
Abstract
Introduction
Low back pain (LBP) is a leading cause of disability and a growing global health problem (Clark & Horton, 2018). Prevalence rates of pregnancy-related LBP (PLBP) or pregnancy-related pelvic girdle pain (PPGP) of 34% to 45% have been identified among pregnant people (Shijagurumayum Acharya et al., 2019; Wu et al., 2004). Of those who experience PLBP, about 20% continue to experience back pain 3 years after childbirth (Norén, et al., 2002) and one in 10 of those with PPGP has severe consequences for up to 11 years (Elden et al., 2016).
Although terminology is used variably, “pregnancy-related pelvic girdle pain”, and “pregnancy-related low back pain” are recognized terms and while they are distinct entities, they can together be considered “pregnancy-related lumbopelvic pain” (Wu et al., 2004). The etiology of pregnancy-related lumbopelvic pain is unknown however it is considered to be multifactorial and associated with biomechanical, vascular, and hormonal changes (Manyozo et al., 2019).
Risk factors for the development of pregnancy-related lumbopelvic pain are a history of low back/pelvic pain (Ceprnja et al., 2021; Kovacs et al., 2012), younger maternal age, higher fetal weight, increased joint mobility, higher body mass index, depression (Kovacs et al., 2012; Wiezer et al., 2020), a heavy workload (Wiezer et al., 2020) increasing parity, greater duration of time spent standing (Ceprnja et al., 2021) and previous trauma to the bony pelvis (Kanakaris et al., 2011). Psychosocial factors including depression, anxiety, fear avoidant beliefs, and catastrophizing are associated with pregnancy-related lumbopelvic pain and the persistence of lumbopelvic pain postpartum (Doğru et al., 2018; Elden et al., 2016; Fernando et al., 2020; Olsson et al., 2012).
Postpartum depressive symptoms are 3 times more prevalent in those with pregnancy-related lumbopelvic pain than those without (Matsuda et al., 2020). Several studies have found that lumbopelvic pain in pregnancy limits performance of daily activities and leads to decreased health-related quality of life (Gomes et al., 2013; Gutke et al., 2018; Stapleton et al., 2002).
High-quality studies evaluating effective interventions for pregnancy-related lumbopelvic pain are lacking despite the prevalence and impact of the condition. A Cochrane Review of interventions for preventing and treating low back and pelvic pain during pregnancy concluded that more and better designed research on interventions to prevent and treat low back and pelvic pain during pregnancy is needed including further research on conservative (e.g., exercise therapy, education, and manual therapy) and complementary treatments (e.g., acupuncture) (Liddle & Pennick, 2015). Occupational therapists are well placed to work with people with pregnancy-related lumbopelvic pain. Occupational therapy has a well-established role in services for people with chronic pain conditions and makes a unique contribution due to its overarching focus on occupation (Lagueux et al., 2018) offering interventions to enable participation in occupation including goal-setting, energy conservation, pacing, self-management, grading activity, and sleep hygiene (Robinson et al., 2011). Occupational therapists enact components of cognitive-behavioural treatments such as promotion of self-management, cognitive restructuring, problem solving, habit reversal, and behavioral activation including goal-setting and pacing (Skjutar et al., 2010; Stanos, 2012). Furthermore, occupational therapists can facilitate parenting occupations and development of parenting skills in those parenting with a physical disability or in difficult social circumstances (Lim et al., 2022; Pastor-Bédard et al., 2022; Wint et al., 2016). Despite the alignment of occupational therapy skills and services with the needs of this population we identified no papers describing occupational therapy practice with pregnant people with lumbopelvic pain.
Qualitative evidence synthesis brings together data from multiple studies and is useful in providing evidence on service users experiences of healthcare and health conditions (Cahill et al., 2018; Hammell, 2001), stakeholder preferences (Noyes et al., 2022) and is valuable in intervention development (Flemming et al., 2019). Qualitative evidence syntheses have been completed on experiences of persistent pelvic girdle pain (PGP) after childbirth (Srisopa & Lucas, 2021) and PPGP (Mackenzie et al., 2018). To date, qualitative literature on the experience of pregnancy-related lumbopelvic pain has not been synthesized. This paper aims to address this gap by identifying and synthesizing existing qualitative research on people's experiences of pregnancy-related lumbopelvic pain during pregnancy or during the postpartum period.
Methods
A systematic review and qualitative evidence synthesis was conducted. The review protocol was registered with Prospero (CRD42021286483). Qualitative evidence synthesis (QES) refers to “a diverse set of methods for combining the data or the results of multiple studies on a topic to generate new knowledge, theory and applications” (Drisko, 2020, p. 736). Barnett-Page and Thomas present an overview of the varied methods for the synthesis of qualitative research for those new to QES. The method of QES we selected was meta-ethnography. This is the most popular method approach to QES and was first described by Noblit and Hare in the 1980s (1988). We selected meta-ethnography as it allows researchers to move beyond summarizing the studies included in a review to generate novel interpretations and conceptual innovation of the phenomenon under study (Cahill et al., 2018; Srisopa & Lucas, 2021).
Terminology
We use the term “pregnant people” throughout this paper in recognition that many people who have uteri including women, transgender men, and nonbinary people can experience pregnancy (MacKinnon et al., 2021).
