
Abstract
Background.
Prioritizing referrals for home care occupational therapy is somewhat subjective, and public and patient perspectives on waiting list priorities are unknown.
Purpose.
To explore the views of home care occupational therapists (OTs), older persons (OPs) and adults with disabilities on waiting list priorities, as well as issues and challenges underlying these priorities.
Method.
We conducted in-depth interviews with 11 OTs, 10 OPs and 9 adults with disabilities. Participants were asked to prioritize referral scenarios while explaining their choices. Directed and conventional content analysis allowed the identification of themes for each group of participants.
Findings.
OTs experienced conflicts of values but mainly prioritized referrals based on client safety. OPs sought to maximize client’s independence, and persons with disabilities aimed to improve clients’ social participation.
Implications.
OTs should seek the perspectives of their target clientele on referral prioritization criteria and strive to adjust prioritization practices accordingly.
Introduction
Home care occupational therapists (OTs) support community-living persons with functional limitations by providing strategies or adaptations to improve their safety and functional abilities (Canadian Home Care Association, 2011; Craig, 2012; Steultjens et al., 2004). However, high demand and limited resources compromise access to these services in some regions of Canada (Canadian Association of Occupational Therapists, 2008b, 2016). Delayed access to occupational therapy can contribute to aggravating clients’ health and function, increasing risk of institutionalization and use of other health care services (Canadian Association of Occupational Therapists, 2008a), reducing the person’s potential to benefit from services when they are eventually received (Hall et al., 2006) and generating anxiety (Ní Shiothcháin & Byrne, 2009). From the therapist’s standpoint, long waiting lists can create ethical tensions (Bushby et al., 2015), increasing the risk of burnout or professional attrition (Pauly et al., 2012).
With the aim of minimizing these negative consequences of waiting, referrals to community occupational therapy are usually prioritized based on client need, using in-house prioritization tools or guidelines (Harding et al., 2010; Harries & Gilhooly, 2011). However, the reliability and validity of such prioritization tools are suboptimal (Harding et al., 2011). One of the shortcomings of referral prioritization tools may lie in the subjectivity and complexity of decisions regarding client priority in the context of limited resources (Carrier et al., 2010). Clinicians’ and managers’ home care resource allocation decisions are influenced by social context factors, such as increasing demand for services, reimbursement policies and cost containment initiatives, performance targets and an orientation towards medical needs (Carrier et al., 2016; Mohammed et al., 2013). In the practice context, professionals’ allocation decisions are influenced by program policies and eligibility criteria, accountability to professional bodies and ethical obligations, the composition of the team, as well as client factors and the professional’s own experiences and beliefs (Fraser et al., 2018; Freeman et al., 2009). However, clinicians are not always conscious of all the reasons that affect their decision about a referral’s priority level (Harries & Gilhooly, 2010).
Adding to the complexity of decision-making when prioritizing referrals, home care OTs try to adopt a client-centered perspective in their practice (Turcotte et al., 2015) but do not know the perspectives of older or disabled community-living persons on waiting list prioritization criteria (Raymond et al., 2013). Patient or public preferences for waiting list priorities have been studied for surgical and medical services (Diederich et al., 2012; Oudhoff et al., 2007), but to our knowledge, this has not been done in the field of rehabilitation. Furthermore, prioritization preference studies typically use quantitative surveys and rarely uncover the reasons for the priorities that are elicited. Incorporating the public and/or patients’ perspectives is becoming increasingly important in establishing priorities for publicly funded health services (Mitton et al., 2009) aiming to improve patients’ experience with services (Ocloo & Matthews, 2016) and fostering the public’s trust in the health care system (Bruni et al., 2007). Fredriksson and Tritter (2017) point out that as service users, patients can provide valuable information about individual preferences and needs, but members of the general public can offer a more “disinterested,” societal view on health care services and allocation decisions. Consequently, balancing patients’ and citizens’ views is deemed to increase the responsiveness and legitimacy of health care policy decisions (Fredriksson & Tritter, 2017). Comparing patients’ or citizens’ views with those of clinicians who make resource allocation decisions can potentially improve the responsiveness of services even further by highlighting similarities and discrepancies between their views and allowing them to work towards harmonization of allocation priorities.
Therefore, to help improve prioritization practices in home care occupational therapy, we explored and compared the perspectives of OTs, older persons (OPs) and adults with disabilities on waiting list prioritization in home care occupational therapy. More specifically, we sought to understand participants’ rationale for prioritization and the underlying challenges and issues that guided their prioritization choices.
