
Abstract
Chronic disease prevention, health, and wellness have become primary practice areas for occupational therapy. Occupational therapists (OTs) in pain rehabilitation are established as essential members of comprehensive and multidisciplinary pain management teams, focusing on increasing occupational performance through participation. This study’s purpose was to investigate OTs’ experiences managing chronic pain and to explore OTs’ effectiveness in supporting clients’ wellness and occupational performance through interventions. Eleven OTs (n = 11) participated with three themes emerging on chronic pain, interventions, and holistic teams. Findings suggest that OTs are successful at treating chronic pain, supporting wellness and occupational performance when their interventions are health-promoting, and clients are enabled to take an active role in their chronic pain management. This study demonstrates the critical impact OTs can have in multidisciplinary teams on clients’ outcomes, such as increased occupational performance, wellness, and quality of life (QOL) through engagement in meaningful occupations.
Introduction
The World Health Organization (WHO) describes chronic pain as a worldwide public health concern (Treede et al., 2015). Treede et al. (2015) described chronic pain as enduring and lasting more than 3 months or requiring longer than average healing time. It is estimated that more than 50 million adults in the United States are affected by chronic pain (Dowell et al., 2016). In addition, adults with chronic pain experience occupational performance limitations that affect their physical and psychological dimensions, impacting self-efficacy, perceived health-related quality of life (QOL), and overall wellness (Lagueux et al., 2018).
Recently, preventing chronic diseases and improving health and wellness became an emergent and primary practice area for Occupational Therapy professionals (Hildenbrand & Lamb, 2013). Hildenbrand & Lamb (2013 stated that Occupational Therapy supports wellness and health-promoting behaviors by engaging individuals in productive and desired occupations. However, there is little evidence about occupational therapists’ (OTs) experiences and beliefs regarding the current interventions for chronic pain management, wellness, and prevention (Brown, 2002).
As explained in the Occupational Therapy Practice Framework: Domain and Process (4th ed.; OTPF-4; American Occupational Therapy Association [AOTA], 2020b), wellness is a series of actions that lead individuals to a more positive way of living. It is heightened level of health, including physical, social, and mental balance (adapted from AOTA, 2020b, p. 66). Wellness is achieved by occupational engagement. As a profession, OTs use this participation in occupations as a driver of health (Hildenbrand & Lamb, 2013). Occupational performance is the ability to participate in desired or necessary occupations (AOTA, 2020b). OTs can promote increased occupational performance, health, and wellness through psychosocial, biological, and social interventions (Biopsychosocial model) training in mind, body, and spirit connection (AOTA, 2020b). The Environment-Health-Occupation-Well-Being (E-HOW) Model is an Occupational Therapy framework for supporting health (Pizzi & Richards, 2017). Proposed by Pizzi in 2017, the E-HOW Model guides OTs to focus on well-being and QOL as primary outcomes of the health care transaction (Pizzi & Richards, 2017).
