n = 18) and external (guideline-, client-, and environmental-related, n = 20) factors shaping guideline implementation behaviour was employed (Gagliardi et al., 2019). The self-efficacy of healthcare professionals in the promotion of movement has been associated with the use of movement strategies in practice (Crisford et al., 2018). Therefore, self-efficacy was determined to be an important internal factor to explore beyond the two questions provided in the Clinician Guideline Determinants Questionnaire (i.e., “I am confident that I possess the skills needed to use the recommendations; I have the autonomy to make changes needed to follow the recommendations”). Thus, 15 additional items were added and adapted from the Early Childhood Educator Confidence in Outdoor Movement, Physical Activity, and Sedentary and Screen Behaviours (ECE-COMPASS) questionnaire to assess the self-efficacy of OTs relevant to the 24-Hour Movement Guidelines (Bruijns et al., 2023). Validated for use with early childhood educators, the ECE-COMPASS was used in this study due to the lack of an existing tool to assess the self-efficacy of OTs to implement movement behaviours with preschoolers. Questions from the survey focused on physical activity and were re-worded to ask the same questions relevant to sedentary behaviour and sleep. ECE-COMPASS items were rated on a scale of 0–100 and were not added to the internal factor items measured with the Clinician Guideline Determinants Questionnaire due to incompatibility of scoring; these scores were examined independently.
Data Analysis
The Statistical Package for the Social Sciences (SPSS version 29; IBM, 2022) was used for data preparation and analysis. Descriptive statistics were conducted to explore demographic factors and the internal (knowledge, attitudes) and external (guideline-, client-, and environmental-related) factors. Descriptive means were maintained in their original form and presented as a score out of 5. Frequencies measured with 5-point Likert scores (1 = strongly disagree to 5 = strongly agree) were re-scored into three summary categories of disagree, neither agree/disagree, and agree, in line with recommendations from Percy (1976) when working with small sample sizes. The Clinician Guideline Determinant Questionnaire 5-point Likert scales were collapsed into continuous variables (Allen & Seaman, 2007), representing a single 5-point score for knowledge, attitudes, and external factors.
Independent sample t-tests were used to examine the relationship between OT education levels (i.e., undergraduate- and graduate-level) and guideline implementation factors. The Pearson correlation coefficient was used to explore the relationship between years of practice and the guideline implementation factors. Scores on knowledge factors were significantly skewed (i.e., >1.50), therefore nonparametric alternatives were used with this outcome (Pallant, 2016).
A combined physical activity variable for OTs was computed by multiplying the number of physically active days by the total minutes spent engaged in each intensity, and by the corresponding metabolic equivalent value, before summing the participants’ total scores (Craig et al., 2003). Time spent sitting and sleeping were reported in minutes per 24-hr period. Median scores, standard deviations, and proportions were used to evaluate the movement behaviours of OTs (Craig et al., 2003). Self-reported adherence to the Canadian 24-Hour Movement Guidelines for Adults was represented as categorical variables (1 = met; 0 = did not meet) based on median participant scores for physical activity, sedentary behaviour, and sleep.
Self-efficacy items measured on the ECE-COMPASS (n = 15) were re-scored into six summary categories based on question themes (Percy, 1976), and provided as an average out of 100, where 0 meant “not confident at all” and 100 meant “completely confident” (Bandura, 2006).
Results
Participants (n = 28) were registered to practice in 7 of 13 provinces and territories in Canada. All identified as women (including trans-women), and most reporting being white (n = 21; 75%). The majority of participants noted that their highest level of occupational therapy-related education was a master's degree (n = 17, 61%), with 17.29 years of practice (SD = 11.31) and 15.30 years of practice in pediatrics specifically (SD = 11.30). Most participants reported meeting each of the physical activity, sedentary behaviour, and sleep guidelines as per the Canadian 24-Hour Movement Guidelines for Adults. See Table 1 for participant demographic characteristics.
Participant Demographics (n = 28).