Search Strategy
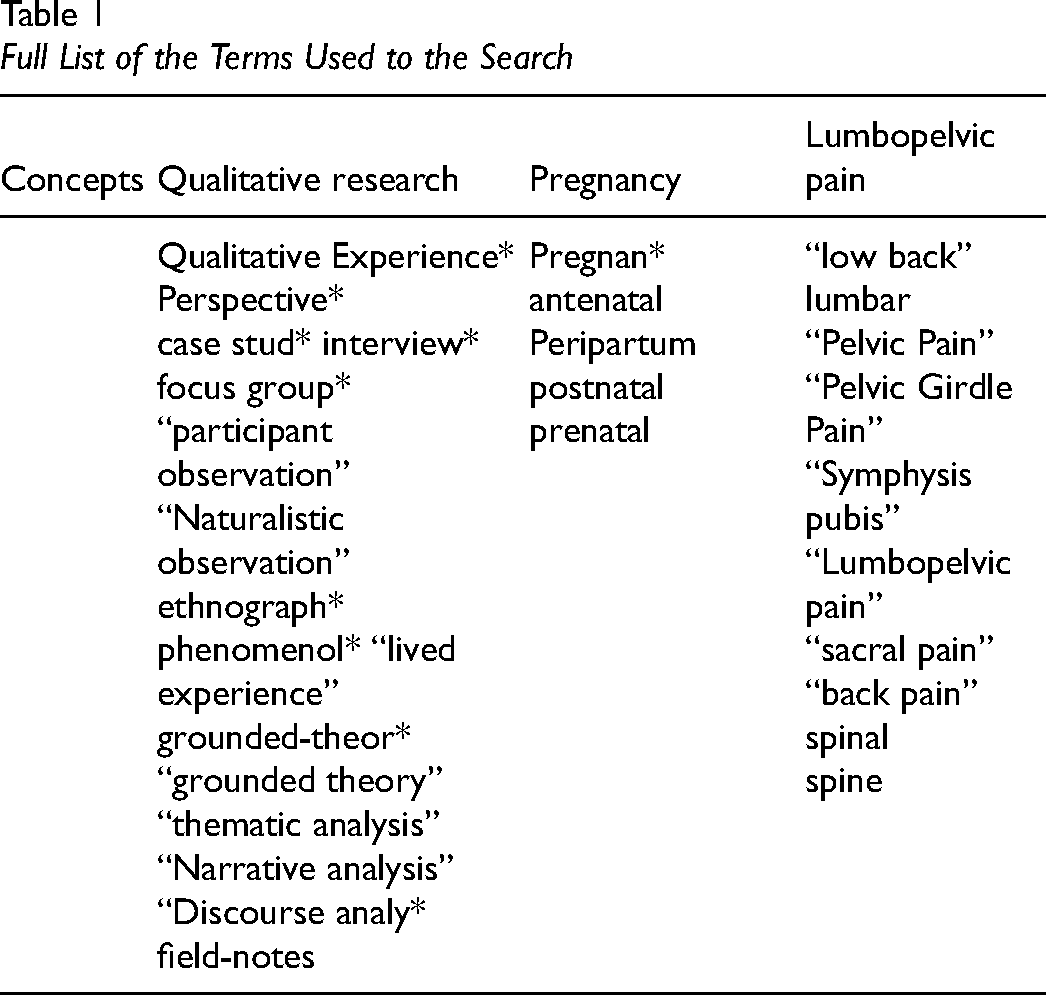
A keyword search of four electronic databases (MEDLINE, CINAHL, PsycINFO, and PsycArticles) was conducted simultaneously through the EBSCOhost platform in September 2021 and was updated in June 2022. MEDLINE and CINAHL are the most frequently searched databases in qualitative syntheses (Booth, 2016). PsycINFO and PsycArticles databases were selected given the review focus on lived experiences. The search was limited to the years 2000 to 2022 and to publications in English language. Three key concepts were used (qualitative research, pregnancy, and lumbopelvic pain). Please see Table 1 for the full list of search terms used.
Full List of the Terms Used to the Search
Inclusion and Exclusion Criteria
Database search results were exported to Rayyan QCRItool (Rayyan Systems Inc., Cambridge, MA, USA; Ouzzani et al., 2016) where duplicates were removed and two research team members (LB and KR) independently examined all search results, reviewing titles, and abstracts according to the following inclusion criteria:
Qualitative study reporting use of recognized methods of qualitative data collection and analysis. Participants are pregnant people or people in the postpartum period. Participants have pregnancy-related lumbopelvic pain (given that previous experience of back or pelvic pain is a major risk factor for pregnancy-related lumbopelvic pain, studies where participants did/did not have previous experience of lumbopelvic pain were included). Study findings report on the experience of living with pregnancy-related lumbopelvic pain.
All included studies were read in full (full-text review) to ensure they met all inclusion criteria by two researchers (LB & KR) and the reference lists of all included studies were checked to identify potential studies for inclusion. Data was extracted from included studies by two members of the team (LB & KR) independently using a custom template and all included studies were appraised using the Critical Appraisal Skills Program qualitative studies checklist (Tong et al., 2007). Disagreements during screening, full-text review, and quality appraisal were resolved through discussion. Qualitative Data analysis software NVivo (QSR International Pty Ltd., 2020) was used to manage the data extraction and synthesis (Bergin, 2011).
Data Analysis
Analysis followed the seven phases of meta-ethnography outlined by Noblit and Hare (1988) and recent publications (Cahill et al., 2018; Cunningham & Uny, 2020) and the eMERGe reporting guidance (Fiani et al., 2020). The full-text pdfs of included papers were uploaded to NVivo software (QSR International Pty Ltd., 2020) and were read in an intensive, repetitive, and a highly active manner (Alam, 2021). Then key concepts or metaphors or themes were extracted from the included studies. The term “first order constructs” refers to direct quotes from participants in the included studies, “second order constructs” refers to interpretations by the authors of the included studies and “third order constructs” are the findings generated by the authors of a meta-ethnography (Vincent & Evans, 2021). Following identification of second order constructs in the included studies they were coded in NVivo and juxtaposed across studies. Next common concepts from studies were grouped together (Stensland & Sanders, 2018) and then translated. We conducted a reciprocal translation as concepts across studies were directly comparable (Stensland & Sanders, 2018). As concepts from individual studies were translated into one another, concepts representing more than one study were generated. In the final analytic phase, we aimed to view the studies as a whole rather than as parts and integrated the concepts identified across the studies to develop a fresh interpretation of our phenomenon of interest (Cahill et al., 2018; Noblit & Hare, 1988).
