
Abstract
Introduction
The research was aimed to evaluate patterns and clinical and environmental predictors of participation in preschool children with developmental disability.
Method
Cross-sectional design was employed. Caregivers (n = 98) of children aged 9–70 months (mean = 48, SD = 1.5) with developmental disability completed a health questionnaire and the Lithuanian Young Children’s Participation and Environment Measure (YC-PEM). Descriptive statistics and multiple linear regressions were performed to identify patterns and predictors of participation at home, daycare/preschool, and the community.
Results
Participation restrictions, based on frequency and variety of activities, were mostly observed in the community setting. Both clinical and environmental factors explained at least two dimensions of participation across all settings. Of the clinical factors, the predictors of participation were found to be the severity but not the number of impairments of body structures and functions and/or activity limitations.
Conclusions
This study emphasizes the role of the environment and activity limitations in explaining participation of preschool children with developmental disability. Findings can re-direct practitioners’ attention towards context-based assessments and interventions to promote health through participation.
Introduction
Developmental disability is a diverse group of chronic conditions characterized by substantial functional limitations in three or more of the areas of major life activity (e.g., motor, social, emotional, cognitive, and language) (Zablotsky et al., 2019). These conditions begin during the developmental period and persist throughout an individual’s lifespan (Centers for Disease Control and Prevention, 2019). The most common developmental disabilities are visual, hearing, and intellectual disability, specific learning disorder, autism spectrum disorder, epilepsy, and cerebral palsy. In 2016, 52.9 million children younger than 5 years had developmental disability worldwide (Global Research on Developmental Disabilities Collaborators, 2018). Children with developmental disability face a range of medical and social issues, leading to activity limitations and participation restriction (Maxwell et al., 2012).
Participation is described as “involvement in life situations” (WHO, 2011) and is considered a key indicator of health and wellbeing (Colver, 2009) as well as an essential outcome of pediatric rehabilitation (Alghamdi et al., 2017). According to a model developed by Imms et al. (2016), the participation construct includes two main themes: attendance and involvement. Attendance is described as the frequency of attending and diversity of activities in which an individual takes part while involvement is described as the experience of attending and related to motivation, persistence, social connections, and affect. The International Classification of Functioning, Disability and Health (ICF) indicates that participation is influenced by a health condition, in addition to personal and environmental factors which are either barriers to or facilitators to a person’s functioning (WHO, 2001).
Internationally, significant efforts have been made to ensure the right of children with disability to participate in meaningful activities (Lim et al., 2016). Intervention strategies such as a tailored home-program and a coaching approach (Wuang et al., 2013) and the Pathways and Resources for Engagement and Participation (PREP) (Anaby et al., 2018) have been developed to guide children and parents about the demands of the environment and how to apply strategies for modifying the environment. Appropriate interventions can only be developed if there is knowledge about the participation levels and environmental barriers and facilitators to participation.
Few studies have examined the participation of children under the age of 6 years old due to a lack of valid measures of participation for this age group. In 2011–2015, Khetani developed Young Children Participation and Environment Measure (YC-PEM) to capture the participation of children aged 2–5 years at home, daycare/preschool, and community and perceived environmental impact on participation in each setting. The YC-PEM is found to have good psychometric properties and can distinguish the participation and perceived supportiveness of the environment between children with and without disabilities (Khetani, 2015). Several studies (Albrecht and Khetani, 2017; Benjamin et al., 2017; Di Marino et al., 2018; Khalifa et al., 2020) have been conducted on young children’s participation using the YC-PEM. Most of them are limited in the types of diagnoses (Khalifa et al., 2020) and settings (Albrecht and Khetani, 2017; Benjamin et al., 2017; Khalifa et al., 2020; Lim et al., 2016), and the majority involves children from North America (Albrecht and Khetani, 2017; Benjamin et al., 2017; Di Marino et al., 2018; Khalifa et al., 2020).
This study aims to evaluate patterns and clinical and environmental predictors of participation in preschool children with developmental disability. To our knowledge, this is the first study that focuses on the participation and environment of young children with developmental disability in Lithuania and Eastern Europe.
Methods
Participants and procedures
Participants were recruited from the children rehabilitation clinic of the university hospital. Eligible participants had to be caregivers of children aged 0–5 years with developmental disability. Parents were asked to complete the YC-PEM and a health questionnaire that included the items related to impairments of a body structure and functions and activity limitations.
Assessment measures
Participation patterns and environmental factors were measured using the YC-PEM. The YC-PEM is a comprehensive parent-reported tool that assesses the participation and environment of young children aged 0–5 with or without developmental disability at home (13 items), daycare/preschool (3 items), and in the community (11 items). Home activities fall into one of the following categories: (1) helping with basic care routine, (2) household chores, (3) interactive and organized play, and (4) socializing with friends and family. Daycare/preschool activities are divided into group learning, socializing with friends, and school excursions and events. Community activities fall into one of the following categories: (1) excursions and outings, (2) classes and groups, (3) community-sponsored activities, and (4) recreation. Each type of child activity was assessed by caregivers along three dimensions: (1) frequency of attending (8-point scale); (2) involvement (5-point scale), and (3) desire for change (yes or no). If caregivers answered “yes,” they indicated what type (s) of change desired (do more or less often, be more interactive, be more helpful, and/or participate in a broader variety of activities).
