
Abstract
Reduced school attendance is a recognised risk factor for poorer outcomes both educationally and across a wide range of social, economic and personal indicators throughout life. Children and young people with chronic health conditions often have poor or disrupted records of school attendance due to periods of hospitalisation and time spent recuperating at home. Keeping students with health conditions connected to school and learning is critical to avoid a trajectory of school absence, disengagement from schoolwork and peers, reduced achievement in education and early school leaving. This paper reports on a research project conducted in Victoria, Australia, to connect 7–12 year old hospitalised children with their school using a specially designed Presence App run on a mobile tablet computer. Nine hospitalised students, their families and schools participated in the trial. Results indicate that the Presence App helped to create and maintain a social presence for the absent child in the classroom and keep students at risk of disengagement connected to school. Our research also showed that while the ‘Presence’ App complemented existing information and communication technology such as videoconferencing and email by connecting hospitalised student and school, it had added advantages over these modes of communication such as creating an on-going classroom presence for the hospitalised child while respecting privacy and attempting to minimise disruption in the hospital and classroom settings.
Keywords
Introduction
Research has shown that children and young people managing a chronic health condition are at higher than usual risk of underachieving academically when compared with their healthy peers (Conley & Bennett, 2000; Forrest, Bevans, Riley, Crespo, & Louis, 2011; Martinez & Ercikan, 2009; Needhan, Crosnoe, & Muller, 2004; Shiu, 2004; Venning, Eliott, Wilson, & Kettler, 2008). Absence from school is a key trigger for school disengagement (Daraganova, 2012; Withers, 2004), and the longer the student is absent, the higher the risk of disengagement and subsequent school drop-out (Balfanz, Herzog, & Mac Iver, 2007). For many students with chronic health conditions, school absence is an unavoidable side effect of ongoing medical treatment, whether in hospital or during recovery periods at home. Reducing the risk of disengagement during these periods of absence is critical in avoiding premature school leaving and educational underachievement for these students. Since the absence itself may be unavoidable, there is a need for strategies to be employed to overcome the effects of such prolonged or repeated absence. This paper reports on a project which developed a technology-based intervention designed to connect students in hospital with their schools, teachers and classmates. The aims of this research project were to:
Examine the current use of technology as a means to connect family members and their hospitalised child. Develop a software application designed to improve the sense of awareness and presence of hospitalised children in home and school settings during periods of absence. Trial the application using tablet technology in a three-way set up (triad) of hospitalised child, home and school. Assess the response to the software application across the hospital, school and home settings for children and young people, parents and siblings, and teachers and classmates.
The findings of the project which relate to the first two research aims have been reported elsewhere (Heidari, 2013; Vetere et al., 2012). This paper reports the findings of the technology trial itself, in the hospital, school and home and discusses the response of users of the software (the Presence App) which we developed and trialled.
While a large and growing number of information and communication technologies (ICTs) such as videoconferencing and email are available off-the-shelf to facilitate communication, our project tailored an approach which carefully considered the specific contexts of the hospital ward and the school classroom by (a) balancing the competing needs for communication and connection with the need for patients, health care workers, teachers and families to maintain privacy and control over personal and sensitive information; and (b) minimising disruption to both medical care and classroom learning. Both hospital and school settings can involve numerous groups of people (students, staff, families, other patients) who may have differing views as to appropriate information to be conveyed technologically to a remote setting. Balancing the need for the individual to remain connected against broader needs for privacy and lack of disruption are ongoing concerns for any technology designed to benefit children and young people, especially those made vulnerable by extended health care, or in situations where parents are not present.
Background and context
In this section, we discuss the use of ICTs to connect hospitalised children to school during periods of absence. In reviewing the literature, we highlight the benefits and disadvantages of different types of ICTs for use in hospital and classroom settings. We outline how the design of the Presence App has been informed by previous research which shows that a sense of social presence can be created by using unobtrusive media rather than information rich media such as videoconferencing. Such low-information media has the added advantage of minimising disruption to home, hospital, school and classroom routines.