Methods
Design
In this article, we report on the qualitative component of a mixed-methods study. The main study (Raymond et al., 2018) consisted of a discrete choice experiment, a type of survey where respondents must choose a preferred option from a set of choices. In each choice task, the 714 participants were asked to select which of two referrals should be seen first by the home care OT. Statistical analysis allowed to quantify and compare the priorities for each group of respondents. For the qualitative component, inspired by Ryan et al. (2009)’s “think-aloud” interviews within a discrete choice experiment, we interviewed a subsample of participants who explained their answers as they completed the questionnaire in order to gain an understanding of the rationale, issues, and challenges guiding their prioritization choices.
Participants and Recruitment
Participants for the qualitative component were selected among the potential participants included in the main study. Maximum variation purposeful sampling (Patton, 2002) was used to ensure heterogeneity in OTs’ years of experience, and older and disabled persons’ age and gender. OTs were recruited from their provincial licensing board’s website. They were eligible if they worked in home care in the greater Montreal area. We considered the OPs and adults with disabilities in this study as targeted members of the public who may or may not be actual occupational therapy clients, reflecting a variety of standpoints on these services while having relevant experiential knowledge on aging or disability. OPs aged 65 or over were recruited from the bank of volunteer participants at the Institut universitaire de gériatrie de Montréal research center. The volunteers in this bank of participants are community-living individuals with an interest in geriatric research; the majority are in good health and have college or university education. Adults with disabilities, aged 18 or over, were recruited from two advocacy groups for people with physical disabilities in Montreal. OPs and adults with disabilities were eligible if they lived at home, were able to read and had no known cognitive impairments according to the organizations where they were recruited.
Potential participants were contacted by mail, and by telephone three weeks later if they had not replied. We continued recruitment until no new codes emerged during data analysis.
Data Collection
We conducted semi-structured, in-depth interviews inspired from think-aloud cognitive interviewing techniques (Drennan, 2003). During the interviews, participants were asked to complete the survey questionnaire while explaining the reasons for their answers. The questionnaire presented eight choice tasks requiring participants to prioritize one of two fictional referral scenarios (see Figure 1). Referral scenarios varied with respect to four factors: time already spent on the waiting list, ability to shower, history of falls in the home and ability to exit the home. The specific scenarios varied between questionnaires, but all questions required participants to make trade-offs between the different attributes of the referrals, that is, history of falls (none, one or a few), ability to shower (able without difficulty, able with difficulty and fear, or unable), ability to exit the home (able without difficulty, able with difficulty and fear, or unable) and wait time (2, 10, or 18 months). These four factors were chosen based on our previous analysis of referral prioritization criteria in home-based occupational therapy (Raymond et al., 2013) because they were frequently used in occupational therapy services but their priority level was inconsistent. In the main study (Raymond et al, 2018), the four factors were chosen by the research team to represent different outcomes such as access to services, quality of life, safety and social participation. The relevance of these four factors was confirmed during a pre-test of the questionnaire and interview guide with a convenience sample of seven people, spanning the three groups of participants (Raymond et al., 2018).
