
Abstract
Background
Bathing is a human occupation for which members of interdisciplinary healthcare teams are consulted, including occupational therapists (Ruest et al., 2022). In Canada, 15% of falls among older adults occur in the bathroom, and many of these falls happen while bathing (Aminzadeh et al., 2000). Among self-care activities, bathing has the highest prevalence of disability; the proportion of Canadian adults reporting difficulty with bathing increased from 2.6% at 70 years of age to 20.8% at 90 years (Guay et al., 2014). Stepping over the edge of the bathtub is an especially challenging and hazardous aspect of transferring for older adults (Aminzadeh et al., 2000; Stevens et al., 2011). Nearly one in four community-dwelling older adults has difficulty with this task (Zimmer & Chappell, 1994). To target bathing autonomy and fall prevention in older adults (Zingmark & Bernspång, 2011), occupational therapists often recommend assistive technology for the bathroom (Guay, Robitaille et al., 2014; Whitehead & Golding-Day, 2019), including grab bars (Clemson & Martin, 1996).
Grab bars used for assistance with stepping into and out of the bathtub must be able to withstand a range of applied forces. Past research has also highlighted that not all grab bars provide equal support (King & Novak, 2017). A permanent vertical grab bar mounted on the side wall of the bathtub has been shown to assist with stepping into and out of the bathtub (Guay et al., 2020; Nirmalanathan, 2019), support balance (King & Novak, 2017; Sekiguchi et al., 2017), and prevent injuries (Levine et al., 2021; Stevens et al., 2011). Compared to horizontal or angled configurations, a vertical grab bar may be preferred for balance recovery following balance loss (Guitard et al., 2011). Consequently, a vertical grab bar is recommended in building codes and standards (CSA Group, 2018; Ontario Building Code, 2013). However, many barriers prevent the installation of permanent grab bars, including cost (Statistics Canada, 2017), incongruence with existing bathroom construction (Bunn et al., 2008; King et al., 2018), unaccommodating landlords (Aminzadeh et al., 2000; Bunn et al., 2008; King et al., 2018), and concerns about the resale value of a home (King et al., 2018). Other barriers to the installation of permanent grab bars include the stigma surrounding devices that may be associated with aging or disability (Aminzadeh et al., 2000).
In the absence of a permanent grab bar, a person may place their hand directly on the shower wall or use temporary options, such as a rim-mounted grab bar. Rim-mounted grab bars typically have a graspable bar (design specifications vary), which secures with a clamp onto a bathtub rim. The clamp employs a pressure fit mechanism by tightening a knob, which squeezes two plates (which may or may not have nonslip padding) against the rim of the bathtub.
To our knowledge, evidence regarding the safety or effectiveness of temporary rim-mounted grab bars for supporting bathing transfers is limited. However, given constraints with the design, this warrants consideration. For instance, a person may have to lean over to use a low rim-mounted grab bar depending on their height; greater forward trunk flexion angles are associated with increased task demands (Takahashi et al., 2006). Moreover, during walking, increased forward trunk flexion at the time of balance loss has been shown to increase an individual's risk of falling (Owings et al., 2001). Consequently, it is likely that increased trunk flexion angles can be problematic if a loss of balance occurs while bathing, as well. However, the solution to that concern, a taller rim-mounted grab bar, would consequently have a longer moment arm, which would generate larger bending moments at the point of contact between the clamp and bathtub rim. These design requirements would place greater mechanical stress on the grab bar, requiring greater material and structural strength to prevent damage to the grab bar itself, as well as a more robust interface between the grab bar and the bathtub.
The primary objective of this study was to compare a rim-mounted grab bar, to a wall-mounted grab bar, and no-grab bar condition, for assistance with stepping into and out of a bathtub on postural task requirements for older adults, and grab bar loading. While rim-mounted grab bars may offer a potential solution to support bathtub transfers where a wall-mounted grab bar is not feasible, we hypothesized that the rim-mounted grab bar may negatively affect postural demands. Additionally, we aimed to characterize perceived safety, comfort, effectiveness, and ease of use when using the various grab bars or with no grab bar use.
Method
Study Design
A repeated-measures design was used for this study, imbedded with a perception questionnaire. All participants provided written informed consent. Ethical approval was received from University Health Network, ethics board approval #REB 19-5230.
Participants
A convenience sample of individuals 65 years of age and over was recruited through community advertisements. All participants were community-dwelling (i.e., individuals living in homes or senior residences) and experiencing bathing difficulty. A sociodemographic survey was then used to capture demographics and self-report bathing difficulty. Specifically, we asked:
Do you have difficulty with bathing tasks, which may include, but not limited to, physical limitations such as balance or mobility impairment or fear of falling? What challenges do you currently face while bathing? Do you have one or more of the following conditions? (Possible answers: inner ear diseases, vestibular disease, lower limb arthritis, balance problems, diabetes, stroke, cardiovascular disease, and concussion.)
To be included in the study, the ability to use a grab bar independently with no additional assistance had to be self-reported. Exclusion criterion was self-reported concussion within the past 6 months or musculoskeletal injury impacting mobility.
Experimental Environment
This protocol was conducted in a custom-designed, experimental bathroom, which included an enameled steel bathtub, and a vinyl bathroom floor (Figure 1). The bathtub had a vertical rim height of 41 cm. The bathroom floor adjacent to the bathtub was covered with vinyl tiles and slip-resistant bathmats with a towel placed over it. The bathroom floor to the bathtub surface had a vertical height difference of 10.5 cm. One solid plywood side wall was present; others had been removed to maximize the visibility of the participant's lower limbs. The bathtub was padded with foam for safety.