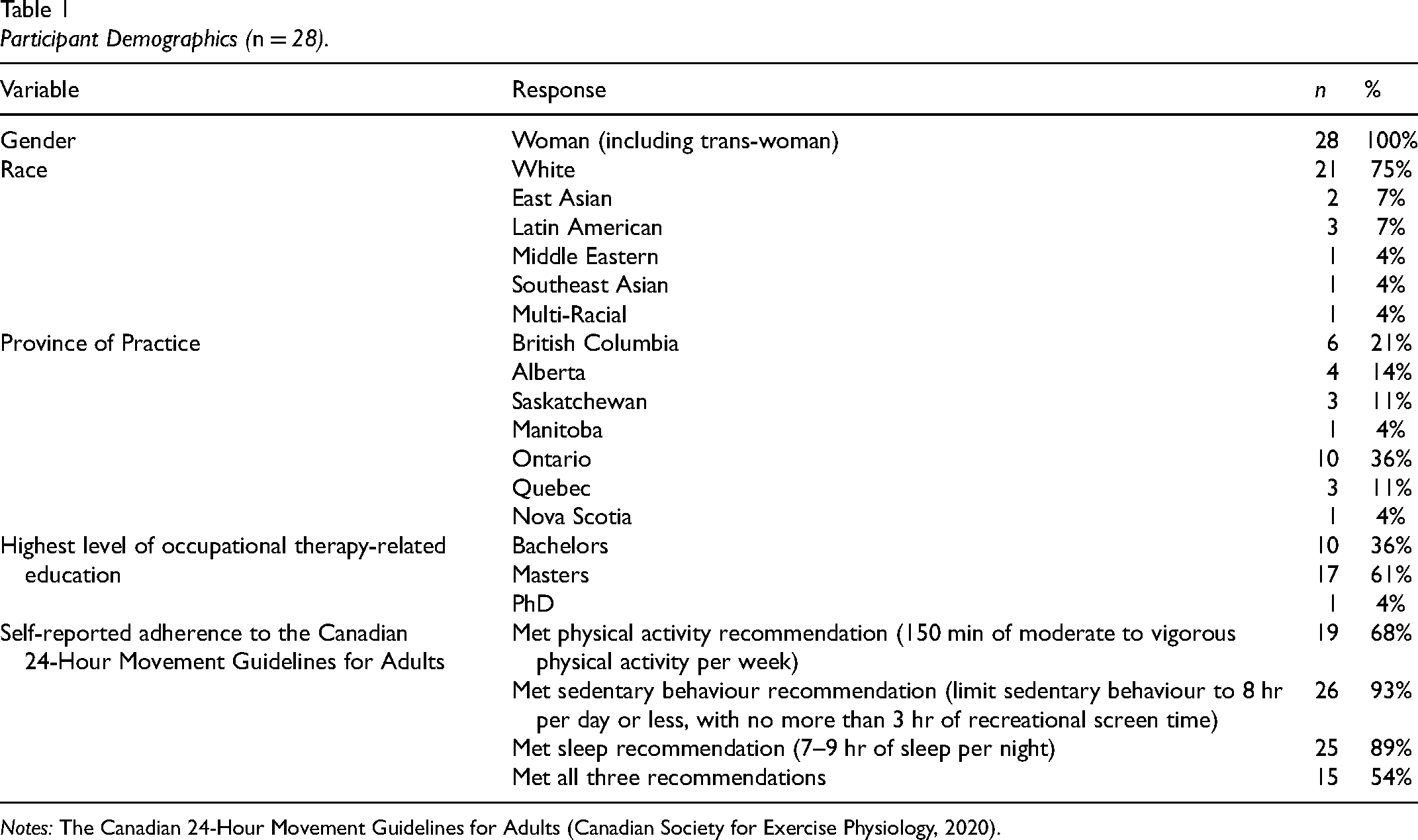
Notes: The Canadian 24-Hour Movement Guidelines for Adults (Canadian Society for Exercise Physiology, 2020).
Guideline Implementation
Knowledge
Knowledge was measured by assessing participants’ awareness and familiarity related to the 24-Hour Movement Guidelines. The majority of participants agreed that they possessed the general knowledge to implement the physical activity (n = 25, 93%), sedentary behaviour (n = 25, 93%), and sleep (n = 21, 84%) recommendations among children with developmental disabilities, with 1 (4%) participant disagreeing with possessing knowledge in all three movement categories. Most participants indicated they were either not at all familiar (n = 7; 37%) or somewhat familiar (n = 9; 47%) with the 24-Hour Movement Guidelines for preschool-aged children.