OTs will likely encounter individuals with chronic pain in various settings (Rochman, 2021). Therefore, understanding OTs’ beliefs and current experiences with managing clients’ chronic pain to promote wellness and occupational performance is essential. This information can influence practice choices and the use of interdisciplinary, occupation-based, client-centered, and evidence-based interventions that affect client outcomes. Therefore, the purpose of this study was to investigate OTs’ beliefs and experiences in managing chronic pain and explore the influence of pain on their perceived effectiveness in supporting their client’s wellness and occupational performance.
Method
Research Design
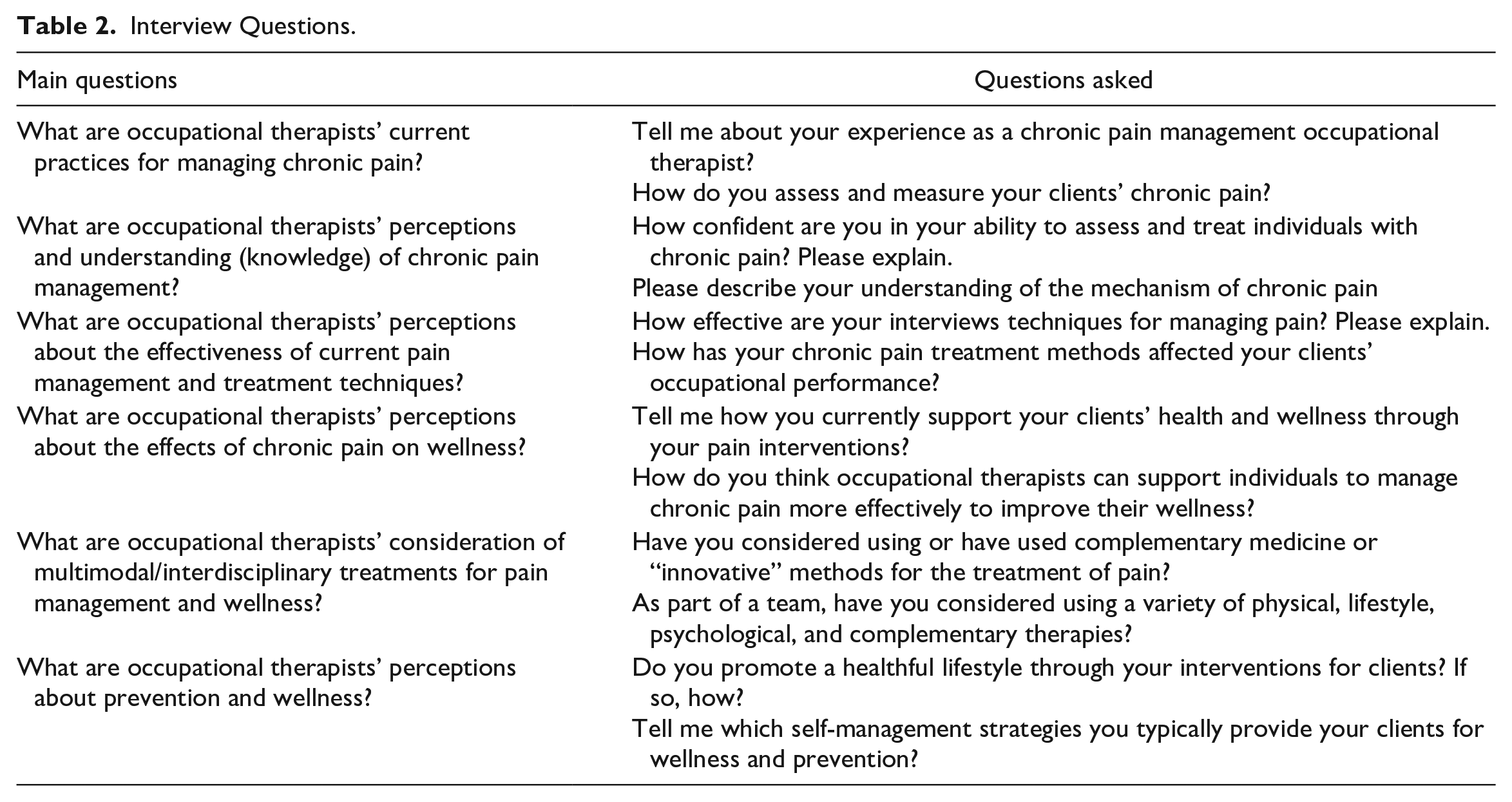
This study used a qualitative descriptive method to understand common experiences therapists have while capturing their voices to illustrate their perceptions of the therapy process (Sandelowski, 2000). Descriptive designs are well matched to represent group perceptions (Patton, 2002). The investigators developed an interview guide to explore current beliefs, experiences, treatment, assessment, and evaluation options used by OTs in the field that support occupational performance and wellness. The guide included questions such as, “tell me how you currently support your clients health and wellness through your pain interventions,” and “How has your chronic pain treatment methods affected your clients’ occupational performance” (see Table 2 for list of questions). The investigators used individual semi-structured in-depth interviews with open-ended questions and analyzed the interview transcripts to access OTs’ beliefs and experiences with managing clients’ chronic pain to promote wellness and occupational performance. The university institutional review board approved the research study. Screening and demographic information were completed digitally through REDCap data collection system hosted at the university (Harris, 2012). Participant consent and interviews were completed online through HIPAA-compliant Zoom.
Participants
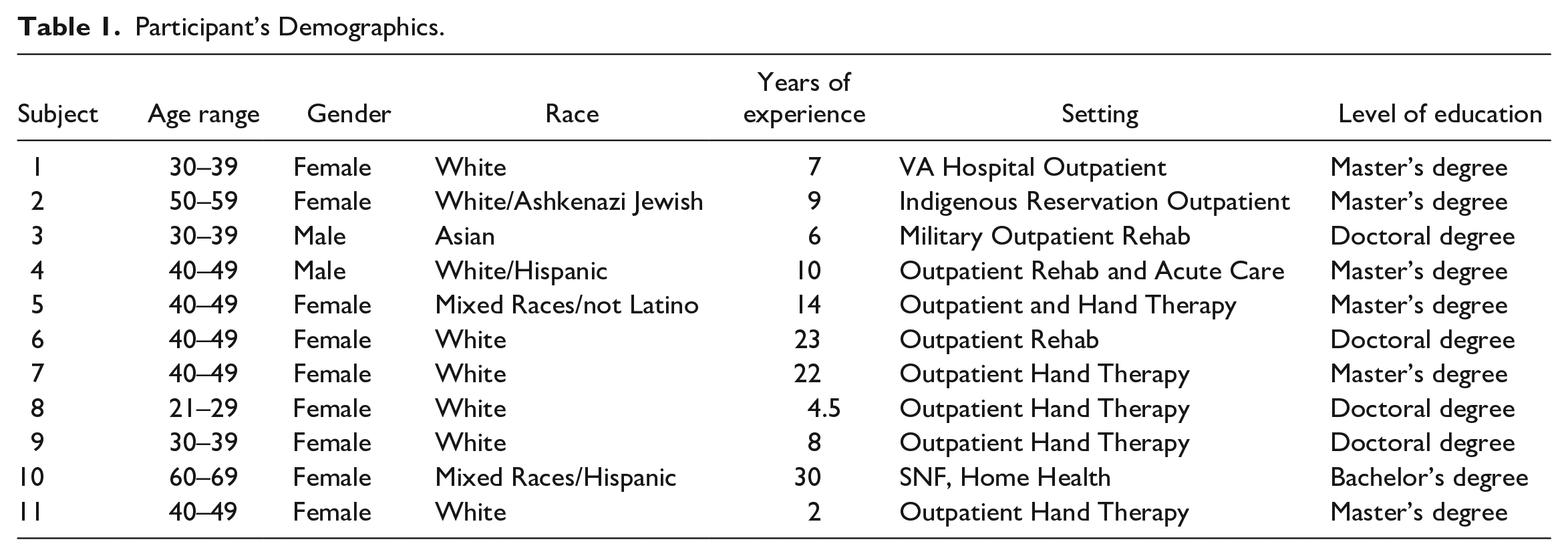
The principal investigator contacted OT references, who provided further contacts or shared study flyers with OTs for recruitment. Snowball sampling was used for further recruitment. A convenience sample was used that included 11 OTs (9 females, 2 males) aged 21 to 69 years old from diverse backgrounds and levels of education who agreed to participate and completed the REDCap demographic information and interviews. Participants were representative of five states (Colorado, Florida, Kentucky, New Mexico, and Texas) and their experience working as an OT ranged from 2 to 30 years, with a mean of 12.5 years. Practice areas included orthopedic and hand therapy, outpatient and inpatient rehabilitation, skilled nursing facility, and home health. Further demographics about participants are shown in Table 1.
Participant’s Demographics.
Data Analysis
Open-ended interview questions were used to collect in-depth responses with clarifying questions asked if needed. These responses were analyzed manually without the use of any qualitative coding software. All the data from the interviews were analyzed using a constant comparison approach, first creating codes, then collapsing them into categories, and then moving to emerging themes, all through an inductive process (Nayar & Stanley, 2014). The investigators reached agreement with the results presented here. The main investigator kept a journal used for continuous reflection and writing of field notes during interviews and debriefing with a peer was conducted weekly for the duration of the study. An audit trail was maintained to report decisions made and also triangulation with the literature was completed throughout the process. Finally, member checking was completed allowing the participants to evaluate whether the study results accurately represented their beliefs and experiences.