Education policy for children with health conditions
Education is a right for all children (UN declaration, 1959) and attendance at school is mandated for all children (within age ranges which vary slightly state by state) in all Australian jurisdictions. Yet, not all children are physically able to attend school, often for reasons of ill health. All Australian state education departments allow exemptions from school attendance requirements for children whose health status precludes them from attending, however little legislative attention has been paid to ensuring that the educational needs of children thus exempted are still being met. ICTs offer potential new means of ensuring children’s right to education is not restricted through school absence due to health care.
Connecting the absent child to their classroom
Maintaining connections to school for children absent due to reasons of health requires both that the child remain interested and engaged, and that the school, classroom teacher and child’s classmates also keep the absent child in mind, both as a friend and as a learner (Yates et al., 2010). While schools are increasingly recognising the importance of supporting the absent child to keep up with school work through emailed or hard copy exchange of worksheets, projects and other forms of homework, maintaining social connections has been more difficult. Increasingly, ICTs such as email and videoconferencing can provide effective mechanisms for maintaining connections between the absent child and his/her class peers. This has the potential to overcome some of the negative outcomes often associated with extended absence from school.
Researchers have begun to examine the design and use of ICTs by hospitalised children. A wide range of ICTs are already being trialled in paediatric hospital settings, aiming to meet a range of social, educational and personal needs of children separated from their usual schools and homes. While many technologies are used to support students’ learning needs, others focus on maintaining social and emotional connections. Hardware such as the robots used in the KlasseContact project in the Netherlands (Ziezon, 2014) allow students to be immersed in the actual classroom in real time. Other projects, such as that by Fels, Samers, and Robertson (2003) trialled the use of much smaller, cheaper and more easily accessible devices (in this case Blackberries®) to maintain social and educational connections between young patients and their friends and teachers at school. The mobility of the Blackberry device was useful for children, because they were confined to bed and could not walk to or sit at a computer. The researchers found that the device was easy for children to use, although concerns were raised over whether such a small device would be too easily lost in the busy hospital ward. At the time of this trial email was also being used by many schools to connect with hospitalised students.
Other researchers have trialled the use of videoconferencing technologies to connect hospital patients with family (Nicholas, Fellner, Koller, Chow, & Brister, 2011; Parsapour et al., 2011) and classroom (Fels & Weiss, 2001; Janssens, Brijs, & Van den Branden, 2010; Weiss, Whiteley, Treviranus, & Fels, 2001). Parsapour and Nicholas studied social connection between patients and their families via videophone, while Weiss studied patients’ use of a robot-like portable videoconferencing system which they remotely controlled to maintain social and educational links with their classroom.
While these studies found that videoconferencing was an effective tool for improving patient connectedness, concerns were raised over the privacy and security of information transmitted in this way. In addition, the researchers recognised the potential risks of children seeing a sick or injured sibling, friend or classmate without being prepared for the medical condition which they might see. There were also particular times when the technology was inappropriate, such as when the child was in distress but the parent was at home, or when the parent was in emotional distress and did not want their child to see them. Technical issues were also identified for the use of high quality audio-visual connections which require high speed internet access at both ends.
Currently in Victoria, hospital and school-based educational support for children includes limited and ad hoc use of technology to connect children to their schools (e.g. via email and teleconferencing) (Wilkie & Jones, 2008). Such connections very often rely on the interest and enthusiasm of the individual classroom teacher in establishing and maintaining the connections, as well as on the persistence and effort of parents in ensuring connections are maintained. Where connection is not maintained, there is a risk that ‘out of sight, out of mind’ may contribute to a disconnection from school for many absent children (Closs, 2000; Hopkins, Green, Henry, Edwards, & Wong, 2013; Hopkins, Moss, Green, & Strong, 2013).
Creating social presence through technology
The idea of social presence is often taken simply as meaning the sense of ‘being there together’ (Schroeder, 2006). When two parties cannot physically ‘be there together’ technology can help users to experience the feeling of social presence.
Media richness theory (Daft & Lengel, 1986) looks at the ability of different types of ICTs to convey not only messages, but information about the person sending the message. This framework ranks face-to-face conversation as the ‘richest’ medium of communication, followed by video communication, then audio communication, and finally typed text (e.g. letter-writing, email or text message) which is considered the ‘leanest’ medium of all.
