
Abstract
Introduction
Advances in neonatal care have increased the survival of infants born with severe medical conditions such as prematurity, genetic syndromes and metabolic disorders necessitating neonatal intensive care (Helenius et al., 2017; Shah et al., 2020). Approximately 14% of all live births in Canada require neonatal intensive care, which represents an annual rate of 60 000 newborns (StatsCan, 2016). Studies reveal that oral feeding is one of the most significant occupational performance areas affected in infants born with severe medical conditions (Johnson et al., 2016; Viswanathan & Jadcherla, 2020). Up to 40% of infants in the neonatal intensive care unit (NICU) may encounter oral feeding difficulties (Johnson et al., 2016; Ross & Browne, 2013).
Occupational therapy practitioners are often involved in the clinical management of infants with oral feeding difficulties while in the NICU. A recent Canadian survey demonstrated that from 1996 to 2019 the role of occupational therapists in the NICU has significantly increased, with oral feeding management as the most common service provided (Borges Nery et al., 2019). Current practices of oral feeding assessment are based on occupational therapists clinical observation of infants’ sucking, swallowing and breathing ability (Hardy et al., 2018). These observations are subjective and provide poor evidence on the underlying suck-swallow-breathe cause of the oral feeding difficulty. Consequently, inappropriate intervention recommendations may be made, inefficiencies in cost-effectiveness arise accompanied by increased distress on families.
Currently, there is a lack of objective method to assess infant's oral feeding skills. The purpose of this study is to develop and test the clinical utility and safety of a nipple monitoring device for the evaluation of oral feeding skills in infants while in the NICU. A nipple monitoring device will provide more accurate identification of infant's suck-swallow-breathe skills and be a significant contribution to occupational therapists’ clinical management of infants with oral feeding difficulties while in the NICU.
Literature Review
Oral feeding process: Oral feeding is a critical occupational performance task for infants in the NICU to achieve because adequate nutritional intake is needed for proper development, parent-infant bonding, and it is a criterion for hospital discharge (Brumbaugh et al., 2018; Fucile et al., 2020a; Goday et al., 2019). Oral feeding in infants is a highly complex multi-system process dependent on the integration of intrinsic factors including the neurological, gastrointestinal, cardio-respiratory and musculoskeletal systems and extrinsic factors including the physical surroundings (e.g., noise level), caregiver competency and stress level to safely generate and coordinate suck, swallow and breathe processes (Lau, 2016; Lau et al., 2012; Mizuno & Ueda, 2003; Viswanathan & Jadcherla, 2020). Nutritive sucking is the rhythmic movement of the tongue and jaw on a bottle/breast to obtain nourishment. During sucking, the bolus of fluid is obtained from the combined components of suction and expression. Suction is the negative intra-oral pressure created by the lowering of the jaw and tongue to draw milk out, and expression is the stripping of the nipple between the tongue and the hard palate. Once the bolus is formed, it is carried to the pharynx by a peristaltic motion of the tongue. As the bolus is collected posteriorly, the swallow is initiated while respiration is interrupted. At this instance, the soft palate rises to close the nasal airway and the epiglottis lowers and closes the laryngeal airway to prevent aspiration (Lau, 2016; Lau et al., 2012; Mizuno & Ueda, 2003; Viswanathan & Jadcherla, 2020). The functioning and coordination of all three suck-swallow-breathe processes are needed for the achievement of safe and successful oral feeding in infants.
Oral feeding difficulties: Oral feeding difficulties in infants are defined as an inability to take an adequate amount of nourishment by mouth to sustain appropriate development (Goday et al., 2019; van den Engel-Hoek, Harding, van Gerven, & Cockerill, 2017). During hospitalization, the most common oral feeding difficulties experienced by infants include difficulty latching on a nipple, disorganized sucking pattern, inefficient sucking, weak suck strength, uncoordinated suck-swallow-breathe which often leads to episodes of apnea, bradycardia, and/or oxygen desaturations, and fatigue while feeding (Crapnell et al., 2013; Lau, 2016; Lau et al., 2012; Park et al., 2015; Pineda et al., 2020). Oral feeding difficulties are often caused by intrinsic factors including disorders of the neurological (E.g., intraventricular hemorrhage), musculoskeletal (E.g., cleft palate), cardiorespiratory (E.g., chronic lung disease), and gastrointestinal systems (E.g.., gastroesophageal reflux) (Burklow et al., 2002; Crapnell et al., 2013; Dodrill et al., 2008; Fucile et al., 2021; Jadcherla et al., 2010; Kashou et al., 2017; Park et al., 2015). Oral feeding difficulties can also arise due to extrinsic factors which are part of their physical surrounding that influence their behavioral responses to the oral feeding experience. For instance, they are physically separated from their mothers, they have multiple caregivers, and they are exposed to bright lights and loud noises from medical equipment. These factors have been identified as potential contributors to the disorganization, distress and irritability that infants often manifest during oral feeding (Fucile S et al., 2020; Pickler et al., 2013; Pickler et al., 2015b).
