
Abstract
Introduction
Chronic pain is defined as intermittent or continuous pain lasting for longer than three months or beyond the expected time for healing (Treede et al., 2019). In Canada, the prevalence of chronic pain for adults older than 18 years of age is at least 18.9%. Half of those living with chronic pain report enduring it for more than 10 years, and one-third rate the pain intensity as severe (Schopflocher et al., 2011). Chronic pain can lead to significant medical, social, and economic losses by impacting people's daily activity participation, productivity, relationships, mental health, quality of life, and overall sense of well-being (D. S. Goldberg & McGee, 2011). Current evidence suggests a high prevalence of chronic pain in veterans; for example, 41%–64% of Canadian veterans experience constant chronic pain, and 23% experience intermitted chronic pain (Reyes Velez et al., 2021; VanDenKerkhof et al., 2015). High rates of musculoskeletal pain are common in veterans as military services require rigorous training and hazardous activities where high risks of injuries are more likely to occur (Gauntlett-Gilbert & Wilson, 2013). In particular, chronic pain is highly associated with arthritis, gastrointestinal issues, back problems, and respiratory issues for the military population (VanDenKerkhof et al., 2015). Chronic pain in veterans is often comorbid with symptoms of anxiety, depression, and post-traumatic stress disorder (PTSD) (El-Gabalawy et al., 2015; Irwin et al., 2014), which might be a trigger for pain and impact one's pain experience.
Chronic pain can persist after injury or be associated with chronic diseases or terminal illnesses (Lynch, 2011). Disability from chronic pain involves the interaction of a person and the physical and social environments. The biopsychosocial nature of chronic pain impacts all levels of a person's participation in occupations and well-being. Studies use various combinations of pain characteristics, mental health status, functioning, activity limitation, and quality of life as indicators to measure the well-being impacts of chronic pain (Reyes Velez et al., 2021). For example, Veterans Affairs Canada reports that 62% of veterans with activity reduction have chronic pain, and 54% have pain interference with work (Veterans Affairs Canada, 2018). Based on a recent systematic review, effective approaches to manage chronic pain in military populations include cognitive-behavioral therapy, positive psychology, yoga, acupuncture, mindfulness-based interventions (MBIs), and biofeedback (Donahue, et al., 2021). As members of a unique profession that adopts a holistic perspective, occupational therapists understand the complexity of chronic pain and enable clients to manage chronic pain by addressing the physical, cognitive, psychological, spiritual, and environmental elements simultaneously. Occupational therapists help people cope and manage their pain using a range of therapeutic tools and strategies (CAOT, 2011). Among these tools, mindfulness meditation is a common intervention that occupational therapists use in pain management.
Mindfulness refers to consciousness or awareness that arises through intentionally attending to the present moment in a nonjudgemental way. Mindfulness meditation is an intervention used in pain management that helps an individual refocus the mind on the present moment while increasing awareness of one's external surroundings, and inner sensations and thoughts, thereby allowing the individual to step back and reframe experiences (Hilton et al., 2017; Kabat-Zinn et al., 1985). A model describing the process of mindfulness for chronic pain illustrates that an individual can accept painful sensations, feelings, and thoughts nonjudgmentally, and focus on the current situation rather than ruminating on past losses or catastrophizing about the future (McCracken & Vowles, 2014). A systematic review found moderate to strong evidence for mindfulness, cognitive and emotional nonreactivity (acceptance), changes in repetitive negative thinking (rumination, worry and concerns), and preliminary evidence for self-compassion and psychological flexibility as underlying mechanisms of MBIs (Gu et al., 2015).
In the past two decades, mindfulness-based interventions (MBIs) have been evaluated and have demonstrated positive outcomes in multiple domains for individuals with chronic pain (Bawa et al., 2015; Creswell, 2017; Hilton et al., 2017; Khoo et al., 2019; Veehof et al., 2016). For example, Mindfulness-Based Stress Reduction (MBSR), developed by Jon Kabat-Zinn, has shown good evidence that it reduces pain symptoms (Creswell, 2017; Kabat-Zinn, 1982). Two randomized control trials showed promising results in reducing self-reported pain and improving functional limitations for young, middle-aged and older adults with chronic pain after receiving the MBSR program (Cherkin et al., 2016; Morone et al., 2016). Particularly for the military and veteran population, various MBIs for living with chronic pain have been adapted and preliminarily tested in the USA (Brintz et al., 2020; Eaton et al., 2020; Kearney et al., 2016; Nassif et al., 2016). Their results were promising; for example, 23%–45% of participants experience clinically meaningful reductions in pain intensity. A recent systematic review reveals that MBIs improve military veterans’ psychological systems, functioning, and quality of life, but rigorous studies are needed to support their efficacy (S. B. Goldberg et al., 2020). Military veterans in the U.S. also reported high levels of nondrug therapy use, including mindfulness or meditation, for pain (Goldsmith et al., 2020).
