
Abstract
Background:
Enhancing self-compassion (SC) was found to enhance Quality of Life (QoL). There is a need to comprehend SC manifestations among adults with attention deficit hyperactivity disorder (ADHD) who experience low QoL to provide a foundation for Recovery-based interventions aiming to enhance SC and QoL among adults with ADHD.
Objective:
To explore SC manifestations and their relationships with ADHD symptoms and ADHD related QoL.
Methods:
A cross-sectional survey used self-rated questionnaires for ADHD symptoms, QoL and SC among 32 adults with ADHD, recruited by a volunteer community sampling.
Results:
Moderate overall SC was noted. Negative SC means were found to be higher than the positive SC means. The positive SC subscale common humanity had the lowest mean while the negative SC subscale overidentification had the highest mean. Overall SC level was found to significantly contribute to ADHD symptoms in predicting QoL variance. Overidentification was found to be a significant partial mediator between ADHD symptoms and QoL.
Conclusion:
Recovery-based interventions aiming to decrease the tendency of adults with ADHD to overidentify with their negative thoughts and feelings and to enhance their realization that their difficulties are shared by others, may have the potential to enhance SC and QoL.
Introduction
Attention-deficit hyperactivity disorder (ADHD) is prevalent among 2.5% of the Western world’s adult population (American Psychiatric Association and DSM-5 Task Force, 2013; Fayyad et al., 2017; Mahdi et al., 2017). Involving impaired regulation of higher brain functions, ADHD is associated with significantly low quality of life (QoL). Health-related QoL is reflected in ADHD’s negative impact on social participation, productivity, and psychological health (Brod et al., 2015). Negative occupational features associated with ADHD among adults, as well as negative psychological features, may include low self-efficacy and low self-esteem (Barkley, 2015; Cook et al., 2014). ADHD in adulthood is conceptualized as a chronic neuropsychiatric health condition, and as such, exclusively medical paradigms are not sufficient to improve the QoL of this population (Coghill et al., 2017). Thus, the authors concluded that it is essential to explore factors with the potential to increase QoL among adults with ADHD because decreasing ADHD symptoms alone is not enough to achieve this goal (Brod et al., 2015; Mahdi et al., 2017).The recovery paradigm in mental health explores resources and processes that promote and support positive identity development and engagement in life roles, alongside chronic health conditions that may include the need to cope with and manage active symptoms (Anthony, 1993; Doroud et al., 2015; Leamy et al., 2011). The recovery paradigm could be applicable to conceptualize and examine the challenges which adults with ADHD may experience, as well as available recourses to overcome them (Adamou et al., 2021).
Grounded in Buddhism, self-compassion (SC) concerns ways of self-relating while facing difficulties such as personal failures or inadequacies (Kabat-Zinn, 1994). Neff (2003) defined SC as a multifaceted construct. Each of its opposite poles represents a compassionate (positive) versus uncompassionate (negative) inclination: (1) SC emotional aspect, including the positive pole, mindfulness—balanced awareness toward personal suffering—versus overidentification—unbalanced awareness resulting in negative self-attribution; (2) SC cognitive aspect, including the positive pole, common humanity—a realization that all humans experience difficulties and imperfections—versus isolation, considering self-difficulties and imperfections as mishaps, that are not experienced by others; and (3) SC behavioral aspect, including the positive pole, self-kindness—offering oneself gentle caring—versus self-judgment, being harshly critical toward oneself (Neff, 2003, 2023).
Greater inclination toward positive SC associates with better psychological and physical health (Homan and Sirois, 2017), with resilience, and with QoL (Neff, 2023). On the other hand, greater inclination toward negative SC associates with more stress and psychopathological symptoms, as consistently reported among various clinical samples (Dimitra et al., 2020; MacBeth and Gumley, 2012).
SC predicts QoL in various populations with chronic health and mental health conditions such as depression, anxiety (Sirois et al., 2015), and diabetes (Ferrari et al., 2017), to name a few. Based on the outcomes of SC training interventions, SC is considered a learned skill rather than a fixed trait (Diedrich et al., 2014; Homan and Sirois, 2017).