Results
The investigators sent flyers to OT references via email. After potential participants saw the flyer, they contacted the primary investigator. If potential participants met the inclusion criteria after an email or phone conversation with the primary investigator, an interview was set up to be conducted via Zoom. Interviews were conducted from June through July 2022. Interviews lasted between 30 and 90 min in length. The primary investigator conducted all interviews and transcribed them verbatim after the conclusion of each interview. Saturation was reached after the sixth interview when the authors noticed similar beliefs and experiences reported by OTs. However, additional interviews were conducted to represent greater geographic areas, practice settings, and OTs’ years of experience. Some of the interview questions are shared in Table 2.
Interview Questions.
A total of three themes emerged from the participants’ responses. The themes included Chronic pain: a stimulating experience for OTs, Pain: Occupational Therapy interventions that address wellness and occupational performance, and Occupational Therapy: holistic pain management teams and complementary medicine.
Chronic Pain: A Stimulating Experience for OTs
The interviewed OTs explained that pain is an unpleasant sensation and a unique experience for each client. They discussed that this sensation or experience occurs in the brain and, if persistent, can change brain structure. This sensation is based on personal experiences that color the perception of how clients see themselves in the world and are influenced by factors such as health, diet, previous experience with pain, previous trauma, cultural and family beliefs, support, and values. As stated by a participant, No pain is the same, no injuries are the same . . . so sometimes when the clinical science doesn’t yield the result maybe there’s something deeper going on and just using your ear (to listen) sometimes can help people a lot. (Participant 8)
OTs explained that they had to look at the impact of trauma on the clients’ experience of chronic pain. The participants shared that they believed most chronic pain clients had experienced trauma, and these traumas could manifest as pain in the human body. Participants shared, I learned in my first experience as a therapist that there’s a huge incidence of sexual and emotional trauma in the chronic pain population. (Participant 6) I think there is deeply ingrained beliefs about pain and I also believe that people have heightened pain levels due to their trauma and psychological and emotional issues so it’s hard. (Participant 2)
In addition, participants defined wellness as an active continuum that encompasses having an optimal balance in several aspects of the individual’s physical, mental, social, and spiritual matters—having a sense of role, identity, and well-being. Participants stated, Wellness is having a healthy, productive and happy life. (Participant 10)
The participants expressed that their experience has also been one of continued learning. Seven out of 11 OTs talked about learning new skills to address chronic pain effectively, therefore increasing their confidence. These skills included learning to communicate complex truths to change clients’ perceptions about pain. They also discussed learning to accept that pain does not always go away and that it is important to teach clients about managing their pain versus the pain resolving. As stated by a participant, Leaning to communicate to people that their pain may or may not go away is a hard lesson to learn . . . that they need to learn to manage their pain versus somebody taking it away for them. (Participant 5)