In occupational therapy, mindfulness approaches were found to contribute to individuals changing their relationship to their body and the pain, and increasing participation in meaningful occupations (Jackson & Bekmuratova, 2020; Takata et al., 2020). Individuals’ depression and psychological distress were decreased while their quality of life and psychological well-being were improved through mindfulness practice (Hawtin & Sullivan, 2011). However, based on a critical appraisal of seven randomized controlled trials (RCTs) and systematic reviews of RCTs, mindfulness was not found to decrease the severity, duration, and long-term chronic nature of pain (Jackson & Bekmuratova, 2020). The level of evidence of MBI for occupational therapy treatment remains limited and more research is warranted to support its efficacy (Hardison & Roll, 2016). With the increasing prevalence of MBIs in all occupational therapy practice areas, it is important to examine the feasibility and effect of MBIs.
This study investigated the effects of the Mindfulness-Based Chronic Pain Management (MBCPMTM) program, developed by Dr. Jackie Gardner-Nix; it was adapted from the traditional MBSR program to accommodate the needs of individuals with chronic pain, using a trauma-informed approach (Gardner-Nix et al., 2008). This 12-week program aimed at easing the suffering of individuals who live with chronic pain by practicing meditation and mindfulness in daily life and exploring topics such as nutrition, exercise, sleep, and medication that can impact chronic pain and well-being. Research has indicated that participants in the MBCPMTM program showed significant improvements in mental health, pain catastrophizing, and levels of suffering (Gardner-Nix et al., 2008, 2014).
Research Purposes and Hypotheses
The purpose of this study was to evaluate the feasibility and preliminary effect of the MBCPMTM program and to understand the lived experience of changes in pain management. We hypothesized that participants who received the MBCPMTM intervention as given by occupational therapists would experience a decrease in pain intensity while reporting improvements in mental health, activity participation, and quality of life. In addition to the quantitative investigation, we also explored participants’ experiences during the intervention to understand how they perceived mindfulness practice as a meaningful occupation that led to changes in occupational performance.
Methods
Study Design
A sequential explanatory mixed-methods design (Ivankova et al., 2006) was used to answer the overarching research question: What are the effects of participation in the MBCPMTM program on perceived pain and life activities? We first collected and analyzed pretest-posttest quantitative data, followed by conducting focus groups and individual phone interviews 2 weeks after the program. The quantitative data and their analysis provide a general understanding of the research question. The qualitative data analysis, by exploring participants’ experiences in-depth, helps us explain the statistical results. Finally, the quantitative and qualitative findings were complementary and informed each other about the feasibility of the MBCPMTM program and participants’ lived experiences of program participation. The study was approved by the University Research Ethics Board (#Pro00090072).
Participants
A convenience sampling method was used to recruit participants. Posters with study information were disseminated to Veteran's Affairs Canada managers and case managers in a Western Canadian city. Potential participants who were interested in participation were referred to the three occupational therapists for MBCPMTM program intervention. Eligibility criteria included the following: (1) veterans; (2) experiencing chronic pain for more than 3 months; (3) over the age of 16 years; (4) able to communicate in English; (5) commitment to attending appointments or therapy; (6) willing to participate in small group activities. We excluded individuals who had active suicidal or homicidal ideation or untreated mental health issues, were severely uncomfortable in a group setting, had moderate to severe cognitive impairment or physical barriers to participation, and those who were unable to commit to regular attendance to a 12-week program held on consecutive weeks.
Data Collection Procedures
From May 2019 to April 2020, three occupational therapists led group sessions for three 12-week MBCPMTM programs, alternating leadership based on their schedules and availability. The three therapists were trained and licensed to facilitate the MBCPMTM program and have experience working with veterans with chronic pain and mental health conditions. The programs were delivered in small groups of 8–10 participants to create a safe and supportive environment.
The participants attended an orientation 2 weeks before the group intervention to learn about the study details and the MBCPMTM intervention, and provided informed consent. In the beginning, the participants received a program package containing “The Mindfulness Solution to Pain” book and its companion audio CDs (Gardner-Nix & Costin-Hall, 2009). The group members met once a week, for 150 min each session, with one scheduled break mid-session. Participants were asked to complete the outcome measures at the beginning of the first group session (pretest) and the end of the last group session (post-test). Two weeks after the last group session, the participants joined a focus group or individual interview to discuss their experience of participation in the program.
Intervention Program
The MBCPMTM involves three modules. Module 1 (sessions 1–4) trains participants in mindfulness and meditation practice, incorporates other contemplative practices, and focuses on mindful living through exercises, homework, and practices outside of formal meditation. Session 5 shows the major effects of stress on the body and mind, highlighting the connection between stress and the body/mind, and forming a bridge to the next module. Module 2 (sessions 6–9) focuses on self-care and compassion, and inspires participants to better care for themselves. Participants learn how they have been viewing the broken parts of the self in a way that can evoke strong emotions. They learn to nurture the self and work with those parts of the self they may have been avoiding or treating without compassion. Module 3 (sessions 10–12) encourages participants to work on behaviors and self-awareness in relationships with others and with one's self. The focus is on understanding how negative interactions can undermine their health. Qualities such as compassion, kindness, gratitude, and appreciation that promote healthy relationships with others and oneself are cultivated. Art or other creative modalities are used to foster increased insight into situations or past experiences which affect the experience of emotion and physical pain as well as healing. This creative exploration can lead to the development of new perspectives, increased understanding and new strategies towards wellness.