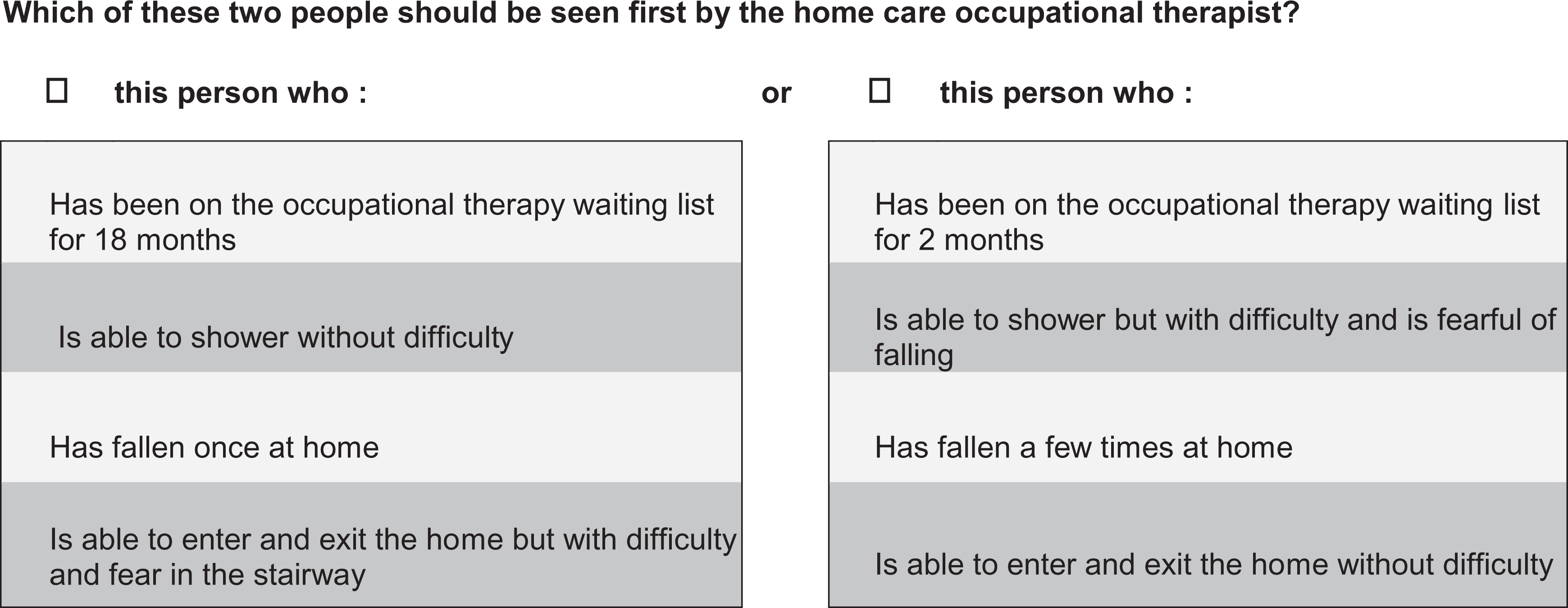
Sample survey question.
In the current, qualitative portion of the study, we used probes as needed to stimulate the discussion. For example: “What made you choose this person?” or “I noticed you hesitated here; can you tell me what was going through your mind?” (Collins, 2003). We also encouraged participants to elaborate on any thoughts regarding the issues that were present in the scenarios, such as explaining the meaning of the four problems described in the case scenarios. For example: “What do you think it might feel like to be unable to exit your home?”
Interviews were videotaped with the camera directed at the questionnaire because participants tended to point at the scenarios while speaking. Each interview lasted approximately 30–45 minutes and took place in a setting chosen by the participants: in their home, their workplace during lunch break, or at the research office. The participants and the interviewer (MHR) did not know each other but participants knew that the interviewer was an OT. Because her clinical experience may have influenced interpretation of the results, she used a reflexivity journal to document impressions and thoughts after each interview and during data analysis. These journal entries were discussed regularly with the other members of the research team, as well as with another researcher external to the project, in order to minimize potential bias.
Data Analysis
We used directed and conventional qualitative content analysis to analyze the data (Hsieh & Shannon, 2005). The verbal content of the interviews was transcribed verbatim by a professional transcription service. The first author then watched the videos while reading the transcripts to get a sense of the whole. Data analysis was performed in two steps using QDA Miner software (Provalis Research, 2011). First, following the deductive approach involved in directed content analysis (Hsieh & Shannon, 2005), we used the four attributes of the referral scenarios (wait time, ability to shower, falls, ability to exit the home wait time) as initial codes. We further coded the reasons given by the participants for prioritizing or not prioritizing each of these attributes. The codes from all interviews were then grouped into categories and subcategories as suggested by Hsieh and Shannon, separately for each group of participants. Results were then compared by noting similarities and differences between groups. Second, conventional content analysis (Hsieh & Shannon, 2005) was used to analyze the underlying issues and challenges that guided participants’ prioritization choices, separately for each group of participants. In this step, which is inductive in nature (Hsieh & Shannon, 2005), we highlighted meaningful units of text and allowed the codes to emerge from the data. We explored the relationships between the codes through monthly discussions with all research team members, drawing on the reflexivity journal in these discussions, and grouped the codes in categories and subcategories. This led to the identification of an overarching theme for each of the three groups of participants.