The environmental scales of the YC-PEM consist of two parts, one for environmental features (e.g., physical layout, sensory qualities, activity demands, social relationships, attitudes, safety, weather, and policies) and the other for resources (e.g., transportation, equipment, programs and services, and supplies). The environment is assessed separately in the home (13 items), daycare/preschool (16 items), and community (17 items) settings. Parents assessed impact of environmental features and resources on a 3-point scale.
Many different summary scores can be computed for the YC-PEM based on the user’s needs (Khetani, 2015). The summary scores of the YC-PEM used in the study were: average frequency—the average of all ratings within a setting (range = 0–7); percentage of activities in which children participate—the number of activities within a setting for which the parent responded 1 to 7 (i.e., ones that the child actually does) divided by the number of possible activities within the setting multiplied by 100 (range = 0–100); average involvement—the average of all ratings within a setting (range = 1–5); percentage of activities in which parents desire for change—sum of the number of items scored as “yes, change desired,” divided by the total number of items, and multiplied by 100 (range = 0–100); supports—the average percentage of environmental items that parents see as supports to the child’s participation (range = 0–100); barriers—the average percentage of environmental items that parents see as barriers to their children’s participation (range = 0–100); environmental helpfulness—parents’ perception of how helpful the environment is in supporting their children’s participation (range = 0–100); environmental resources—parents’ perception of the availability of resources to support their children’s participation in the setting (range = 0–100); overall environmental support—sum of ratings across all environmental features and resources items, divided by the maximum possible score, and multiplied by 100 (range = 0–100).
Internal consistency of the original YC-PEM version ranges from 0.68 to 0.96 for the participation scale and from 0.92 to 0.96 for the environment scale. Test re-test reliability is also sufficient (0.31–0.93 and 0.91–0.94 for the participation and environment scales) (Khetani, 2015). Translation into the Lithuanian language of the YC-PEM was performed according to guidelines described by Wild et al. (2005). This process included a forward and backward translation, a discussion between researches and translators, and finalization. The internal consistency of the YC-PEM scales was assessed by calculating the Cronbach’s alpha coefficient. Convergence validity was determined by calculating Spearman correlation coefficients between the desire for change and the overall environmental support scales. The Lithuanian version of the YC-PEM has acceptable reliability (internal consistency 0.73–0.89 for the participation scale and 0.51–0.71 for the environment scale). There was a statistically significant mean inverse correlation between the desire for change and the overall environmental support scales at home (r = −0.454, p < 0.001), daycare/preschool (r = −0.353, p = 0.002), and the community (r = −0.428, p < 0.001) settings.