Positionality
The search and analysis were completed by an occupational therapy PhD candidate (LB) and an occupational therapy academic (KR) who both have clinical experience of working with people with chronic pain.
Findings
Included Studies
Initial searches retrieved 1965 articles. After removal of duplicates, title and abstract screening 29 records were selected for full-text reading and 23 articles were included for analysis. The process is shown in a PRISMA flowchart diagram (Page et al., 2021) in Figure 1.
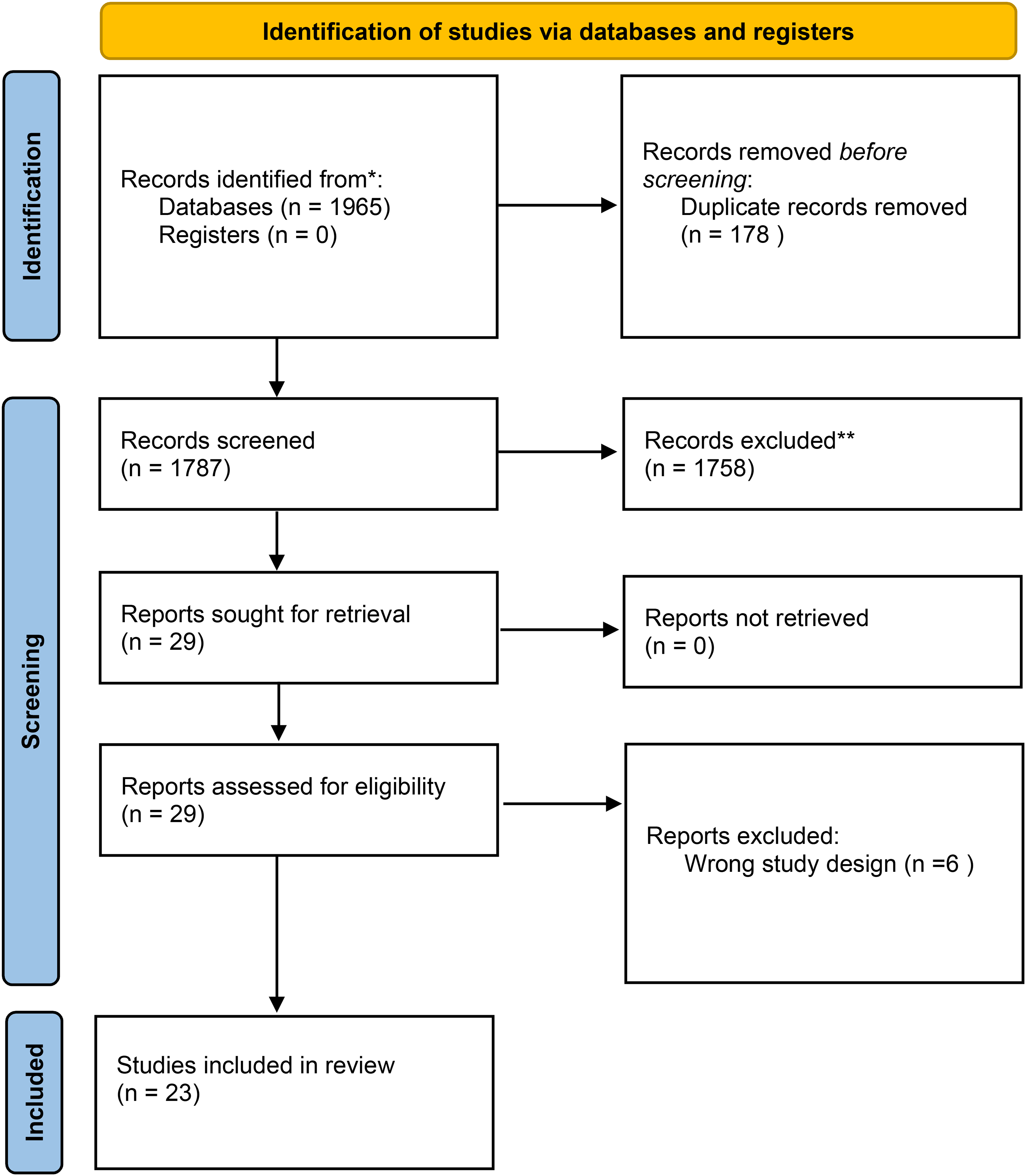
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only.