A recent meta-analysis found that SC interventions significantly increased SC among various nonclinical samples (Golden et al., 2020). Although the impact of SC interventions on reducing active symptoms such as depression, anxiety, and stress had small-to-moderate effect (Han and Kim, 2023), SC training was found to increase SC and QoL among different adult populations with chronic health and mental health conditions (Diedrich et al., 2014; Homan and Sirois, 2017). Several studies indicated that ADHD symptoms are associated with greater tendency to negative SC (Beaton et al., 2020, 2022; Farmer et al., 2022). However, there is a lack of knowledge about SC relationships with aspects of QoL among adults with ADHD.
This study explored SC manifestations among adults with ADHD and their associations with ADHD-related QoL and ADHD symptoms. These finding are a part of a larger study about the relationships between occupational identity, QoL, and recovery processes among adults with ADHD (Paley, 2021). It was hypothesized that positive SC is positively correlated with QoL and negatively correlated with ADHD symptoms. It was also hypothesized that negative SC is negatively correlated with QoL and positively correlated with ADHD symptoms. Finally, total SC, and each of the SC subscales, were hypothesized to separately predict QoL above and beyond ADHD symptoms.
Methods
A quantitative cross-sectional method utilizing structured questionnaires was implemented. A volunteer sampling was utilized to recruit participants via social media networks. The primary inclusion criteria when advertising the research in social groups for adults with ADHD was a diagnosis of ADHD by a licensed neurologist or psychiatrist. Exclusion criteria were (a) self-reported entitlement for a disability pension, indicating considerable incapacity to work because of a medical disability or (b) a self-reported health condition (other than ADHD) that impeded participation in daily life.
The study sample included 32 participants (17 women, 15 men) diagnosed with ADHD by a qualified medical professional. Their mean age was 39 years (standard deviation (SD) = 7.65). Nearly all participants reported having current employment (97%), an academic degree (88%), and a spouse (81%). The participants’ demographic information is listed in Table 1.
Participants’ demographic characteristics (N = 32).
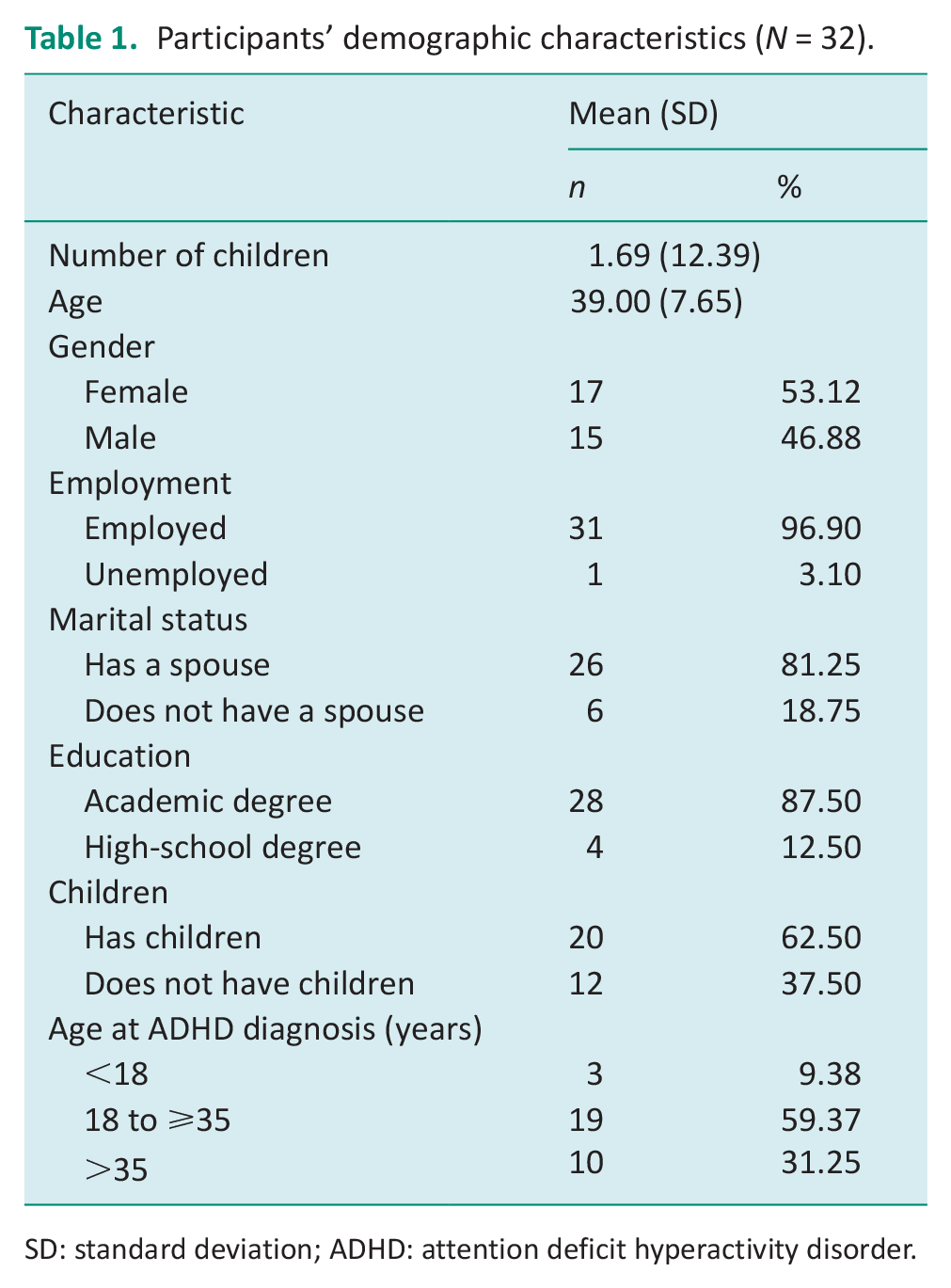
SD: standard deviation; ADHD: attention deficit hyperactivity disorder.
Instruments
Adult ADHD Self-Report Scale symptom checklist version 1.1