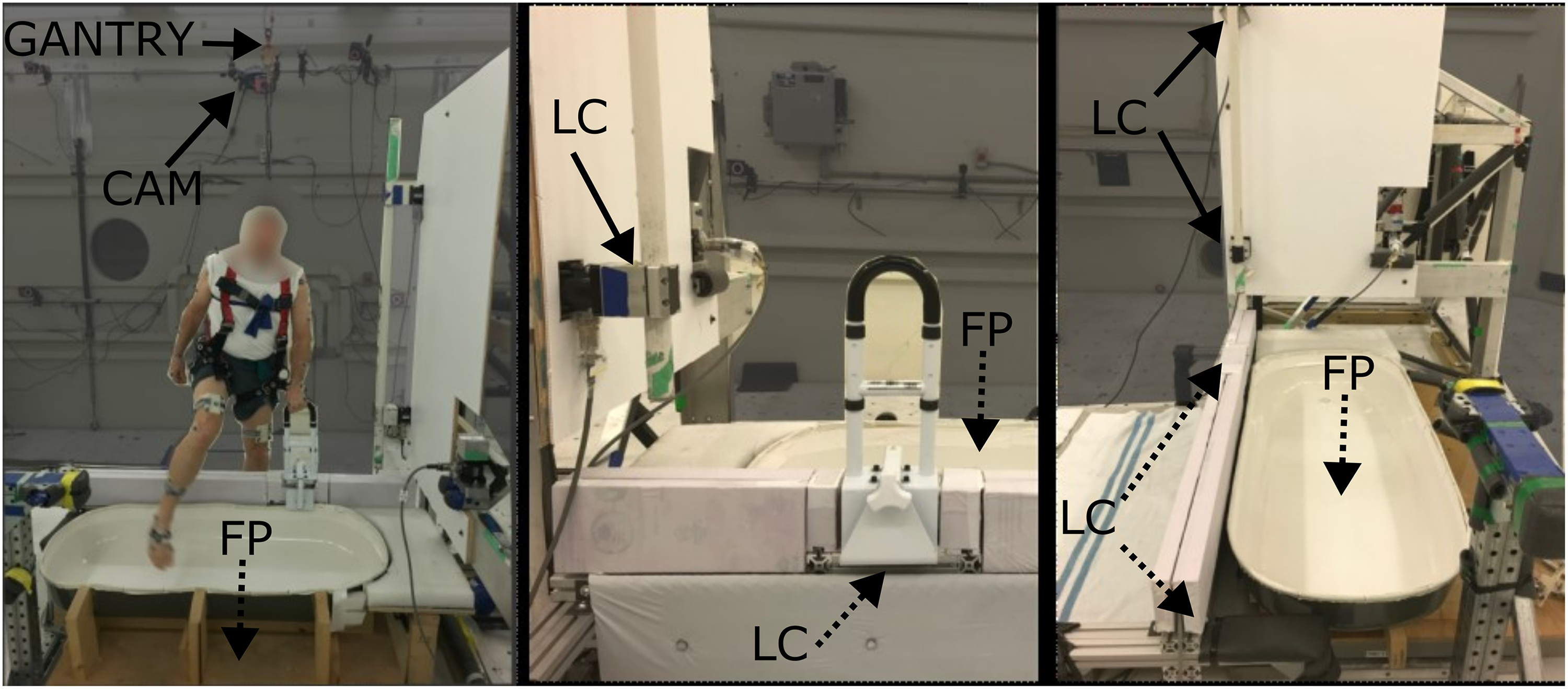
Experimental environment, with load cells (LC), force plates (FP), cameras (CAM), and an overhead gantry (GANTRY) indicated. Solid arrows show visible equipment, while dashed arrows indicate the equipment that is blocked from view. Left: harnessed participant stepping into the bathtub using the rim-mounted grab bar. Vertical grab bar and wall visible. Middle: low rim-mounted grab bar affixed to the bathtub rim, surrounded by foam. Right: vertical grab bar, bathtub, and bathroom floor. Rim-mounted grab bar removed.
A metal bridge extended over the bathroom floor and bathtub. Mounted to this bridge were a firm foam board which replaced the original bathtub rim (maintained at 41 cm in height) and a tri-axial load cell (1000 Hz; MC33A-1000, AMTI, Watertown, MA, USA) which collected force data from the rim-mounted grab bar. Mounting the rim-mounted grab bar on the bridge permitted direct measurement of the force applied to the grab bar (i.e., separating grab bar forces from other forces applied to the bathtub) and minimized noise within the force signal. A vertical grab bar mounted on the side wall was also attached to two tri-axial load cells (1000 Hz; MC33A-1000, AMTI, Watertown, MA, USA) on either end to capture applied forces. Finally, 15 motion capture cameras were mounted within the laboratory space to capture kinematics (250 Hz, Motion Analysis, Santa Rosa, CA) while the participant stepped into and out of the bathtub.
For all testing, the bathtub surface was wetted with 1 L of a soapy water solution (diluted sodium lauryl sulfate, 2 g/L) (King & Novak, 2017).
Assistance Conditions for Stepping into and Out of the Bathtub
For this study, four assistance conditions were presented; we use the term “assistance” in this study to describe the external assistance provided by a device (grab bar or wall) when stepping into and out of the bathtub. Assistance by a person was not provided.
Low rim-mounted grab bar: Participants used a grab bar mounted on the bathtub rim, with the top of the grab bar located 36.5 cm above the rim (77.5 cm above the bathroom floor and 67 cm above the bathtub floor) and the lowest setting available on the grab bar. High rim-mounted grab bar: Participants used a grab bar mounted on the bathtub rim, with the top of the grab bar located 46 cm above the rim (87 cm above the bathroom floor and 76.5 cm above the bathtub floor) and the highest setting available on the grab bar. Vertical grab bar mounted on the side wall: Participants used a vertically oriented grab bar mounted and secured on the side wall in line with the bathtub rim (bottom of the grab bar mounted ∼5 cm above the bathtub rim, 46 cm above the bathroom floor and 35.5 cm above the bathtub floor). The vertical grab bar was constructed of smooth, powder-coated steel, 127.5 cm in length (maximum height 132.5 cm above the bathtub rim, 173.5 cm above the bathroom floor and 163 cm above the bathtub floor). Wall-use-only support: Participants touched the wall for support (left arm of the participant—stepping into; right arm of the participant—stepping out). No grab bar was available.