Characteristics of the Included Studies
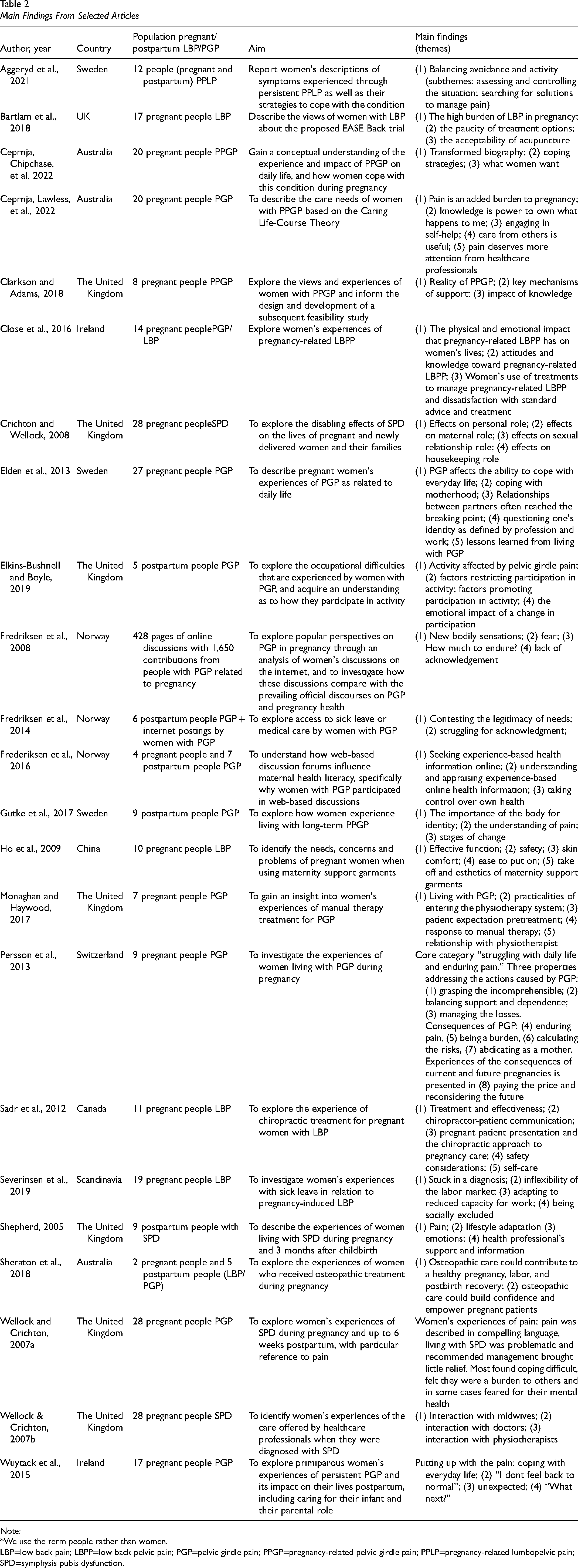
Characteristics of the included studies are presented in Table 2. Of the 23 studies, four studies included those with PLBP only (Bartlam et al., 2018; Ho et al., 2009; Sadr et al., 2012; Severinsen et al., 2019), three studies included those with PLBP and those with PPGP(Aggeryd et al., 2021; Close et al., 2016; Sheraton et al., 2018) and the remaining 16 included people with PPGP only.
Main Findings From Selected Articles
Note:
*We use the term people rather than women.
LBP=low back pain; LBPP=low back pelvic pain; PGP=pelvic girdle pain; PPGP=pregnancy-related pelvic girdle pain; PPLP=pregnancy-related lumbopelvic pain; SPD=symphysis pubis dysfunction.
Quality Appraisal
Results of the quality appraisal are presented in Table 3.
Results of the Quality Appraisal (Critical Appraisal Skills Program)
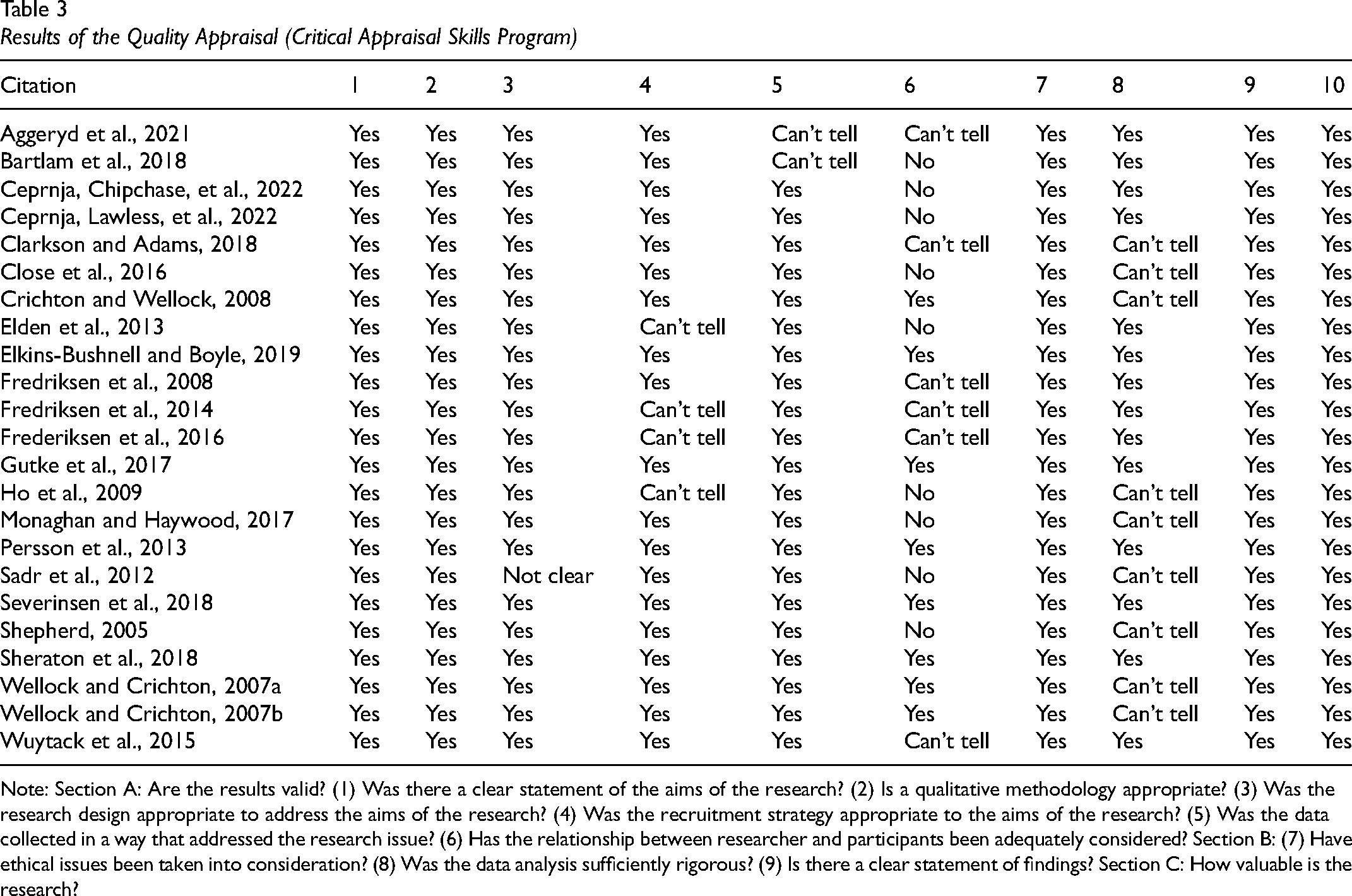
Note: Section A: Are the results valid? (1) Was there a clear statement of the aims of the research? (2) Is a qualitative methodology appropriate? (3) Was the research design appropriate to address the aims of the research? (4) Was the recruitment strategy appropriate to the aims of the research? (5) Was the data collected in a way that addressed the research issue? (6) Has the relationship between researcher and participants been adequately considered? Section B: (7) Have ethical issues been taken into consideration? (8) Was the data analysis sufficiently rigorous? (9) Is there a clear statement of findings? Section C: How valuable is the research?
List of Themes
Analysis identified four higher order themes:(1) uncertainties about pregnancy-related lumbopelvic pain, (2) struggles to achieve treatment and pain management, (3) profound activity consequences, and (4) emotional wellbeing, relationship, and identity impacts of pregnancy-related lumbopelvic pain.
“The information about SPD [Symphysis Pubis Dysfunction] isn’t widely available, there is not enough information on it, there ought to be leaflets in doctors surgeries or things like that the doctors can give you.” (Iris) (Shepherd, 2005)
In a study analyzing discussions about PGP and LBP on the internet participants indicated that most of their information comes from others living with PGP/LBP which may be of poor quality or misleading (Frederiksen et al., 2016). In one study people thought the reason they developed lumbopelvic pain was because they were in poor physical shape at the time of the pregnancy or labor (Aggeryd et al., 2021). “I think that I would have had less problems if I had been better at exercising. When I just had my baby, my abdominal muscles were so weak I think that's why I got so many problems.” (Participant 6) (Aggeryd et al., 2021)
Across multiple studies participants reported that they or healthcare providers viewed pain, but not specifically lumbopelvic pain, as inherent to pregnancy (Bartlam et al., 2018; Clarkson & Adams, 2018; Close et al., 2016; Elden et al., 2013; Fredriksen et al., 2008; Monaghan & Haywood, 2017; Severinsen et al., 2019; Shepherd, 2005; Wuytack et al., 2015). Participants perceived healthcare providers lacked understanding of pregnancy-related lumbopelvic pain which led to treatment delays and inadequate care (Fredriksen et al., 2014; Monaghan & Haywood, 2017; Shepherd, 2005). One study described how midwives, doctors, and physiotherapists need to be more receptive, sensitive, and empathizing with pregnant people in pain (Wellock & Crichton, 2007b). “I told the doctor about my terrible back pain, but he did not make any comments .He gave me the sick leave, and sent me out. He may have been busy, but he only offered me 3 minutes. He did not mention physiotherapy, he did not examine my back or my pelvis, he did not tell me what to avoid or what to do in order to recover.”(Fredriksen et al., 2014)