The instrument was developed by the World Health Organization (Kessler et al., 2005). The contents presented in the items is congruent with DSM-IV criteria for ADHD (American Psychiatric Association and DSM-5 Task Force, 2013). The first six items serve to screen for ADHD, and the following 12 items serve to assess ADHD symptoms severity. All items are scored on a 5-point Likert scale. With a good test–retest reliability (r = 0.84), and good internal consistency (Cronbach’s α = 0.88) (Adler et al., 2006).
Adult ADHD QoL scale
A self-administered questionnaire, consisting of 29 items, rated on a 5-point scale (Brod et al. 2006). Four subscales indicate ADHD’s impact on life outlook, productivity, psychological health, and relationships. The Adult ADHD QoL (AAQoL) is used in both research and clinical practice (Marfatia et al., 2011). Higher scores indicate better QoL. Good and acceptable internal consistency was found for the AAQoL total and subscales, accordingly (Cronbach’s α = 0.93 total scale; α > 0.70 subscales), and good test–retest reliability (intraclass correlation coefficient alpha = 0.86) was found. The AAQoL has good construct validity for each scale and for differentiating between adults with and without ADHD (Brod et al., 2006; Matza et al., 2007, 2011). It was validated among European samples with ADHD (Brod et al., 2015).
Self-Compassion Scale
The Self-Compassion Scale (SCS) is a self-report questionnaire that addresses self-relating during difficult times (Neff, 2003). After its 26 items are scored (ranging from 1 = never to 5 = always), they are computed into 3 positive (self-kindness, mindfulness, and common humanity) and negative (isolation, overidentification, and self-judgment) subscales. The total mean is computed after each negative item score is reversed (i.e., range from 1 = always, to 5 = never). Higher scores for each subscale’s mean indicate greater positive or negative inclination, and a higher total mean indicates more positive overall SC. According to Neff (n.d.) total SC scores may be roughly classified to three levels, low SC (SC total < 2.5), moderate SC (2.5 < SC total < 3.5), and high SC (3.5 < SC total). Good internal consistency (Cronbach’s α ranged from 0.75 to 0.92) and good test–retest reliability (correlation coefficient of SC total score = 0.93; subscales ranged between 0.80 and 0.88) have been reported (Neff, 2003; Neff et al., 2019).
Procedures
The study received ethical approval from the Hebrew University. A personal meeting was conducted with each of the participants in which the participants completed the questionnaires. Participants signed a consent letter at the beginning of the meeting to participate in the study. Although the questionnaires were self-administered the personal meeting enabled them to ask clarification questions if needed.