Clinical data were collected using a questionnaire based on a Developmental code set from the ICF for children and youth (Ellingsen, 2011). Two versions of the questionnaire were used, one for children under 2 years of age and the other for children between 3 and 5 years of age. Both questionnaires included items on impairment of a body structure and functions as well as activity limitations. The severity of a problem indicated in the item was measured on a five-point Likert Scale (from 0 = no problem to 4 = serious problem). A total number of impairments of a body structure and functions, in addition to a total number of activity limitations, were calculated to represent the complexity of the condition with each possible impairment or limitation being counted as “1.” The sum of a respondent’s Likert scores indicating the degree of a problem was calculated to represent the overall severity of impairments of body structures and functions alongside activity limitations.
Statistical analyses
Data were analyzed using Statistical Package for Social Science 22 for Windows (SPSS) and Microsoft Office Excel. Statistically significant differences in probability plots were marked as p<0.05.
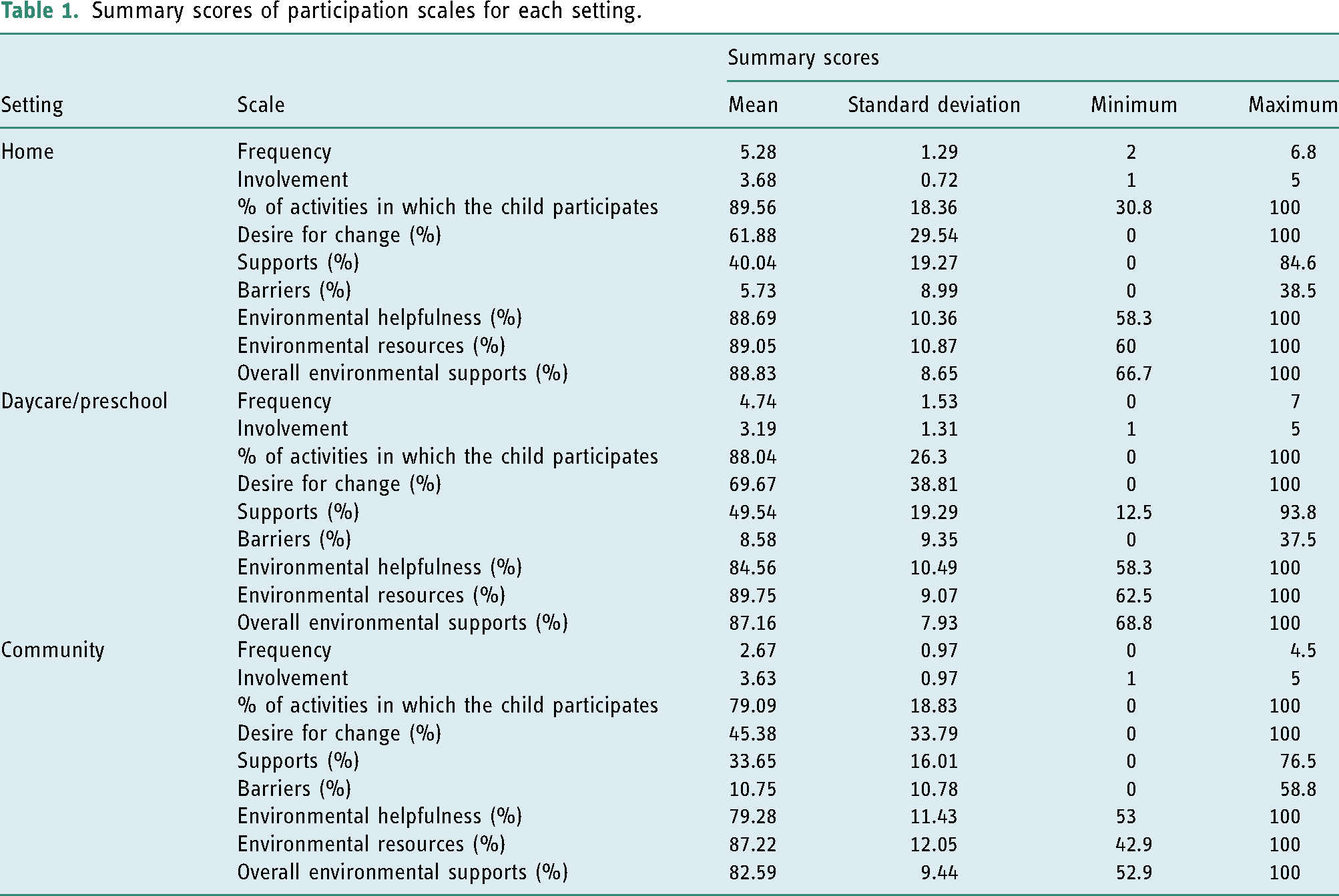
Characteristics of study participants were defined using descriptive statistics. Three participation summary scores (frequency, involvement, and desire for change) and five environmental summary scores (environmental supports, barriers, helpfulness, resources, and overall environmental supports) were calculated for each setting (home, daycare/preschool, and the community) to assess participation across these settings.
Multiple regression analyses were used to describe the clinical and environmental variables associated with participation. The regression models examined each setting (home, daycare/preschool, and the community) separately: twelve models were tested. The dependent variables were the summary scores of the YC-PEM subscales: average frequency, average involvement, the average variety of activities, and the percent of activities in which the change is desired. The potential predictors were clinical factors (i.e., the number and severity of impairments of body structures and functions, the number and severity of activity limitations), scores of the environmental scales and the summary scores of the environmental subscales (i.e., supports, barriers, environmental helpfulness, environmental resources, and overall environmental supports). The assumptions of the multiple regressions were tested by analyzing histograms, normal probability plots of the residuals, scatterplots of the residuals, and the variance inflation factor values. 95% confidence intervals were used to check the accuracy of regression parameters. R2 was reported (in percentage) to evaluate the size to which the examined variables could explain the variance of participation.
Results
Participants
Ninety-eight families raising children with developmental disability agreed to participate in the study. The age of the participants was 9–70 (mean ± SD = 48 ± 1.5) months. Half of the study participants were older than 4 years. Children were diagnosed with global developmental delay without definitive etiologic diagnosis (n = 43), autism (n = 25), cerebral palsy (n = 12), epileptic encephalopathy (n = 5), moderate to profound hearing loss (n = 4), Down syndrome (n = 3), fetal alcohol syndrome (n = 2), blindness (n = 1), fragile X syndrome (n = 1), Angelman syndrome (n = 1), and Smith–Magenis syndrome (n = 1). The mean number of activity limitations (e.g., exploring objects, learning through play, vocalizing, and maintaining a body position) reported by parents was 9.05 (±4.75) and the mean number of impairments of body structures and functions (e.g., growth impairment, incontinence, and pain) was 5.54 (±2.77). The most significant problems were reported in the activity domain.
Participation patterns
Summary scores of participation scales for each setting.