While ‘rich’ media technologies such as videoconferencing provide an effective medium to convey social presence (Short, Williams, & Christie, 1976), prior research has demonstrated that people do not always need to see or hear each other in order to feel a social connection, and that this is especially true if the people already know each other well (Walther, 1992). Rich media can also have disadvantages in that it can breach privacy and cause disruption (Madell & Muncer, 2007) and may require significant effort to set up and manage (Ames, Go, Kaye, & Spasojevic, 2010). Video communication can also reduce the users’ power to control what information is transmitted about their context and activities and people who are shy, or self-conscious about their appearance may prefer lean media (Goby, 2006). Rich media are typically synchronous and therefore require the users to be simultaneously available, or to interrupt activities, in order to communicate. For these reasons, people sometimes prefer a lean medium even when a richer one is available.
The Presence App uses ambient technology, a type of lean media, to foster social presence while minimising disruption to home, hospital, school and classroom routines. The purpose of ambient technology is to represent information which may be interesting but is not urgently required, in an aesthetically pleasing and unobtrusive manner (Mankoff et al., 2003). Information is often represented visually in an abstract form that invites interpretation. During the design phase of this research, the use of a Presence App to suggest social presence, rather than sustained rich communication, emerged as particularly appropriate for both the classroom and hospital ward setting. This is because both for schools and hospitals, control over information transmission to, from and between children needs to be highly regulated. Schools implement strict regulation over their networked communication to ensure that children in classrooms are not exposed to inappropriate, distressing or decontextualised content which they may not be mature enough to handle. Schools are also required to ensure that inappropriate content is not created or conveyed by students to each other. In this context, such information could include video footage of a child undergoing a medical procedure, or a child transmitting images of themself in an altered state due to their illness or their treatment regime. Children in the classroom may not be prepared for such images, or may see them out of context. There is also a risk that the child in hospital may inadvertently include another patient or health care professional in their footage, potentially breaching the privacy of others. Health care professionals are particularly sensitive to the capture and transmission of health information due to the risks to the privacy of an individual’s health information (which is protected under Victorian legislation) as well as the potential for health information to be misinterpreted or misused.
Presence App
The Presence App was designed to allow patients, their families and classmates to establish a sense of connection with each other, while being sensitive to the particular needs of:
the child (for example not interfering with their privacy and medical care), the school (for example being respectful of privacy and classroom activities), and the family (for example taking into consideration the burden of maintaining a household while caring for a child in hospital).
Trial participants.
The Presence App aimed to support a sense of social presence in the home and classroom for the physically absent child isolated in hospital, as well as conveying to the child the social presence of the family and class with their ongoing structures, individuals and routines. It was designed by researchers and developed with the assistance of a professional app developer.
The Presence App extends the work of a previous project examining the use of an Ambient Orb (Vetere et al., 2012), which successfully demonstrated that ambient technology was effective in maintaining and enhancing social connection between the child in hospital and the classmates at school, as well as establishing a sense of social presence for the absent child. The Ambient Orb (a digitally controlled colour-changing light) was placed in the hospitalised child’s classroom and controlled by the child in hospital. The child in hospital could remotely switch the classroom orb on and off, and change its colour. The Presence App extended this concept of creating social presence through ambient technology by allowing two-way communication, having multiple connections (activity levels, colour and photographs) and using contemporary tablet-based technology, rather than a simple light.
Methodology
The research used a mixed methods approach to data collection. We began with a quantitative survey of parent–child technology use in the hospital, to gather baseline data about connectedness and technologically mediated communication. This was followed up through workshops with a number of project stakeholders, to assess the effectiveness of various possible technological opportunities for connection. The data collected through the workshop process were used to inform the design of the Presence App, to be used on a touch screen tablet. Once the app had been created, a real-world trial was conducted using the app on tablet-based technology with nine 7–12 year old children in hospital, their families and their schools. Qualitative, face-to-face interviews were conducted with each participant (including child, parents, teachers and classmates) both before and after the trial period was conducted, resulting in a rich set of qualitative data.
We designed our technology after a series of workshops that were intended to focus on the concerns and suggestions of these key stakeholders:
Young patients (represented at the workshop by hospital staff) Teachers of young patients Families of young patients
Each workshop comprised three groups of people:
3–4 representatives of the stakeholder group (a, b or c above), 3–4 technology / Human Computer Interaction experts, and 3–4 researchers.