Impact of oral feeding disorders on family wellbeing: Substantial evidence demonstrates that oral feeding disorders in infants while in the NICU have a negative effect on parent-infant bonding, increase parental stress, impede the transition from full tube to full oral feeds, and prolong hospitalization because attainment of full oral feeds is a criteria for hospital discharge (Aagaard et al., 2015; Chung et al., 2014; Pickler et al., 2015a; Schanler et al., 1999; Silberstein et al., 2009). Oral feeding disorders can persist and lead to long-term feeding problems beyond the NICU stay. The most common long-term feeding problems include oral-motor difficulties in ability to chew and bite, increased likelihood of vomiting and gagging when transitioning to solid food, picky eating, and delayed self-feeding skills (Gire et al., 2019; Goldstein & Malcolm, 2019; Samara et al., 2010; Sanchez et al., 2018; Sanchez et al., 2016). Such long-term feeding problems have negative consequences on children's physical growth, ability to socialize with peers, emotional well-being, cognitive function, and quality of life (Goday et al., 2019; Goldstein & Malcolm, 2019; Kwon et al., 2020; Parker et al., 2016; Robinson et al., 2022). Moreover, many families face high levels of anxiety, stress, and fatigue related to the increased health and financial needs associated with feeding problems during their early year's post-NICU discharge (Aagaard et al., 2015; Amorim et al., 2018; Parker et al., 2016; Silverman et al., 2021).
Current clinical practice management: For health providers and parents the primary goal is achievement of safe oral feeding in infants prior to hospital discharge (Fucile et al., 2020b; Jadcherla et al., 2017; Jadcherla et al., 2010; Viswanathan & Jadcherla, 2020). Infants who present with oral feeding difficulties during the NICU stay are often referred to occupational therapy services (Borges Nery et al., 2019; Hardy et al., 2018). The occupational therapist performs an evaluation which is either a standardized feeding assessment or an informal assessment. Both are observationally based and typically involve assessing infants’ oral-motor structures i.e., lips, jaw, cheeks, tongue, palate, and evaluating their sucking skill, behavioral state, and physiologic response while feeding. The occupational therapist uses gloved fingers to assess the oral-motor structures and suck. The suck strength, rate, and coordination are estimated via tactile feedback from the finger. Based on the evaluation findings, an intervention plan is derived (Borges Nery et al., 2019; Fucile S et al., 2020; Hardy et al., 2018). However, identification of the suck, swallow or breathe problems as underlying causes of the oral feeding difficulty is influenced by clinical experiences of the therapist (Hardy et al., 2018). Hence, incorrect explanatory factors and inappropriate intervention recommendations may be made, and inefficiencies in cost-effectiveness and increased family distress are all consequences. Objective and measurable parameters are needed to objectively assess oral motor skills, in particular suck-swallow-breathe, in infants with oral feeding difficulties.
Tools for measuring oral feeding skills: A review of the literature revealed several apparatus’ have been developed to quantitatively measure sucking, swallowing and breathing ability in infants. The review has identified several such tools including the infant system (Capilouto et al., 2017), Kron Nutritive Sucking Apparatus (Kron et al., 1963), Medoff-Cooper Apparatus (White-Traut et al., 2013), Mizuno-Ueda Sucking Apparatus (Mizuno & Ueda, 2003), and the Oral-Motor Kinetic Apparatus (Lau et al., 1997). However, they have several clinical limitations. In particular, almost all the tools have been designed for research purposes and thus some are fairly complex to set up (Kron et al., 1963; Lau et al., 1997; White-Traut et al., 2013), most tools necessitate an experienced feeder (Kron et al., 1963; Lau et al., 1997; White-Traut et al., 2013) , the flow of milk is controlled (i.e., milk flows out of the nipple only when the infant has reached a certain suck strength threshold, Kron et al., 1963) , can only monitor bottle feeds (Kron et al., 1963; White-Traut et al., 2013) or use a specialized nipple (Capilouto et al., 2017), and some only sucking is monitored (Capitulo, 2005; Kron et al., 1963; White-Traut et al., 2013). To the authors knowledge, there is limited user-friendly quantitative clinical tool to evaluate suck-swallow-breathe in infants in the NICU.