Attitudes
The attitudes of OTs related to the 24-Hour Movement Guidelines for use with young children with developmental disabilities were measured by assessing participants’ agreement levels, presence/absence of relevant skills, outcome expectancies, motivations, and self-efficacy to use the 24-Hour Movement Guidelines. No participants disagreed with the importance of physical activity and sleep for the healthy development of young children with developmental disabilities, or their relevance to occupational therapy. Some disagreed with the importance of limiting sedentary behaviour for healthy development (n = 3, 11%) and for occupational performance/balance (n = 5, 18%). Overall, most participants agreed they were trained in skills needed to use the movement behaviour recommendations. When asked about their intention and actual/future use of the 24-Hour Movement Guidelines in practice with preschool-aged children with developmental disabilities, most indicated that they had not used the guidelines in the past but will consider using the physical activity (n = 17, 61%) and sedentary behaviour (n = 14, 50%) recommendations in practice in the future. Several participants indicated that they had previously used the physical activity (n = 11, 39%), sedentary behaviour (n = 13, 46%), and sleep (n = 16, 57%) recommendations with young children with developmental disabilities, and 11 (39%) participants responded that they regularly apply the sleep recommendation in this population. Most participants (n = 22, 96%) reported that they agreed with the content of the 24-Hour Movement Guidelines for young children with developmental