The major findings arising from the workshops can be summarized under the following headings:
Media
High-fidelity media such as video, while considered desirable by some stakeholders, were ruled out by others because of problems concerning privacy, disruption and synchronicity. Staff from schools and health care settings felt that they were too busy for continuous synchronous communication and did not welcome the distraction and disruption of audio and video communication.
The desire of some parents to visualize in real time the medical status of their child was not acceptable to the hospital, who would not risk breaching patient privacy, or indeed alarming parents with data that could be misinterpreted.
Classroom conditions
Teachers were concerned about control in classrooms, and emphasized that both real-time video connections and text-based social media could be a distraction, so that their use would have to be restricted to particular times. Neither the sick child nor the technology could be allowed to become the whole focus of the class. It was necessary that teachers had control over the device, for example, by being able to switch it off when required. It was also emphasized that not every child in the classroom would consider themselves a friend of the patient. Nor did the technology in its current form lend itself to the secondary school setting, in which students were mobile between classrooms for much of the day and numerous teachers would need to be involved.
Asymmetry and conflict
It was noted that many communication scenarios were symmetrical (in principle if not always in reality), with users assumed to have similar communication needs and being provided with the same features. However our design context had different needs and constraints for patients, hospital staff, classmates, teachers and family members.
Whereas the classroom is busy, the patient is more likely to suffer from boredom. Whereas parents want frequent updates about their child’s condition, treatment and state of mind, it is possible that neither the patient nor the hospital would want to provide such updates via technology. It was important for us to design a technology which worked in both directions while still taking account of asymmetry in usage.
Designing the technology
Given the complex set of (sometimes contradictory) desires and constraints conveyed by participants in our workshops, the technology needed to have the following properties:
It should be portable, but not tiny – allowing the technology to be used where it is convenient. It should not use audio or video modalities – to minimise disruption and protect privacy. It should not allow text messages – to minimise disruption and the possibility of inappropriate messages. Children should be able to communicate both with their class at school and with their family. However the classroom and the family do not communicate directly with each other. Nor should the technology afford communication between patients, between classes or between families. Users should be provided with several modalities, from which they could choose the most apt in specific situations.
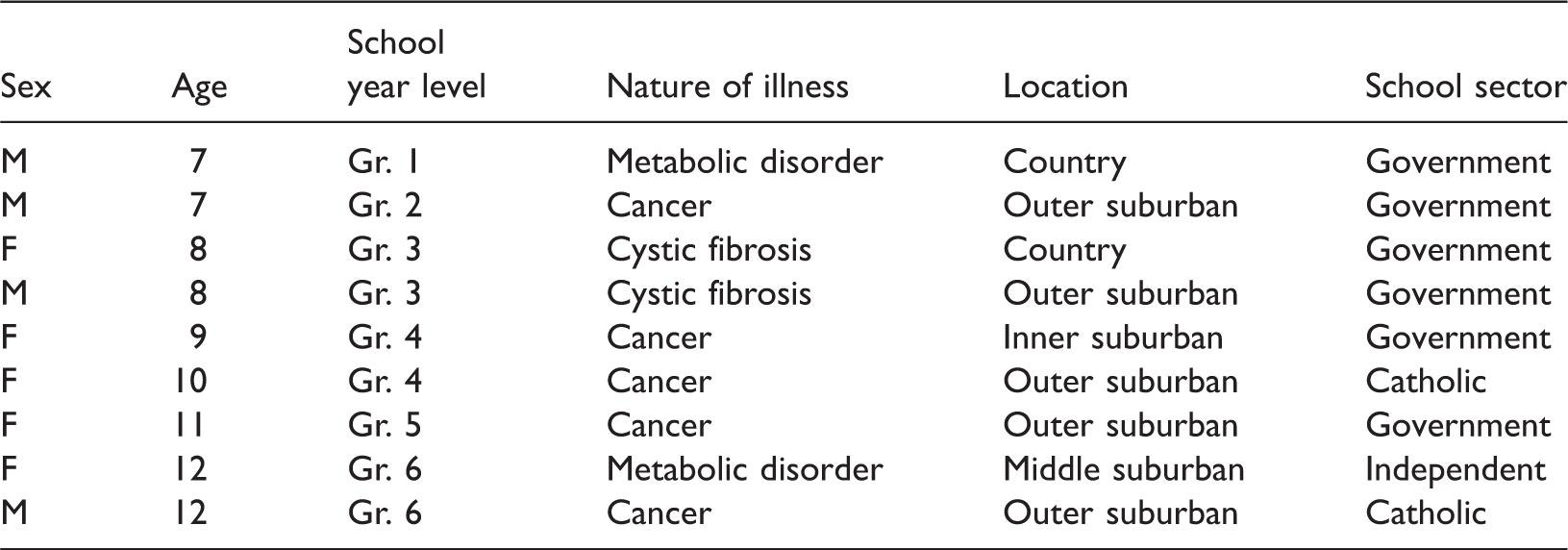
These considerations led us to propose the design of the Presence App as described above. The nine children who participated in the technology trial were all students at Victorian primary schools, in grades 1–6 (aged between 7 and 12 years) who had an expected inpatient stay in hospital of two weeks or more. Each child who participated in the trial had serious or chronic health condition requiring recurrent hospitalisation and periods of absence from school. Students were from inner Melbourne, the outer suburbs of Melbourne and regional Victoria and attended a mixture of government, Catholic and independent schools. Participants were given a tablet computer with the Presence App installed for use during the trial. A second tablet, also running the Presence App, was provided to each child’s usual school teacher for use in the classroom during the child’s absence. The families of students who participated were also offered the opportunity to trial the tablet at home, although only four homes participated in this way. Two children did not complete the trial because they were discharged from hospital earlier than anticipated. They were able to use the Presence App for a short time and provide feedback. The remaining seven participants used the Presence App for periods varying between two weeks and one month (Table 1).
