
Abstract
Western Australian schools are expected to educate beyond the classroom context, promoting the health of students, their families and their communities. Little is known about the frequency with which schools employ newsletters to communicate health messages. This content analysis draws from a sample of 70 newsletters from 46 diverse Western Australian schools, to explore the frequency with which health messages were communicated. Across an average of 1.3 newsletters per school during the November period, 48 instances of a health-promoting message were identified, giving an average of 0.69 health-promoting messages per newsletter. This result suggests that school newsletters may be underutilised as a mechanism for health promotion within school communities. While mental health issues were explored to the greatest extent, a number of areas, such as smoking, alcohol and substance abuse and sun safety received limited attention. Health-promoting messages about driver road safety were comparatively highly represented in the sample, which was unanticipated. While this paper offers insight into the frequency of health message communication through newsletters, and the kinds of messages being transmitted, longitudinal research in this area could provide further insight, in addition to examination of parental perceptions of school newsletter mediated health messages.
Keywords
Introduction
Education in Australian schools is not solely concerned with the facilitation of learning experiences in the classroom, and nor are the students the exclusive subjects of learning. Contemporary Western Australian public (also known as government) schools are expected to play a role in promoting the health of students, their families and their communities. Promotion of student health is imbedded in the Australian Curriculum, with “Personal and Social Capability” one of its General Capabilities, and this includes a health element that is concerned with fostering students' “sense of self-worth, self-awareness and personal identity that enables them to manage their emotional, mental, spiritual and physical wellbeing,” helping students to “form and maintain healthy relationships” (Australian Curriculum, Assessment and Reporting Authority (ACARA), n.d. c). The expectation that health education extends beyond classroom delivery to parents and the community is a key component of state based policies for health education. For example, the Department of Education, Western Australia (DETWA) is supportive of a Health Promoting Schools Framework (DETWA, n.d.), which promotes the World Health Organisation's (WHO) Global School Health Initiative, in which school based health promotion is not limited to student education, rather it “strives to improve the health of school personnel, families and community members as well as students” (WHO, 1998, p. 2). The WHO document was preceded by an Australian government initiative from the National Health and Medical Research Council (NHMRC) (1996), which includes the school providing “consultancy, advice and advocacy to school personnel (e.g. teachers, administrators), students and parents, either on specific health issues or on more general approaches to school-based health promotion” (p. 19), positioning schools as health educators to their families and communities. The role of schools in providing health education beyond school boundaries is well-recognised, as “schools also provide a valuable link with parents and the community” (Lynagh, Schofield, & Sanson-Fisher, 1997, p. 44). Thus, engagement with parents is situated as a key factor in the success of school health initiatives.
In line with this holistic conception of community health education through schools, school newsletters are used to inform parents of health promotion initiatives and issues that may impact on student and family health. The use of newsletters as a mechanism to promote health is unlike health education in the classroom, as the intended audience and subject is the adult parent or guardian. In their evaluation of current research, in health promotion in schools, Leger, Kolbe, Lee, McCall, & Young (2007) found that formal intervention, such as specific program implementation, was not necessary to precipitate significant health gains within the school community, and that school engagement with its local community, including parents, is a factor which contributes to the building of “health protective factors,” reducing “risk taking behaviour” (p. 111). Thus, informal health education initiatives disseminated through school newsletters may yield educational benefit for both students and their parents, as “involvement of parents, care-givers and local community members can act as a strong reinforcement and support for strategies implemented in schools” (Lynagh et al., 1997, p. 44). Researchers have commonly used school newsletters as part of a suite of educational initiatives to transmit health-promoting messages, as parents are situated as “perhaps the most frequent and important partners” in school based health promotion (Burgher, Rasmussen, & Rivett, 1999, p. 8). For example, Fekkes, Pijpers, and Verloove-Vanhorick (2005) suggest that, “schools can inform parents via newsletters on the school policy on bullying and explicitly ask parents to report to the teacher if their child is being bullied” (p. 88). The use of school newsletters as an educational vehicle is seldom interrogated, with limited research exploring frequency of educational message dissemination, and which messages are commonly shared in this manner.