Statistical analysis
Descriptive statistics were used to determine normal distributions. Pearson’s correlations were computed to examine the hypotheses regarding the associations between SCS, Adult ADHD Self-Report Scale (ASRS), and AAQoL scores. Seven hierarchical regressions were computed to determine if each of the SCS scores separately predicted AAQoL above and beyond the ASRS (Table 2). During statistical analysis, it was noted that the magnitude of the ASRS regression coefficient association with AAQoL was extremely reduced when overidentification was also in the regression equation. Therefore, the examination of a mediation model was added to determine if overidentification significantly mediated between the independent variable (IV; ASRS) and the dependent variable (DV; AAQoL). According to Baron and Kenny’s (1986) recommendations, and as shown in Figure 1, the unstandardized regression coefficient associations were tested between the IV and the mediator (*a), between the mediator and the DV (when the IV is also present; *b), and between the IV and DV (in the absence of the mediator). Then, Sobel’s statistic was used, with Sobel’s z-value =
Means and SDs for the AAQoL, SC and ASRS scales (N = 32).
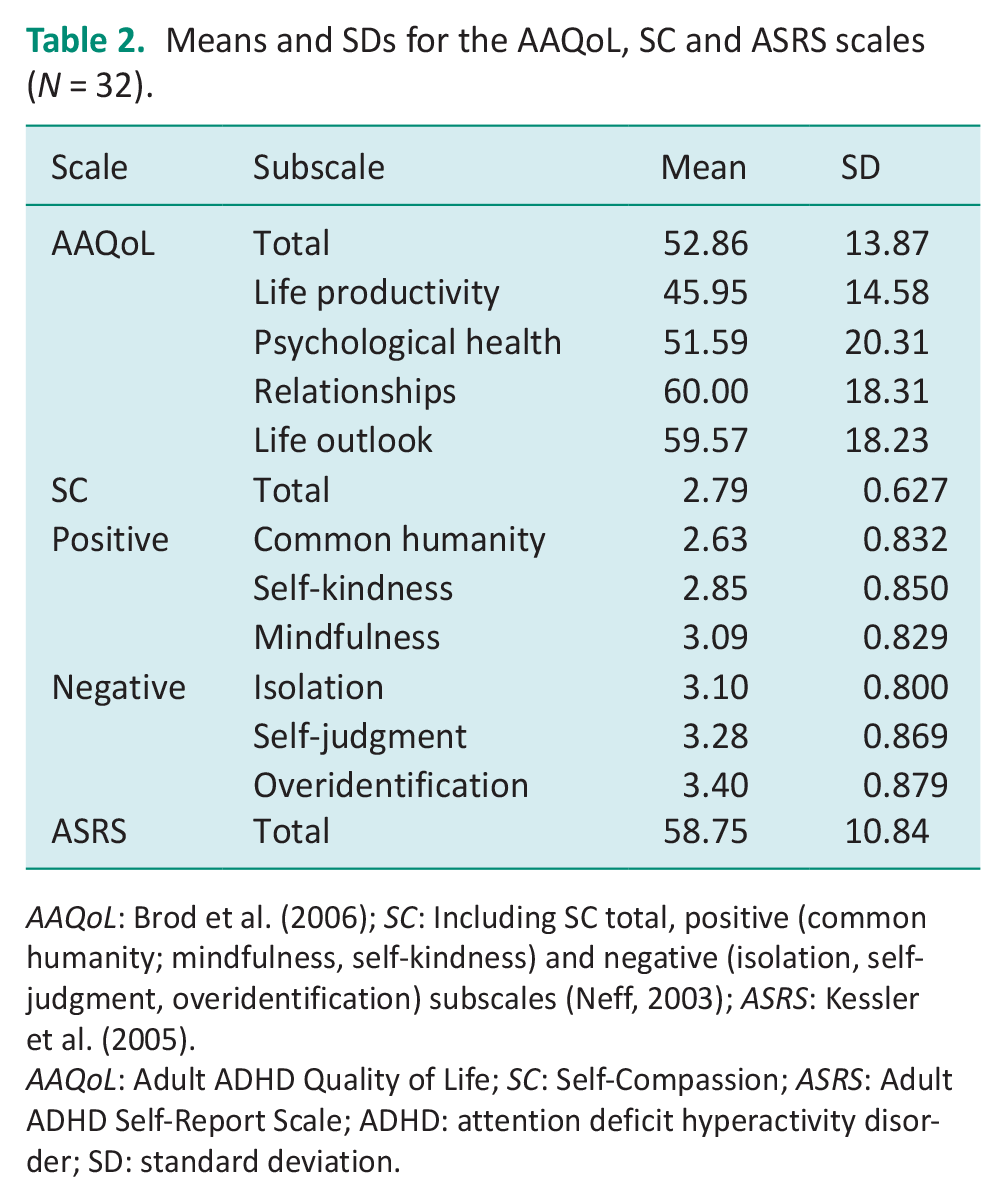
AAQoL: Brod et al. (2006); SC: Including SC total, positive (common humanity; mindfulness, self-kindness) and negative (isolation, self-judgment, overidentification) subscales (Neff, 2003); ASRS: Kessler et al. (2005).