Semi-structured face-to-face interviews were conducted with each participant (including child, parents, teachers and classmates) both before and after the trial period (see Appendix 1), resulting in a rich set of qualitative data. Photographic data and usage statistics were also analysed to add depth to the interview data, as well as providing objective evidence of usage patterns and preferences, supplementing the subjectively recorded responses of participants.
The data were analysed in three ways (Denzin and Lincoln, 2005; Graneheim & Lundman, 2004). First, data were collated from the various participants as triads of child, parent and school, coalescing into a rich case study centred around each child. By pulling all the data sets together in a child-centred way, we were able to establish a thorough picture of how each child connected via the Presence App with their family members, teachers and classmates. Secondly, a thematic analysis was conducted on the case studies to identify common themes emerging from the data. Research team members divided the case studies up and independently coded the responses. This inductive coding was then analysed to draw out pertinent themes. The whole research team then met together to compare and collate themes and assess the most important/commonly occurring (Miles & Huberman, 1994; Patton, 2002). Finally, a site analysis was performed, using the data grouped by user location (hospital, school, home) rather than in triads around the child. The results of the trial in each setting were very different and this site analysis allowed us to examine differences specific to the needs of users in each location.
Findings
While a large number of themes were identified, this paper reports in particular on those concerning the use of our technology to keep children and young people connected to their peers and their educational journey. As discussed below, the ambient technology was more successfully employed in the hospital setting and the school setting than in the home.
School and home contexts
It was clear from our research that ambient technology was well suited to the classroom setting, where its lean communication affordances, low bandwidth and unobtrusive design worked well with the visibility, privacy and distraction constraints of a busy classroom. This contrasted with the use of the same technology in the home, where parents and siblings found the use of the app ‘limited’ and insufficient to meet their very high needs for connection, information sharing and regular communication with the child in hospital. In fact, in many cases the parent or family hardly used the device, since they were always or almost always present in the hospital with their child. In addition, families in this trial were well connected via a variety of devices, using mobile telephones, landlines, portable computers and tablets to link the hospitalised child with parents, siblings and other extended family members (Heidari, 2013). We conclude that despite parent interest in having an additional means of communication with their child, in practice the use of ambient technology did not effectively meet the needs of families.
In contrast, the technology was embraced in classroom settings. The main themes which emerged in the context of the primary school classroom were:
Balancing teacher control with classmate control of device, maintaining social connections, and maintaining academic connections / connections to learning.