In order to investigate the use of school newsletters to promote health messages, an extensive content analysis of newsletters from Western Australian public schools was undertaken. Exploring the role of the school newsletter in providing education to parents beyond the physical confines of the school can be perceived as reflective of a social ecological theory of health promotion, as it accounts for environmental influences on health and well-being, acknowledging “the interdependencies that exist among a person's … major activity setting and life domains,” as well as the effect of “physical and social conditions” on well-being, with meaningful intrapersonal interactions, such as those between parent and child, situated as influential (Stokols, 1996, p. 288–289). When students learn about a health promotion issue, and parents reinforce awareness of this issue in the home context after being informed via school newsletters, this recognises core principles of the ecological model, in that it is responsive to the importance of “multiple influences on specific health behaviors,” reflective of the theoretical premise that “multi-level interventions should be most effective in changing behaviour” (Sallis, Owen, & Fisher, 2008, p. 466). This research sought to develop insight into the extent to which school newsletters are used to promote health, as well as which health promotion messages Western Australian public schools sought to engage parental support for.
Method
Sample
In order to determine the sample for the content analysis, an online Sample Size Calculator was used (Creative Research Systems, n.d.). The following formula was used:
Z = Z value (e.g. 1.96 for 95% confidence level) p = percentage picking a choice, expressed as decimal (.5 used for sample size needed) c = confidence interval, expressed as decimal (e.g. .04 = ±4).
The total number of public schools in Western Australia in 2014 was first determined. The sample was based on 518 public primary schools and 174 public secondary teaching institutions – including district high schools, which also cater for primary school students, and colleges. Mature age colleges were excluded from the sample. Sample size calculation determined that data from 21 secondary schools and 23 primary schools would be needed, and thus it was decided to sample from 23 schools in each category to ensure a balanced sample.
Subsequently, an online true random number generator tool (random.org) was used to define a random sample of 23 primary schools and 23 secondary schools/district high schools from the full list of all Western Australian public schools.
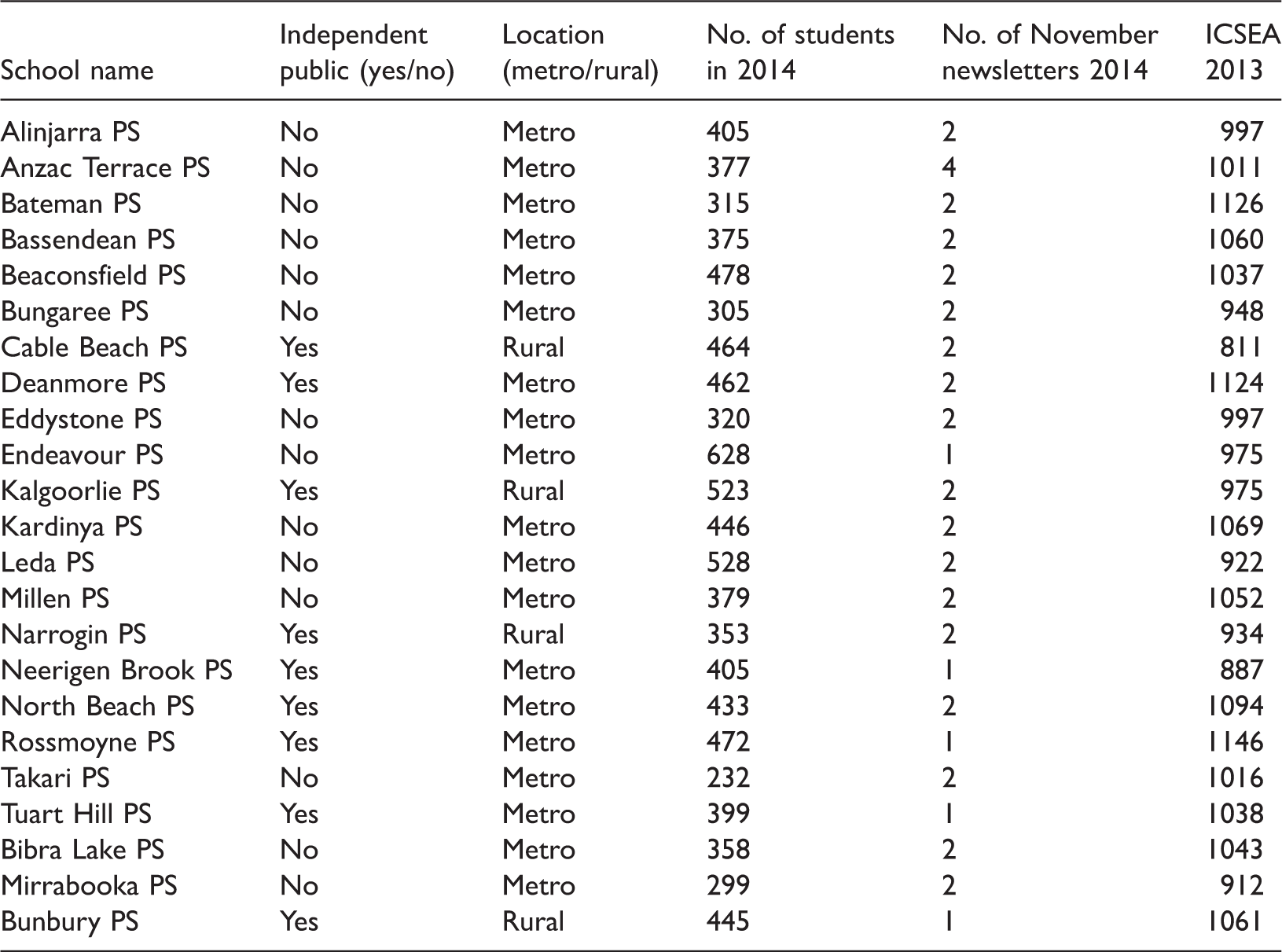
Primary schools (PS)
Secondary schools: District high schools (DHS), senior high schools (SHS), and secondary colleges (SC). a
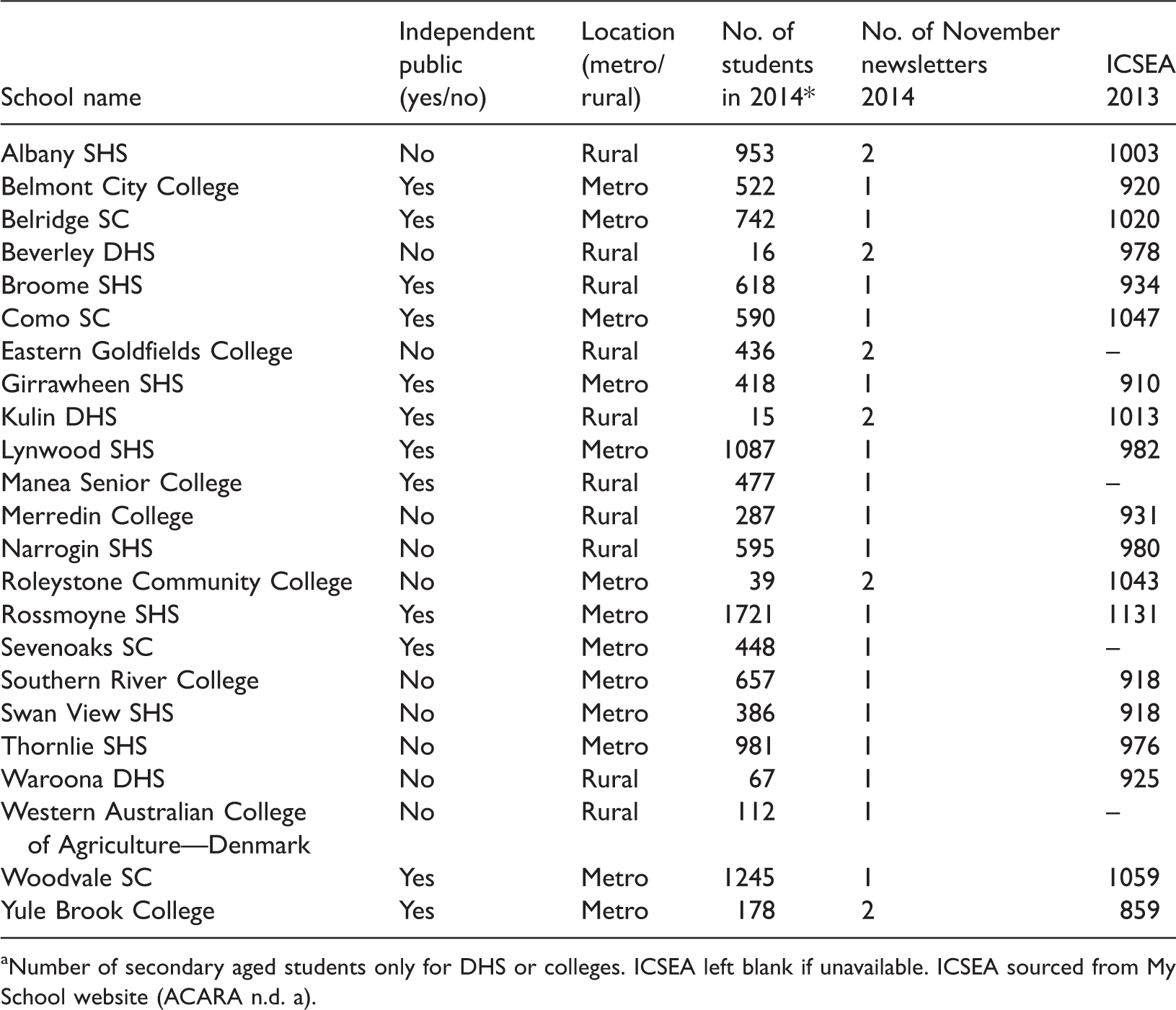
Number of secondary aged students only for DHS or colleges. ICSEA left blank if unavailable. ICSEA sourced from My School website (ACARA n.d. a).
Their school value on the Index of Community Socio-Educational Advantage (ICSEA) is included to illustrate the diversity within the range. The Average ICSEA value for primary and secondary schools is 1000 (ACARA, n.d. b).
Method of analysis