AAQoL: Adult ADHD Quality of Life; SC: Self-Compassion; ASRS: Adult ADHD Self-Report Scale; ADHD: attention deficit hyperactivity disorder; SD: standard deviation.
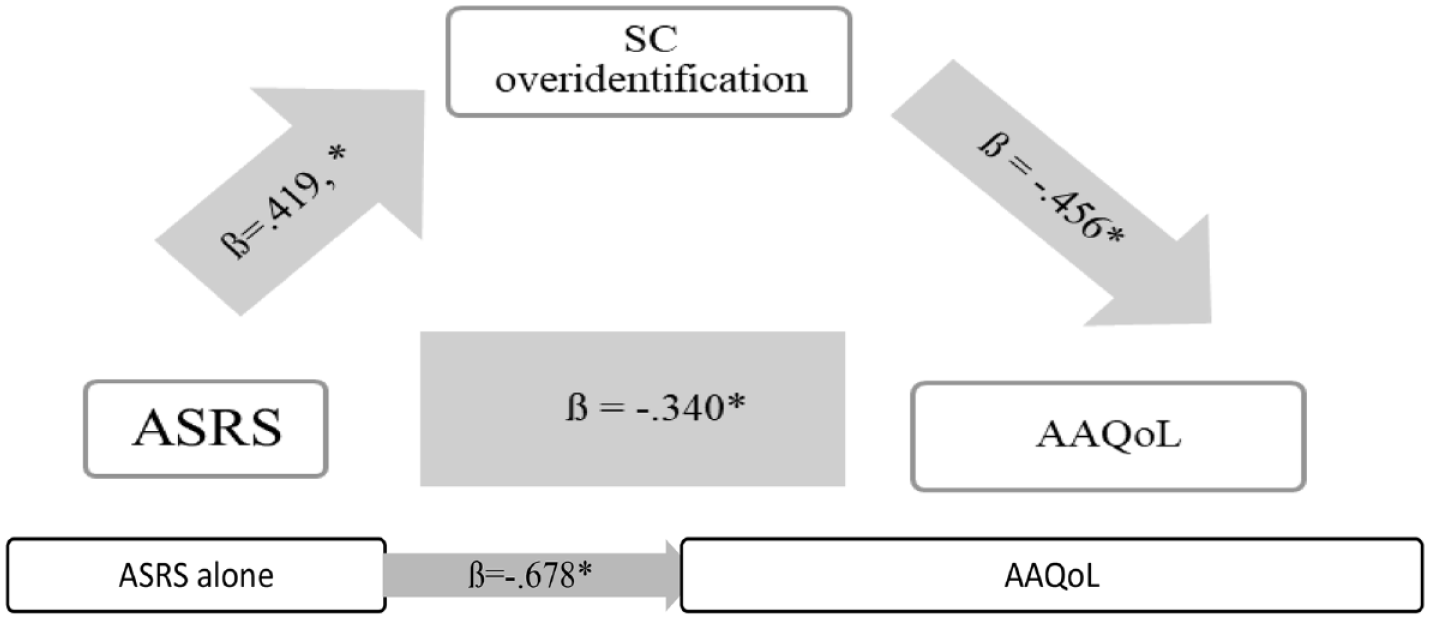
Mediation model between ASRS and AAQoL by SC overidentification.
Results
Descriptive statistics
The ASRS mean score (ADHD symptoms scale) was 58.75 (SD = 10.84, ASRS), above clinical threshold (>51). The AAQoL mean scores (ADHD related QoL scale) was 52.85 (SD = 13.87), with subscales mean scores ranging from 45.9 (SD = 14.58; life productivity) to 60 (SD = 18.31; relationships). The SC total mean was 2.79 (SD = 0.627), with subscales mean ranging from 2.63 (SD = 0.832; common humanity) to 3.40 (SD = 0.800; overidentification).