Acupuncture was used by some participants for pain management, however reservations were expressed about the lack of evidence on the effects and potential risks (Bartlam et al., 2018). Paracetamol was a commonly used analgesic (Aggeryd et al., 2021; Close et al., 2016; Elkins-Bushnell & Boyle, 2019), however fear of taking medication because of possible harm to the baby was reported (Clarkson & Adams, 2018; Close et al., 2016; Elkins-Bushnell & Boyle, 2019). “You can’t take medication when you’re pregnant apart from paracetamol and that doesn’t work… If it was safe for the baby, fine, if it didn’t affect the baby.” (P7) (Clarkson & Adams, 2018)
Studies point to an ambivalent attitude toward the use of exercise as a treatment. There was awareness of exercises as a form of treatment for pregnancy-related lumbopelvic pain, especially core strengthening and stretching, but few reports of adherence (Gutke et al., 2018; Sadr et al., 2012). Participants mentioned yoga, walking, Pilates, and swimming as good for symptom relief (Close et al., 2016; Wellock & Crichton, 2007a, 2007b). However, there were reports of worsening pain at the beginning of the exercises and improved wellbeing by doing them (Aggeryd et al., 2021). “My exercise is like a routine, I can experience a lot of pain when I start, but I know exercising makes me feel better afterwards. Sometimes I have to take painkillers to be able to exercise.” (Participant 3) (Aggeryd et al., 2021)
Participants report that the use of abdominal belts or belts reduces the pressure on the back; however, there is concern about the ease of changing these clothes, as well as safety, esthetic, and comfort concerns (Ho et al., 2009). “This (the brief C) one is difficult to wear and the belly gets in the way…it's difficult even when I put on underwear…before I am pregnant, I can just stand and wear it easily, now I have to sit on a chair first and then put it on slowly…(P3, housewife aged 30)” (Ho et al., 2009)
To manage pain and/or improve function, participants used hot water bottles, hot baths, pillows, adjustable beds, acupressure mats, transcutaneous electrical neurostimulation and pregnancy clothing and belts (Aggeryd et al., 2021; Ceprnja, Lawless, et al., 2022; Close et al., 2016; Elkins-Bushnell & Boyle, 2019; Ho et al., 2009; Sadr et al., 2012; Wellock & Crichton, 2007a, 2007b), adaptations in movement or environment or footwear and specialist devices (Aggeryd et al., 2021; Close et al., 2016; Elkins-Bushnell & Boyle, 2019; Fredriksen et al., 2008; Gutke et al., 2018; Ho et al., 2009; Sadr et al., 2012). Some participants needed crutches (Close et al., 2016), others needed adaptations at home, such as using long cables to remove clothes from the washing machine or a table with wheels to stand with support (Aggeryd et al., 2021; Elkins-Bushnell & Boyle, 2019). Activity planning and task avoidance were reported to prevent pain exacerbation, for example choosing fewer active games with their children or online shopping (Aggeryd et al., 2021; Elkins-Bushnell & Boyle, 2019).