The method of content analysis employed was Conventional Content Analysis (Hsieh & Shannon, 2005). This inductive approach avoids the use of pre-developed categories to allow these to emerge from analysis of the data, and the typical reporting order is different, as “relevant theories or other research findings are addressed in the discussion section of the study,” rather than in the introduction (Hsieh & Shannon, 2005, p. 1279). The data collection was limited to the newsletters output of each school over one month, namely November 2014. This timing was not only convenient for the authors but also well away from both the start and the end of the school term. Newsletter output varied between schools, with a range of 1–4 newsletters over this month. Primary schools had a higher newsletter output, with 41 newsletters ultimately sourced from the primary school sample, and 29 newsletters from the secondary school sample (N = 70). The overall average was 1.3 newsletters per school.
Defining and identifying health messages
To identify health messages, criteria needed to be established to create a useful working definition, as health issues were communicated in newsletters in a variety of forms, from brief, shallow mentions of an issue with no supporting information, to detailed educative sections with supplementary website links. There is no guarantee that the inclusion of health education messages in school newsletters signifies that they are informed by “theoretical models that identify influences in the behavioural change process” (Corcoran, 2007, p. 10). However, even without an understanding of a theoretical base, it is likely that the school staff crafting the messages in the newsletters might have at least an intuitive understanding that a health message should be communicated in a persuasive manner in order for it to have any potential to trigger behavioural change (National Collaborating Centre for Methods and Tools (NCCMT), 2010).