Correlation between AAQoL, SCS, and ASRS
All the Pearson’s correlation results are listed in Table 3. The AAQoL was found to have a very strong positive correlation with total SC (r = 0.706; SC total, p < 0.01), and strong correlations with the positive SC subscales except mindfulness (r = 0.597; common humanity; r = 0.593; self-kindness, r = −0.599; p < 0.01). The AAQoL had strong negative correlations with the negative SC subscales (r = −0.599; overidentification; r = −0.531, isolation; r = −0.509, self-judgment p < 0.01), and with the ASRS (r = −0.532, p < 0.01). The only SCS found to significantly correlate with ASRS was overidentification, with a medium positive correlation (r = 0.423, p = 0.016; overidentification).
Pearson correlations between AAQoL, ASRS and SCS (N = 32).
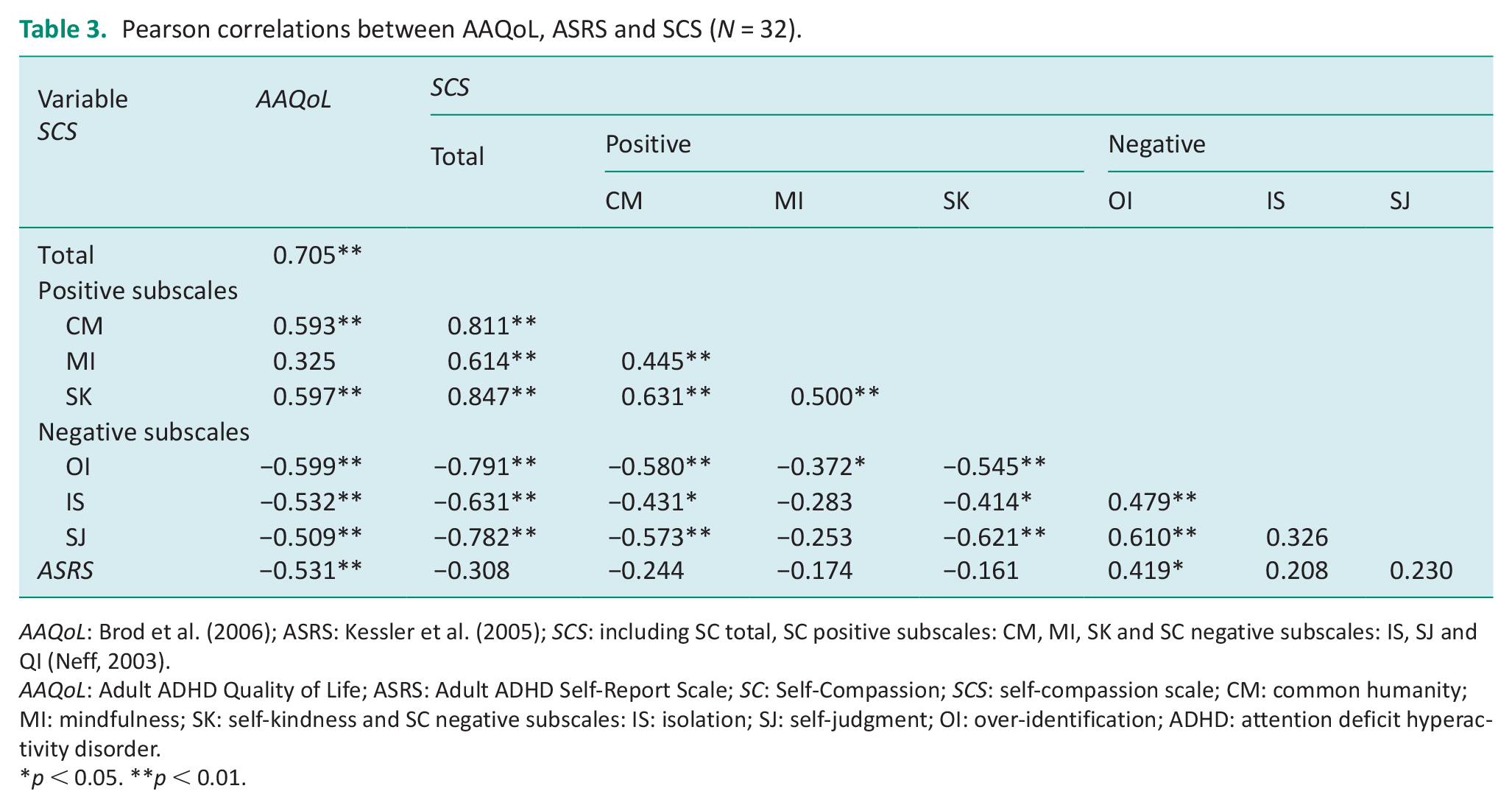
AAQoL: Brod et al. (2006); ASRS: Kessler et al. (2005); SCS: including SC total, SC positive subscales: CM, MI, SK and SC negative subscales: IS, SJ and QI (Neff, 2003).