They described the importance of determining when clients are ready for change and new information so that pain management can be more effective. They talked about learning to use non-traditional interventions and feel comfortable practicing using evidence-based methods, explaining: I think we do great if we approach it correctly and we don’t get stuck in whatever box of the setting (traditional interventions) that we’re working in . . . our behavioral health background is huge in chronic pain and that’s why we can be really awesome in that setting ’cause we understand that background and the impact. (Participant 9)
Participants believed this new learning could be achieved through readings, research, and practice. Most of the OTs reported feeling comfortable treating individuals with chronic pain. However, based on their responses, their confidence in treating pain and wellness increased with years of experience, client population, and seeking and knowing resources to learn about pain. As one subject stated, I’m pretty comfortable, I’ve been doing it longer than I’ve done any other type of OT so I feel each individual is different, sometimes you have great rapport with somebody and other times it’s harder but I feel like I can work with any individual from any background, with any baggage, and teach them maybe more than somebody else or teach them more than they already knew. (Participant 6)
The participants also discussed the marked difference between their confidence and effectiveness. While several talked about being confident, their effectiveness rating varied from low to high. The majority believed that to be effective several factors have to be aligned. For instance, having resources, being part of a multidisciplinary pain management team, and most importantly, they believed their effectiveness was intrinsically tied to the client’s buy-in, resilience, autonomy, and readiness for change. As explained by a participant, So much with chronic pain is getting the person to have autonomy back ’cause they feel like the pain controls them versus them having any control of the pain. (Participant 9) The common denominator is client buy-in, if someone believes they can get better vs someone who unfortunately is stuck and can’t get out of that mentality. (Participant 9)
Although OTs had different personal effectiveness ratings, all reported receiving positive feedback from their clients, especially those clients who have been looking for answers and ways to decrease their pain. As stated by one OT, You have the opportunity to make meaningful change in a population that’s been desperately seeking something, sometimes for months and sometimes for years and years and nobody else gave it to them. (Participant 6)
Pain: Occupational Therapy Interventions That Address Wellness and Occupational Performance
OTs selected client-centered interventions driven by assessment tools that they felt were the most effective in measuring pain to support wellness and occupational performance. Although many interventions were named, all interviewed OTs reported using individualized, holistic, multimodal interventions. Some of the most widely described interventions included education (pain neuroscience), exercise, active modalities, movement, yoga, mindfulness practice, graded motor imagery, breathing and relaxation techniques, and manual therapy. One participant stated, I actually like to do more things like honestly even yoga, visualization. I go much outside of just a typical hand clinic realm with them . . . in a sense I am trying to reframe their identity and the way they experience the world without pain, that tends to be a lot of the treatment. (Participant 9)