Outcome Measures
To understand the characteristics of participants, demographic data were collected, including age, gender, education level, employment status, and pain duration. The primary outcome of interest (the level of catastrophic thinking in relation to pain) and the secondary outcomes (mental health and quality of life) were measured using the following instruments:
The Pain Catastrophizing Scale (PCS) (Sullivan, 1995): The PCS was used to understand participants’ catastrophizing levels when they are in pain. Catastrophizing, defined as “an exaggerated negative mental set brought to bear during the actual or anticipated painful experience,” is the psychological perception of pain and can be inconsistent with one's actual pain intensity (Sullivan et al., 2001). The PCS is a 13-item scale that asks people's perception of pain in three domains: rumination (persisting negative thoughts), magnification (fear-driven pain exacerbations), and helplessness (the sense of no control). Each item is scored on a five-point scale (0–4), with higher scores indicating a greater level of catastrophic thinking (Sullivan et al., 1995). The PCS total score, ranging from 1 to 52, is computed by summing responses to all 13 items. A total PCS score of 30 represents a clinically relevant level of catastrophizing. A numeric pain scale was also included in the outcome measure, asking participants to rate their pain intensity in different situations: right now, at best, at worst, and usually, on a 0 (no pain) to 10 (excruciating pain) scale. In this study, we calculated the total scores of both the PCS and numeric pain scale for data analysis. The PCS has strong evidence of validity and internal consistency when used with the adult community and pain outpatient samples (Osman et al., 2000). The Patient-Reported Outcomes Measurement Information System (PROMIS) (Cella et al., 2010) is a set of tools that assesses people's health and well-being through seven domains: depression, anxiety, physical function, pain interference, fatigue, sleep disturbance, and ability to participate in social roles and activities. In this study, participants’ self-reported mental health and quality of life were evaluated using the PROMIS-29, a generic, health-related quality-of-life survey that measures each of the seven PROMIS domains with four questions, using a 5-point Likert Scale and one 11-point rating scale for pain intensity. The PROMIS-29 scoring guidelines were followed using T-scores, which are standardized with a mean of 50 and standard deviation (SD) of 10, with lower scores indicating better functioning. A change of at least half the standard deviation (5 points) is clinically meaningful (Cella et al., 2010). An effect size in the range of 0.33–0.50 generally corresponds to a clinically important difference in PROM outcomes (Norman et al., 2003; Spiegelhalter et al., 1999). Studies report that PROMIS-29 is useful for various populations and has good psychometric properties—for example, it's highly correlated with numeric ratings of pain and the Medical Outcomes Study Short Form (SF-36) (Katz et al., 2017). At the end of the program (week 12), the participants were asked to complete an end-of-course evaluation form. The evaluation form asked questions about changes in various aspects of life, such as their requirement for medication, sleeping habits, engagements in work, productive activities, socialization, and recreational activities.
Focus Groups/Individual Interviews
The participants were asked to attend a one-hour follow-up focus group to discuss the changing experience perceived during the program. One research assistant, who did not participate in the program, facilitated the focus groups. A semi-structured interview protocol was developed based on the MBCPMTM program components and the research question. The following interview topics were discussed: (1) Overall feelings about the program (e.g., What were the things you did not enjoy that much?); (2) Mind–body connection experience (e.g., What was your experience in connecting your negative thoughts, emotions, or stress to your body or pain?); (3) Pain management before and after the program (e.g., What were the changes in your daily life, such as eating, sleeping, activity patterns, in the past three months?). The research assistant contacted those who could not attend the focus group for individual phone interviews. The interview questions were the same as the focus group questions. The conversations during the focus groups and phone interviews were audio-recorded and transcribed verbatim.
Due to the COVID-19 pandemic, the third group (January 2020–April 2020) was switched from in person to online format in response to the public health restrictions for the last five sessions. The therapists facilitated the group in the same manner, but through remote delivery. The follow-up focus group 2 weeks after the intervention was also conducted online via Zoom. The post-test measures were sent to the participants by email.
Data Analysis
A quantitative analysis was conducted first using the Statistical Package for the Social Science version 26.0. Descriptive statistics such as means and standard deviations were used to characterize the group. Wilcoxon tests were conducted to examine changes in measure scores at preintervention and postintervention. The G*Power© software version 3.1.9.4 was used to calculate the effect sizes (i.e., Cohen's D) and the power of the tests. All tests were set to be two-tailed at p = .05 level.
The qualitative data, including focus group and interview transcriptions, were analyzed using a conventional content analysis method (Hsieh & Shannon, 2005) to help elaborate on the quantitative results. The first step involved two team researchers independently reading through the interviews to get familiar with the data. Next, they read through each interview again, coding the interview to highlight the content that appears important, reoccurring, and/or rare, following the three steps: (1) Initial coding and labeling. Through open coding and incident-by-incident coding, opinions, events, conditions or phenomena were given conceptual labels. By comparing concepts for similarities and differences, the researchers accumulated the basic codes. (2) Categorizing. Conceptually similar codes were grouped together to form categories and subcategories using more abstract headings. The two researchers repeated these steps to keep challenging and comparing codes and categories. Then axial coding was used to relate categories to subcategories and to specify the properties and dimensions of a category. (3) Developing themes. Relevant categories were organized to develop themes. To establish the credibility of the analysis, analyst triangulation was used to illuminate potential bias and blind spots. Both researchers completed the analysis independently, then compared findings to ensure consistency within and consensus about the identified themes.