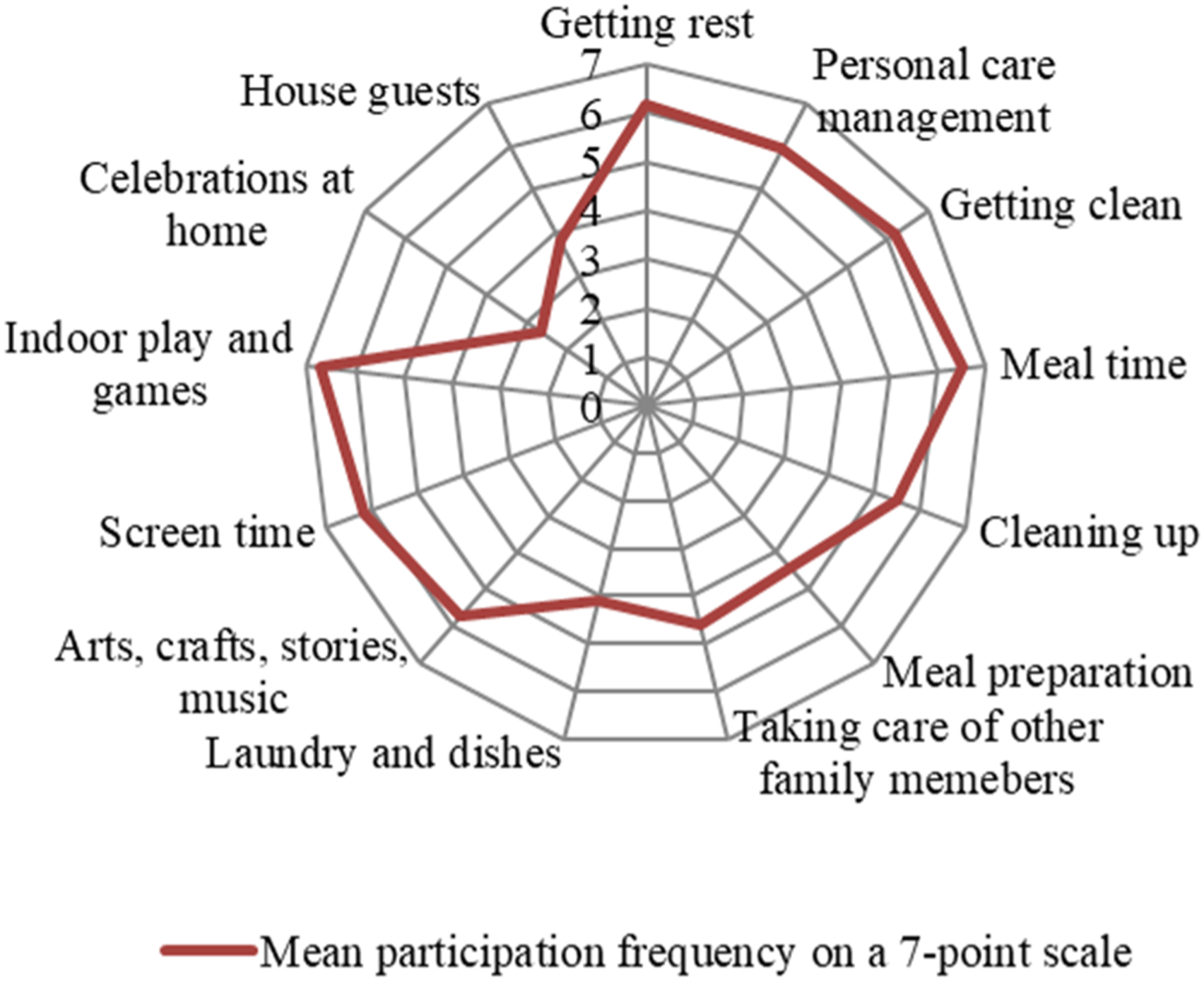
Mean participation frequency in home-based activities.
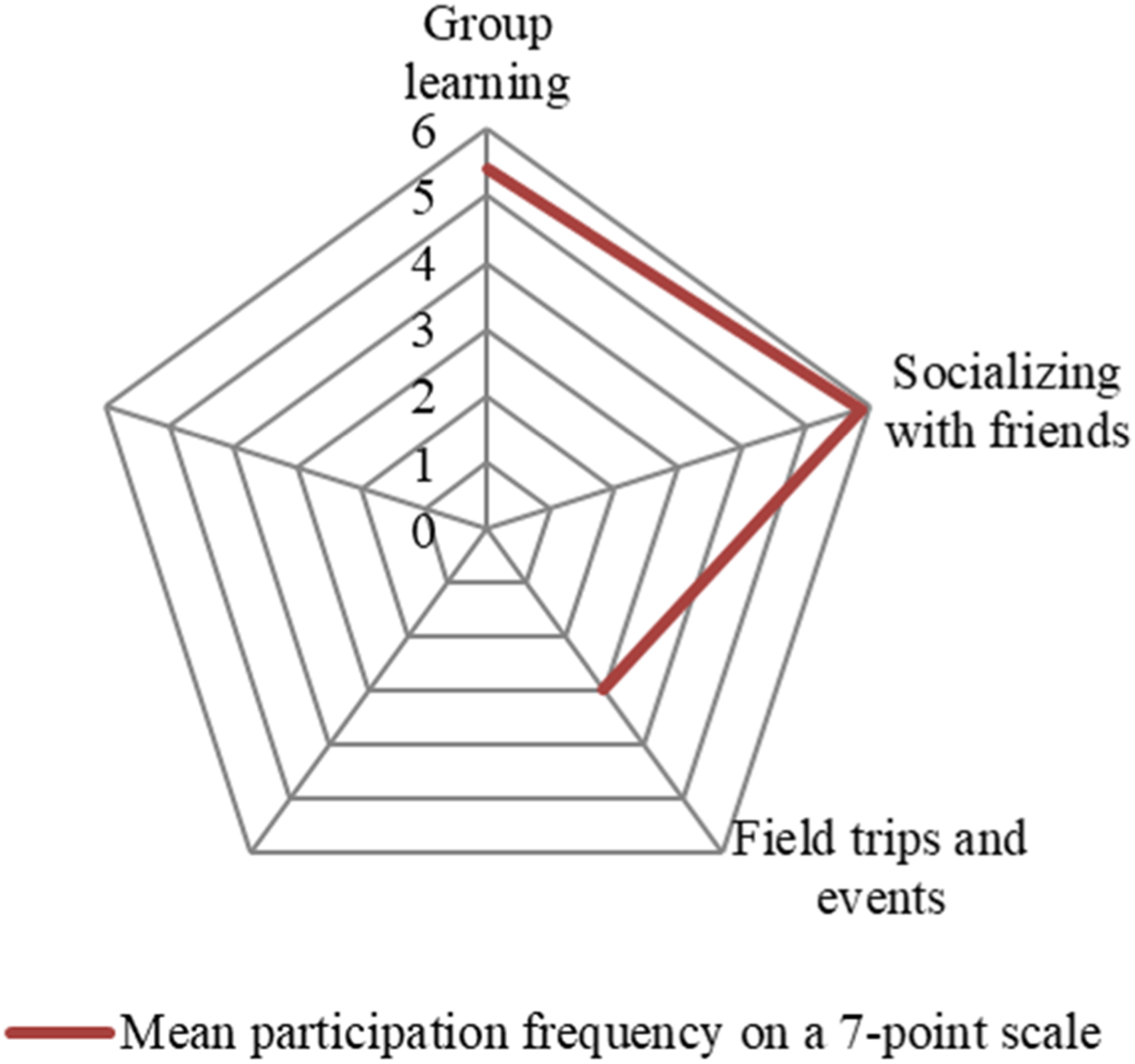
Mean participation frequency in daycare/preschool activities.