Teacher control of the device
In particular, we found that individual teachers were a significant influence on the way the technology was received, incorporated, utilised or ignored in the classroom setting. In this trial, the tablet was most extensively and effectively used in classrooms where the teacher and to some extent the child’s friends were already highly motivated to maintain connections between the hospitalised child and the school. The Presence App was found to complement the range of other communication strategies being enacted to connect with the hospitalised child in these instances. While students and teachers were very enthusiastic about rich media ICTs such as video and audio connections, teachers in particular were mindful of certain times in the hospitalised child’s medical care where rich media communication might be inappropriate or overtaxing for the hospitalised child. Teachers were also aware of the potential disruption to classroom routines caused by direct communication methods. They usually implemented strict controls around the use of technologies such as email and Skype™, for example, setting aside a particular time of the day during which communication could occur (often just before lunch, or just before the end of the school day), or setting rules for the types of conversations which could occur.
Although the Presence App was designed to be suitable for students to have free access to in the classroom, we found that teachers managed their class’s use of the tablet in several ways. In some classes the teacher was in charge of the tablet’s use. Oh, well normally if you wanted to change a colour we had to ask [teacher’s name]. (Classmate) Generally in the mornings I would say, ‘What colour would you like to change?’, or if somebody was working well I’d say, ‘Would you like to change the background colour?’. Or if we noticed that [child’s name] had changed the colour of his balls [blobs], we might change the colour of the background. (Teacher)
In other schools, teachers accepted the tablet reluctantly upon request by the parent or the child. Such teachers expressed opinions such as the need for the absent child to focus on their health care, with a belief that education could ‘wait’ until the child returned to school. While such beliefs may stem from a consideration of the stress families are under when their child is ill, and a reluctance to burden the child or family with school work, research shows that keeping up with their school work even during periods of ill health is critical for the wellbeing both of children with health conditions and their families (Jackson, 2013). In cases where classroom teachers held these kinds of beliefs, the use of the tablet tended to fall on the students, who were enthusiastic about using it even when the teacher was less enthusiastic. In these cases, however, the use of the tablet tended to drop off after a while as the novelty value fades, as is often the case in technology trials (Salomon, 1990).
Connection for socialising
A key design aim for this technology was to enhance the social connectedness that hospitalised children enjoy with classmates and family. It was clear from our pre-trial interviews that disconnection from peers was a major issue for children who missed large amounts of school. He’s talked about them[his school friends] a few times, and like if a game comes “Aw so and so at school, he plays this game”, … and then you can see that he sort of misses that … (Parent) I know she doesn’t like it [being in hospital], and she wants to come back to school. I know the very first time that she was allowed home she was very excited and asked the doctor if she could come back to school to visit and he said, no, so she was pretty upset by that, said, I just want to come back. (Parent) When [child’s name] sent us something it was good because it made us think that she was thinking of us. (Teacher) It felt like we were more connected to her. (Classmate) Well, yeah, yes because when like I looked at it ‘cause when I would look down and see it I felt like, oh, I wonder what [child’s name]’s doing right now? (Classmate) I’m sad about like ‘cause now we can’t really connect to [child’s name], we can’t… she can’t connect to us. (Classmate)
It should be noted that while some (but not all) of the students in our trial also used other technological means to connect with their classmates and teachers, the findings presented here represent their reflections on the Presence App and the tablet, which we hoped would complement, and perhaps stimulate, the use of more information rich media as and when appropriate for both the class at school and the child in hospital.
Connection for learning
One can envisage two kinds of mediated connection for hospitalised children: a connection to social life and a connection to learning. The primary aim of this technology was social connection, as described above, and connection to the school and classroom environment, rather than curriculum content. The ambient nature of our technology does not directly address teaching support and only indirectly supports learning through solidifying social connection to school. A range of off-the-shelf technology solutions such as videoconferencing are currently being trialled in many out-of-school settings to allow absent students participate in regular classes (Ziezon, 2014), ensuring that absence from school does not mean missed classes. While we recognise the effectiveness of such tools in particular settings, we also found that often in our context, such tools were inappropriate. We also posit that the investment in technology hardware currently required is unlikely to be accessible to the majority of Australian schools. Our app therefore focussed on facilitating social connections rather than supporting direct teaching and learning. Nonetheless, some schools did use the Presence App to connect the hospitalised child to education processes, in particular through photo-sharing. This was particularly evident in one case where the child’s connection to social life and peers was already constrained.