Findings
Participants Characteristics
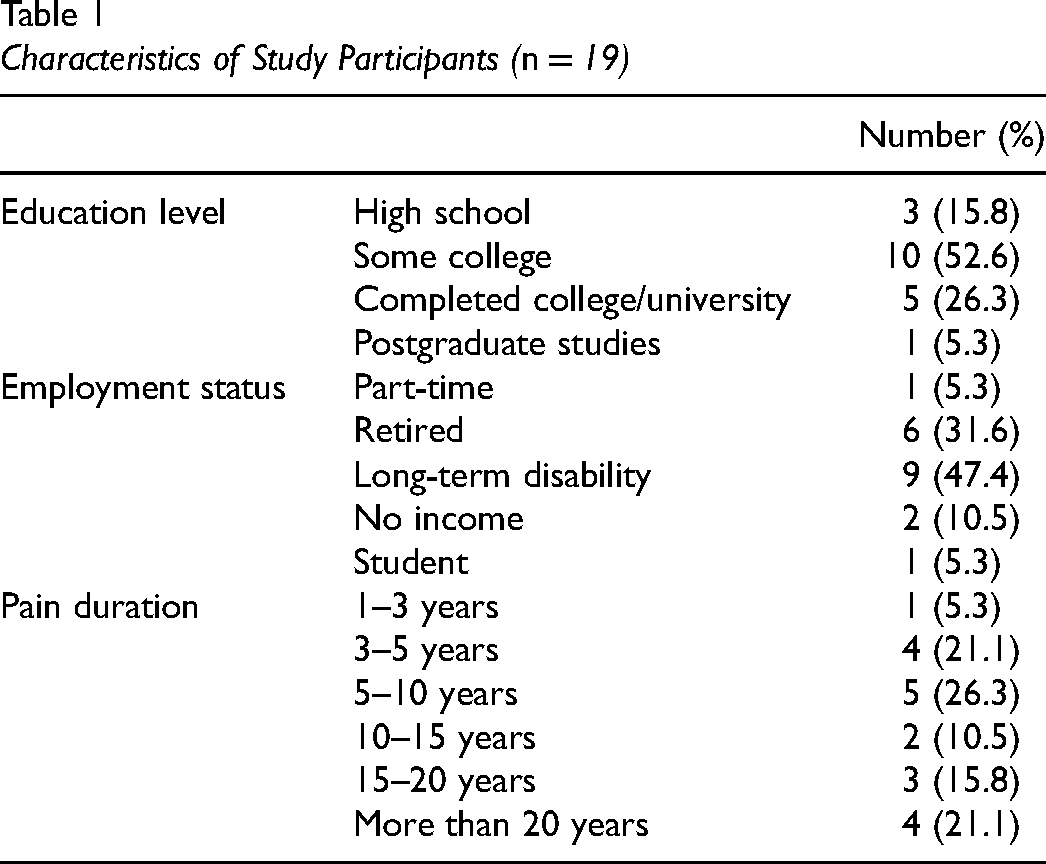
Among the 31 veterans enrolled in the program, 25 completed the 12-week program. Of the 25 participants, 19 completed both premeasure and postmeasure and were included in data analysis. Among the 19 participants, the mean age was 50.7 years (range: 32–68), and the gender was evenly distributed (10 men and 9 women). Almost half of the participants were unemployed due to long-term disability. Their pain duration ranged from 1 to 3 years to more than 20 years.
Table 1 provides detailed information on the characteristics of the 19 participants.
Characteristics of Study Participants (n = 19)
Quantitative Outcomes
Pain Catastrophizing and Pain Level
An improvement was observed for the PCS (see Table 2). The results showed the PCS scores significantly decreased (p = 0.002) from pretest (mean = 32.58) to post-test (mean = 24.32), with an effect size of 0.84 and power of 92%. Considering the cut-off score (30) of the PCS, this finding presented clinically relevant levels of improvement in catastrophizing thinking. However, there were no statistically significant differences for the numeric pain scale reflecting intensity. This result indicated that although participants’ pain intensity did not decrease significantly after the intervention, their psychological perceptions of pain improved.