disabilities. While several participants (n = 21, 78%) agreed that using the guidelines is associated with advantages for themselves, their practice/organization, or their clients, two participants disagreed (7%). No participants (0%) reported feeling that following the guidelines for young children with developmental disabilities was associated with any disadvantages. Table 2 provides a summary of participant responses related to attitudes influencing the use of the 24-Hour Movement Guidelines in occupational therapy practice. Means and standard deviations for clinician self-efficacy items are displayed in Table 3. On average, OTs reported that they felt moderately to completely confident implementing the guidelines for young children with developmental disabilities; however, some participants reported low or no confidence in specific items.
Participants’ (n = 28) Attitudes Related to Use of the Guidelines in Occupational Therapy.
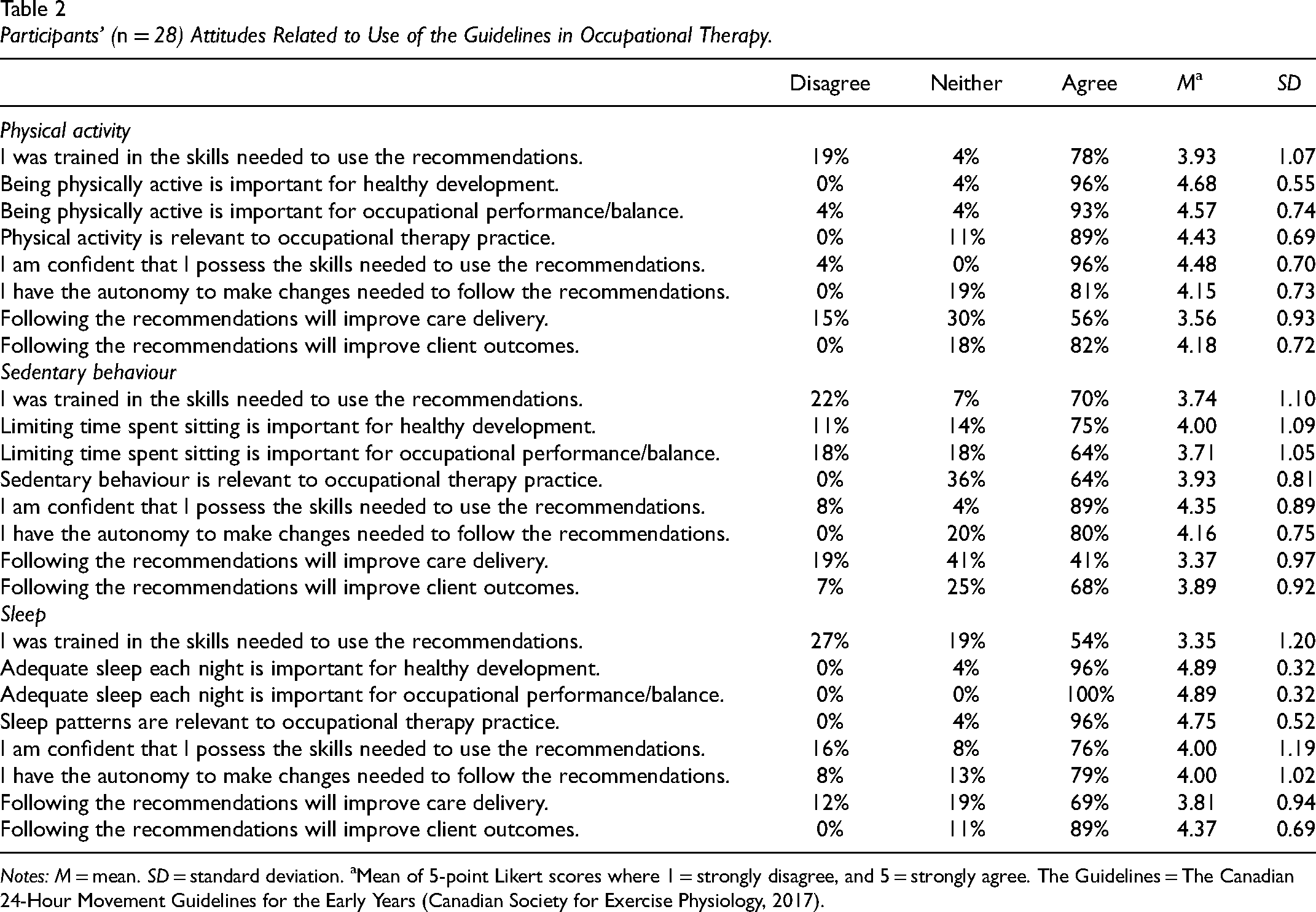
Notes: M = mean. SD = standard deviation. aMean of 5-point Likert scores where 1 = strongly disagree, and 5 = strongly agree. The Guidelines = The Canadian 24-Hour Movement Guidelines for the Early Years (Canadian Society for Exercise Physiology, 2017).
Clinician (n = 28) Self-Efficacy Regarding Implementing the Guidelines in Practice.
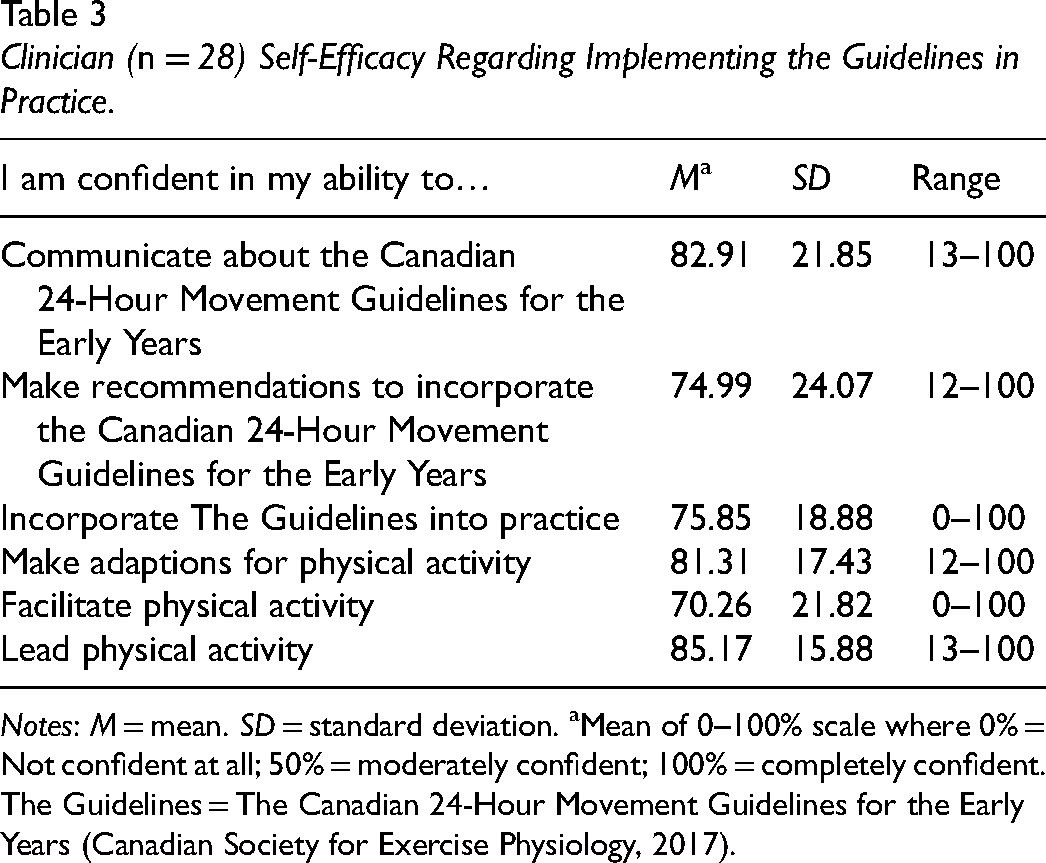
Notes: M = mean. SD = standard deviation. aMean of 0–100% scale where 0% = Not confident at all; 50% = moderately confident; 100% = completely confident. The Guidelines = The Canadian 24-Hour Movement Guidelines for the Early Years (Canadian Society for Exercise Physiology, 2017).