In order to foster credibility of the analysis, the coding and data analysis process were reviewed with all members of the research team, both at the beginning and towards the end of the coding process. Furthermore, excerpts from two interviews were coded by another team member (DF) and results were compared for further refinement of the codes. A decision trail was also kept during all steps of data collection and analysis.
Ethical Aspects
The project was approved by the research ethics committee of the Institut universitaire de gériatrie de Montréal research center. Participants received written information about the project before the interview and had a chance to ask questions before giving written informed consent. OPs and adults with disabilities received a gift certificate and OTs received an honorarium in compensation for their participation. Participants also received a summary of the results.
Findings
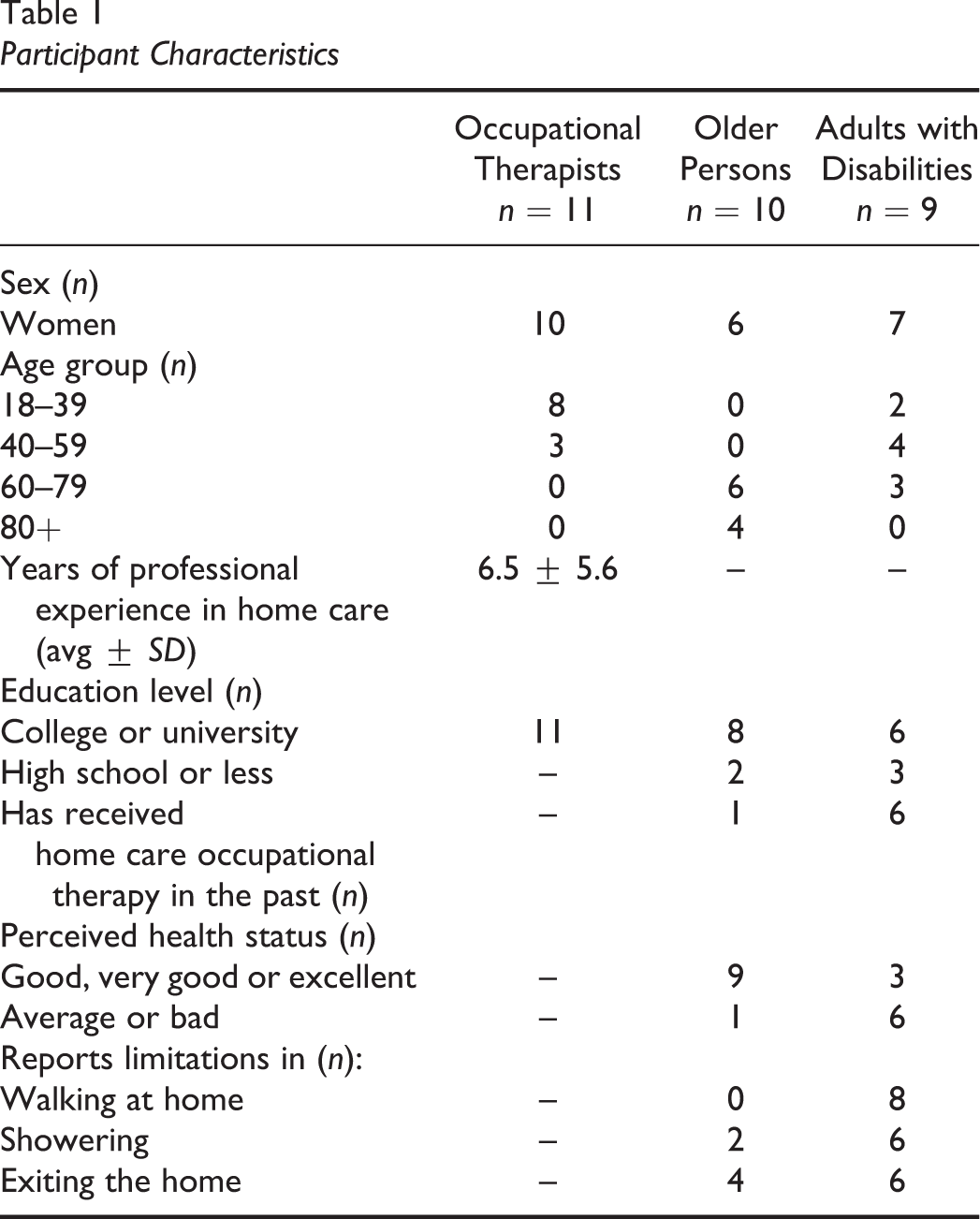
Eleven OTs, 10 OPs and 9 adults with disabilities participated in the study. All participants’ sociodemographic characteristics are presented in Table 1. All OTs worked at different institutions in the greater Montreal area. Women were predominant in all groups. In proportion, participants in the OPs group had a higher education level and better-perceived health than participants in the adults with disabilities group. Almost all adults with disabilities had functional limitations in walking, bathing, or exiting the home, and had either received or were on a waiting list for home care occupational therapy services. Few participants in the OPs’ group had functional limitations or had personal experience with home care occupational therapy services.