The low and high rim-mounted assistance conditions included in this study were achieved using the same height-adjustable grab bar, constructed of powder-coated steel. The graspable portion of the rim-mounted grab bar was curved, and its grip was oriented parallel to the bathtub rim (see Figure 1). It was positioned as close to the control end of the bathtub as possible while remaining on the straight (not curved) edge of the bathtub. Based on the recommendation of three clinical occupational therapists, the placement aimed to maximize the space between the grab bar and a hypothetical bath seat (if one was present) to mimic clinical recommendations.
For the purpose of this study, the rim-mounted grab bar (RTL12036-ADJ, Drive Medical, Port Washington, NY, USA) was modified such that it could be securely bolted in place. Modification was necessary to ensure participant safety (due to the potential risk of the rim-mounted grab bar dislodging from the rim) and to ensure force recordings were accurate.
Participant Instrumentation and Procedure
Prior to data collection, participants were instrumented with reflective motion capture markers. Rigid clusters and individual markers were placed on the participant's thorax, pelvis, thigh, shank, and feet segments (Greene, 2020), according to international biomechanics standards (Wu et al., 2002; Wu et al., 2005). For safety, participants also wore an overhead harness throughout the protocol.
Following instrumentation, participants were instructed to approach and step into the bathtub, stand for a few seconds, and then step out of the bathtub; they were instructed to use the grab bar (or wall) throughout the trial. To ensure other entry and exit strategies were self-selected, no further instructions were provided. Participants were barefoot throughout testing and could dry their feet upon exiting the bathtub between trials. Both the grab bars and participants’ hands remained dry throughout testing.
Participants completed three trials per assistance condition. All trials for one condition were completed before moving on to another condition. The order of grab bar conditions was randomized.
Exploration of User Perception
Immediately following each condition, after all trials were complete, participants verbally reported on a 5-point Likert scale their perception of safety (very unsafe to very safe), comfort (very uncomfortable to very comfortable), effectiveness (very ineffective to very effective), and ease of use (very challenging to use to very easy to use) of the respective grab bar or wall (Guitard et al., 2011). Responses were recorded by a research team member.
Data Processing and Analyses
Motion capture data were processed using Cortex (Version 6, Motion Analysis Corporation, Santa Rosa, CA) and then modeled in Visual 3D (Version 6, C-Motion, Inc., Kingston, ON). Whole-body centre of mass (COM) and the trunk segment kinematics were determined using a 12-segment, link-segment biomechanical model (bilateral foot, shank, thigh, pelvis, trunk, bilateral upper arm, lower arm, hand). Load cell data were resampled to 250 Hz to allow syncing with motion capture data. All data were filtered using a low-pass Butterworth filter with a cut-off frequency of 6 Hz.
Bathtub entry and exit were analyzed separately. For both bathtub entry and exit, biomechanical variables were determined between trial start (i.e., the instant at which the whole-body COM velocity in the perpendicular axis reached 5% of peak) and trial end (i.e., the instant at which the trailing foot was flat on the floor).
To quantify the postural requirements of the task, the peak forward and lateral trunk flexion angles were determined and measured relative to the global vertical. Peak resultant forces applied to the grab bars were also determined to quantify grab bar loading. Resultant grab bar forces were standardized to participant body weight (% BW) as an indicator of the extent of the grab bar's role in task performance (Nirmalanathan, 2019). To understand the average behavior, all biomechanical variables were reported as a mean of the three trials.
To evaluate the effect of the grab bar assistance condition, a one-way repeated measures ANOVA was conducted for each biomechanical variable of interest, including one within-subject factor (grab bar assistance condition). Mauchly's test of sphericity was conducted, and the Greenhouse–Geisser correction was applied where violated. Post hoc comparisons with Bonferroni corrections were conducted after the identification of a significant main effect. Significance levels were considered at p < .05 for all analyses (Bonferroni correction p < .017). Statistical analyses were conducted in R Version 3.6.3 (R Core Team, 2020) using the package rstatix.
Sociodemographic and clinical data, as well as perception scores (of safety, comfort, effectiveness, and ease of use), were analyzed using descriptive statistics and presented with mean and standard deviations or frequency and percentage, computed with Microsoft Excel.