External Factors
External factors assessed included guideline-related, client-related, and environmental-related barriers to the implementation of the 24-Hour Movement Guidelines. Eleven external factors were examined, with items broken down into the three-movement categories (Table 4). Most respondents agreed that the 24-Hour Movement Guidelines are consistent with available evidence (n = 15, 79%) and that the evidence underlying the recommendations is provided (n = 11, 56%). OTs agreed that the format and layout of the guidelines are easy to navigate (n = 26, 96%), and the wording of the recommendations is clear and unambiguous (n = 24, 89%). When considering their clients who are young children with developmental disabilities, 11 respondents (46%) agreed that recommendations are consistent with client values and preferences, while 10 (42%) neither agreed/disagreed. Most participants either disagreed (n = 5, 38%) or neither agreed/disagreed (n = 5, 38%) when asked if the guidelines describe whether client preferences were collected and influenced the recommendations. Most respondents disagreed that colleagues inside (n = 11, 84%) and outside (n = 4, 40%) of their organizations use the 24-Hour Movement Guidelines with young children with developmental disabilities. While most agreed that their organization provides the support needed to use the guidelines (n = 15, 63%), fewer respondents agreed that the guidelines were accompanied by implementation tools (n = 9, 50%). When asked if the tools available are helpful in practice, most OTs disagreed, neither agreed/disagreed, or were unsure (n = 11, 61%).
Participants’ (n = 28) Perceptions of External Factors Impacting the Use of Guidelines in Occupational Therapy Practice.
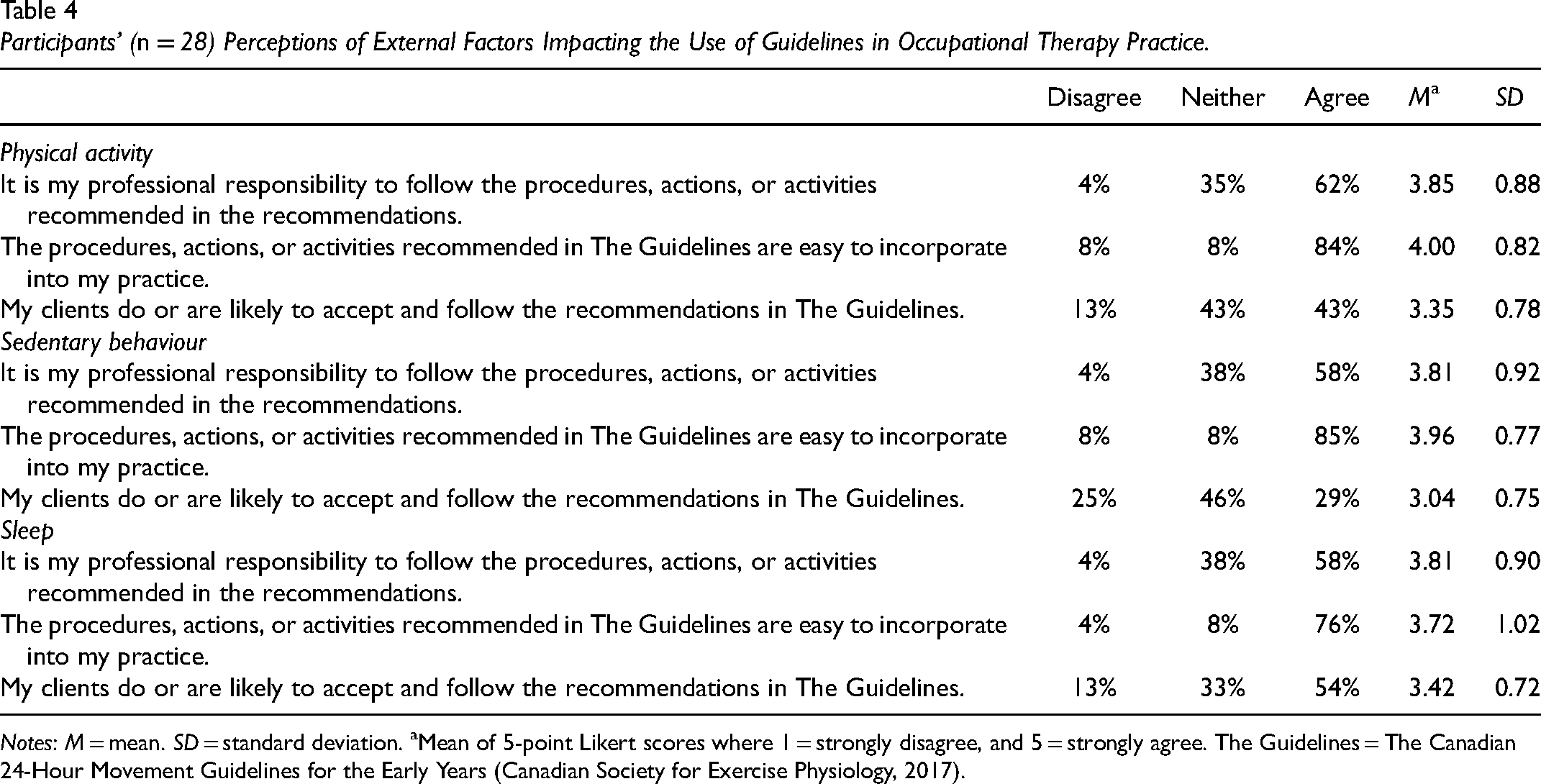
Notes: M = mean. SD = standard deviation. aMean of 5-point Likert scores where 1 = strongly disagree, and 5 = strongly agree. The Guidelines = The Canadian 24-Hour Movement Guidelines for the Early Years (Canadian Society for Exercise Physiology, 2017).
Education, Clinical Experience, and Guideline Implementation
There was a non-significant difference in knowledge between participants who completed undergraduate (n = 10, Mdn = 4.00) and graduate level (n = 18, Mdn = 4.00) occupational therapy training (U = 81.00, z = −.44, p = .66, r = −.083). There was a medium, non-significant difference in attitudes (Mdiff = 0.24, t (28) = 1.46, p = .16, d = 0.59) favouring OTs with undergraduate