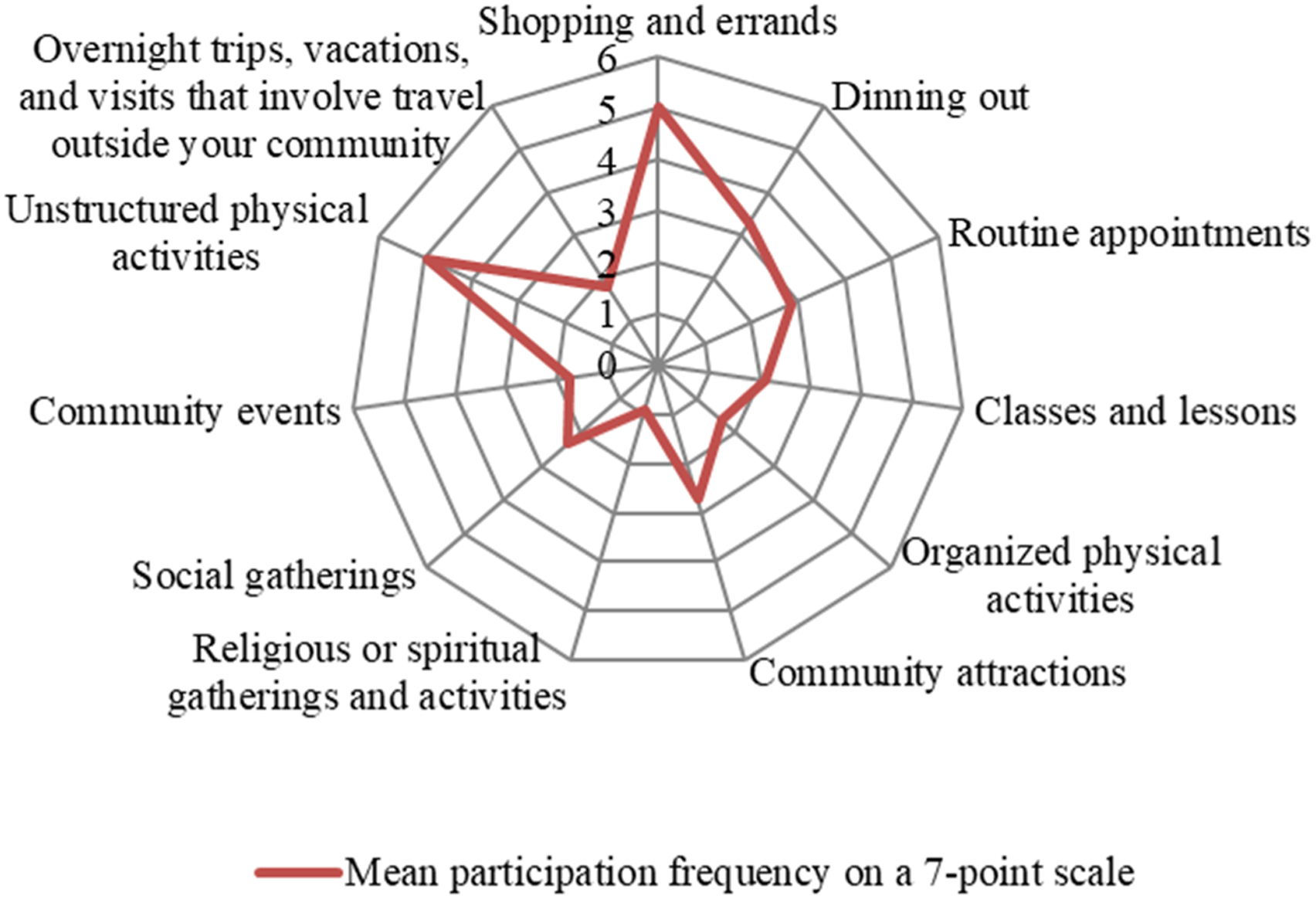
Mean participation frequency in community activities. The explanatory factors of participation levels
The mean scores of overall environmental supports were different across settings: home (88.8%) and daycare/preschool (87.2%) settings scored higher, while the community setting (83%) scored lower. The most common environmental supports that were evident across all settings were the time (52–68.4%) and money (62.2–70.4%) spent by families to promote the child’s participation, and supplies (40.8–79.6). The common supports were also access to personal transportation to get to daycare/preschool and community activities (66.3% and 88.8%, respectively) and programs/services available at home and in the community (40.8% and 59.2%).