Findings
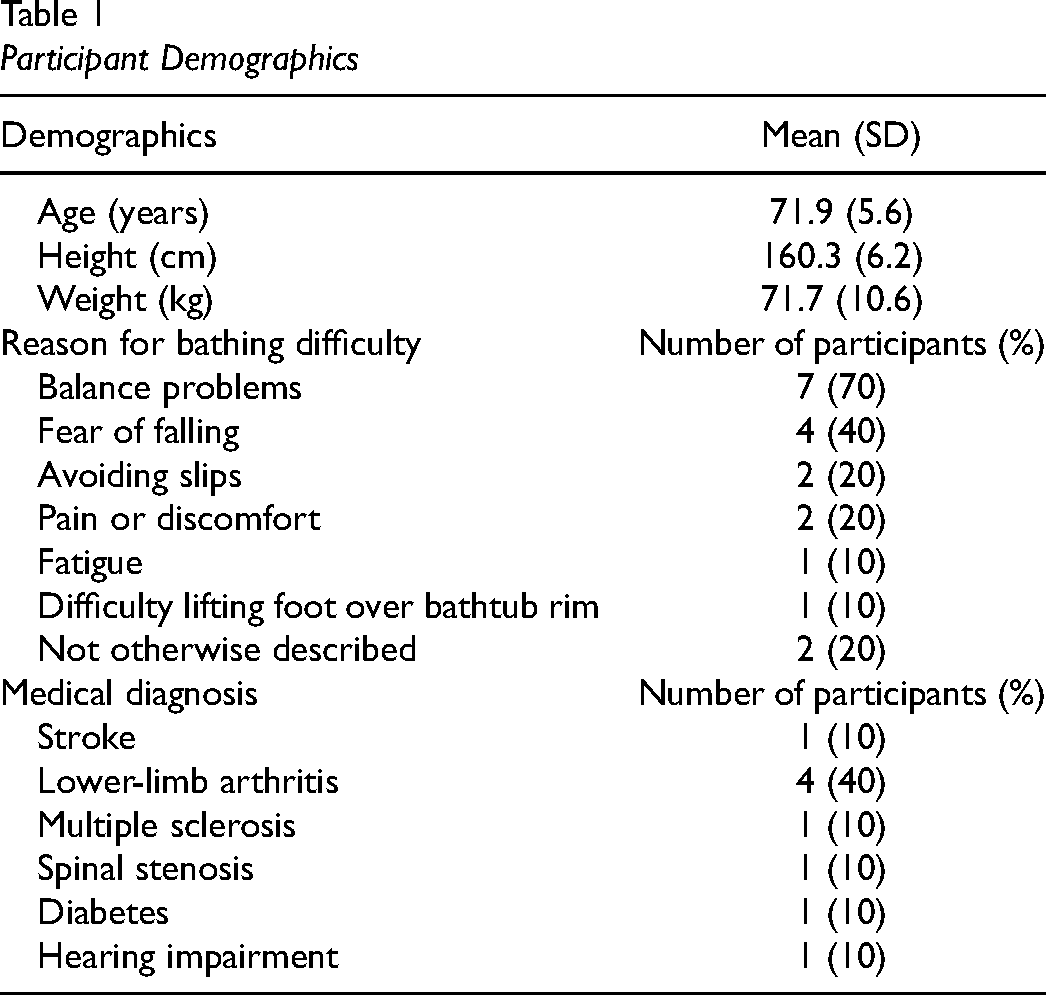
Ten older adults (eight females, two males) participated and they reported a variety of reasons for bathing difficulty (Table 1). The number of reasons indicated by individual participants ranged from 0 to 5, with a mean of 1.8 reasons cited across all participants. In addition to bathing difficulty, participants also presented with medical diagnoses (Table 1).
Participant Demographics
Four of the ten participants refused to complete the wall-use (i.e., no grab bar) condition (reasons were not documented). For one additional participant, the motion capture data for the wall-use condition were not collected due to technical difficulties during data acquisition. Accordingly, statistical comparisons for measures of posture and loading were not made between the wall-use condition and grab bar conditions. All participants completed the protocol with the use of the other grab bar assistance conditions.
Postural Requirements
Peak forward trunk flexion differed significantly by grab bar assistance condition during both entry (F(1.74, 15.70) = 33.12, p < .001) and exit (F(1.25, 11.21) = 46.67, p < .001, Figure 2). Use of the low rim-mounted grab bar resulted in greater forward trunk flexion when compared to the high rim-mounted grab bar (∼25% greater during entry (t = −5.41, p = .001); ∼28% greater during exit) (t = −8.93, p < .001)) and the vertical grab bar (∼51% greater during entry (t = 6.89, p < .001); ∼73% greater during exit (t = 7.53, p < .001). While to a lesser extent than the low rim-mounted grab bar, the high rim-mounted grab bar also resulted in greater trunk flexion when compared to vertical grab bar use during bathtub entry (21% greater) and exit (36% greater) (t = 3.62, p = .017 and t = 4.61, p = .004, respectively). There was no significant main effect of the grab bar assistance condition on measures of lateral trunk flexion during bathtub entry (14.7 ± 4.1°, F(1.58, 14.19) = 2.31, p = .142) or exit (15.5 ± 4.8°, F(1.66, 14.97) = 1.56, p = .242).