training. There was a large, non-significant difference in external factors (Mdiff = 0.33, t (27) = 1.90, p = .70, d = 0.81) between OTs with undergraduate and graduate training, favouring those with graduate training. There was a small, negative, non-significant correlation between knowledge and years of practice (rho = −0.14, p = .47), and a small, positive, non-significant correlation between attitudes and years of practice (r = .11, p = .57). There was a medium, negative, significant correlation between external factors and years of practice (r = −.37, p = .05).
Discussion
Application of the 24-Hour Movement Guidelines in occupational therapy practice with young children with developmental disabilities is a promising opportunity to support children's development and well-being. Long-term, movement may also help to shape health-promoting and adaptive behaviours among children and across the life course (Rollo et al., 2020). OTs are well positioned to integrate the guidelines and to adapt the current recommendations for children with disabilities. This study sought to examine factors influencing the use of the 24-Hour Movement Guidelines in pediatric occupational therapy practice when working with young children (aged 3–4 years) with developmental disabilities. While most participants indicated they were not at all or only somewhat familiar with the guidelines, in general, participants reported moderate to high agreement with the recommendations, with some variation based on the type of movement behaviour. Specifically, participants were in favour of using the physical activity and sleep recommendations in practice but were less consistent in their perspectives on limiting sedentary screen time. This is important to note because clinician agreement has been shown to be a strong influencer of guideline implementation in practice (Cabana et al., 1999; Cabana & Flores, 2002; Gravel et al., 2006). This means that building awareness of the 24-Hour Movement Guidelines may be valuable starting point for use in occupational therapy. This study also explored relationships between OT education level and years of practice and whether they influenced the implementation of the guidelines in practice. No significant relationships were observed, suggesting that OT's education, nor years or practice, are related to the factors that shape the use of the guidelines (Pallant, 2016); however, caution should be used when interpreting these results given the small sample.