Rationale
There is an increased awareness among occupational therapists and parents on the impact of oral feeding difficulties in infants and their families’ well-being. The field of Occupational Therapy in the management of oral feeding difficulties in the NICU continues to grow. To date, there is limited quantitative method to evaluate oral feeding difficulties. The
Method
Study Design
A pre-experimental design pilot study was performed. This study design was selected to test the clinical utility and safety of the nipple monitoring device to ensure it did not interfere with infants’ oral feeding performance and cause any adverse events. The study was approved by Queen's University and affiliate hospitals Human Subjects Research Ethics Board.
Participant
A total of 16 infants were recruited for this study from the level II-III NICU at Kingston Health Sciences Centre (KHSC). A research assistant reviewed the medical charts of newly admitted infants for eligibility. All eligible parents were approached by the research assistant who explained the study to the parents and obtained written consent. Parents whose infants met the following inclusion criteria were invited to participate: 1) born at less than or equal to 34 weeks gestational age (GA) as determined by obstetric ultrasonogram and clinical examination; 2) appropriate size for their GA; and 3) receiving only tube feedings (orogastric or nasogastric). As a first step, the nipple monitoring device was tested on clinically stable infants to ensure it does not increase infants stress as denoted by physiological reactions such as episodes of apnea, bradycardia and oxygen desaturations. Infants with the following severe medical complications were excluded: 1) bronchopulmonary dysplasia (BPD); 2) necrotizing enterocolitis (NEC); 3) intraventricular hemorrhage (IVH) grades III and IV; 4) periventricular leukomalacia (PVL); 5) genetic/metabolic syndromes and 6) congenital anomalies (e.g., heart, oral, etc.) because of their tendency to be clinically unstable.
Procedure
After obtaining written consent, the research assistant reviewed participants’ medical chart on a daily basis to monitor their progression with oral feeds. When infants were receiving three or more oral feeds per day, two oral feeding sessions were monitored during their scheduled oral feeding times during the day. One of the oral feeding sessions was monitored with the nipple monitoring device and the other without the device. These oral feeding periods were selected because the two oral feeds can be monitored within a 24-h period to ensure results were not influenced by infant maturation. Parents were invited to feed their infants in their customary manner at the bedside in the NICU. In instances where parents were not available, the bedside nurse participated in the recording. To assess clinical utility and safety of the nipple monitoring device, only bottle feeds were recorded. As a first step towards testing clinical utility and safety of the nipple-monitoring device breast feeds were not recorded because oral feeding performance and adverse events may be influenced by maternal factors such as milk supply or variable speed of milk flow from the breast, and thus we would not be able to differentiate whether it was the nipple-device or maternal factor influencing these outcomes. The research assistant arrived 15 min prior to the scheduled oral feeds, to set-up the nipple monitoring device and to address any parent or nurse questions/concerns prior to the oral feeding session. During the oral feeding recordings, the research assistant recorded oral feeding performance, adverse events, and behavioral state (awake, crying, asleep) and interruptions (burping).