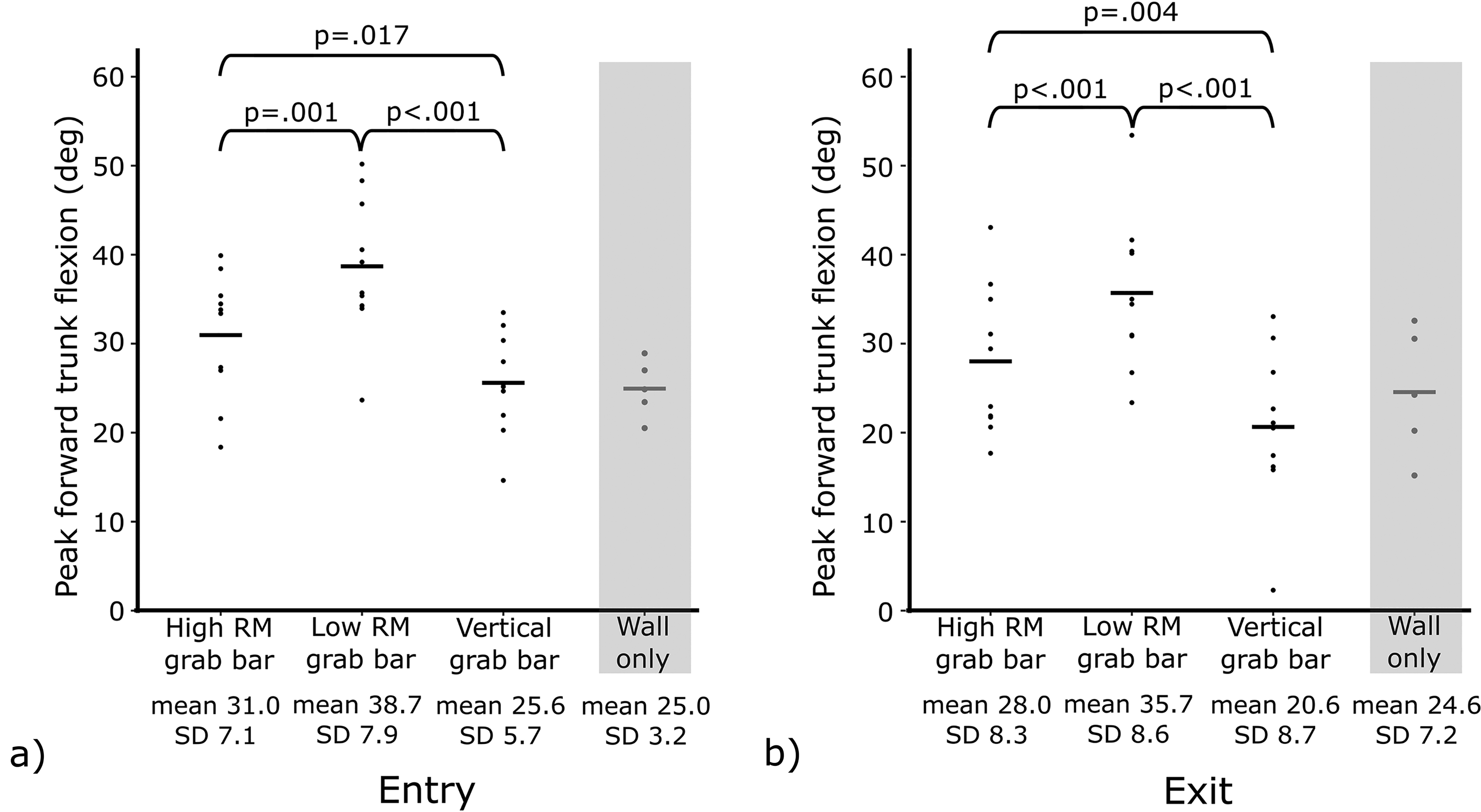
Peak forward trunk flexion during entry (a) and exit (b) for the three grab bar conditions (high rim-mounted (RM) grab bar, low rim-mounted grab bar, and vertical grab bar) and wall use. Data are presented for individual participants (dots), with the participant mean for each condition (horizontal line). Pairwise comparison p-values are specified in the figure. Note: the plot includes wall data (shaded gray area) for visual comparison; wall data were not included in statistical analyses.
Grab Bar Loading
Peak grab bar loading is summarized in Figure 3. During both bathtub entry and exit, there was a significant main effect of grab bar assistance condition on grab bar loading (F(1.38, 11.05) = 54.11, p < .001 and F(1.27, 10.18) = 15.55, p = .002, respectively). Pairwise comparisons revealed that participants applied less force on the vertical grab bar than the high or low rim-mounted grab bars while stepping into (t = 12.30, p < .001 and t = 7.66, p < 0.001, respectively) and out of the bathtub (t = 4.09, p = .010 and t = 4.16, p = .010, respectively) (>50% less force during entry and >30% less force during exit). No significant difference was found between the high and low rim-mounted grab bars during bathtub entry (t = −1.56, p = .474 or exit (t = −2.63, p = .091).
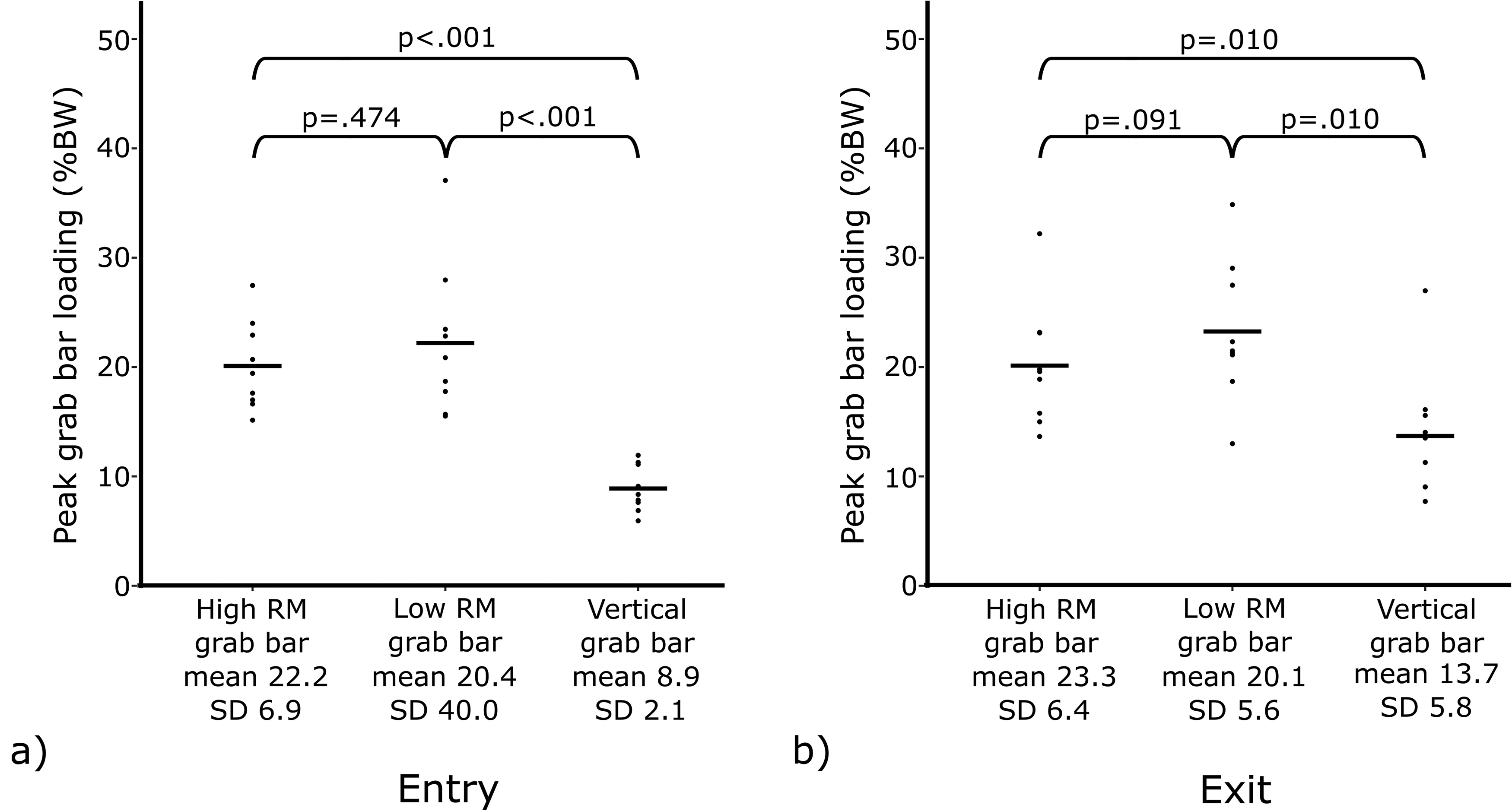
Peak grab bar loading, standardized to body weight (%BW), during bathtub entry (a) and exit (b for the three grab bar conditions (high rim-mounted (RM) grab bar, low rim-mounted grab bar, and vertical grab bar). Data are presented for individual participants (dots), with the participant mean for each condition (horizontal line). Pairwise comparison p-values are specified in the figure.