Despite an overall lack of awareness and training related to the 24-Hour Movement Guidelines as noted by participants, around half indicated that they had used the recommendations previously, and some indicated relatively high autonomy to use the guidelines in the future with young children with developmental disabilities. Healthcare practitioners have previously reported using the guidelines despite limited knowledge, which was linked to practitioners’ value of movement behaviours in their treatment methods (Riazi et al., 2017). While OTs may experience limited training opportunities, their competence, and autonomy to use the guidelines may be related to the alignment between their current practice, the movement recommendations, and the pluralistic occupation-centered practice in occupational therapy (Frolek Clark & Kingsley, 2020; Walder et al., 2021). Generally, OTs employ versatile skills and intervention methods, emphasizing a holistic approach to care. OTs are considered healthcare generalists who have the self-efficacy to adapt their approaches based on client needs (Walder et al., 2021). However, participants’ self-efficacy to implement the guidelines with young children with developmental disabilities varied widely, which may have been related to a lack of opportunities for training on the strategies to integrate movement behaviours in practice (Latimer-Cheung et al., 2016).
Participants in this study held the most positive perceptions towards the sleep recommendation of the 24-Hour Movement Guidelines. All participants agreed that adequate sleep is important for occupational performance/balance among young children with developmental disabilities, and the large majority indicated that sleep patterns are relevant to occupational therapy. Sleep is often prioritized by both clinicians and parents of young children as an important occupation (Gronski, 2022), and most pediatric OTs address sleep within their practice (Piller et al., 2021). However, Piller et al. (2021) found that OTs do not typically feel equipped to address sleep issues, and there is a lack of evidence on effective interventions to support sleep in the early years. These findings were reiterated in the present study, as approximately one-quarter of participants indicated they were not trained on the skills to use the sleep recommendations. Moreover, agreement with having the autonomy to make changes to follow this recommendation was the lowest of the movement behaviours. Several respondents also indicated that they disagreed with sleep recommendations being easy to incorporate in practice. This may be related to a lack of knowledge, training opportunities, and evidence-based resources, all previously identified as barriers to the implementation of the sleep recommendation (Ip, 2023).
Compared to physical activity and sleep, OTs were less likely to agree on the role of limiting sedentary screen time relevant to occupational therapy. They also perceived client acceptance of the sedentary behaviour recommendations less positively than the other movement behaviours. This may be a consequence of differences in the value of sedentary behaviours in therapeutic interventions, diagnostic categories of children typically seen in their practice, or the reasons for the use of screens by clients (e.g., verbal vs nonverbal communication). While OTs may feel aspects of the sedentary screen time recommendation have relevance for use in their discipline, they may not be applicable or easily integrated into practice if they do not align with the goals and preferences of young children with developmental disabilities and their parents. Sedentary and screen-based activities are also frequently used in occupational therapy with video game-based interventions. For example, adaptive video games using a joystick, and active games focusing on balance, strength training, and aerobics have shown moderate level evidence of improvement in gross motor skills in preschool-aged children (Frolek Clark & Kingsley, 2020). While sedentary screen time from a physiological standpoint may be detrimental to a child's health, sedentary pursuits such as reading and colouring can also be considered occupations of preschoolers and are linked with positive developmental outcomes (Poitras et al., 2017). Furthermore, screens can be used in occupational therapy practice to improve accessibility to fine motor activities that improve visual motor integration and bimanual activities for children with developmental disabilities (Coutinho et al., 2017). To work towards a balance of movement behaviours that ensure optimal health outcomes for young children with developmental disabilities, OTs should build awareness surrounding balancing the contexts and quality of sedentary behaviour activities, in addition to the individual needs of the child and their family (Dwyer et al., 2009).