For the purposes of this analysis, health messages were defined as the presentation of health information about a health issue impacting on students and/or their families, inclusive of any educational information, which could be perceived to constitute advice or persuasion. Clearly, this is a subjective measure, particularly in the absence of similar research studies to inform the criteria. Focus questions were applied to identify if the message warranted inclusion. Both needed to be met in order for inclusion.
Is a health issue/message mentioned? Is the issue supported by educative information aimed at informing and/or engaging parents?
For example, one primary school announced a new mandatory uniform policy for the wearing of hats with a 360-degree brim. This section did not provide any explanation as to why a 360-degree brim was desirable in relation to sun safety, and therefore the item was excluded from analysis. An item in the same newsletter detailed the Walk to School Day Health Breakfast; it included a description of what constituted a healthy breakfast, and thus this was included. This item however did not include a supporting comment about why a healthy breakfast is beneficial, and thus it would be considered to be at the shallow end of what constitutes educative provision.
These messages were not limited to those clearly supported by school-based learning. Advertisements for health workshops provided by external providers were included when a health message was apparent in the advertisement. Safety messages, such as advice about road rules and sun safety, were also included as they were viewed as being health promoting.
As there is scope for a considerable degree of subjectivity in this area, the researchers sought to establish intercoder reliability in an “attempt to reduce the error and bias generated when individuals (perhaps unconsciously) take shortcuts when processing the voluminous amount of text-based data generated by qualitative inquiry” (Hruschka et al., 2004, p. 309). Two coders independently coded the responses, and then discussed discrepancies, negotiating modifications until a final dataset was created. This dataset included the agreed upon health promotion messages and the negotiated codes.
As such, while the analysis in this paper is concerned with the manifest content, “the visible, obvious components” of the newsletters, it is also concerned with the latent content of the texts (Graneheum & Lundman, 2003), in the consideration of which health messages could be deemed health promoting.
Findings
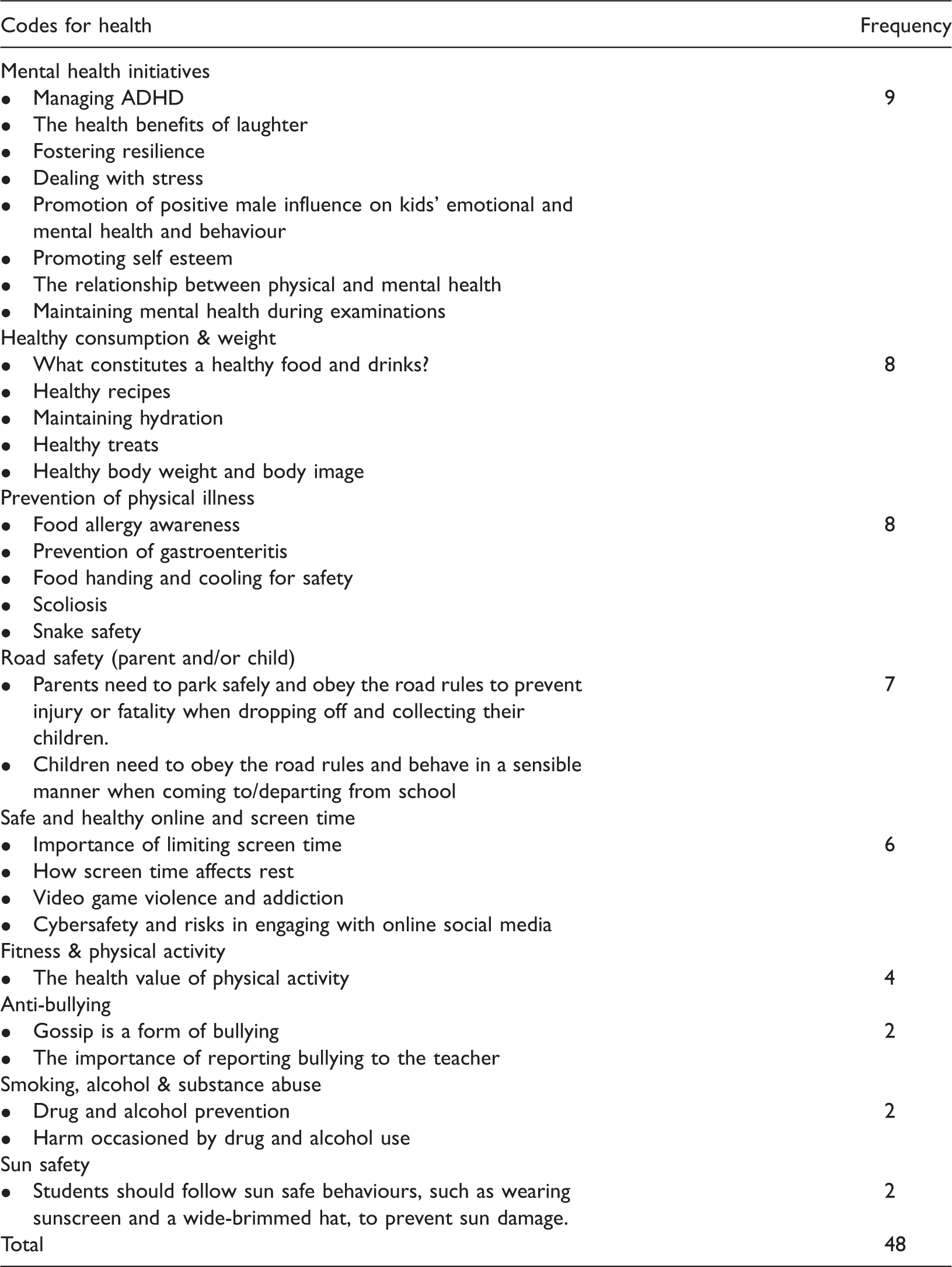