Several teachers used photo-sharing to convey educational activities that were occurring in class to the child in hospital. We took it to specialist classes with them and then sent photos from what they were doing, then we sent one of them cleaning the table but some of the girls went at the end of the art session and they sent photos of that. And we wrote some messages too. (Teacher) I took a photo of [name] and [name] writing in their ‘special writers’ note books, and I said, ‘[name] and [name] are writing in their ‘special writers’ notebooks’, like explanatory messages. (Teacher) Interviewer: And what sort of photos did you take with it? Classmate: Just like the class in action, sort of thing. Interviewer: So what sort of actions? Classmate: Like working and just sometimes we all got together for a photo. You’ll see lots of photos with pads and tampons and we had to estimate how much each pad and tampon would hold … So it was a maths task, but it was also part of our growth and development. (Teacher) We took more whole group things. I guess that when we were doing an event or something was happening, so that she didn’t miss out on it we’d take a photo. (Teacher) So things that she was missing out on, to try and give her an insight what was happening when she wasn’t here, we would take a photo and send it to her. (Teacher)
Two of the hospitalised children reported becoming more aware of classroom activity via the moving-dots ambient activity display. Usually when they’re loud it’s probably at art time. (Child) Interviewer: And so when the balls are moving slowly, what do you think is happening? Child: Um, it’s probably quiet reading time because it’s not loud and everything.
Discussion – Implications of using ambient technology to keep students connected to school
In this project, we attempted to design a technology for promoting awareness and connectedness which was specifically suited to the hospital and classroom contexts. We are aware only of a few existing technologies that are designed explicitly for this context (e.g. Parsapour et al., 2011; Weiss et al., 2001). There is, however, an increasingly large range of off-the-shelf communication mobile Internet-based technologies such as laptops, tablets and smart-phones. We found evidence that families and schools were making significant use of commercially-available communication technologies in order to solve the problem of maintaining connection with a hospitalised child. We do not regard this finding as precluding the need for technology explicitly designed for this context. On the contrary, the fairly extensive use made of off-the-shelf technologies by our participants indicates a willingness to establish mediated connection with hospitalised children via a variety of modes. Furthermore, our discovery during the design workshops that teachers fear problems of classroom disruption while hospital staff share similar concerns around privacy and transmission of inappropriate information when using off-the-shelf technologies suggests a need for a design that better suits this context. Similar recent research using videoconferencing technology to connect paediatric cancer patients with their schools encountered this very resistance in the hospital setting (Ellis et al., 2013), demonstrating the limitations of using information-rich technologies in this setting.
The very specific constraints in both hospital and classroom settings for privacy, control over information and disruption to other routines render many existing rich communication technologies less than ideal. Previous research into the use of videoconferencing to connect hospital patients with family and classroom (Fels & Weiss, 2001; Nicholas et al., 2011; Parsapour et al., 2011; Weiss et al., 2001) has outlined a number of considerations when using video in these contexts such as the privacy and security of information transmitted (particularly if the video link was left on unintentionally), the risks of children seeing confronting images of sick or injured siblings or classmates and technical issues stemming from the requirement of high speed internet access at both ends.
Our research has demonstrated that a low bandwidth, low information but engaging ambient technology on a tablet computer can facilitate the creation of a sense of social presence (Schroeder, 2006; Walther, 1992) and assist in maintaining a sense of connection to both the social and academic environment of the classroom. While the use of ambient technology was insufficient for communication between the hospitalised child and their family at home, it was ideal for the more institutionally constrained connections required between the hospital and the school.
As schools and classrooms make increasing use of ubiquitous technologies, a Presence App which could run on the corner of an interactive whiteboard in a child’s classroom, making use of existing bandwidth and school-based resources, would be a feasible development for schools and other learning settings, such as kindergartens and alternative settings. Unlike many other proprietary communication tools, the app does not demand focal attention, it is constantly on, and offers a sense of presence without the need for explicit verbal interactions or video connection. A downloadable app, with a simple and engaging user interface limits the need for dedicated hardware, expensive, high end user support, extensive training or separate, independent installation and set-up, all of which would likely prove prohibitive both to schools and to hospitals.