Perception of Safety, Comfort, Effectiveness, and Ease of Use
Participant ratings of each grab bar condition have been summarized in Figure 4, including the perception of safety, comfort, effectiveness, and ease of use. In terms of safety perception, the vertical grab bar was rated as very safe by all participants, while the high and low rim-mounted grab bars were rated as “very safe” or “safe” by 70% and 40% of participants, respectively. Four participants refused to complete the wall condition, and participants that completed the wall-only condition rated it as neutral, safe, or very unsafe, with neutral as the highest rating. Perceived comfort, effectiveness, and ease of use followed similar trends.
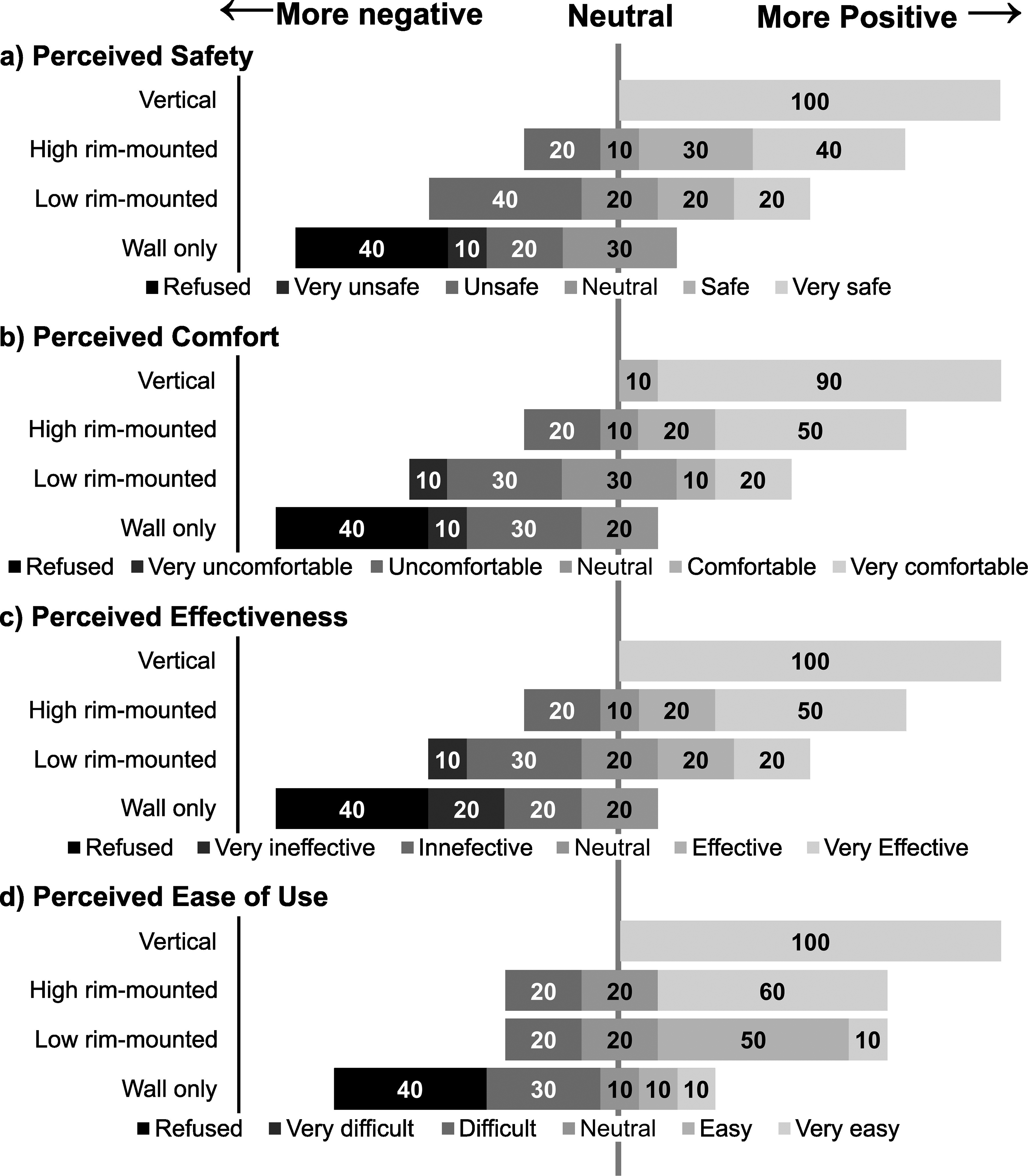
From top to bottom: perception of safety, comfort, effectiveness, and ease of use for each assistance condition. Divergent bar plots display percent of participants who selected each response, aligned to neutral responses. Responses to the left of the neutral line are negative responses or conditions that were refused by participants; responses to the right of the neutral line are positive.