Physical (5.1–19.4% in different settings), cognitive (18.4–38.8%), and social (12.2–42.9%) demands of typical activities at home, daycare/preschool, and community were reported as the most significant barriers to child’s participation. A lack of public transportation was one of the most reported barriers to daycare/preschool (16.3%) and community (18.4%) participation.
Multivariate associations of clinical and environmental factors with participation summary scores.
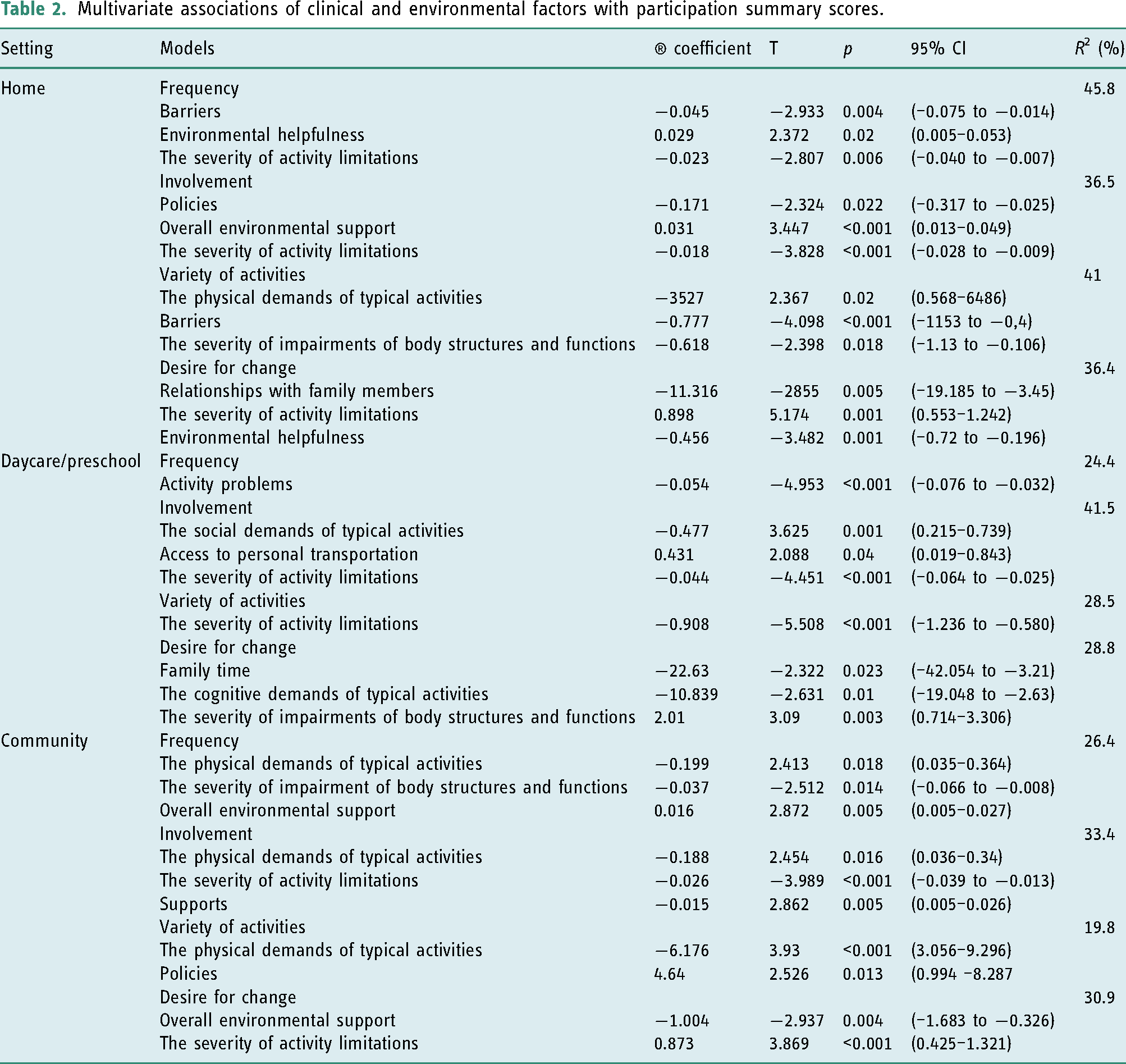
In a home setting, environmental barriers, helpfulness, and the severity of activity limitations explained the frequency of participation with a variance of 45.8%. Policies (e.g., parent’s work hours, time off, residential and workplace policies), the severity of activity limitations, and overall environmental support were the strongest predictors to involvement (36.5% of the variance). The physical demands of typical activities, the severity of impairments of body structures and functions, and environmental barriers accounted for the variety of activities that children participated in (41% of the variance). Relationships with family members, environmental helpfulness, and the severity of activity limitations were the strongest predictors of the number of activities that parents wanted to change, explaining 36.4% of the variance.