“In the morning when I get up, I kind of crawl out of bed…”(Bartlam et al., 2018)
Due to the pain, it was not easy to carry children, bathe them, dress them, run after them, play on the floor or participate with them in outdoor activities, such as playing, riding a bicycle and going to the park (Crichton & Wellock, 2008; Elden et al., 2013; Elkins-Bushnell & Boyle, 2019; Persson et al., 2013; Shepherd, 2005; Wuytack et al., 2015).
Pain affected the ability of pregnant people to participate in social activities due to diminished mobility and sitting tolerance, difficulty accessing places or difficulties engaging in physical activities such as bike riding (Elkins-Bushnell & Boyle, 2019) and in some cases pain led to avoidance of social events and preference for virtual contacts (Clarkson & Adams, 2018). Pain caused difficulty sitting or standing for a long time in the workplace (Close et al., 2016; Elkins-Bushnell & Boyle, 2019; Severinsen et al., 2019). Pain was described as exhausting, resulting in an increased need for rest. However, during sleep and relaxation, pain is often most perceived (Close et al., 2016) and pain also affects the quality of sleep: moving in bed can cause pain and lead to awakening, and pregnancy does not allow better posture choices at bedtime (Aggeryd et al., 2021; Persson et al., 2013; Shepherd, 2005). “When you are sleeping and the body totally relaxes that seems to be the absolute worst…and at some point, it would wake me…wake me out of my sleep.” (Close et al., 2016)
Three studies outlined PGP impacts on sexual activities including, pain necessitating physical separation from partner in bed, inability to have sex due to pain (Elden et al., 2013), and decreased libido and frustration with expectations about sex life during pregnancy (Crichton & Wellock, 2008; Persson et al., 2013).
Responses to pain affecting activities varied, with some studies reporting that people “move on” despite the pain and accomplish activities either by getting support from family members, health professionals, or colleagues or by not having a choice to avoid certain activities (Wuytack et al., 2015). Other studies cited examples of people needing to abandon tasks or work during the most critical period of pain (Crichton & Wellock, 2008; Sadr et al., 2012; Shepherd, 2005).
Lack of awareness of pregnancy-related lumbopelvic pain by healthcare providers, colleagues, and employers led to many feeling judged for complaining about symptoms and/or needing sick leave (Close et al., 2016; Elden et al., 2013; Fredriksen et al., 2014). “It feels like my colleagues have to work harder as I’m incapable and then one of my colleague, who has no family nor has been pregnant, has huge problems to understand what this is like… she once said to me: I’ve never met someone panting as much as you do.”(Close et al., 2016)
The struggle between pain and the need to participate in activities led to feelings of frustration, helplessness, dissatisfaction, and affected mood (Monaghan & Haywood, 2017; Persson et al., 2013; Wuytack et al., 2015).
Pregnancy-related lumbopelvic pain led to concern about returning to work after sick leave (Wuytack et al., 2015), and in some cases, there was a need to change jobs because of pain (Aggeryd et al., 2021; Bartlam et al., 2018). Participants reported difficulty accepting a reduction in work (Elden et al., 2013; Severinsen et al., 2019), concern about productivity and fear of sick leave (Close et al., 2016; Crichton & Wellock, 2008). Difficulty completing work tasks led to frustration and concern about working less or overloading colleagues (Elden et al., 2013; Persson et al., 2013; Severinsen et al., 2019). “[I]t was one of the reasons why I actually chose, you know, sick leave, it was also this enormous sense of guilt that, I can’t, I can’t be there for my colleagues the way I want to be.” (I:9) (Severinsen et al., 2019)
Participants report receiving assistance from close family, especially husbands (Ceprnja, Chipchase, et al., 2022; Crichton & Wellock, 2008; Shepherd, 2005) and friends (Wellock & Crichton, 2007a, 2007b; Wuytack et al., 2015) leading to the need to revise expectations in relation to independence. “It's just learning to pace myself really and learning that my body can’t do what it used to do, which is pretty horrible when you’re in your early thirties.” (P3) (Elkins-Bushnell & Boyle, 2019)
Due to difficulties performing domestic tasks, many pregnant people started to share tasks with their partners (Bartlam et al., 2018; Elden et al., 2013; Monaghan & Haywood, 2017). Concerns about the impact of the condition on relationships were articulated and pregnant people described themselves as more sensitive and as having less patience, with moments of conflict with their partners due to the division of tasks and their mood (Elden et al., 2013) and partners, in turn, according to the pregnant people, feel frustrated by having their routine changed with work overload or by having a partner unable to fulfill their role (Elden et al., 2013; Monaghan & Haywood, 2017; Shepherd, 2005). In contrast in one study the care offered by the partner to the person with PGP brought them closer (Elden et al., 2013).