PCS, Numeric Pain Scale, and PROMIS-29 Scores at Pretest and Post-Test
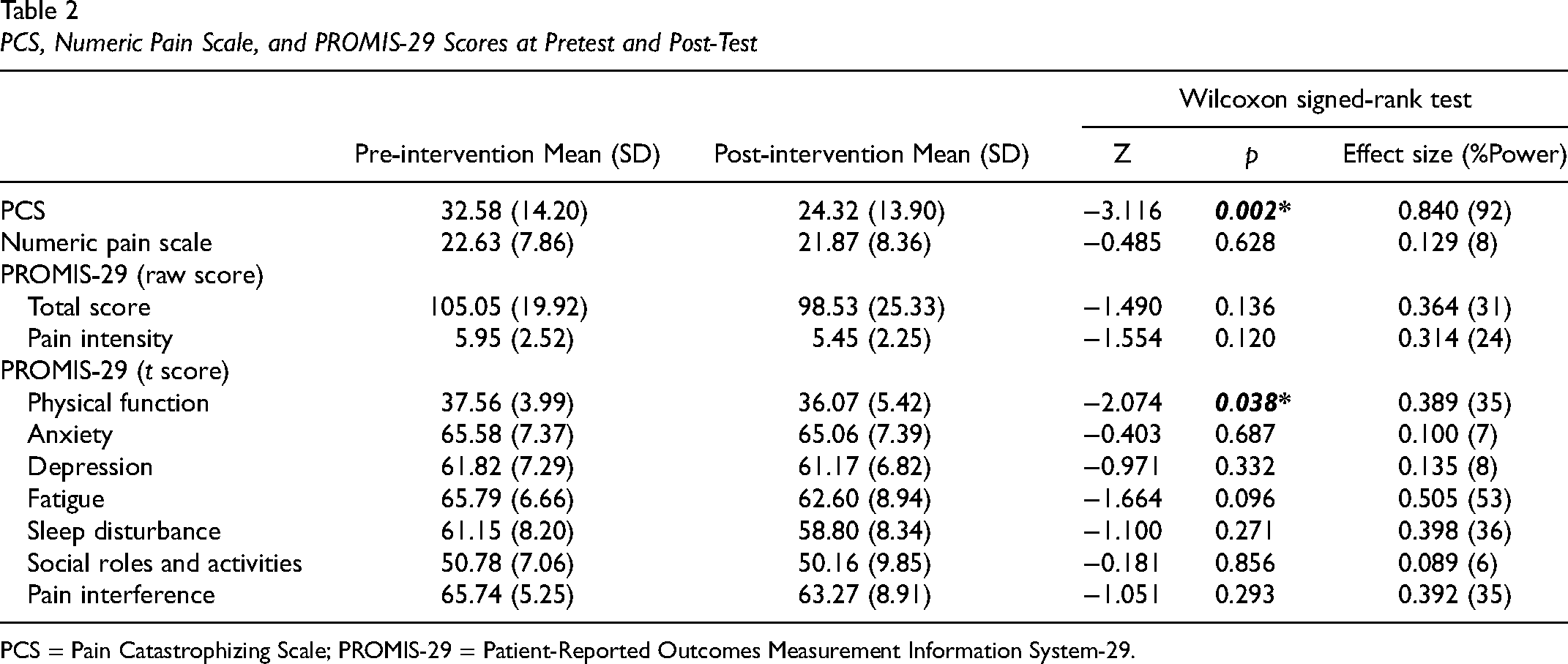
PCS = Pain Catastrophizing Scale; PROMIS-29 = Patient-Reported Outcomes Measurement Information System-29.
Mental Health and Quality of Life
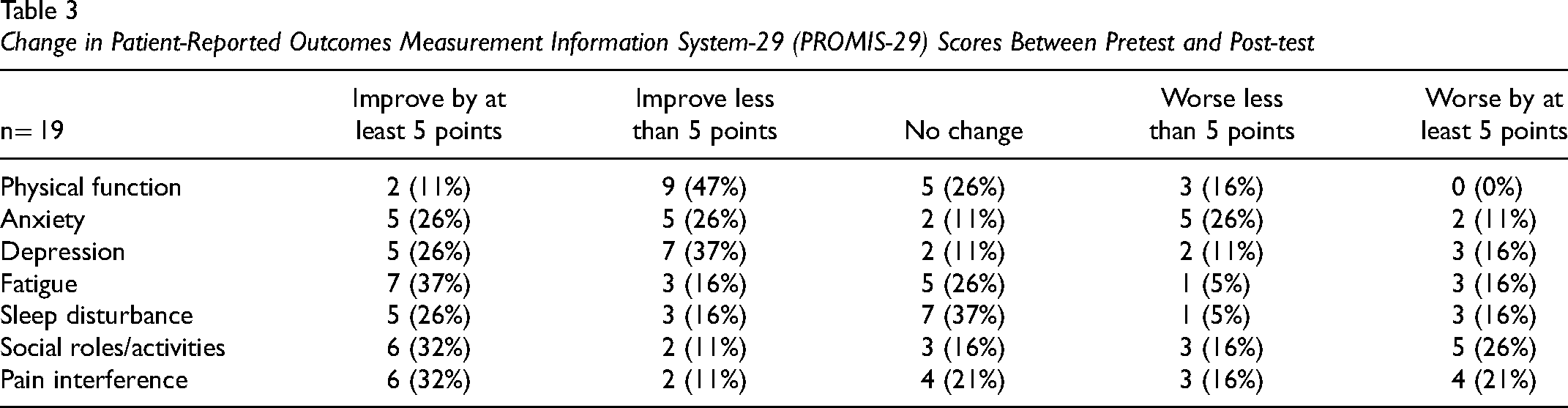
Although the total scores and the sub-scores for each domain of PROMIS-29 decreased, only changes in the physical function domain were statistically significant between pretest and post-test, with an effect size (ES) of 0.389 and power of 35% (see Table 2). Three domains – fatigue (ES = 0.505), sleep disturbance (ES = 0.398), and pain interference (ES = 0.392) – showed clinically meaningful differences between pretest and post-test (with an effect size greater than 0.33). Due to small sample size, we also present the magnitude of change from pretest to post-test in five categories using 0.5 SD (ie, 5 points) as a clinically meaningful difference. Thirty-seven percent of participants had a clinically meaningful change in the fatigue domain; 32% of participants showed a clinically meaningful change in the social role/activities domain and the pain interference domain (see Table 3).