Some participants believed manual therapy and modalities were not as effective or essential tools for chronic pain management. As stated by one OT, I find that if it’s modalities or manual therapy that clients can only receive in clinic, they attach that they can only feel better at the clinic or constantly needing that treatment. (Participant 9)
OTs described intervening to increase body awareness and relaxation and decrease kinesiophobia, sympathetic arousal, stress, and anxiety. Some supported using cognitive behavioral therapy and the cognitive orientation to daily occupational performance (CO-OP) (Scammell et al., 2016), while others used movement and active modalities. The intent, participants said, is not for the pain to disappear but to empower the client to learn about the pain, to make changes one small habit at a time, modify their view of pain, take care of themselves, and eventually make lasting changes to their lifestyles. As explained by a participant, It’s about how you use this knowledge to change your performance and your approach going forward, we are trying to create permanent lasting change, so it’s all about what they do after, we want them to be doing some sort of exercise program, but they also need a self-care piece whatever that looks like. (Participant 6)
The participants explained that education is one of the most important approaches for treating chronic pain and supporting wellness. The goal is to encourage self-management and prevention by educating clients. Some education topics included resilience, meditation and relaxation, rest and recovery, healthy habits or routines, sleep hygiene, exercise, and nutrition. Individuals can start by writing their self-management or safety plan throughout their therapeutic process. All information obtained can be built based on their occupations, activities, and desired outcomes so clients can be independent and resilient. One OT said, The only thing that’s lasting is empowering a client to take better care of themselves and giving them the tools that they need to do that. (Participant 6)
The participants shared that to properly assess individuals it was essential to develop a comprehensive occupational profile. The ultimate goal for these OTs was to treat the whole person, empower the client, and help them to internalize and generalize this newly acquired information. As explained by participants, I am a much better therapist when I look at the whole person, I am such a much better therapist even at treating upper extremity conditions when I look at how they’re breathing how their posture is, what position your rib cage is in when you’re doing your upper extremity movements. (Participant 6) Doing it right, where you assess them very well, you have very good rapport, you understand them, they trust you, you attack from all angles, you’re trying you know all things, tapping into their motivation, and all of that including other disciplines in there too. (Participant 3)
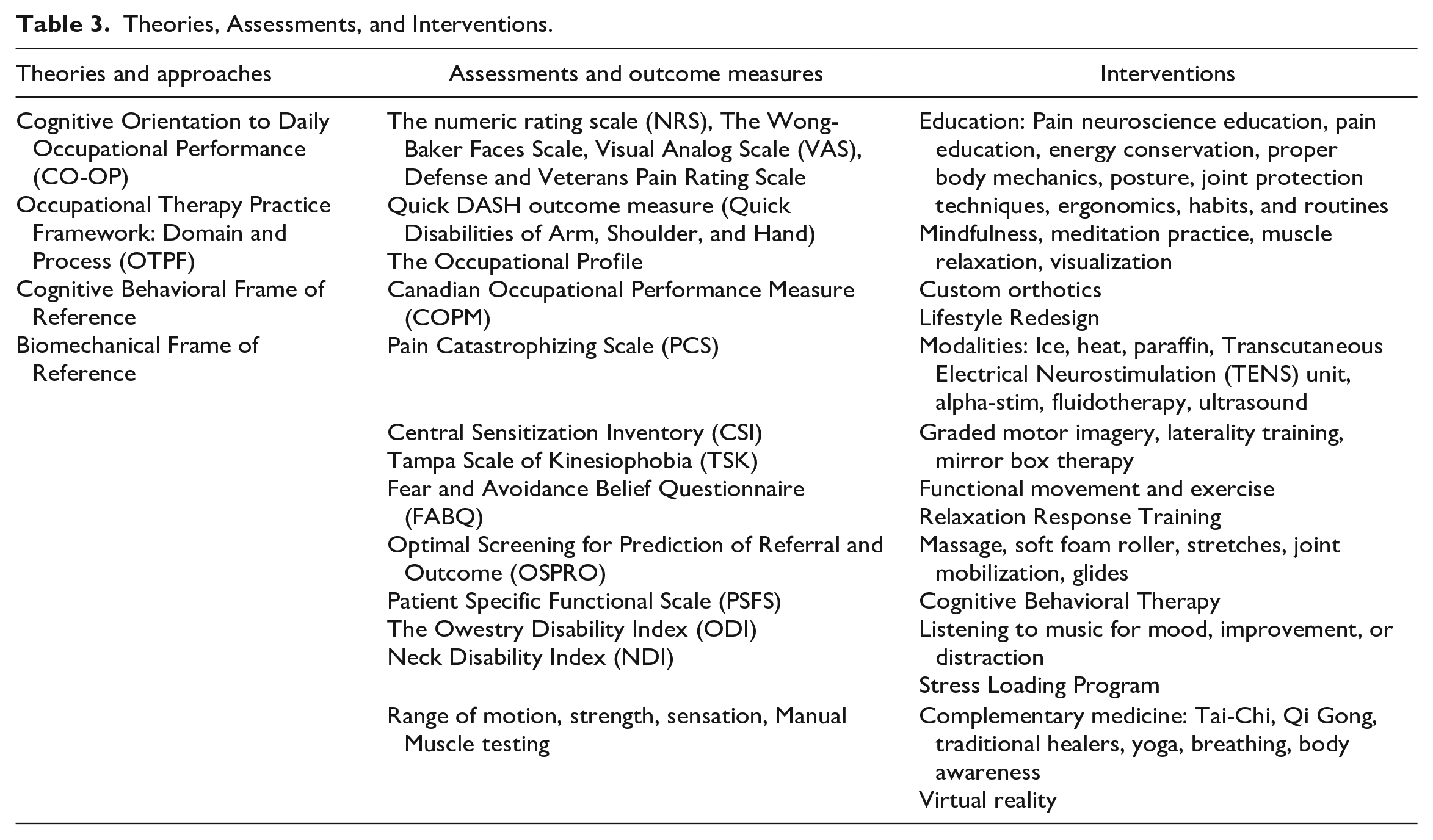
Table 3 illustrates the theories, approaches, assessments, outcome measures, and interventions used by the OTs in this study.
Theories, Assessments, and Interventions.
Occupational Therapy: Holistic Pain Management Teams and Complementary Medicine
Some participants reflected on the effects of the opioid crisis or drug overdose deaths in the United States on treating chronic pain. The OTs shared that the societal and government response to this crisis changed the way pain had to be treated by all medical providers. As the participants explained, the amount and ways narcotics and pain medications were being prescribed versus therapy prescriptions for pain were significantly different from previous years.