Concerns about the aggravation and persistence of pain after delivery (Aggeryd et al., 2021; Monaghan & Haywood, 2017; Wuytack et al., 2015) and concerns about further pregnancies were reported across the included studies (Aggeryd et al., 2021; Elden et al., 2013; Monaghan & Haywood, 2017; Persson et al., 2013; Shepherd, 2005; Wuytack et al., 2015). “In the past we discussed three or four children. But now I will definitely not commit myself to another pregnancy until they solve this problem.” (Rose) (Elden et al., 2013)
Some also reported fear of childbirth due to lumbopelvic pain (Clarkson & Adams, 2018; Close et al., 2016; Shepherd, 2005). “I had pelvic pain as well and a bit like yourself I was worried about how this baby was going to come out.” Participant 3 (Close et al., 2016)
Difficulty caring for the baby or older children was frequently mentioned as something that concerned participants (Ceprnja, Chipchase, et al., 2022; Shepherd, 2005; Wuytack et al., 2015). Some reported feeling frustrated for not meeting their own or societal expectations of parenting or motherhood (Aggeryd et al., 2021; Elden et al., 2013; Elkins-Bushnell & Boyle, 2019; Gutke et al., 2018; Severinsen et al., 2019; Wuytack et al., 2015). “I am feeling guilty about how I am feeling about this baby. Thinking … maybe better to not have baby. As a mother, there's always guilt. For my son now we are not doing any activities, which is not fair for him. Imagine as a mum how you are feeling, your child is just watching tv and you are just lying down. I wanted to help but I can’t do it.” (Leah) (Ceprnja, Chipchase, et al., 2022)
Many believed they were not good mothers and that pain interfered with their relationships with their children (Aggeryd et al., 2021; Ceprnja, Chipchase, et al., 2022; Crichton & Wellock, 2008; Persson et al., 2013). “I am a caring, loving person, I love to hug people and show them how much I care. But I can’t even hold a little baby, I can’t lift my daughter to hug and to hold her, and I never could. It makes me sad; I don’t feel like a whole person.” (Participant 8) (Aggeryd et al., 2021)
In one study, mothers reported fear of breastfeeding in case it would cause further pain (Shepherd, 2005). Although some felt joy of having a baby despite the frustration and discomfort of pain (Wuytack et al., 2015), others felt sad and inadequate because they wanted to be alone away from their children (Elden et al., 2013) or because they did not want to hug them (Wuytack et al., 2015).
Discussion
Statement of Principal Findings
This review found that lack of awareness, misunderstandings, and uncertainties about pregnancy-related lumbopelvic pain are common (theme1), people living with this condition struggle to access adequate treatment or achieve adequate pain management (theme 2), pregnancy-related lumbopelvic pain has profound impacts on activity participation (theme 3) with negative consequences for emotional wellbeing, relationships, and identity (theme 4).
Across studies included in our review pregnancy-related lumbopelvic pain was reported to affect all areas of occupational performance, including self-care, leisure, work, and rest. This reflects a large body of research on the impact of LBP and musculoskeletal pain (Gizzi et al., 2019; Turk et al., 2016) and the impact of PGP on activities (Gutke et al., 2018; Stapleton et al., 2002). Our findings align with the concept of occupational disruption (Nizzero et al., 2017) whereby changes in activity participation led to negative emotional consequences including experiences of worry, guilt, sadness, frustration, feelings of inadequacy, and helplessness. Activity consequences were also had identity and social implications. Furthermore, in keeping with the concept of occupational disruption (Nizzero et al., 2017) the multitude of effects of PPGP on occupation led to efforts to manage the disruption, for example, by modifying previous occupations. The centrality of occupational disruption to the experience of pregnancy-related lumbopelvic pain supports the development and evaluation of occupational therapy interventions for this population whose needs mirror other people living with ongoing pain conditions where occupational therapists have a well-established role (Lagueux et al., 2018) and offer tools for pain management and activity performance (Skjutar et al., 2010).
We found that people with pregnancy-related lumbopelvic pain struggle to access adequate treatment and this reflects findings from a Cochrane review where some evidence supporting exercise interventions for this population was identified (Liddle & Pennick, 2015). In our review reports of ambivalent attitudes to exercise were reported and there was no clear consensus on helpful or effective interventions. Many self-initiated strategies to manage pain and accomplish activities were reported such as activity planning, task avoidance, use of aids, and environmental adaptations. These strategies reflect approaches used by occupational therapists with people with ongoing pain conditions including the development of coping and problem-solving skills and self-management approaches (Skjutar et al., 2010). It is important to note that only a proportion of people with pregnancy-related lumbopelvic pain develop chronic symptoms, 20% have continued symptoms 3 years postpartum (Norén, Östgaard, Johansson, Östgaard, Ostgaard, et al., 2002). Therefore, occupational therapy services may be most appropriate for those at risk of chronicity or for those with established ongoing symptoms.