In this trial the Presence App was most effectively used in classrooms where the teacher was highly motivated to keep the hospitalised child connected to the classroom and were already using other modes of communication. In these instances, the Presence App was seen to complement existing communication strategies. The Presence App was found to establish stronger connections in some cases where there was little existing connection to the school, by prompting the teacher to connect with the hospitalised child. Although the Presence App was designed to be suitable for students to have free access to in the classroom, in most cases the teacher managed their class’s use of the tablet.
Limitations of this study/recommendations for future study
This research focused on children in primary school, who, for practical reasons, proved to be the best population for this trial. In secondary school (grades 7–12 in Victoria) adolescent demands for social contact with peers and friends become even more urgent, and the possibility of disconnection from education concomitantly rises. The nature of secondary education, where students move around to different classrooms and are taught by multiple teachers precluded their inclusion in this trial, however many secondary school students now carry smart-phones or tablets and this offers tantalising new possibilities to engage adolescents in peer-mediated connections to school, rather than or in addition to, institutionally controlled connections through teachers and classrooms. Future work could build on this project by incorporating the use of a Presence App into existing secondary school classroom technology, moving seamlessly between network enabled classrooms across the school as the hospitalised student’s individual timetable requires. Future work could also focus on the connection needs of younger children, in pre-school and kindergarten, whose social relationships and peer friendships are just beginning to form.
Our sample was too small for us to detect differences between school settings, across the government, Catholic and independent sectors, however this is another area which could be further explored in future work, as differences in schools’ and pupils’ IT resources and institutional restrictions may have an impact on the ways in which technology may best be utilised.
More work is also needed which will focus more closely on the impact of the game-like environment of broadband enabled apps, building engagement and rapport between physically separated students through joint immersion in virtual educational games and online social learning. This is an area of burgeoning research which could be usefully harnessed to meet the needs of vulnerable students absent from school due to a health condition. It is clear, however, that utilising the affordances of mobile technologies to connect absent students with their classrooms can be a highly effective means of overcoming technical, institutional and personal barriers to staying engaged with school during hospitalisation.
The Presence App.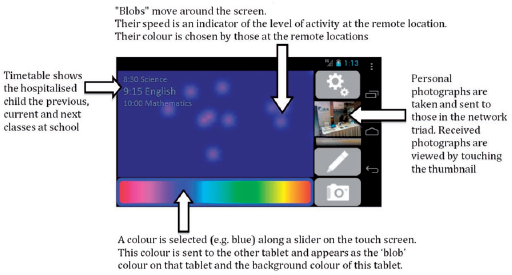
Conclusion
Keeping children connected to school and learning during absence for health care is of critical importance in ensuring these children do not prematurely disengage from their expected educational journeys. Research in a number of diverse contexts has consistently demonstrated that lean media, such as our presence App, can provide useful, ongoing social connections without associated issues of distraction and inappropriate transmission of information. This is a significant consideration for communication technologies used in the sensitive contexts of both hospital and home. Our project has developed and demonstrated a simple app which helps to keep children connected to school and learning despite absence due to hospitalisation. The trial of the app builds on previous research findings and demonstrates that technological mediated communication can meet the needs of children in hospital for social connection to their classroom, while at the same time taking account of the very specific needs of both hospital and classroom settings for minimising risk, protecting privacy and reducing potential disruption to both health care and classroom learning.
Footnotes
Acknowledgements
The authors would like to acknowledge the participation in this research by all the students, families, teachers and classmates, at a time of heightened stress and uncertainty. The project could not have gone ahead without them. We thank Tsharni Zazryn, Courtney Hempton and Lars Kulik for their help in conducting this research.
Declaration of conflicting interests
None declared.
Funding
The authors gratefully acknowledge financial support from Telematics Trust, the Institute for a Broadband Enabled Society at the University of Melbourne, and the Department of Education and Early Childhood Development (Victoria). The Royal Children’s Hospital Education Institute is funded by the Victorian Department of Education and Early Childhood Development. We thank Huawei Australia for providing tablet computers. Our funding sources and supporters had no role in designing the study, the collection, analysis and interpretation of data, the writing of the report, nor the decision to submit the article for publication.