There was a range of health issues explored in the November newsletters, with a total of 48 instances observed across the 70 newsletters in the sample, giving an average of 0.69 health-promoting messages per newsletter. A number of categories could have been subsumed into other codes; for instance, anti-bullying could have been categorised as a mental health and physical health issue, however it receives significant research attention in its own right, and thus agreement was reached between coders to maintain it as an independent code.
Frequency of health promotion messages in school newsletters.
Discussion
That the average across the range was less than one health-promoting message per newsletter (0.69) suggests that school newsletters are being underutilised as a source of health promotion in the school community. While all of the health codes discussed in this paper had relevance for both primary and secondary students, it was expected that emphasis would differ in response to the different developmental levels of young people, occurring across the schooling continuum. In the new Australian Curriculum for Health and Physical Education, this is situated as a “key idea” and is described as the provision of “ongoing, developmentally appropriate and explicit learning about health and movement” (ACARA, n.d. e). For example, road safety in primary school would be expected to be primarily concerned with the fundamentals, such as looking both ways before entering a road as a pedestrian, while road safety at secondary level was expected to be concerned more with entering the road as a driver. However, due to the paucity of road safety messages aimed at young people at either school level, this progression could not be observed.
A variety of mental health initiatives were communicated during this period, and it is likely that the comparatively high frequency was reflective of local mental health events in October and November, such as Mental Health Week and World Mental Health Day. Some initiatives were specifically focussed at parents, such as information and guidance given about Triple P Positive Parenting (Lynwood Senior High School, 2014). Engaging parents in mental health promotion by providing clear health-promoting messages that place parents in a supportive role is reflective of the positioning of parental liaison as a key component of a successful whole-school approach to mental health. In-class skills work alone has been found to be insufficient, “and that for optimal impact, skills work needs to be embedded within a whole-school, multi-modal approach which typically includes changes to school ethos, teacher education, liaison with parents, parenting education, community involvement and coordinated work with outside agencies” (Weare & Nind, 2011, p. 65).