LBP and PGP are frequent causes of sick leave from work among pregnant people (Backhausen et al., 2018; Dørheim et al., 2013; Malmqvist et al., 2015). None of the included studies focused exclusively on vocational experiences however nine studies discussed workplace difficulties or sick leave from work. Occupational therapists have a well-established role in vocational rehabilitation for people with chronic pain (Lagueux et al., 2018). Several evidence-based interventions to support people with LBP continue to work have developed and evaluated such as liaison with employers, work modifications, early return to work, and multidisciplinary interventions (Wegrzynek et al., 2020). In further developing the occupational therapy role with pregnant people vocational interventions are a potential area of focus. Given the societal and personal burden of sick leave associated with pregnancy-related lumbopelvic pain development of effective vocational interventions should be prioritized.
Unlike studies with other populations with musculoskeletal pain our synthesis identified specific concerns related to becoming a parent or parenting a newborn with PGP/LBP including concerns about taking medications that affect the health of their babies. Medication hesitancy among pregnant people is common (Twigg et al., 2016) and has also been reported by others with chronic diseases such as rheumatoid arthritis in pregnancy (Krause & Makol, 2016). A recent review identified that pharmacological management of pain in pregnancy should be tailored to the lowest therapeutic dose and shortest possible duration as certain analgesics may increase the risk for adverse fetal and pregnancy outcomes however inadequately managed pain can result in adverse outcomes for the pregnant person such as such as depression (Black et al., 2019). The hesitancy of pregnant people to take medication and the risks associated with pharmacological management of pain in pregnancy and add further impetus to the development and evaluation of conservative interventions such as those delivered by occupational therapists for this population.
In addition to concern about treatment, parents report difficulties performing occupations related to parenting when they experience pain such as playing and caring for infants and this led to unmet expectations about the parental role and identity consequences in addition to the restrictions and suffering of chronic pain. The postpartum period itself, with the sudden change in daily life, distancing people from their personal interests, and making it difficult to reconcile occupational roles are factors that can produce stress, fatigue, frustrations, and feelings of overload (De Ciências et al., 2018). Evidence from occupational therapy practice with parents with physical disabilities and mental health difficulties could inform occupational therapy practice with this population (Lim et al., 2022; Pastor-Bédard et al., 2022; Wint et al., 2016). Occupational therapy interventions to support parents can benefit the emotional and physical environment for child development (Acharya, 2014), therefore, development of interventions for parents with lumbopelvic pain may also potentially support positive child development outcomes. Evidence suggests children with parent(s) with chronic pain experience adverse outcomes and as such their wellbeing should also be considered. A systematic review of 59 studies found increased pain complaints, greater externalizing and internalizing problems and poorer social competence in offspring of parents with chronic pain (Higgins et al., 2015).
Across the included studies participants reported identity consequences, lack of awareness of their condition, judgments by others and challenges meeting the expectations of others as a partner, a parent, or an employee. Misconceptions about the condition were common with beliefs that pain is inherent to pregnancy or caused by the individual's physical condition. It is well-established that chronic pain makes people vulnerable to stigmatizing reactions from others. Stigma can be experienced as not being believed by others, workplace hostility feeling blamed or dismissed (De Ruddere & Craig, 2016). Stigma about pain, especially chronic pain, may arise in the healthcare encounter because of perceptions that chronic pain has no plausible organic explanation (De Ruddere & Craig, 2016). This discrediting of pain can lead people to hide their pain (Crowe et al., 2017). Stigma has real consequences for wellbeing (Hoyt et al., 2019) and has important implications for healthcare providers working with this population. Today, it is recognized that pain is influenced not just by biological factors and, therefore, its treatment is multimodal. The biopsychosocial model of care is accepted as the best approach (Bevers et al., 2016). The biopsychosocial approach aligns with the humanistic and client-centered philosophy of occupational therapy reflected in its frameworks and models of practice (American Occupational Therapy Association, 2021; Townsend & Polatajko, 2013). Interpersonal elements of the clinician—patient interaction are key to adopting the biopsychosocial model in practice and again this aligns with occupational therapy practice where working consciously with the interpersonal side of the therapeutic relationship to enable optimal outcomes for the service user is prioritized (Solman & Clouston, 2016). In working with this population, as with all people with chronic pain, it is important that occupational therapists believe and respect the individuals’ account of pain and its impact.
Implications for Occupational Therapy Practice
This review has identified the centrality of occupational disruption to the experience of pregnancy-related lumbopelvic pain and has identified that occupational therapy interventions for this population should be developed and evaluated. Occupational therapy interventions could improve functional, work, parenting, and wellbeing outcomes for this population alongside improving child outcomes.
Limitations
The review is limited in terms of the included studies. Most were conducted in high-income countries, and none collected data longitudinally.
Conclusion
A synthesis of qualitative studies found that people with pregnancy-related lumbopelvic pain experience occupational disruption and negative wellbeing impacts, struggle to access adequate treatment and face lack of awareness of their condition. Occupational therapists do not traditionally work with this population. Given the prevalence of pregnancy-related lumbopelvic pain and the occupational consequences of this condition there is a pressing need to robustly evaluate if occupational therapy interventions could improve functional, work, parenting, and wellbeing outcomes for this population.
Key Messages
Pregnant people and people in the postpartum period living with pregnancy-related lumbopelvic pain report little knowledge of the condition before pregnancy and difficulty achieving adequate treatment and pain management.
Pregnancy-related lumbopelvic pain profoundly affects participation in activities of daily living, relationships, identity, and wellbeing.
Occupational therapy interventions for pregnant people and people in the postpartum period living with pregnancy-related lumbopelvic pain should be developed and robustly evaluated.
Footnotes
Funding
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001, Process number 88881.624486 / 2021-01 of the PDSE program - Sep21 / Feb22.