AAQoL: Adult ADHD Quality of Life; ASRS: Adult ADHD Self-Report Scale; SC: Self-Compassion; SCS: self-compassion scale; CM: common humanity; MI: mindfulness; SK: self-kindness and SC negative subscales: IS: isolation; SJ: self-judgment; OI: over-identification; ADHD: attention deficit hyperactivity disorder.
p < 0.05. **p < 0.01.
Hierarchical regression models for ASRS and SCS scales explaining AAQoL
Seven hierarchical regression models separately performed found total SC and five subscales, significantly explained AAQoL variance above and beyond that accounted for by ASRS. Self-kindness significantly explained AAQoL above and beyond ASRS (F change (1, 29) = 13.549, p = 0.001), with R² change of 0.269. Common humanity significantly explained AAQoL above and beyond ASRS (F change (1, 29) = 13.549, p = 0.001), with R² change of 0.229. Self-judgment significantly explained AAQoL above and beyond ASRS (F change (1, 29) = 8.197, p = 0.008), with R² change of 0.158. Isolation significantly explained AAQoL (p = 0.0001) above and beyond ASRS (F change (1, 29) = 9.739, p = 0.004), with R² change of 0.180. Overidentification significantly explained AAQoL above and beyond ASRS (F change (1, 29) = 10.464, p = 0.003), with R² change of 190.
Total SC significantly explained AAQoL above and beyond the ASRS (F change (1, 29) = 23.768, p-F change = 0.000) with R² change of 0.323.
Together, ASRS and SC total scores significantly explained a large portion of AAQoL variance (F (1, 30) = 22.240, F (1, 30) = 22.211, p = 0.000), with R² of 0.605 (p = 0.002). SC total explained a higher portion of AAQoL (R² change = 0.323; SC total) compared to the ASRS (R² change = 0.282; ASRS).
Mediation analyses
The beta regression coefficient for the association between ASRS and AAQoL (ß = −0.531, p = 0.002) decreased the most when overidentification also predicted AAQoL (ß = −0.340, p = 0.032). Therefore, overidentification was tested for mediating the association between ASRS and AAQoL. Figure 1 includes all the mediation analysis. The Sobel’s z-value was computed and found significant; therefore, overidentification was found to be a significant partial* mediator between the ASRS and AAQoL association.
(*Because the regression coefficient association between ASRS and AAQoL remained significant when overidentification was present (B = −4.33, t = −2.24, p = 0.032), despite its diminished magnitude, compared to the regression coefficient association between ASRS and AAQoL alone (B = −6.78, t = −3.43, p = 0.002)).
Discussion
SC is a recognized internal resource that contributes significantly to QoL (Neff, 2023). The study goals were to explore SC manifestations among adults with ADHD and the relationships between SC and QoL. Participants reported high levels of ADHD symptoms, low levels of ADHD-related QoL, and a strong negative correlation was found between them. Participant’s ADHD symptoms alone predicted less than 30% of their ADHD-related QoL variance. So far, a limited number of studies explored SC among adults with an ADHD diagnosis (Beaton et al., 2020), ADHD traits (Farmer et al., 2022), and dual diagnosis of ADHD and learning disorders (Willoughby and Evans, 2019). Total SC levels in these studies varied from low-to-moderate total SC, with similar results to the findings presented in this study (Beaton et al., 2020; Farmer et al., 2022; Willoughby and Evans, 2019).