Participant Characteristics
In this section, we first present the rationale for participants’ prioritization choices based on the four types of problems presented in the referral scenarios. Subsequently, we present the challenges and issues that guided prioritization choices for each participant group.
Rationale for Prioritization Choices
Despite certain similarities, participants in each group had different interpretations of the four problems reflected in the referral scenarios, which influenced their prioritization choices.
Falls
For all three groups of respondents, the scenarios where the person had fallen were often prioritized due to the risk of injury.
For OTs, in particular, falls represented a threat to the person’s safety and physical integrity, which was the strongest factor in their decision. “You know, you break your hip, you can easily die” (OT #3). Prioritizing falls was also aimed at reducing health care costs and future demand for services due to injury.
OPs were particularly attentive to the fear associated with falling. “I’m afraid of falling. […] Like your hips, they become very very fragile as you get older” (OP #6). Physically disabled persons were more concerned with the self-image of the person who fell. “If I fall, I have to drag myself around to try to get up, I look like a worm” (Person with disabilities, [PWD] #10). For both older and physically disabled participants, how strongly they prioritized falls also depended on their own experiences with falls and whether they had been injured or not.
Ability to exit the home
All three groups of respondents recognized potential social and health implications of being housebound. Nevertheless, OTs did not tend to prioritize housebound people. “As OTs, we want our client to be integrated [in the community] as long as possible, active and all that, but when we prioritize…it’s not what stands out” (OT #2). One therapist explained that she did not prioritize clients’ needs to exit the home because her mandate was home care rather than community care. Some therapists said they were not comfortable with this restricted view of their mandate but still applied it in their choices.
Furthermore, many therapists argued that interventions to address problems with home access may not be feasible because they stated governmental subsidies are not always sufficient to adapt the entrance. Most therapists suggested alternative resources that could compensate for the person’s inability to get out of the house, such as ordering groceries or referring them to physiotherapy instead.
The OPs and persons with disabilities groups were more articulate about the emotional implications of being housebound. “It’s important to be able to go out, to have a social life, to be independent, to be able to, psychologically, not get depressed” (PWD #9). Many of them stated that being housebound could make you “go crazy” or were preoccupied with the risk of depression or even suicide.
On a more fundamental level, being able to get out of the home was seen by older or disabled participants as a means of belonging to society. “I have to go see people. […] I will sit at the mall, and I will look at the people walking by” (OP #4). Some viewed the housebound people in the scenarios as being “imprisoned.” One person explained that she used to feel like a bird in a cage when she was unable to exit her apartment building on her own. With the new automatic door opener obtained through her OT, “I can fly away. Now I can leave the building like everybody else” (PWD #5). For this participant and many others, being able to exit the home independently symbolized freedom and the possibility of participating in society.
Ability to shower
Although some OTs recognized that sponge bathing might not be as comfortable as showering, in general, they gave low priority to scenarios where the person was unable to shower because they could always sponge bathe instead. Having the ability to sponge bathe was seen as sufficient to maintain hygiene. Moreover, some therapists considered that problems with showering or bathing could be addressed by other categories of personnel such as specially trained home health aides. Whenever OTs did prioritize a scenario because of the person’s difficulty showering, it was because they perceived a risk of falling in the shower.
The views of the older and disabled participants on the importance of showering varied. For some, sponge bathing was not too problematic. For others, proper showering or bathing was much more crucial. “Can only sponge wash at the sink, so for me, it’s a catastrophe. I am going to die the day that I won’t be able to take a bath” (OP #7). Participants in those two groups generally perceived sponge bathing as less effective in terms of cleanliness. For some, proper bathing or showering was also important to reduce pain and improve flexibility. Many older or disabled participants were concerned with the odors that could develop from a lack of proper hygiene. For people with disabilities, body odor was important in terms of the person’s dignity. “Well, it’s the person’s dignity! When I get out of the shower and I smell good, I feel really good, I am ready to face a lot of things, you know” (PWD #3). One older participant explained: “If I have to take a sponge bath, it’s because…my balance, you know, is probably causing some problems” (OP #10). As such, scenarios where the person had difficulty showering were emotionally challenging for some older participants, who were reminded of their own declining independence.