Instrumentation
The nipple monitoring device was designed to evaluate sucking, swallowing, and breathing (Figure 1). This tool allows parents or nurses to feed their infant in their customary manner at the bedside in the NICU. To measure sucking, a polyethylene micro tube (PE-9, Scientific Commodities, Lake Havasu City, AZ) was inserted through to the tip of the nipple. For breastfeeds, it may be taped on the lateral boarder of the areola. The tubing was connected to a pressure transducer (TruWave PX-Series Transducer, Fogg System, Aurora, CO). This allowed recording of suction component (the intra-oral negative pressure generated). For standardization purposes only standard ‘yellow’ nipples were used during the monitored oral feedings (Enfamil Standard flow, Mead Johnson & Company, LLC. Evansville, IN). However, any type of nipple (e.g., slow, medium, fast flow) may be used with this device. To monitor swallow bipolar surface electromyography (EMG) electrodes (Biopac Systems Canada, Inc. Montreal, QC) were placed on the right and left side of the hyoid bone. This allowed recording of infrahyoid muscle activity which are involved in swallowing. To monitor breathing a pressure pad connected to a respiratory transducer (SS67L, Biopac Systems Canada Inc., Montreal, QC) was placed over the thoraco-abdominal junction using a chest strap. This allowed for changes in respiratory effort during inhalation and exhalation. These were recorded as a biphasic wave with a positive pressure change as a marker for inspiration and negative pressure wave as a marker for expiration. All signals were recorded using four channel acquisition hardware system (Biopac MP 36 RWSW) and Acknowledge software (Biopac Systems, Inc., Montreal, QC) linked to a laptop computer. Sucking, swallowing, and breathing activities were monitored directly on the computer screen providing direct feedback to the researcher. After each oral feeding session, data was stored for later analyses.
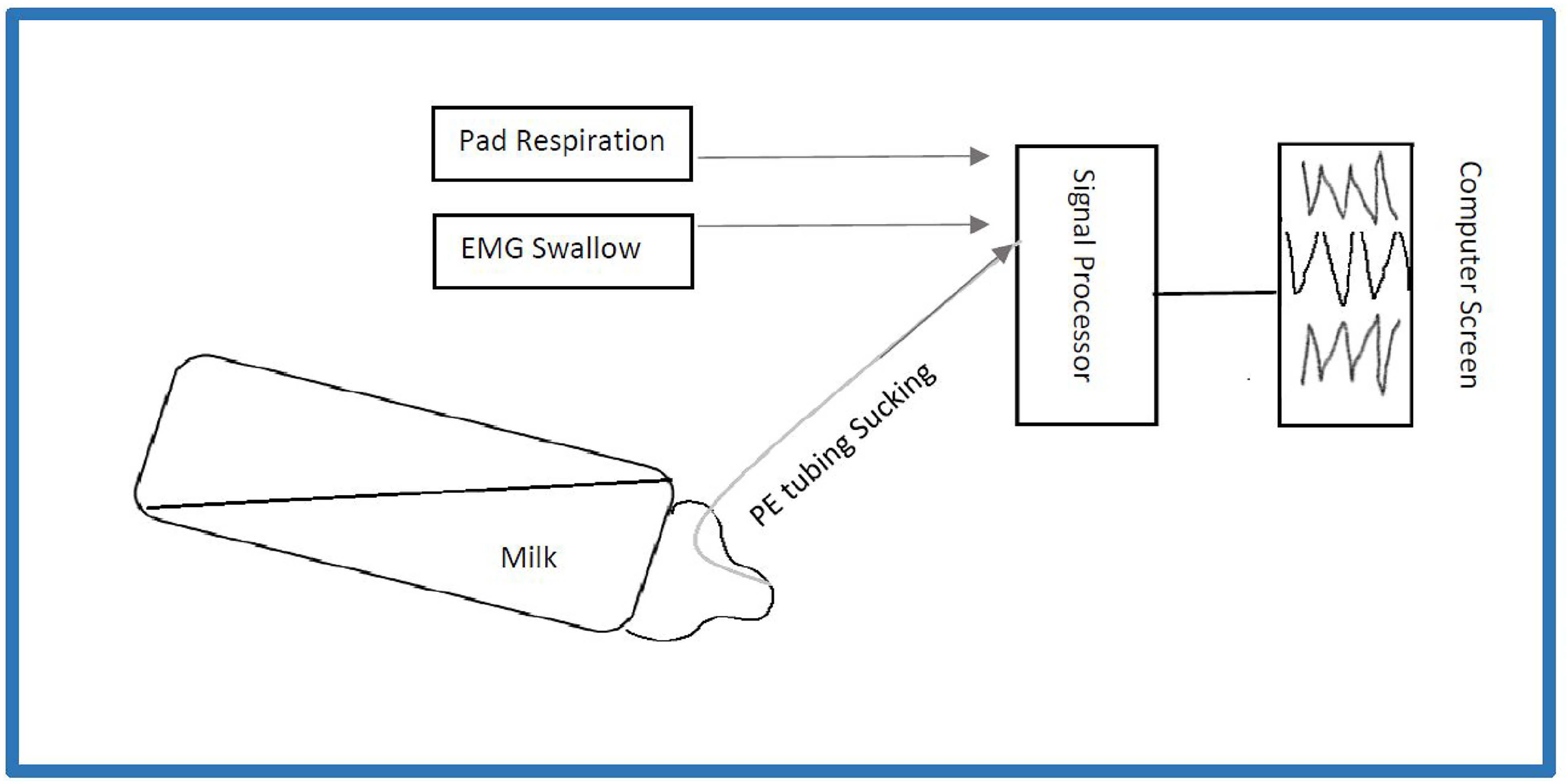
Nipple monitoring device. A schematic of the nipple monitoring device where in polyethylene (PE) tubing is inserted through the nipple to monitor suction component of sucking, electromyography (EMG) electrodes are used to monitor swallow, and a respiratory pad is used to monitor respiratory movement (abdominal inspiration & expiration). All three sensors are connected to a signal processor which is then connected to a laptop computer providing direct feedback to the evaluator.