When studying the daycare/preschool setting, linear regression analyses revealed that the severity of a child’s activity limitations was the only variable explaining 24.4% of the variance in frequency and 28.5% of the variance in the variety of the activities. The access to personal transportation, the social demands of typical activities, and the severity of activity limitations affected the level of involvement, with a variance of 41.5%. Parents’ desire for a change was largely related to the family time devoted to promoting the child’s participation, the physical demands of typical activities, and the severity of impairments of a body structure and functions (28.8% of the variance). Based on the beta coefficients, the time spent by the family and the physical demands of typical activities were associated with a lower number of activities that parents wanted to change. The severity of a child’s impairments of body structure and functions was associated with a greater number of activities that parents wanted to change.
In a community setting, the physical demands of typical activities served as a significant factor in explaining three participation dimensions: frequency, involvement, and a variety of activities that children participate in. Along with the severity of impairment of body structures and functions and overall environmental support, the physical demands of typical activities accounted for 26.4% of the variance of participation frequency, and together with the severity of activity limitations and environmental supports accounted for 33.4% of the variance of involvement. The variety of community-based activities was strongly associated with policies and the physical demands of typical activities (19.8% of the variance). When it comes to the desire for change in community participation, overall environmental support, and the severity of a child’s activity limitations, accounted for 30.9% of the variance of this domain.
Discussion and implications
This study applied the YC-PEM to build culturally and clinically relevant knowledge about participation patterns and participation predictors in preschool children with developmental disability. Study results are consistent with and expanded upon prior research (Albrecht and Khetani, 2017; Benjamin et al., 2017; Di Marino et al., 2018; Khalifa et al., 2020; Khetani, 2015; Lim et al., 2016) on the participation of young children and participation predictors, the most important of which were environmental supports.
Participation patterns
This study finds that preschool children with developmental disability participated more frequently and in a broader range of activities in the home setting, which was also reported in other studies (Di Marino et al., 2018; Khetani, 2015). The mean frequency of home participation of Lithuanian preschool children was almost the same as that of their peers with (Di Marino et al., 2018; Khetani, 2015) and without disability (Khetani, 2015) living in other countries. Screen time, indoor play and games, mealtime, personal care management, and getting clean were reported to have the highest frequency. Other studies that analyzed the home participation of typically developing and/or disabled preschool or school-age children also identified screen-time activities as the most common (Bakaniene and Prasauskiene, 2020; Di Marino et al., 2018; Larson and Verma, 1999; Law et al, 2011, 2013). Lithuanian children with developmental disability quite rarely (on average from once each week to several times in the last month) participated in household chores, such as meal preparation, taking care of family members, and laundry handling. Similar data can be found in the literature on home participation of preschool and school-aged children with different types of disability in different countries (Bakaniene and Prasauskiene, 2020; Di Marino et al., 2018; Khalifa et al., 2020; Larson and Verma, 1999). We do not have data on the participation of typically developing Lithuanian children household chores and in general, therefore we cannot conclude whether the participation of children with disability in household chores is lower or not. Nevertheless, it is clearly insufficient. Participation in chores together with parents or independently provides learning opportunities for children to practice their problem-solving skills, increase family socializing, and teach them to take responsibilities (Dunst et al., 2000). Early intervention teams should pay attention to this and find ways to involve a child with developmental disability in household chores as a naturally occurring learning environment.
Lithuanian children with developmental disability were relatively often involved in in-group learning, socializing with friends, field trips, and events. The mean frequency of participation in in-group learning was 6 (out of 7), for socializing with friends 5.5, and for field trips and events 3. These frequencies of participation of Lithuanian children with disability are higher than that of their peers with disability living in North America (Benjamin et al., 2017; Khalifa et al., 2020; Khetani, 2015) and almost the same as in typically developing North American children (Benjamin et al., 2017; Khetani, 2015). These differences in results may have been due to differences in the study population (e.g., children with a specific diagnosis of autism spectrum disorder vs developmental disability), instrument used to measure participation, and national education policies. In Lithuania, children with or without disability are required to attend kindergarten regularly. Home or clinic-based therapy services may limit attendance at preschool activities for children with developmental disability, but are not so common as to have a significant effect.
Our findings also indicated that children with developmental disability generally have lower rates of participation in community settings when compared to other settings, which was also found in other studies (Di Marino et al., 2018; Khalifa et al., 2020; Khetani, 2015). Interestingly, although the number and frequency of activities performed were the lowest in the community, parents indicated the lowest need for change in this setting. A recent qualitative study reported that parents raising children with a developmental disability avoid participating in community activities for several reasons, the most important of which was considerable effort needed to prepare to leave home and difficulties in managing a child’s behavior in an often unpredictable community environment (Khetani, 2015). This highlights that in order to improve the participation of children with disability in the community, it is necessary to focus on the whole family rather than just the child and his/her capabilities.