Generally, our findings indicate that OTs felt positively toward the 24-Hour Movement Guidelines. However, the results also suggest that OTs perceived that the guidelines in their current form may not be adequate to support integration in practice due to the perceived internal and external factors influencing their use with children with developmental disabilities. This finding supports recommendations made by Martin Ginis and colleagues (2016) that rehabilitation professionals lack knowledge on how to use the recommendations to implement the guidelines for clients with disabilities. Therefore, informational and implementation resources are required to support knowledge translation (Martin Ginis et al., 2016). Research has demonstrated the importance of capacity building to support knowledge and attitudes related to promoting movement behaviours in educators of young children (Bourke et al., 2024). Bourke et al.'s (2024) findings suggest that guidelines in combination with capacity building, in the form of professional development or resource generation, could support better integration of the 24-Hour Movement Guidelines. Only half of the participants in the current study agreed that the guidelines were accompanied by implementation tools, with most indicating they were unsure, disagreeing, or neither agreeing/disagreeing that available tools are helpful in practice. Moreover, a systematic review by Huijg et al. (2015) identified implementation resources (i.e., assessment and intervention protocols, prescription aids, and educational materials) as facilitators for healthcare providers to implement movement behaviours in practice. Resources developed for OTs should support tailoring the recommendations to individual client needs, abilities, interests, and occupational goals (Taylor et al., 2023a), and be quick and easy to administer (Morgan et al., 2023a). Further, training should be used to support OTs to implement the 24-Hour Movement Guidelines. This should include training opportunities that: (1) educate pediatric OTs on the importance of the guidelines for young children with developmental disabilities, as well as the role OTs can play in supporting engagement; (2) build knowledge, confidence, and skills that could increase the integration of the guidelines by OTs (Morgan et al., 2023b); and (3) build competence in pre-service OTs, which has been identified as a predictor of OT students self-efficacy to integrate best practice (Thomas & Law, 2013).
This study was the first to explore factors influencing the use of the 24-Hour Movement Guidelines with children with developmental disabilities by pediatric OTs in Canada, making important contributions to the literature and future practice. However, there are limitations which must be acknowledged. First, the sample was small. While efforts were made to recruit a large, geographically representative sample, only 28 OTs participated, all of whom identified as women. This may have been due to the inclusion criteria of working with children aged 3–4 years, which potentially limited eligibility. While this was necessary to align with the specific age ranges of the corresponding guidelines, this made for a smaller pool of potential participants. This influenced both the generalizability and reliability of findings and statistical techniques employed. For example, we were unable to conduct regression models to predict the effect of the knowledge, attitudes, and external factors on their use, beyond associations. Moreover, the Clinician Guideline Determinants Questionnaire was a self-report tool, which may have led to variations in interpretations in reporting and social desirability bias. Finally, participants’ self-reported movement behaviours were high and exceeded national averages (Rollo et al., 2022), which could have been attributed to the self-report methodology, or personal investment in movement behaviours, and this may have led to response bias. Despite these limitations, information available through the Canadian Institute for Health Information (2022) indicated that our small sample was relatively representative of the current practitioners in Canada, based on province of practice and gender (i.e., 91% of OTs in Canada identified as female). Therefore, by conducting an initial examination of factors influencing the implementation of the guidelines in occupational therapy, opportunities to support the integration of this resource in practice have been identified. Future research is needed to understand the perspectives of OTs on the value and challenges of employing the 24-Hour Movement Guidelines in their current form, the validity of the resource for children with a variety of disabilities and necessary modifications, and to expand on opportunities for knowledge translation.
Conclusion
The 24-Hour Movement Guidelines may be a promising resource to support health, well-being, and development of preschoolers with developmental disabilities, and OTs are well suited to integrate the recommendations into practice to support uptake. While OTs generally felt positively towards the integration of the guidelines in practice, there was some variation based on the specific type of movement behaviours. Further adaptations to the guidelines are required to better suit the needs of young children with developmental disabilities. Future research should further investigate capacity-building opportunities to provide modifications to the guidelines to accommodate diverse needs and abilities when implemented, and the integration of the 24-Hour Movement Guidelines by OTs in practice.
Key Messages
Occupational therapists (OTs) feel that the Canadian 24-Hour Movement Guidelines for the Early Years are important for preschool-aged children with developmental disabilities and OTs are well-positioned to implement the tool. Despite overall agreement with the guidelines, OTs note that training, self-efficacy to implement the resource, and implementation tools are lacking. To support the integration of the 24-Hour Movement Behaviour Guidelines with young children with developmental disabilities in practice, OT-specific implementation resources and training opportunities are needed.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.