As shared by participants, They were doing the draw down on all of the opioids . . . so they were not refilling and not prescribing opioids to veterans with chronic pain. (Participant 1) The addiction levels are so high and thankfully doctors don’t want to choose that (narcotics) first and so they send people to rehab. (Participant 2)
Participants explained that this client’s context change led to the creation of holistic pain management teams. The participants believed they were more successful in treating pain and supporting wellness when working in holistic multidisciplinary teams. Those who believed they had experienced the highest levels of success treating pain had collaborated or directly communicated with other health care professionals or were actively involved in pain management teams. As explained by one subject, You need the multidisciplinary approach to effectively manage all facets that pain impacts and help to treat it from different disciplines . . . I think you’re only as good as the team you’re on. (Participant 7)
OTs reported they had the opportunity to learn about complementary medicine and emergent methods for treating pain sometimes from providers outside of the profession. The OTs in this study who used these methods described the benefits of complementary medicine.
As explained by one participant, There’s evidence to show that Tai chi movements in particular have been proven to reduce a lot of people’s pain and so does meditation . . . and mindfulness-based stress reduction. (Participant 2).
The complementary medicine described by OTs included yoga, acupuncture, battlefield acupuncture, mindfulness, creative arts, Tai-Chi, visualization, progressive muscle relaxation, and alpha-stim electrotherapy. Although most reported not having a way to rate the effectiveness of these treatment methods, most OTs reported support for complementary medicine with one participant stating: I like complementary therapies and support their use, for instance I really like acupuncture but I do not do it myself, I typically make suggestions to clients about other interventions . . . like mindfulness, breathing, Tai-chi, reiki and many others. (Participant 10)
Discussion
In this study, we explored the beliefs and experiences of OTs managing chronic pain to support wellness and occupational performance. The study identified that OTs perceived managing chronic pain as a complex and demanding process. Although most reported it was demanding, they also described their experience as primarily positive and rewarding. OTs reported having difficulty with client’s context and performance patterns (AOTA, 2020b). As explained in the OTPF-4, context and performance patterns can shape the individual’s occupational performance (AOTA, 2020b). For instance, environmental factors, such as the client’s natural and physical environment, can facilitate or hinder an individual’s ability to participate (AOTA, 2020b). The OTs in this study believed pain is inherently tied to the client’s beliefs about pain, accessibility to services, and population culture. In addition, a participant illustrated how an environmental factor (military culture) could prevent individuals from seeking care due to apprehension of being labeled weak. Also, the context includes personal factors. Personal factors refer to the person’s essence or background (i.e., race and cultural identity, attitudes, and life experiences) and not the individual’s health state (AOTA, 2020b). For example, OTs described the importance of knowing that pain is dynamic and different for every client. Then there are performance patterns, including habits, routines, roles, and rituals (AOTA, 2020b). OTs believed that to produce lasting change, the effects of treatment had to go beyond the clinic by empowering clients to shift patterns, habits, and routines to self-regulate and self-manage pain.
Chronic pain is multifaceted and subjectively experienced by clients. Participants explained their role as OTs after the drawdown of prescription pain medication during the opioid crisis. Some participants described being disliked because clients were getting therapy prescriptions versus medication prescriptions from their physicians. This environmental change reflected poorly on the OTs’ perceived effectiveness. Treating pain, as they said, requires client buy-in and empowerment. OTs described themselves as fixers or helpers. They explained that chronic pain is challenging because it is hard to realize that pain may never disappear, and as a fixer, it is difficult to recognize that pain cannot be fixed. Instead, it takes approaching pain from multiple angles and helping clients understand that life adjustments can happen when there is knowledge, acceptance, and willingness for change. AOTA (2021) describes that occupational therapy interventions should focus on self-management to increase participation. Evidence strongly supports self-management and self-advocacy as effective pain management interventions. It is believed that improving self-advocacy can lead to increased confidence to change habits, roles, and routines and therefore increases occupational performance (AOTA, 2021).
OTs explained that besides needing exceptional skills and knowledge about pain, it is essential to consider the client’s factors, such as social and cultural background and life experiences. OTs described the complexity of looking at the whole person, their experiences with pain, cultural beliefs about pain, social attitudes toward pain management, and experience with trauma. For example, trauma may result from historical trauma (i.e., Indigenous population), psychological trauma from abuse, violence, disasters, or wars (veterans and military populations). Most OTs shared that they experienced a high incidence of trauma in clients with chronic pain. These traumas may manifest as pain in the human body. As explained by Lumley et al. (2022), trauma might be the cause of chronic pain, as well as its lingering and intensifying effects. These effects may be due to trauma disrupting the individual’s emotional, cognitive, physical, and cognitive systems (Lumley et al., 2022). These findings validated the importance of how OTs assess, evaluate, and treat chronic pain, the profession’s mental health background, and the inclusion of pain education within academic curriculums.