Change in Patient-Reported Outcomes Measurement Information System-29 (PROMIS-29) Scores Between Pretest and Post-test
End-of-Course Evaluation
The results of the end-of-course evaluation form indicate that the participants were generally satisfied with the program. When asked 15 questions related to satisfaction toward the program (e.g., The purpose of each session was communicated clearly; I found these sessions to offer a positive learning experience; The sessions were successful in achieving my objectives; I found the resources and readings helpful; I would recommend this course to others), an average of 4.45 was rated on a 5-point scale. Of the 19 participants who completed the training and both premeasure and postmeasure, 32% of participants reported taking less medication, partly as a result of the program. Forty-five percent (45%) of participants noted the better quality of sleep after the intervention (easier to fall asleep and/or sleep through the night). Seventy-five percent (75%) of participants felt they were more productive in their daily lives. Forty-five percent indicated they had more engagement with family and friends, and 60% showed more engagement in their favorite hobbies.
Qualitative Outcomes
Of the 19 participants who completed the training and both premeasure and postmeasure, 17 participants participated in either an individual interview or a focus group interview. The following themes emerged from the qualitative data analysis: (1) We are not alone! (2) I have a sense of awareness, choices, and control; (3) It does work! (4) Program effects on pain intensity and pain management.
We are not Alone!
Most participants valued the connections, support, and mutual learning within the groups. This further explains the areas of satisfaction participants experienced. The ability to meet and interact with other people who have similar backgrounds and understand “the demons that you face” helped them know that “we are not alone in the struggle” (Participant #16). During the program, they had the opportunity to share with others about their experiences, like Participant #18, who stated, “[You] have a safe place to kind of open up and share what's going on. You don't feel judged”. Participants prized the opportunities to learn from others, as Participant # 1 appreciated “hear[ing] what other people had to say and what they go through and like what they’ve used to cope with the pain and how they work with it.” Participant #19 concluded that “… I gained more confidence I guess just being surrounded by other people that were going through the same thing. I didn’t feel alone anymore”.
I Have a Sense of Awareness, Choices, and Control
The interventions facilitated self-reflection and resulted in raising awareness of the mind–body connection. Participants felt they were able to recognize their emotional and behavioral responses in anxiety-provoking situations, like Participant #6, who shared, “once I had that awareness, it was like an ‘ah-ha’ moment … then I started kind of seeing ‘OK, if I feel anxiety or if I feel stress is my pain worse?’” She further denoted, “I mean, the pain is there regardless, it's just how we manage it and that awareness of it, right? Sometimes it did alleviate and sometimes it didn’t. But that awareness was huge” (Participant #6).
More recognition of “where am I—am I going to be in the combat mode?” gives people a sense of self-control and autonomy, for example, Participant #4 stated: I understand my choices, that I make really do affect the people around me. And so, you know, just having more recognition and being OK with sometimes it's OK to fight back. Sometimes I need to. And sometimes it's—I just need to show more of that compassion and just have that gentle approach.
Participants felt they could better recognize how their emotional and behavioral responses such as anxiety-provoking situations could influence their perception of pain. Participants agreed that being mindful of the self and the body was a good coping strategy to readjust their lives. For instance, Participant #8 mentioned that, in his life, “everything was go, go, go” and then “… all of a sudden everything just stops and your body doesn't know how to slow down”. He was able to utilize the strategies learned from the program and shared that “[I now] don't rush to do anything … take my time … more focused on what I was doing where I am not allowing other thoughts to come in”. Similarly, Participant #12 shared, “I am more relaxed and do things and I am more aware of my body … I am better at fulfilling the needs that my body requires … more settled about this than being angry about it and anxious and stressed”. Participant #3 further concluded the experience of awareness and agency as: I notice that I am able to do more things … they give us tools, like small meditation and small breathing techniques that I can use when I am in a certain place and I start to be in pain, I can use those to help me cope with it.
It Does Work in my Life!
Participants found that being mindful and practicing mindfulness helps them improve various aspects of their daily lives. Participant #3 gave an example: “I know that I get uptight when I’m driving … [my wife] she's going to rub that knee for me and I’m going to relax, and so—yeah, it does work, you know, this mindfulness”. Another participant noted that “[after learning about mindfulness] you feel more rested, you can manage the day, manage the pain, be more mindful, be in the moment and just have more balance” (Participant #18). Some participants reported changes in their mental status and quality of life. Participant #13 stated, “my mental health was all over the place…but with the program, it really helped my mental health … my physical pain and it helped my sleep”. Another participant also mentioned sleeping: “even that 5 min or 10 min of meditation during the day, I am sleeping better at night” (Participant #6).
The three themes aligned with the PCS result that participants’ pain catastrophizing level improved. Their mental set brought to bear during painful experiences changed as we did not hear any rumination and magnification of pain. Instead, participants could share hopeful and optimistic thinking of the pain and practice mindfulness as a meaningful occupation in their daily lives.