Discussion
This study examined postural requirements and grab bar loading for older adults with bathing difficulty as they stepped in and out of a bathtub while using a low rim-mounted grab bar, high rim-mounted grab bar, vertical grab bar, and the wall for assistance. Our main findings indicated that participants adopted a more forward-flexed trunk while using the low rim-mounted grab bar, while the least degree of flexion corresponded with vertical grab bar use. Grab bar loading was also greater on both rim-mounted grab bars compared to a vertical grab bar. While the high rim-mounted grab bar did not offer any advantage compared to the low rim-mounted grab bar with respect to force requirements, it did require comparatively less forward trunk flexion. Aligning with the biomechanical findings, the vertical grab bar was frequently rated highly on safety, comfort, effectiveness, and ease of use by participants. Taken together, the findings suggest that a vertical grab bar can reduce task demands through a lesser range of motion and reduced force requirements compared to both the high and low rim-mounted grab bars.
Posture considerations are important when completing a challenging task such as bathtub entry and exit. Participants limited forward trunk flexion to the greatest extent with vertical grab bar use while adopting the most flexed posture with the low rim-mounted grab bar. Adopting a more forward-flexed posture during an obstacle-crossing task can alter musculoskeletal demands on the spine (Takahashi et al., 2006). For individuals with a limited range of motion, such as those with arthritis (Machado et al., 2010), low back pain (Reis & Macedo, 2015), or obesity (Larsson & Mattsson, 2001), greater flexion requirements may limit successful task completion in the absence of compensatory movements. Other demands associated with stooping forward and standing up include blood pressure effects and increased demands on the vestibular system, both of which can challenge balance systems. While we did not achieve a large enough participant sample to statistically evaluate the preference outcomes, the low rim-mounted grab bar was frequently rated in the neutral to poor range across comfort, effectiveness, and ease of use, which may reflect the greater forward flexion required to use it.
Control of the flexed trunk is also critical for balance control and fall avoidance (Goldberg et al., 2005; Grabiner et al., 2008). As one flexes forward, the moment of force acting on the trunk increases due to the longer moment arm (McGorry et al., 2001); these moments must be counteracted by postural muscles in order to maintain stability (Grabiner et al., 2008; Saha et al., 2007). When considered alongside other typical changes associated with aging, such as reduced strength (Alexander, 1994; Doherty, 2001; Kovacs, 2005) or vestibular system changes (Allen et al., 2016), greater trunk flexion may limit an older adult's ability to generate the necessary postural responses to maintain dynamic balance during an obstacle crossing task (Hahn et al., 2005). Owings and colleagues (2001) found that greater forward trunk flexion at the time of balance loss increases the risk of falls. The trunk flexion angles we observed for the rim-mounted grab bars, particularly the low rim-mounted grab bar, in many cases exceed the trunk flexion reported by Owing and colleagues for successful balance recovery at foot flat following balance loss (mean (SD) 30.3° (8.8°)) and approach the trunk flexion reported for failed balance recovery (45.8°(13.6°)); considering the high level of trunk flexion when no balance loss has yet occurred, trunk flexion during a balance loss during bathing transfer may increase further. Consequently, the larger forward trunk angle while using the rim-mounted grab bars may also have implications for one's ability to maintain balance and recover balance in the event of a balance loss. If an individual were to lose balance while using a rim-mounted grab bar, particularly when set at a low height inducing even more trunk flexion, they may be in a more compromised position with respect to fall avoidance compared to a vertical grab bar. Further research investigating the use of the rim-mounted grab bars following balance loss is needed to determine if this is indeed the case. In a homecare setting, health professionals such as occupational therapists, could consider whether a rim-mounted grab bar is tall enough for a person who wishes to use one; if excessive trunk flexion is observed, alternative assistive devices might be favored.
Along with posture, considerations of grab bar loading may have implications for safe use. Using the vertical grab bar allowed participants to step into and out of the bathtub while applying lower forces compared to the high and low rim-mounted grab bars. Conversely, participants applied the highest forces on the low rim-mounted grab bar (mean of 23% body weight), double the force on the vertical grab bar during entry and nearly double during exit. Similarly, a recent study found that younger adults loaded vertical grab bars up to 19% of their body weight while stepping into the bathtub, sitting down within the tub, standing up, and stepping out, but loaded horizontal grab bars up to 28% BW for the same task (Guay et al., 2020). While lower applied loads do not necessarily translate to improved safety, it has been suggested that high applied handhold forces are a compensatory strategy to increase stabilizing moments with handholds of lower heights (Komisar et al., 2018; Maki & Fernie, 1988). The vertical grab bar accommodates a higher grasping height allowing users to apply lower forces to achieve a similar stabilizing moment. In the absence of a similar moment arm advantage with the rim-mounted grab bar, users may compensate by applying greater forces, as demonstrated in the present study. Similarly, the forward trunk flexion observed for the rim-mounted grab bar may make it more difficult for the user to produce sufficient internal stabilizing moments (Alexander, 1994; Doherty, 2001; Saha et al., 2007) and individuals may compensate by relying more heavily on the grab bar. Ultimately, the loads applied to the grab bar must be considered with reference to the load sustainable by the grab bar. While we did not test the failure load of any of the grab bars in this study, future work should evaluate what loads can be sustained by the grab bars. As temporary grab bars are designed to be installed by the user, rather than a professional, it is unclear whether rim-mounted grab bars are typically installed effectively to sustain the loads applied during bathing transfers as intended. Users may not install the device as intended by the manufacturer, which is likely critical for the performance outcomes of the grab bars; this also requires further investigation.