Wait time
For all three groups of respondents, time already spent on the waiting list was a lesser factor in their choice of scenario. It was considered in relation to the other problems. “I will consider it, well for me, if the risks and the impact on function are about the same [in both scenarios]” (OT #1). In the OPs and disabled adults participant groups, scenarios with very long wait times elicited various emotional reactions. Some imagined that the person left waiting would feel rejected. “You feel like you’ve been forgotten…. It’s really, for your ego, it’s very hard” (OP #1). Others expressed feelings of anger, frustration or decreased confidence in the health care system.
Underlying Issues and Challenges Guiding Prioritization Choices
Throughout the survey, the three groups of participants viewed and interpreted the questions through a different lens, each tinted by their own challenges and issues. These lenses guided their prioritization choices by making participants more or less attentive to the various problems presented in the scenarios, and at times influenced the process or ease of their decision-making.
Occupational therapists
For the OTs, the main theme that arose when prioritizing referrals was a conflict of values. On one hand, regardless of which institution they worked in, therapists prioritized in order to maximize the client’s safety above all, with the aim of protecting their physical health and integrity and reducing health care costs. “I’ve been in home care for 10 years and I’ve become accustomed to the fact that that’s the priority. So, at one point, you end up thinking like the institution, so to speak” (OT #4). Conscious of the limited resources, they tried to find alternative solutions so that the clients could address their problems without occupational therapy. Keeping in mind their service’s prioritization criteria, they aimed for equitable distribution of resources and were careful not to favor certain clients at the expense of others.
On the other hand, many OTs expressed regret because they felt that their prioritization choices clashed with some of their core professional values. Prioritizing referrals based mainly on safety was often seen as a barrier to client-centered practice because therapists were unable to prioritize the client’s meaningful activities, like getting out of the house to participate in society, if their safety was not at risk. “What’s meaningful for the person isn’t necessarily meaningful for the health care system, and so they’re [clients are] sort of, they’re kind of stuck following what’s meaningful for the health care system” (OT #10). Some therapists also wished they could apply a more holistic view of health and well-being when prioritizing referrals. “I think it can be a good idea to consider the emotional aspect, but in all honesty, it’s not done” (OT #5). A few therapists expressed difficult feelings while becoming conscious of these conflicting values during the interview. One participant came to tears while struggling to choose between referrals, and another expressed disappointment with respect to her professional ideals: “It’s sort of ‘ouch’ in the sense that I didn’t become an OT just to, you know, evaluate falls and transfers. I became an OT precisely because I find it important to consider what is important for the person” (OT #10). Despite these tensions, these therapists maintained their initial priority choices.
Older persons
In the OPs group, the underlying theme was striving to maintain independence. This tended to make older participants favor referral scenarios where the person had difficulty exiting the home, with the explicit goal of preventing loss of capacities. Participants were also sensitive to scenarios where people had any sort of difficulty or fear, interpreting them as signs of an impending loss of capacities. “It’s frustrating because then we realize that we’re aging, we’re losing capacities, we used to do that, you know…” (OP #10). If left unattended, participants stated that difficulties could lead to a growing fear of falling or a sense of vulnerability that could keep the person from engaging in the activities that were important to them. “It can be enough fear to stop them from going out” (OP #5). Beyond reliance on health care services, they stressed the person’s own responsibility in adopting careful behavior to prevent injuries. “As for me, instead of being anxious, I tell myself, oops, use the handrail, be careful with each step” (OP #7). Above all, older participants emphasized the importance of overcoming these difficulties and fears: A lot of people give up. They say, “No, I can’t do it.” But you have to try. […] As long as you can, you have to tell yourself: “No, I’ll try to do that on my own…. I don’t want to stop. I will go for as long as I’m able to” (OP #6).