Data Collection
Participants’ baseline characteristics were monitored including gestational age, birth weight, sex, first born, twin, and medical history (numbers of days receiving tube feedings, number of days to reach full oral feeds, number of days receiving ventilator and continuous positive airway respiratory support). As a first step, it is important to establish clinical utility and safety, and thus only oral feeding outcomes and adverse events were tested. To assess the clinical utility and safety of the nipple monitoring device the following oral feeding performances were monitored during the two oral feeding sessions: Oral feed duration (minutes), intake volume defined as the volume of milk taken over the prescribed volume of milk (percent), and rate of transfer described as volume of milk taken over duration of the oral feed (ml/minutes). Milk, in this study, refers to human milk or formula with no thickener added. Infants received the same type of milk for the two recorded oral feeding sessions thus minimizing the texture of milk influencing results. The occurrence of adverse events during the feeds were also recorded including episodes of apnea, bradycardia, and oxygen desaturations. These outcomes and adverse events were compared between the two sessions to ensure the nipple monitoring device does not interfere with infants’ oral feeding ability and cause physiological adverse episodes. Moreover, these specific oral feeding outcome and adverse events were selected because they can be accurately recorded by the research assistant at the bedside, and are generally and successfully used in previous studies to capture oral motor skills and safety with oral feeds (Lau, 2016; Mizuno & Ueda, 2006; White-Traut et al., 2013). Sucking outcomes for the first five minutes of the oral feed were also collected, including suck strength (average suction amplitude generated), average sucking burst (seconds), suck count (average number of sucks/burst), and suck rate (number of sucks/sucking burst duration). The first five minutes of the oral feed was analyzed because fatigue is minimal, and thus infants’ true potential sucking skills are captured. The research assistant abstracted this information using Acknowledge software. These sucking outcomes were collected to assess the construct soundness of the nipple monitoring device through descriptive appraisal with literature findings.
Data Analysis and Sample Size
Descriptive statistics (means [standard deviations] and frequencies [percentages]) were used to describe participants’ baseline characteristics. A paired sample T-test was used to compare oral feeding outcomes (duration, intake volume, and rate of transfer) between the two recorded sessions. Fisher's Exact test was used to compare the occurrences of adverse events between the two monitored oral feeding sessions. Significance was defined at the 0.05 level. Analyses were performed using the Statistical Program for Social Sciences software version 27.0 (SPSS, Inc., Chicago, IL).
Sample size estimation was derived from comparing paired differences in intake volume between the two monitored oral feeding sessions because it is a criterion to advance oral feeds. The study required a sample size of 16 to achieve a power of 80% and a level of significance of 5% (two sided) for detecting a mean difference of 8 ml between pairs, assuming the standard deviation of the differences to be 10 ml.