Program Effects on Pain Intensity and Pain Management
Participants had mixed responses regarding the perceived level of pain intensity. Some stated that their pain level had decreased, or at least they were “bringing it to a manageable level” after participating in the program. One participant stated: [Before] when my pain became a 9, I would feel that and then take it to a 10. I would be fearful of it and it made it worse … Now, when it is approaching an 8, I just say—I acknowledge it, I am like, there you are. That's OK, and I don't get upset about it as much as I used to … I feel like I have really controlled that threshold where I don't need to get upset about it and I don't need to take it to a 10 … I can actually get it to decrease a little bit instead of increasing. (Participant #17)
Doing group activities such as creating and sharing artwork helped participants divert their attention from pain to here-and-now, resulting in perceived lower pain intensity. Participant #13 described the experience of doing art: “to be so concentrated at doing numbers and just the smell of paint and the numbers and the colors and just doing that, it put your mind into something else.” Another participant shared her experience of connecting herself with her artwork: I drew another one of like a stick person without a head or without a face and then they had a jug of water and then it was like pouring. So it's like water. The coolness helps to relieve the pain in my back. (Participant #19)
In contrast, some participants reported their pain intensity had increased which was attributed to being more aware of it than before, like one who explained: “I am more aware of the intensity now, before it was just—I guess I just masked it or whatever, and I don’t know, maybe it is more heightened now because I am aware of it” (Participant #6). Additionally, there were also some who reported their pain had not changed “as a result of other underlying issues on the side” (Participant #15), i.e., such as PTSD.
The findings explain the quantitative results which indicated psychological perceptions of pain improved, but the pain intensity did not decrease significantly. However, mindfulness allowed participants to utilize internal resources and view and focus the pain in another way. Several participants expressed that being mindful had helped them learn to control their attention, bring themselves to the present moment, and forget about the pain, even if it still existed. One participant shared: That doesn't take away from the fact that the pain is still there, the injury is still there, but it allows me to feel painless and to know that it is not debilitating for me. I won't let it be … naturally find a way to control it, to recognize it, to acknowledge it. (Participant #15)
Participant #13 noted the lingering effects of meditation: “…when we were doing it [meditation] in class, I could see a whole difference for the rest of the day and a couple of days after, I was really calm, and I could really manage my pain after”.
Other Comments on the Intervention
Several participants noted there should be a follow-up in addition to the 12-week program. They were “raw and open” (participant 7) after the 12-week program as they were more aware of their pain and stress. Participant 17 further elaborated: I was more aware of my depression and anxiety for sure, …, it's just a 12-week program, I find that maybe it's not long enough because you’re just peeling off those layers of the onion, the first few layers, and then that's when the shit happens. And then once you realize that—and that's where I am, that awareness of it, now what?
Participants in the third focus group all echoed this suggestion, for example, one participant stated: “we just need more—we need to get deeper and a better understanding of mindfulness and how it works” (Participant 26).
Analysis of Attrition
Among the 31 veterans enrolled in the program, 6 individuals (20%) did not complete the 12-week program, and an additional 6 did not complete the evaluation. The major reasons for attrition, based on follow up phone calls to these individuals, were: deterioration in mental health (n = 4), not meeting personal needs (n = 3), and difficulty with the transition to virtual meetings during the pandemic (n = 3). Those who experienced deterioration in mental health had prior diagnoses of PTSD or other mental illnesses, and reported that they felt anxious and challenged in the group.
Discussion
In this study, the feasibility and preliminary effects of a MBI for chronic pain were investigated. The findings indicated statistically significant improvements in pain catastrophizing and physical health-related quality of life, as well as clinically meaningful changes in fatigue, sleep disturbance, social activities, and pain interference domains of the health-related quality-of-life survey (PROMIS-29). Qualitative data support the quantitative findings showing participants’ strong sense of group therapeutic factors and effects on self-awareness, self-control, pain management, positive thinking of pain, and overall quality of life.
Our results echoed Gardner-Nix and colleagues’ (2008) findings that the intervention decreases scores in the PCS and improves the physical components of the SF-36, a measure of self-reported health status, after 10 weeks of the MBCPM program. Although the mean pain scores and the mental health constructs of PROMIS-29 scores changed in the expected direction, we did not observe statistically significant differences. This result could be linked to the small sample size of this study. In addition, during the COVID-19 pandemic, one group was required to suddenly transition from in person to virtual and several had to drop out due to additional childcare responsibilities, lack of technology, or due to being triggered by the anxiety of the situation. Due to high attrition, although significant improvements from the baseline were observed, we were unable to collect sufficient follow-up data to verify if the effects were maintained after the intervention. Thus, our effect results are preliminary.
These results were consistent with Chiesa and Serretti's (2011) systematic review of MBIs for chronic pain. They found that the evidence of MBI on the improvement of pain perception was significant, while it was not well supported for reducing specific depressive symptoms. In terms of secondary outcomes, they found significant improvement in stress reduction, coping with pain, anxiety levels, and some quality of life domains in the MBI groups. Our qualitative results, which enhanced our understanding of the lived experience of participating in the MBCPMTM program, also indicated similar findings. Our participants appreciated that their mental health and several aspects of their quality of life had improved, although the quantitative measures did not detect significant changes. Participants felt more empowered as they were more aware of their physical and mental status. The findings of the end-of-course evaluation also revealed similar positive results.