Healthy food consumption and weight was given greater focus than fitness and physical activity, with greater emphasis on what students eat than their exercise levels. While physical activity was often mentioned in the newsletter, there were only four instances of it being mentioned in the context of being a healthy activity. While the elements of good nutrition can be taught to students at school from a young age, as parents are the primary providers of students' foods, student agency is likely to be limited, and parents' personal food preferences have been found to be highly influential over their children's choices (Birch & Fisher, 1998; Scaglioni, Salvioni, & Galimberti, 2008). Partnership with parents was fostered through a range of initiatives; for example, two rural district high schools featured an identical “Go Health! What's in a treat?” section, which discourages parents from rewarding their children with unhealthy food, and suggests a range of healthy alternatives (Beverley District High School (Beverley DHS), 2014, p. 5; Kulin District High School (Kulin DHS), 2014, p. 5).
The comparative frequency of health promotion messages around road safety aimed directly at driving parents rather than driving or pedestrian students was unanticipated. These messages were accompanied on occasion by visual supports, such as diagrams illustrating what constitutes double parking (Deanmore Primary School (Deanmore PS), 2014, p. 9). Only one of the seven messages was concerned with health issues arising from students' behaviours – the other six were directed at parents picking up children from dangerous locations; speeding in the school zone; driver distraction, with the risk of using a mobile phone while driving highlighted; and double parking. Parental irresponsibility in regard to ensuring the safety of children in school zones was strongly addressed, with one principal requesting parents “don't be cavalier with the safety of someone else's child when you would not put your child in such danger” (Bateman Primary School (Bateman PS), 2014).
Safe and healthy online and screen time was urged in six instances, with importance of limiting screen time, impact of screen time on sleep, video game violence and addiction and potential health and safety risks in engaging with online social media all explored. As schools increasingly adopt a Bring Your Own Device (BYOD) approach, and presumably subsequently increase the screen time of their students, using school as a site for promoting the recognition of health issues that occur during online time is particularly pertinent (Merga, 2015).
Anti-bullying messages appeared at the same comparative infrequency as messages about Smoking, Alcohol & Substance Abuse, with both categories only mentioned in a health-promoting manner twice. This was unanticipated, as the annual Leaver's Week (also known in the Eastern states of Australia as Schoolies Week) occurred between the 24th and 27th November in 2014. Such celebrations are frequently accompanied by substantial alcohol and drug abuse (Lam et al., 2014), so a high level of engagement of parental support to encourage safe behaviours was anticipated, but not observed. Research also suggests that Leaver's or Schoolies participants are at risk of engaging in unsafe sex (Lubman, Droste, Pennay, Hyder, & Miller, 2014), however there were no health-promoting messages about safe sex practices in the school newsletters studied. While schools more frequently mentioned that their students had participated in activities around issues such as anti-smoking educational initiatives, they rarely did so in a manner that explored the health imperatives of these approaches to any degree. This was surprising as research suggests that “family norms and attitudes also strongly affect adolescent smoking” (Viner et al., 2012, p. 1647), and thus greater emphasis in engaging parents was expected. “Alcohol and other drugs” becomes a focus area of the new Australian Curriculum as early as Year 3 (ACARA, n.d. d), and as such, the importance of early and ongoing health promotion in this area may gain increased attention. The focus in anti-bullying was to identify gossip as a form of bullying, and to encourage the reporting of bullying, relatively shallow explorations of the issues.