Results
A total of sixteen premature infants participated in this study. Six mothers, one father, and nine nurses fed the infant in their customary manner for the recorded sessions. With regards to baseline characteristics (Table 1), participants had a mean birth weight of 2170 ± 574 grams and mean gestational age of 33 ± 2 weeks. Overall, there was an equal distribution of gender, adequate Apgar scores, less than half of participants necessitated respiratory assistance, participants started oral feeds at 34 ± 0.7 weeks and transitioned from full tube to full oral feeds in 11 ± 6 days. Table 2 reveals no statistically significant difference in oral feed duration, intake volume, rate of transfer between the two monitored sessions (with the nipple monitoring device and without the nipple monitoring device). There was no occurrence in adverse events, including episodes of apnea, bradycardia, and oxygen desaturation. Table 3 illustrates the sucking measure outcomes of the participants.
Baseline Characteristics
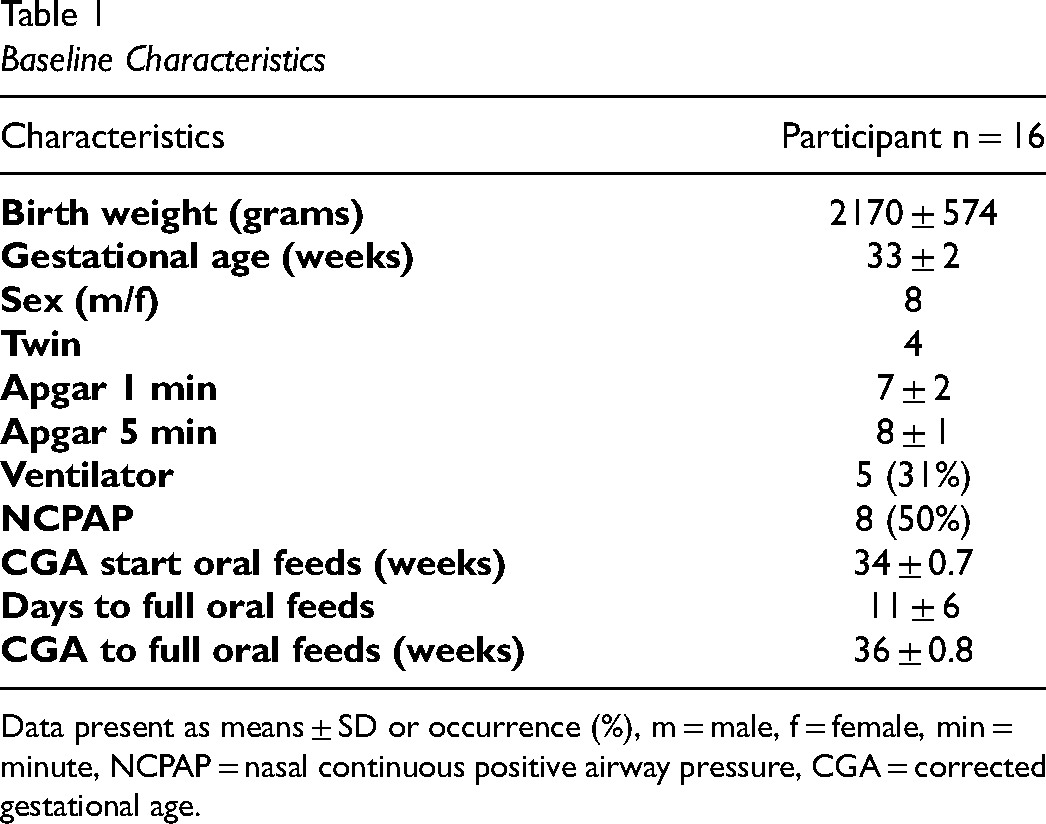
Data present as means ± SD or occurrence (%), m = male, f = female, min = minute, NCPAP = nasal continuous positive airway pressure, CGA = corrected gestational age.