Due to the small sample size of participants with wall-only condition data (n = 5), statistical analyses were not conducted including this condition. During both entry and exit, peak forward trunk flexion means were similar between wall use and vertical grab bar use (mean difference, entry = .6, exit = 4.0°), so postural demands may be minimized. However, a wall offers no graspable surface on which to apply stabilizing forces and no rigid support for the user to anchor the body in the event of a slip (King & Novak, 2017; Komisar et al., 2018; Maki & McIlroy, 1997). Older adults require grab bars to regain balance nearly 60% of the time following a perturbation (Guitard et al., 2011). Similarly, Levine et al. (2021) found that younger adults were also 75% less likely to experience a fall or balance loss when a grab bar was present during a balance perturbation, compared to a wall-only condition. It is plausible that these changes would be more pronounced for older adults or persons with bathing difficulty. Therefore, despite the potentially lower postural demands observed with wall use, this option has been shown to be associated with a greater risk of falling (Guitard et al., 2011; King & Novak, 2017; Levine et al., 2021). A wall only to support while stepping over the edge of the bathtub rim may further explain why four participants refused to complete this assistance condition and why the wall was rated as unsafe by seven out of the 10 participants.
There are some limitations to be acknowledged. First, this study included four assistance conditions, with one rim-mounted grab bar tested at its maximum and minimum height. However, other designs of temporary rim-mounted grab bars exist. For example, some rim-mounted grab bars have a graspable portion perpendicular to the bathtub rim, rather than the parallel configuration of the grab bar in this study. Therefore, the limited number of conditions tested does not represent all options commercially available or recommended by health professionals, including occupational therapists. Still, all available rim-mounted grab bars are limited in height due to the trade-off between grab bar height and load required at the clamp–rim interface. The magnitude and importance of this effect was demonstrated by the rim-mounted grab bar model used in this study. Future studies may improve understanding of the effect of design elements such as handle configuration, material or texture on biomechanical outcomes during transfers and balance recovery. Second, this study examined grab bar use only while stepping into and out of the bathtub only; grab bars may be used for other portions of bathing or the occupation of personal hygiene. Tasks such as adjusting the faucet or sitting down in the bathtub could be considered in future studies. Third, the rim-mounted grab bar was modified such that it was securely bolted in place, rather than attached temporarily. While this was necessary for the study, it presents limitations. Given its temporary nature, installation challenges or contaminants such as water, soap, and repeated use could weaken the integrity of the grab bar–bathtub interface. Since the findings of the present study indicate that while stepping in and out of the bathtub, users apply high forces on the rim-mounted grab bars, it is unknown whether a temporary rim-mounted grab bar could withstand these forces without dismounting from the bathtub rim. This gap also highlights another important consideration for safety: to investigate, including using mechanical testing, whether the forces applied to the rim-mounted grab bar during nonfalling scenarios, such as those applied during this study, or during a slip, could cause the grab bar to dislodge from the bathtub rim. Fourth, while we evaluated biomechanical metrics separately for bathtub entry and exit, we only evaluated perceptions of the grab bar for the entire bathtub entry/exit transfer. Some participants may have perceived a grab bar more or less favorably for entry or exit, which may have biased the perception scores higher or lower. However, in a real-world scenario, a grab bar user would likely have the same grab bar(s) installed for both tasks and would be unable to change grab bars between entry and exit, so our perception data captures the overall performance of each grab bar. Finally, we did not have enough statistical power to analyze the grab bar preference data; however, participant preference and perception likely had a significant impact on outcomes such as whether or not a participant refused a condition, or how much they felt comfortable loading a grab bar. It would be valuable to undertake future research regarding preferences and perceptions of factors such as safety and comfort, as well as broader factors in home modification decision-making, such as cost or style, in selecting and using bathing assistive devices.
Conclusion
Our findings demonstrate that the type of grab bar used to assist with stepping into and out of the bathtub impacts posture and grab bar loading; this provides evidence beyond the perception of safety or comfort. Our results suggested that the vertical grab bar reduced task demands through a lesser range of motion and reduced force requirements compared to both the high and low rim-mounted grab bars and was favorably perceived by participants. While the high rim-mounted grab bar did not offer any advantage compared to the low rim-mounted grab bar with respect to force requirements, the required forward trunk flexion was smaller. Overall, this work provides empirical results, highlighting the effect of rim-mounted grab bars on biomechanical measures of safety and task demands while stepping into and out of the bathtub. For bathing entry and exit transfers, occupational therapists may want to consider those results suggesting a permanently mounted vertical grab bar to be installed. For situations where a vertical grab bar cannot be installed, and a rim-mounted grab bar is preferred, clinicians should consider whether the height of a rim-mounted grab bar is adequate for a person. In the absence of clinical guidelines for acceptable trunk flexion with respect to balance, clinicians should select a grab bar that minimizes trunk flexion for their clients. Finally, clinicians should ensure that the grab bar can be installed on the bathtub rim such that it supports the loads applied during bathing transfers.
Key Messages
The type of grab bar used during bathing transfers has implications for postural demands.
Permanent vertical grab bars minimize postural demands and loading requirements, compared to the rim-mounted grab bar included in this study.
Nearly half of the participants refused to get in and out of the bathtub with the wall-only (i.e., no grab bar) support highlighting the importance of general grab bar availability in bathrooms.
A permanent, vertical grab bar is favorably perceived by users; the low rim-mounted grab bar or wall assistance was unfavorably perceived by a high percentage of users.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from the Canadian Institutes of Health Research (Project Grant #159579). The third author received salary support from the Fonds de Recherche du Québec—Santé.