Persons with disabilities
The persons with disabilities group’s overarching challenge was a quest for social participation. Therefore, exiting the home was their highest priority, in the goal of allowing the people in the scenarios to be included, to be involved in meaningful activities and to contribute to society. For example, a few participants in this group were preoccupied with the impact of the problems described in the scenarios on the person’s ability to work and contribute to public funding. “I have to work because otherwise we won’t have enough money to pay for health insurance for all the other people too” (PWD #1). The scenarios presented in the questionnaires, in particular the people who had difficulty exiting the home, also evoked personal situations where the participants had felt excluded from society. “You know, I’m a person, I am able to make a difference in certain people’s lives, and it’s just, I’m a citizen, and give me a chance to reach my potential instead of parking me in a corner” (PWD #9). The physically disabled participants also worried about the impact of the problems in the scenarios on the person’s image or status in relation to others. One person explained that she felt bad when she fell and scratched her face. “I would like for my face to always look OK because I am handicapped and the only thing I have, not that I’m so beautiful, but, is my face” (PWD #5). One person with disabilities also stressed the importance of proper showering because body odor could give society another reason to marginalize the person.
The long wait times in the scenarios also reminded many participants with disabilities of difficulties they had experienced in accessing occupational therapy or other health care services. Because of delayed access to services, some had to use alternatives that compromised their dignity. For example, one participant discussed modifications she had made to her eating habits as a result of not receiving occupational therapy to help her. “Now I stopped eating steak, I only eat ground beef because I’m not able to cut my food. Well for me, eating steak like that, I feel sort of like an animal” (PWD #2). Many participants in this group felt that because their service needs were less often related to safety, they did not fit with the system’s priorities, which made some feel disillusioned. “For me, now, I try to avoid having to do with them [OTs]. And I find it frustrating to have to go through an OT according to criteria that are imposed on them” (PWD #8). All in all, through their referral priority choices, participants with disabilities stressed the importance of allocating occupational therapy in such a way as to maximize clients’ opportunities for participation, in line with the client’s individual priorities.
In summary, despite certain similarities, the way each group of participants interpreted and prioritized the four problems in the referral scenarios differed according to the various issues and challenges underlying their perspectives.
Discussion
The results of this study highlight the unique perspectives of home care OTs, OPs and adults with disabilities on waiting list prioritization criteria. The analysis revealed that there were more differences than similarities in each group’s views. Their waiting list prioritization preferences were influenced by different pursuits: OTs struggled to reconcile conflicting professional values, OPs strove to overcome fears and maintain their independence, and persons with disabilities called for more inclusion, participation, and enfranchisement in health care services and the rest of society.
The OTs’ viewpoint was characterized by a conflict between values they attributed to the health care system, namely safety, physical integrity, and equity, and other professional values such as client-centered practice, that is, respecting the client’s choices and priorities, and holism, that is, adopting a broader view of health and interventions. In studies exploring OTs’ values (Clair & Newcombe, 2014; Drolet & Désormeaux-Moreau, 2016), safety is often said to enter in conflict with other values such as respect for the client’s autonomy. In the present study, therapists prioritized safety even if it had to be done at the expense of social participation and independence. Rather than reflecting a lack of awareness on the importance of these outcomes for older and disabled persons, the therapists’ prioritization choices and the difficulties they encountered while making them may illustrate tensions that can occur as OTs struggle to reconcile their professional values with organizational needs and systemic constraints (Durocher et al., 2016; Mackey, 2014). None of the therapists in the current study mentioned individual institution-specific policies to justify their prioritization choices. Rather, these choices could be rooted in what Carrier et al. (2015) call the “home care discourse,” stemming from the governmental home care policy, which states that the program’s main goal is to help clients remain at home as long as possible.
From the OPs’ stance, home care occupational therapy was seen as a valuable service that could help clients hold onto their fleeting independence. Nonetheless, beyond access to services, these participants focused on their personal responsibility in confronting their fear of falling and remaining active. This point of view reflects coping strategies used by some seniors to adapt to aging, such as self-control and accepting responsibility (Levasseur & Couture, 2015) instead of restricting their activities. Occupational therapy could support the use of appropriate coping strategies by teaching them early on so as to prevent disability (Provencher et al., 2016). However, doing so in a timely manner would require a shift from the current curative approach of home-based occupational therapy to a prevention and health-promotion approach (Turcotte et al., 2015). In the long run, prevention and promotion may save time and eliminate future demand for services.