Comparison of Oral Feeding Performances with and Without the Nipple Monitoring Device
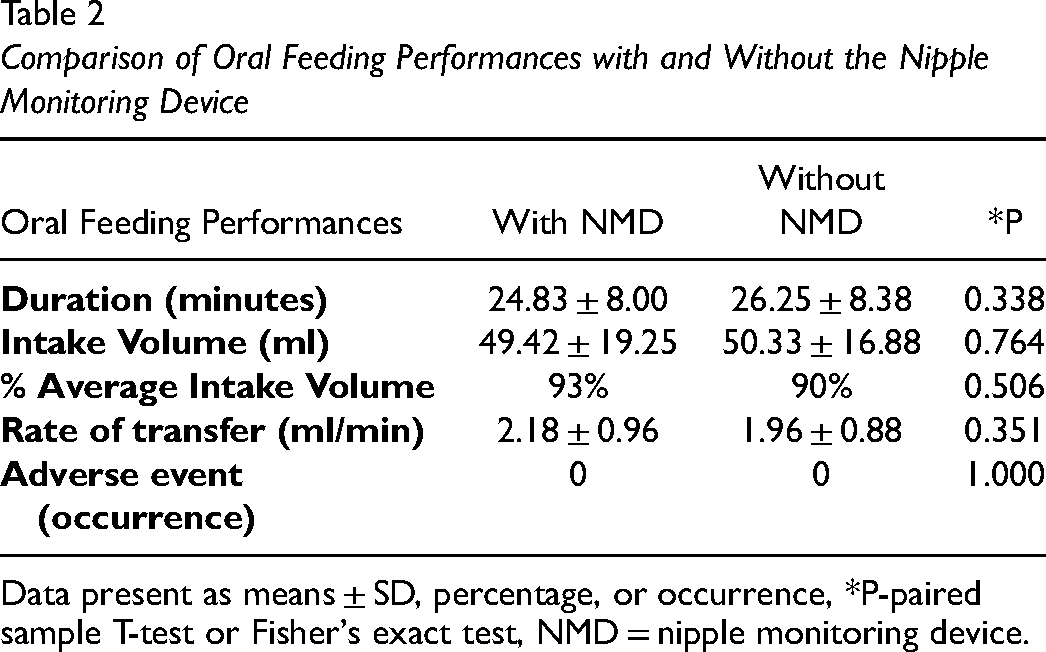
Data present as means ± SD, percentage, or occurrence, *P-paired sample T-test or Fisher's exact test, NMD = nipple monitoring device.
Sucking Outcomes with the Nipple Monitoring Device
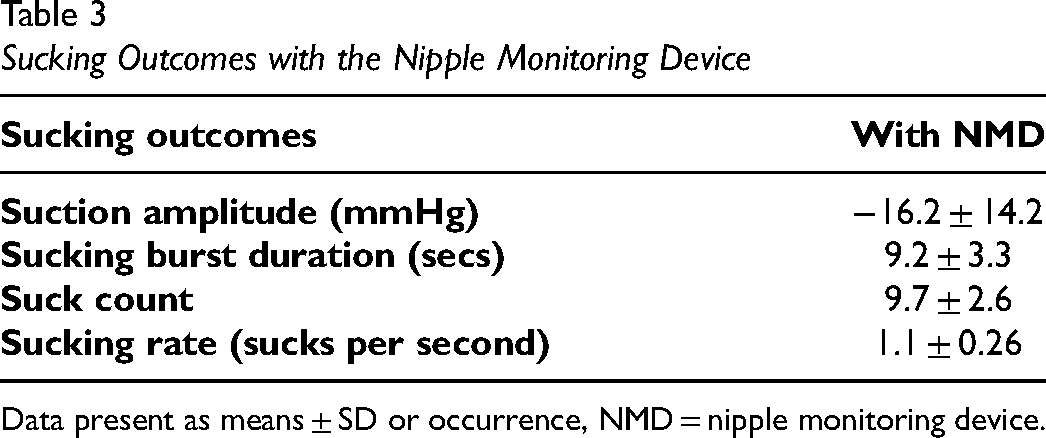
Data present as means ± SD or occurrence, NMD = nipple monitoring device.
Discussion
As the survival of infants with complex health conditions continues to grow, in parallel, the role of Occupational Therapy in the clinical management of oral feeding difficulties will continue to increase (Borges Nery et al., 2019). As the field of Occupational Therapy takes on a more prominent role in feeding infants with complex health conditions, there is an imminent need for a more objective evaluative approach to improve current clinical management of oral feeding in the NICU. This research project developed and tested a nipple monitoring device to evaluate oral feeding skills in infants with complex health conditions. The results from this study suggest that the nipple monitoring tool appears to be a clinically useful and safe tool for occupational therapists’ clinical practice.