This study identified that OTs are more effective at addressing chronic pain by treating it as a unique and client-specific sensation, perception, and experience. Chronic pain is best assessed and addressed when looking at the client’s needs, context, and occupations and including health promotion and wellness as the ultimate goals of the interaction between the OT and the client. This study illustrated how chronic pain management is ineffective when OTs conceptualize and treat chronic pain as separate from the client’s context and address it individually from trauma, personal, environmental, social, occupational, and physical dimensions. OTs are effective at treating chronic pain and supporting wellness and occupational performance when their interventions are health-promoting, and clients are encouraged and enabled to take an active role in their chronic pain management. The E-HOW model supports these findings by providing a framework for OTs to provide services that improve occupational participation, QOL, and well-being. OTs can support wellness by facilitating client’s awareness of the need for change, promoting health behaviors, and encouraging occupational participation (Pizzi & Richards, 2017). Also, the biopsychosocial model is considered the most used and effective approach to treating chronic pain (AOTA, 2021). Chronic pain or chronic conditions are best addressed by treating the whole person and recognizing chronic pain’s biological, social, and psychological components. The emphasis, therapists stated, should not be to find a cure but to decrease the impact of the symptoms on occupational performance, health, and wellness (AOTA, 2021). Occupational Therapy approaches and interventions should lead to health promotion outcomes of increased QOL, participation, well-being, occupational performance, and occupational justice (AOTA, 2020a).
OTs in this study shared multiple interventions they believed helped address chronic pain, occupational performance, and overall health and wellness, as well as empowering the client to make health decisions and increase their self-management skills. These holistic and perceived effective interventions included general pain client education, pain neuroscience client education, breathing, mindfulness and meditation, muscle relaxation, yoga and body awareness training, graded motor imagery, posture and body mechanics training, sleep hygiene, and functional movement and exercise. While these interventions were believed to be effective, OTs emphasized that it is just as essential to build trust and rapport with clients to be an effective chronic pain management OT. Manual therapy and modalities were not included on the list above because there was a lack of agreement among the study participants on the use and effectiveness of manual therapy and modalities for managing chronic pain. While some OTs expressed support for manual therapy based on the client population’s needs (i.e., geriatrics), research, and familiar interventions, other therapists disagreed because, they said, it is not an intervention the client can take home. It may increase dependence on clinical treatments and create a revolving door effect. AOTA (2020b) lists physical agent modalities (PAMs) as a pain intervention or preparatory method for engagement in an occupation that should be used with the focus of educating and training the client to promote self-application and self-management (AOTA, 2020b). Hesselstrand et al. (2015) explained that using multiple combined interventions may help clients with chronic pain due to an interactive effect between the strategies. Therefore, OTs need to start by completing a needs assessment through an occupational profile to select appropriate interventions for the specific client (Hesselstrand et al., 2015).
This study identified that OTs believed they address chronic pain and wellness more efficiently as part of holistic multidisciplinary rehabilitation teams or by having direct access to other pain professionals. Participants expressed their support for a comprehensive multidisciplinary pain management program that addresses chronic pain through the biopsychosocial model and focuses on self-management. Participants reflected on the exceptional ability OTs have to address chronic pain. It was further identified that OTs have a distinct ability to guide clients through functional restoration, functional movement, and behavioral health interventions allowing them to experience high levels of success when treating clients with chronic pain. As one participant stated, OTs are poised to bridge and fill the gap between other professions and achieve successful outcomes in pain management teams.
OTs are encouraged to consider complementary and integrative health, such as acupuncture and massage, mind-body behavioral interventions, and meditative movement therapies by U.S. Department of Health and Human Services (HHS, 2019). OTs can either refer out clients or provide complementary medicine interventions themselves as they are able based on their state’s practice acts. The selection of interventions should be based on client needs, clinical expertise, and evidence (HHS, 2019). Figure 1 illustrates the application of the OTPF and E-HOW model and the approaches and interventions used to enhance occupational performance, health, QOL, and wellness.