Factors influencing participation
In this study, environmental factors had the strongest contribution in explaining participation for at least three (out of 4) dimensions, whereas the contribution of the severity of impairments of body structures and functions and/or activity limitations was lower, but observed in all participation dimensions across all settings. Out of environmental factors, the physical demands of typical activities had the greatest contribution in explaining participation in the community and home, while the social ones were the critical contributory factor for involvement in daycare/preschool activities. These findings emphasize the importance of environmental modifications (or universal design) as well as family and other stakeholders coaching on ways of grading and adapting specific activities to the child’s abilities. These activities should be made manageable and accessible.
The importance of the environmental factors in explaining the participation for both preschool and school-aged children was also established in other studies (Albrecht and Khetani, 2017; Anaby et al., 2014; Bakaniene and Prasauskiene, 2020; Chiarello et al., 2016; Di Marino et al., 2018; Eriksson, 2005; Khalifa et al., 2020; Khetani et al., 2013). Unlike the findings of our study, other studies found no or little direct effects of health impairments and/or functional limitations on young children’s participation. Albrecht et al. (2017) used the YC-PEM to study the effects of child, family, and environmental factors on young children’s participation in home-based activities. The results of structural equation modeling showed that children’s participation was related to perceived environmental support, while functional limitations and performance had only an indirect effect on participation. That is, fewer functional limitations and higher task performance were associated with greater environmental support and a correspondingly greater level of involvement in home activities. In a study by Di Marino et al. (2018), the participation of young children at home, daycare/preschool, and community, as assessed by YC-PEM, was mainly related to the environment and family functioning. Children’s functional issues contributed to involvement in daycare/preschool activities, and health conditions were not associated with any dimension of participation.
When compared to other studies, our findings show a greater impact of health impairments and activity limitations on the participation of children with disability. These findings are potentially related to a socio-cultural context. Lithuania has been a member of the European Union since 2004 and shares many aspects of European culture and tradition. However, its history and political transition after the post-Soviet era created particular economic and social circumstances. Oftentimes, disability is seen as a medical pathology, a loss, a source of problems, the otherness, leading to limited personal opportunities. Children with developmental disability are seen as in need of exceptional care and individual treatment, which should be continued until they reach age-appropriate developmental milestones (Guščinskienė and Žalkauskaitė, 2011; Raudeliūnaitė and Šavareikaitė, 2013; Ruškus, 2020). When the emphasis is placed on the child with the disability rather than the environment, parents underestimate the impact of environmental factors on the child’s participation. Programs to change attitudes toward disability, as well as children with disability, are much needed. Parents and clinicians should pay more attention to interventions at the level of the environment and focus on strengthening and developing new context-based therapies.
Study limitations
The study included a convenience sample, drawn from one health facility that may not represent a larger geographical population. Our sample, however, was heterogeneous with regards to the types of developmental disability represented. The number of health impairments and activity limitations, as reported by parents captured the complexity of the child’s condition. Although this model has proven to be effective in testing models of participation (Anaby et al., 2014; Di Marino et al., 2018), standardized measures of a child’s functioning could also be included.
The study did not investigate family factors (i.e., marital status, family relations, and income) that might also have an impact on participation. While the YC-PEM includes some family-related environmental factors as barriers or support, measuring of family background and socio-economic status, or testing of children’s participation in diverse groups in terms of socioeconomic status would have provided a more complete picture of the participation and determinants of participation for children with developmental disability.
Furthermore, the study data were collected from parents and direct observations of children’s participation were not included in the study. Future studies should include a qualitative dimension for a deeper understanding of children’s participation from parents’ perspectives.
Although multiple regression analysis describes the strength and character of the relationship between child factors, environmental support and barriers, and participation, cause and effect cannot be claimed because of the cross-sectional design of the study. Longitudinal intervention-based studies are needed to determine how participation can be predicted or changed over time.
Conclusion
This study extends previous knowledge about participation patterns and predictors of participation of preschool children with developmental disability.
Preschool children with developmental disability participated in various activities at home, daycare/preschool, and the community. However, the parents need a deeper understanding of the impact of environmental barriers and supports on child participation. Clinicians should use more environment-modifying interventions while taking into account the child’s level of functioning. Future studies should explore the type of participation changes desired by parents as well as the strategies used by parents to promote their child’s participation. Detailed information about parental desires for changes in participation could guide rehabilitation specialists in working on specific types of activities. Parent-reported strategies to promote the participation of children with developmental disability could offer service providers as well as policy-makers ideas for practice and system changes.
Key findings
Predictors of participation were environmental factors, the severity of child’s health impairments and activity limitations. Policies, the severity of activity limitations, and overall environmental support were the strongest predictors to the child’s involvement in home activities. Environment-modifying interventions, which consider the child’s level of functioning, are essential to ensuring the participation of children with developmental disability.
What the study has added
The participation of Lithuanian preschool children with developmental disability is relatively high in home and daycare/preschool settings. However, in the community setting, their participation is significantly restricted. Preschool children participation is influenced by environmental factors in addition to the severity of health impairments and activity limitations.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included in the conduct of the research.
Footnotes
Research ethics
Ethical approval was obtained from the Department of Bioethics of the University (No. BEC-SR(M)-55, 2018).
Consent
Written informed consent was obtained from the caregivers of children participating in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Contributorship
All authors made substantial contribution to all of the following: (1) the concept and design of the study and acquisition, analysis or interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of version to be submitted.