Oral feeding in infants involves coordination of suck, swallow and breathe processes (Lau, 2016). Oral feeding difficulties arise when there is a dysfunction in any one of these systems and most often include difficulty latching on a nipple, disorganized sucking pattern, inefficient sucking, weak suck strength, uncoordinated suck-swallow, uncoordinated swallow-breathe in infants (Crapnell et al., 2013; Pineda et al., 2020; Ross & Browne, 2013; Viswanathan & Jadcherla, 2020). These difficulties clinically often present as episodes of apnea, bradycardia, and/or oxygen desaturations, unwillingness to feed, spitting up/turning head away and fatigue while feeding. Customarily these suck-swallow-breathe difficulties are identified via observational methods which limits detection of explanatory factors (Hardy et al., 2018). The nipple monitoring device, presented herein, is able to provide quantitative suck, swallow and breathing measures. Moreover, the study results reveal that the nipple monitoring device components (such as the intra-oral tube, EMG pads, or respiratory pad) do not interfere with infants’ oral feeding ability as denoted by the lack of significant difference in oral feeding performances (duration, intake volume, rate of transfer) between the two oral feeds with and without nipple monitoring device.
Overall safety of the nipple monitoring device was also investigated to ensure it can be used as a clinical tool. For this study we defined safety, based on previous literature as the occurrence of any adverse reactions defined as episodes of apnea, bradycardia, and/or oxygen desaturations while feeding. The study results reveal there was no occurrence in adverse reactions during the monitored oral feeding sessions with the nipple monitoring device. Based on these findings, the nipple monitoring device appears to be a safe bedside clinical tool that may be used to detect aberrations in oral feeding by occupational therapists.
These study results support the construct soundness of the nipple monitoring device. The values we obtained for suction amplitude and suck rate are analogous to those found by Mizuno and Ueda (2006) which used a similar method to monitor sucking, specifically intra-oral pressure generated via a tube inserted in the nipple and flush to the tip (Mizuno & Ueda, 2006). These results are preliminary and the next step towards establishing the clinical utility of the nipple monitoring device necessitates extensive testing of its psychometric (reliability and validity) properties.
Limitations
The study has several limits. The tool was only tested during one oral feed, with infants who were clinically stable, and sample size was small, which limits clinical generalizability. There was no formal methodology to gather parent or provider feedback from the tool. The feeders (parents or nurses) for the two oral feeding sessions differed, which may impact the reliability of the results. However, the nipple monitoring device was designed as a clinical practice tool wherein there is a great amount of variety among the caregivers (parents, guardians or nurses with varied years of experiences) feeding the infants while in the NICU.
Implications for Practice
As the survival of infants with severe medical conditions continues to increase so is the role of occupational therapists in the NICU. Oral feeding is one of the major concerns for parents whose infant is in the NICU and is a necessary milestone for infants to achieve for discharge from the NICU. This study introduces the nipple monitoring device as a unique, safe and family-centered tool for the quantitative assessment and intervention planning of oral feeding for the field of Occupational Therapy.
Future Studies
Future studies to test the nipple monitoring device psychometric properties on a larger and more diverse population and with multiple oral feeding recordings, including breast feeds, is needed to ensure clinical acceptability. Furthermore, occupational therapists and caregiver formal and anonymous method to obtain feedback, such as an online written questionnaire, would provide more in-depth and unbiased insight on overall satisfaction and feasibility with the tool.
Conclusion
Oral feeding is a prominent occupational performance problem for infants with complex health conditions and their families in the NICU. Occupational therapists play a key role in the clinical management of oral feeding. This study has shown that the nipple monitoring device is a unique quantitative method which may be used for objective assessment and intervention planning of infants’ oral motor skills in the NICU for the field of occupational therapy.
Key Messages
• The nipple monitoring tool quantitatively may quantitatively measure infants’ suck, swallow and breathe abilities with no observed adverse events.
• The nipple monitoring tool is a safe bedside tool which may be used by occupational therapists.
• It is a family-centered tool because parents may be directly involved in the oral feeding assessment of their child with the nipple monitoring tool.
Footnotes
Acknowledgments
We thank all families who participated in this study, without whom the study would not be completed. We also thank Jessica Samson for her assistance in the data collection.
Funding
This study was supported by the University Hospitals Kingston Foundation – Innovation Fund.
Authorship Contribution
Dr. Sandra Fucile & Dr. Kimberly Dow both were involved for the inception of the research project, study design development, data collection and analysis, and writing of the manuscript.
Declaration of Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.