For the disabled participants in this study, the waiting list prioritization tasks evoked frustrations they had experienced when trying to access services, and also revealed their quest for participation and participation enfranchisement. Participation enfranchisement entails not only being included but also being a valued and respected member of society (Heinemann et al., 2013). In general, participants in this group viewed occupational therapy services as essential in order to overcome difficulties in certain valued occupations such as showering and getting out of the home. Because these activities represent gateways to social participation and dignity, they wished that they could be given higher priority on waiting lists even if limitations in these activities do not necessarily compromise their safety. The opinions of the physically disabled participants in our study are consistent with the findings of Neri and Kroll (2003), who report that disabled adults who have difficulty accessing health care services experience feelings of devaluation and limitations in social participation. Equally, Fadyl et al. (2011) found that people with disabilities need to be more involved in their health care services and ask that response to health care needs be adapted to each person’s unique context.
Study Limitations
The OPs and disabled participants in this study were not recruited as actual occupational therapy clients but were recruited for their lived experience of age or disability. In particular, the OPs group had few functional limitations and little experience with occupational therapy services, suggesting that their opinions may be more reflective of the public than the patient perspective. Therefore, although the results of this study cannot be transferred to home care occupational therapy clients, they highlight a range of public and patient perspectives that can be considered when making resource allocation decisions. Furthermore, for statistical reasons, the scenarios used in the questionnaire included only four of the many possible attributes of true occupational therapy referrals. Other perspectives may have emerged with actual, more complete referrals.
Future Research
Ideally, participatory research would bring therapists, actual service users, members of the public, caregivers and program managers together to come to a mutual agreement on waiting list prioritization criteria. Such participatory research could serve as a basis for developing a standardized referral prioritization tool and for approaching decisionmakers at the policy level, in the hopes of addressing the systemic or social factors that influence resource allocation in home care.
Implications for Practice
This study shows that home care OTs, older members of the public and adults with disabilities can have valuable and complementary perspectives on waiting list prioritization criteria. Although safety remains an important concern, findings show that other outcomes, such as independence and social participation, may need to be considered more often when prioritizing referrals. In a context of limited resources, OTs need to be fully aware of these competing outcomes and to be creative in their search of solutions to maintain their full scope of practice, in alignment with their professional values and the potential needs of their clients. First, seeking the opinion of clients, caregivers or patient partners on their program’s waiting list prioritization criteria would likely provide valuable insight to improve service allocation. Furthermore, clinicians and managers could examine their waiting list management practices to see if certain clienteles are systematically pushed back on the waiting list by higher priority referrals. If so, it would be possible to use strategies to ensure that these lower-priority clients eventually access services, such as applying maximum wait times or dedicating staff to these clients (Raymond et al., 2016). However, if these changes cannot be implemented without seriously compromising the safety of higher priority clients, it may not be realistic to achieve them without increased funding to home care programs.
Conclusion
This study sheds light on issues and challenges underlying waiting list prioritization in home care occupational therapy. Although OTs tend to prioritize problems that compromise the person’s safety, they experience a conflict of values in doing so. Seeking the perspective of older and disabled participants has shown that issues around independence and participation may be equally important to consider. Ongoing reflection about waiting list management is necessary to align resource allocation with the priorities of OPs and disabled community-living individuals.
Key Messages
Home care OTs, OPs, and persons with disabilities have different perspectives on occupational therapy referral prioritization criteria.
While OTs mainly prioritized referral scenarios based on the person’s safety, older and disabled participants mainly aimed to maximize other outcomes such as independence and social participation.
OTs should be aware of these competing outcomes when prioritizing referrals and seek to align their prioritization practices with the priorities of their clientele.
Footnotes
Acknowledgments
We wish to thank all participants and the organizations where they were recruited as well as Services Verbatim for interview transcriptions.
Author Contributions
All authors participated in study design, data analysis and writing the manuscript. Marie-Hélène Raymond performed data collection.
Declaration of Conflicting Interests
Marie-Hélène Raymond was employed part-time as a home care occupational therapist at the time of the study, working mainly with OPs. She did not know any of the study participants personally. She was also a supporting member of Ex aequo, an advocacy group for persons with physical disabilities (2014–2017). Debbie Feldman and Louise Demers declare that they have no conflicts of interest.
Funding
This study was funded by the Quebec Rehabilitation Research Network (REPAR) in partnership with the Office des personnes handicapées du Québec. Marie-Hélène Raymond received support from the Fonds de la recherche du Québec-Santé and the Centre for Interdisciplinary Research in Rehabilitation of Greater Montreal.