The lowest SC score in the finding was for common humanity (a realization that all humans experience difficulties and imperfections). Beaton et al., (2020) suggests that the low level for the positive SC subscale of common humanity is related to perceived criticism from others (Beaton et al., 2020). Studies indicate that adults with ADHD suffer from a strong sense of inadequacy, lack of social understanding, and lack of social acceptance (Brod et al., 2006, 2015; Schott, 2012; Toner et al., 2006). The highest SC mean found was for the overidentification subscale which was also in line with high levels of overidentification among adults with ADHD found in several other SC studies (Beaton et al., 2020; Farmer et al., 2022). Overidentification was found to be a significant partial mediator between ASRS and AAQoL. These findings indicate that adults with ADHD may tend to overidentify with their negative thoughts and feelings. This negative SC tendency was explained by Neff (2003, 2023) as related to dysregulated emotions which could lead to negative self -perceptions (Neff, 2003, 2023). Indeed, emotional regulation difficulties are recognized as a core ADHD-related feature (Beheshti et al., 2020; Biederman et al., 2020). This is also in line with the study findings that indicate a significant positive correlation between ADHD symptoms and the overidentification subscale. Positive correlations were also found in studies between various psychopathological symptoms and the negative SC subscales, but not with the positive SC subscales (Dimitra et al., 2020; Körner et al., 2015; Macbeth and Gumley, 2012; Neff et al., 2017). Farmer et al. (2022) found that ADHD symptoms were significantly correlated with the negative SC subscales but not with the positive ones.
All the SCS except for mindfulness significantly contributed to explaining QoL variance among study participants. The highest SC contribution in explaining QoL was for the total SC mean. These findings are consistent with other SC studies in various clinical and nonclinical samples, reporting the significant overall SC contribution in predicting QoL, well-being, and other health outcomes (Germer and Neff, 2019). Although significant correlations were found between the SCS and aspects of well-being and mental health in a few SC studies among adults with ADHD (Beaton et al., 2020; Farmer et al., 2022) no other study used the ADHD-related QoL measure (Brod et al., 2015) as was used in this study. QoL is an established outcome measure in adults with ADHD studies (Coghill et al., 2017).
Turgay et al. (2012) claim that adults with ADHD are prone to face imbalance between multiple occupational demands and few available resources resulting with negative impact over QoL (Turgay et al., 2012). The findings of the study indicate that SC could be a significant resource for improving QoL among adults with ADHD. These findings illuminate the relevancy of implementing the Recovery perspective in occupational therapy with adults with ADHD (Adamou et al., 2021). One of the major objectives of this approach is to find ways to lead a satisfying life despite the limitations of the disability. Recovery-based interventions, aiming to enhance SC among adults with ADHD have the potential for enhancing ADHD related QoL. One of the ways to achieve this goal could be by strengthening positive patterns of SC among adults with ADHD which could lead to an increase in their QoL.
The operational model of SC, according to Neff (2023), includes overall SC as well as distinctive SC facets, with negative versus positive poles. This model is in contradiction to the claim that all the negative SC facets and all the positive ones represent separate concepts (Neff, 2023). Therefore, strengthening the positive poles of SC could lead to an increase in overall SC. It could enable improving ADHD-related QoL alongside management of active ADHD symptoms.
This study is a preliminary study with a small volunteer sample and consequently with a limited generalizability. Therefore, there is a need for more studies with larger and more diverse samples. The findings of this study are consistent with the conclusions of previous studies conducted among adults with ADHD (Brod et al., 2006, 2015; Mahdi et al., 2017; Newark et al., 2012; Turgay et al., 2012) that there is a need to explore internal and external resources which have potential to increase ADHD-related QoL. They also illuminate the need to develop social environments that would enable adults with ADHD to share their experienced difficulties without facing negative SC which may have an impact on their QoL.
Key findings
SC, ways of self-relating while facing difficulties, contributed to explaining QoL variance among adults with ADHD.
SC could be a significant resource for improving ADHD-related QoL.
What the study has added
Recovery-based interventions aiming to strengthen the positive dimensions of SC and to decrease the negative dimensions of SC could enable to improve ADHD-related QoL.
Footnotes
Acknowledgements
The authors would like to thank all study participants for their time and willingness to share their occupational narratives.
Author’s note
Tamar Paley is now affiliated to School of Occupational Therapy Faculty of Medicine, The Hebrew University, Jerusalem, Israel.
Research ethics
The study received ethical approval from the Hebrew University Institutional Review Board, Number: 122015.
Consent
Written informed consent was obtained from participants.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included in the conduct of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared no financial support for the research, authorship, and/or publication of this article.
Contributorship
All the authors researched literature and conceived the study and were involved in gaining ethical approval. T.P. was involved in participants’ recruitment, she conducted the interviews and gathered the data. All the authors analyzed the data. T.P. wrote the first draft of the manuscript. All the authors contributed to the final version of the manuscript.