Interestingly, the participants reported mixed responses when asked about the change in perceived pain intensity. Being mindful and learning about the mind–body connection led to different results—some participants noted it was helpful for pain management, while others thought being more aware of their pain had increased their perceived pain level. Participants also commented that a 12-week program was too short to fully address the chronic pain and other personal mental health issues such as post-traumatic anxiety, which might be associated with their pain. The intervention did not identify substantial changes in social roles and activity participation in either the quantitative or qualitative data. This could be due to the short duration of the intervention and the lack of long term follow up. As chronic pain is a long-term problem, it may be beneficial to have a longer- period of program and follow up to expose the program's sustained effect. Future studies may consider the program length potentially adapted to veterans. Another consideration is that, given the high attrition in this study, longer programs may not be attractive to potential participants.
In addition to the effects of mindfulness, social support was another major theme that appeared in the focus groups or interviews. Yalom's group therapeutic factors (Kivlighan & Goldfine, 1991) such as interpersonal learning, group cohesiveness, self-understanding, universality, and imparting information were evident during the group interventions. Participants valued the opportunity to meet other people with similar military and chronic pain experiences. They shared common experiences and the understanding of personal struggles. The relationships built in the groups enabled mutual support and learning and facilitated self-reflection and self-discovery. In fact, the second and third groups have reached a certain level of maturity. The group members were able to continue meeting after the MBCPMTM program ended.
In the past decades, MBIs have shown preliminary results on the efficacy of mental and physical disorders, including for patients experiencing chronic pain (Chiesa & Serretti, 2011). The intervention is based on the notion that the cultivation of nonjudgmental awareness, openness, and acceptance of present experiences will allow people to act more reflectively rather than impulsively. Our themes from the qualitative findings reflect well on this effect, as participants highly valued their greater awareness of the mind–body connection. Participants showed greater awareness of the stream of thoughts flowing through the mind. Some participants recognized that self-talk or narratives may elicit automatic emotional or behavioral reactions and that mindfulness can often offer a moment to choose an appropriate response for the situation. This understanding and ability to self-regulate can result in a greater sense of self-control and agency in daily life.
Significant attrition was a major issue in this study. Twenty percent of participants dropped out of the program, and 40% did not complete the evaluation. Goldberg et al. (2020), in their systematic review, found that veterans randomized to MBIs showed higher rates of attrition than those randomized to other control interventions. The acceptability of MBIs among this population seems questionable. However, recent research has emphasized the need for trauma sensitivity in meditation therapy (Lindahl et al., 2017; Treleaven, 2018). Regardless of a trauma-informed approach used by the MBCPMTM program, future research should explore MBIs acceptability among veterans and possible adaptations for this population that are culturally appropriate and trauma-informed.
Limitations
Although this study provides promising results of the MBCPMTM program on chronic pain, such findings must be interpreted with caution because of inherent limitations. First, the absence of a control group and randomization, a small sample size given the difficulty of recruiting participants, and limited research resources are methodological shortcomings of this study. However, establishing baseline data helped us mitigate this limitation. Second, the high attrition rate and low response rate of the follow-up measure resulted in reduced statistical power for testing effect. The small number of participants puts effect size estimates at risk for small sample bias. Third, three mindfulness groups were conducted at different times, at different locations, and group sizes differed. In addition, the third group occurred during the COVID-19 pandemic and the intervention delivery method had to shift to an online format at the halfway point. The impact of these changes was not investigated. However, the MBCPMTM program is standardized and manualized. Thus, the method and procedures followed for each of the three groups were consistent throughout the study.
Implications for Future Study
This study was one of the few studies to investigate the lived experience of participating in a mindfulness-based program. The results demonstrated how a mindfulness program addresses chronic pain by changing individuals’ perception, thoughts, and relationship to the pain. However, it was conducted with relatively small sample size and in a short timeframe. The generalizations of the findings are limited, and significant changes to lifestyle and occupations may not have been detected. Future studies could recruit participants from various backgrounds on a large scale, include control groups to maximize validity, and build evidence on the effects of social roles and activity participation. Also, evidence of the lasting effect of mindfulness-based chronic pain programs is sparse. Although this study planned to include follow-up measures as one of the outcomes, the low response rate did not allow follow-up measures. To reduce potential bias, it is essential that future studies properly account for attrition, particularly given evidence of higher dropout within MBIs among the veteran population.
Conclusion
This study investigated the effects of the MBCPMTM program on veterans managing chronic pain. The findings suggest that MBIs may be a promising treatment option for improving psychological perceptions of pain and physically-related quality of life. This study contributes to the OT literature on the feasibility of implementing MBIs into chronic pain management programs. The high rate of attrition is a significant limitation to address in the future. Exploration of factors associated with attrition can inform the adaptation of MBIs for military veterans living with chronic pain. Future studies should consider the impact of MBIs on social roles and activity participation
Key Messages
The MBCPMTM program offers tools for pain management and is beneficial for individuals living with chronic pain.
MBI helps people change their perceptions about pain.
Group support provides important therapeutic effects in mindfulness-based group intervention.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and or publication of this article: This mindfulness intervention program was funded by the 2018–2019 Veteran and Family Well-being Fund, Veterans Affairs Canada. The research was funded by Occupational Therapy Performance Unit at the University of Alberta, Klassen Rehabilitation Consulting, Mindful Pain Management, and JLSmith Occupational Therapy Services Ltd.
Ethical Approval
The study was approved by the University Research Ethics Board (#Pro00090072).