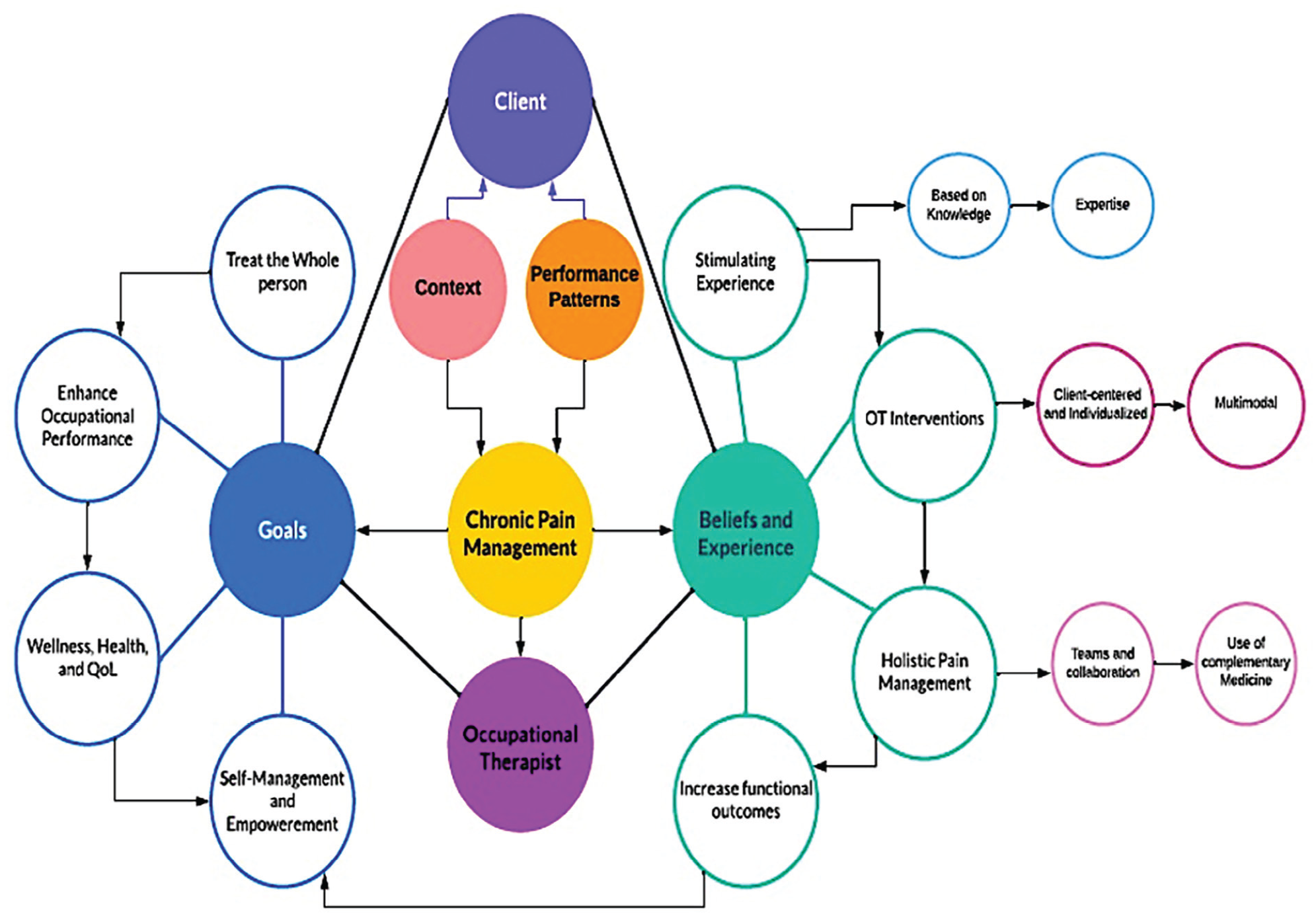
Chronic Pain Management Process.
Implications
This study provides further evidence of the importance of chronic pain, wellness, and prevention awareness and understanding in the field of Occupational Therapy. Chronic pain education and the essential role of Occupational Therapy in pain management teams for the population’s overall health and wellness are accentuated by this study’s findings. The results also highlight the importance of OTs, Occupational therapy assistants, and OT students for the future of the profession as leaders in prevention and wellness. These findings suggest that it is essential to further the knowledge of OTs through pain education courses that focus on wellness and prevention. In addition, the prevalence of chronic pain in all practice settings calls for Occupational Therapy practitioners to be prepared to assess and treat the impact chronic pain has on occupational performance and engagement. Future studies should explore the availability and organizational support for multidisciplinary pain management teams (including occupational therapy assistants), the use of time and resources to support prevention, wellness, and overall health in Occupational Therapy, and funding, insurance, and reimbursement for the practice of prevention and wellness in Occupational Therapy.
Limitations
This study used a snowballing sampling methodology, limiting the findings’ generalizability yet saturation was reached. Also, most participants identified as Caucasian women who were OTs. However, this sample is representative of the United States Occupational Therapy profession demographics, where almost 84% identify as non-Hispanic Caucasian women (Brown et al., 2021).
Conclusion
This study emphasizes Occupational Therapy’s unique and exceptional contribution to chronic pain management. OTs can effectively treat and address chronic pain to support occupational performance, wellness, and life satisfaction through clients’ empowerment for self-management, regulation, and active engagement in desired occupations. OTs believed all interventions were successful at treating chronic pain management. However, they found it was more effective to build trust and rapport, listen and understand, and finally use client-centered and evidence-based interventions. The literature further supports that the profession of Occupational Therapy can address pain and promote health, wellness, and life satisfaction through occupation. OTs are remarkably equipped to assess and treat clients living with chronic pain through education and the use of multiple interventions that address functional outcomes rather than eliminating pain which is a rather ambitious and often elusive goal of clients and OTs.
Footnotes
Acknowledgements
The authors would like to acknowledge and thank the occupational therapists who participated in this study for sharing their beliefs, experiences, and time.
Authors’ Note
The views and information presented are those of the authors and do not represent the official position of the U.S. Army Medical Center of Excellence, the U.S. Army Training and Doctrine Command, or the Departments of the Army, Department Defense, or the U.S. Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics and Patient Consent
This study was approved by University of Kentucky, Office of Research Integrity (Institutional Review Protocol reference number 80071).