As November newsletters were selected, and November is the month before the season of summer officially begins in Australia, it was anticipated that a greater focus on sun safety would be observed, however there were only two instances of sun safety messages mentioned. Temperatures are generally warm in the Perth metropolitan area during this month, with a mean average of 26.5 ℃ and relatively low rainfall, with only six rain days on average (Weatherzone, 2015), so outdoor activities and play can be embraced. The UV index in Perth as recorded between 11:50 and 13:20 over each day of November in 2014 ranged between 9 and 13 (Australian Radiation Protection and Nuclear Safety Agency (ARPANSA), 2014), and therefore the Perth Metropolitan consistently reached the very high (8–10) and extreme (11+) UV ranges (Australian Government Bureau of Meteorology (AGBM), 2015). As parents are usually the providers of hats and sunscreen, a greater emphasis on sun safety would be recommended.
Limitations
This study was constrained by a number of limitations. The school newsletter is not the only means of communication with parents, so this study does not capture health promotion messages communicated with parents through other means. Subjectivity in data interpretation and analysis is a key issue when evaluating the “trustworthiness of findings in qualitative content analysis” (Graneheum & Lundman, 2003, p. 106). Having two parties code the data was an effort to overcome this issue, however it is a limitation inherent in the method. Impact of grants, international and community events and competitions may all influence the findings by directing health interest, as well as research interests of school-based researchers where relevant. While the sample size of 46 schools is robust, yielding 70 newsletters, the analysis is of health messages transmitted over a single month. A greater period of time would give more holistic and fulsome insight into the health messages schools deem worthy of transmission.
This sampling strategy no doubt lead to an over-representation of schools inclined to communicate via electronic means, presumably with parents with high levels of digital literacy. Small schools in remote areas were often excluded due to the lack of an online newsletter, and even a school website in many cases. Despite this limitation, a diverse range of schools were in the sample, which was inclusive of number of schools outside the metropolitan area, as per Tables 1 and 2.
Conclusions
This study aims to provide insight into types of health messages being disseminated by schools. Capturing information about which health messages are deemed important enough to justify transmitting to parents through newsletters offers some insight into the key health concerns as determined by contemporary schools, as well as the breadth of the range of issues they promote. Data collection over a greater period of time would provide a longitudinal insight into the range of health messages contemporary Western Australian schools deem worthy of transmission.
The school newsletter was found to be underutilised as a mechanism of health education, though whether this is due to the exploitation of other mechanisms of school/parent communication is beyond the scope of this study. A number of areas were surprisingly under-addressed, most notably sun safety despite the increasing UV levels in November, and alcohol and drug abuse, despite the positioning of Leavers Week at the end of November, with unsafe sex not addressed at all. Innumerable lost opportunities were observed, where a health issue was given a cursory mention without any supporting educative information. Road safety initiatives are generally concerned with instructing children in road safety, both as pedestrians and future drivers. That a number of schools used their newsletter to address the unsafe driving practices of parents for the health promotion of their students is an area warranting further consideration and study.
From an educational perspective, health promotion interventions in school newsletters could also be evaluated in terms of their accessibility in future research. At this stage, little is known about whether most school newsletters meet the literacy levels of the nearly half of Australian adults performing at under Level 3 in literacy (Australian Bureau of Statistics (ABS), 2008), and thus future research is warranted to examine the general accessibility of school generated attempts at health promotion through newsletters. While schools are accustomed to adapting content through teaching and learning adjustments to be responsive to student communication needs, whether the same level of consideration is given to meeting parent communication needs is not known. Health messages could be tested by a readability tool for complexity. Accompanying pictures or diagrams would also help to improve accessibility. It would also be useful to explore how the intended parental audience receives these attempts at education and/or intervention, as parental feedback is situated as a key component of educational interventions (NHMRC, 1996), and yet the effect of health messages received through the newsletter conduit on parents is not well understood.
While this paper does not evaluate the prevalence or efficacy of specific health initiatives or interventions, it provides insight into the current messages schools use to engage community support. The findings suggest that schools should consider increasing their use of school newsletters to communicate key health messages to be responsive to the new Australian Curriculum requirements in Health and Physical Education, as well as the general capability, “Personal and Social Capability”, which should be addressed across all learning areas.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.