
Abstract
Introduction:
People diagnosed with borderline personality disorder experience persistent functional impairment despite current evidence-based treatment. Domains of daily living functioning, such as establishing a routine, household management and self-care, can be important goals for rehabilitation. This review aimed to scope and synthesise programmes that address the daily living functioning of people diagnosed with borderline personality disorder.
Methods:
This review followed the PRISMA Extension for Scoping Reviews Checklist and the Joanna Briggs Institute scoping review methodological guidance. Eight databases (Medline, PsycINFO, ASSIA, CINAHL, Embase, Emcare, ProQuest Dissertations & Theses Global and Scopus) and grey literature were searched.
Results:
Forty-four records were found spanning 12 countries, from 1987 to 2025, comprising research studies, educational materials and programme summaries. Programmes included independent living skills development, residential facilities, outpatient treatment and occupational therapy, with rehabilitation and recovery the most frequently used approaches. The domains of daily living functioning were health (n = 189), relational (n = 84), responsibility (n = 67), personal (n = 61), leisure (n = 53), routine (n = 42) and household (n = 30). Measures used to describe changes in functioning varied considerably.
Conclusions:
Programmes supporting the daily living functioning of people diagnosed with borderline personality disorder exist. However, the evidence base is currently disparate. No single programme addressed all identified domains of daily living functioning. Comprehensive, evidence-based rehabilitation programmes addressing all domains of daily living functioning are needed to enable functional recovery for people diagnosed with borderline personality disorder.
Keywords
Introduction
Borderline personality disorder (BPD) is a severe mental illness characterised by intense and unstable relationships, distorted sense of self, emotional dysregulation and impulsivity (American Psychiatric Association, 2013). Self-harm and suicidality are hallmark features (Lak et al., 2025). People diagnosed with BPD are prevalent in psychiatric settings (Zimmerman et al., 2005) and frequently seek support from emergency and mental health services during periods of crisis (Warrender et al., 2020).
BPD is complex and challenging to treat. Medications can manage some symptoms, but they do not lessen the severity of the disorder (Gartlehner et al., 2021; Stoffers-Winterling et al., 2022). Clinical practice guidelines currently recommend psychotherapy as the primary treatment for BPD (Aslam et al., 2025). However, only 50% of people who receive evidence-based psychotherapy respond to treatment (Woodbridge et al., 2022). Long-term functional impairment remains a significant problem (Álvarez-Tomás et al., 2019; Choi-Kain et al., 2020). Persistent challenges in functional recovery manifest as disability benefits (Kramer et al., 2023) and prolonged psychotherapy (Zanarini et al., 2004). From patient perspectives, increased support is needed to develop practical skills and participate more meaningfully in daily activities (Katsakou and Pistrang, 2018; Woodbridge et al., 2023).
Research into the functioning of people diagnosed with BPD currently focuses on symptomatic remission, having one emotionally sustaining relationship (relational functioning) and full-time work or study (vocational functioning) (Grenyer et al., 2022; Zanarini et al., 2010a, 2018). The complexity of functioning is reduced to a single score on the Global Assessment of Functioning (GAF) (Endicott et al., 1976; Gold, 2014). Relational and vocational domains have been synthesised elsewhere (Di Bartolomeo et al., 2024; Kernot et al., 2023; Lazarus et al., 2014; Sinnaeve et al., 2015; Steele et al., 2019). However, this work has not captured the multi-faceted nature of daily living functioning, and more attention to other domains is required. Daily living functioning refers to activities and routines in daily life, such as household management, financial responsibilities, leisure pursuits and self-care.
The literature that describes programmes addressing other domains of daily living functioning remains disparate, yet these programmes may provide important rehabilitation support and enable functional recovery. Therefore, the aim of this review was to scope and synthesise such programmes. The review question was, ‘What programs are available to support people diagnosed with BPD to address their daily living functioning?’
Methods
This review followed Arksey and O’Malley’s (2005) framework for scoping reviews, the PRISMA Extension for Scoping Reviews (PRISMA-ScR) Checklist (Tricco et al., 2018) and the Joanna Briggs Institute (JBI) methodological guidance (Peters et al., 2020). The protocol was pre-registered on the Open Science Framework (https://osf.io/h87ea/).
Inclusion criteria
The population for this review was ‘people diagnosed with BPD’, the concept was ‘daily living functioning’, and the context was ‘programmes’ (with no restrictions on settings). A BPD diagnosis was based on self-report, formal research methods or a health professional’s assessment (using Diagnostic and Statistical Manual of Mental Disorders [DSM] or International Classification of Diseases [ICD] frameworks). Records describing programmes addressing daily living functioning for people diagnosed with BPD aged 16+ were included. Programs could be structured and facilitator-led or self-management resources. Grey literature and relevant secondary research articles were also included, with the latter set aside for citation searching. There were no date or language restrictions in the database search, with Google Translate used for non-English records. Programmes based on established psychotherapies were included if they specifically addressed domains beyond relational or vocational functioning. All comorbidities were included, provided the programme involved at least one person diagnosed with BPD. Records that focused on mental illness without mention of BPD were excluded, as were programmes that only addressed relational or vocational functioning.
Record sources
Eight databases were searched: Medline, PsycINFO, ASSIA, CINAHL, Embase, Emcare, ProQuest Dissertations & Theses Global and Scopus. For grey literature, Google and Google Scholar were searched alongside BPD organisation websites internationally. These organisations were also contacted directly to identify any additional relevant programmes.
Search strategy
Search terms were developed with support from an academic librarian and informed by the domains of daily living functioning outlined by Desrosiers et al. (2017), including activities and routines in daily life such as self-care, health, household, financial, time management and leisure. Supplementary File 1 contains the complete search terms for all databases and the grey literature search strategy, with all searches conducted on the same day by the first reviewer. Medline was used to test and refine the final search strategy. Citation searching was conducted using the reference lists of included records and the ‘cited by’ function in Google Scholar was used to locate new records.
Record screening and selection
Records retrieved from the search strategy on 5 August 2025 were initially uploaded into Endnote (Clarivate, 2024) and then transferred into Covidence (Veritas Health Innovation, 2024) for duplicate removal. Two reviewers independently screened titles and abstracts in Covidence, followed by full-text screening. An independent third reviewer resolved discrepancies.
Data extraction and synthesis
Characteristics of the included records (author, year, country and aim), programme details (aim, approach, facilitator and setting) and measures used to describe changes in functioning were extracted into Excel. All extraction was completed by the first reviewer, with a second reviewer independently checking the extraction of 15% of the included records to ensure relevancy and accuracy. A third reviewer resolved disagreements. Domains of daily living functioning (health, relational, responsibility, personal, leisure, routine and household) were synthesised based on Desrosiers et al.’s (2017) assessment tool. The domains of daily living functioning addressed by programmes were coded using conventional content analysis (Hsieh and Shannon, 2005), using frequency counts of content. The measures used to describe changes in functioning within the quantitative studies were collated and critiqued for reliability and validity. The Excel worksheets were then converted into tables, with regular team discussions at all stages of the process.
Results
A flowchart of the search and screening results is available in Figure 1. The database search identified 2,309 records for title and abstract screening, from which 2,184 were excluded. There were 125 full-text records, from which 22 were included. An additional 22 records were identified via other search methods, leading to 44 inclusions overall.
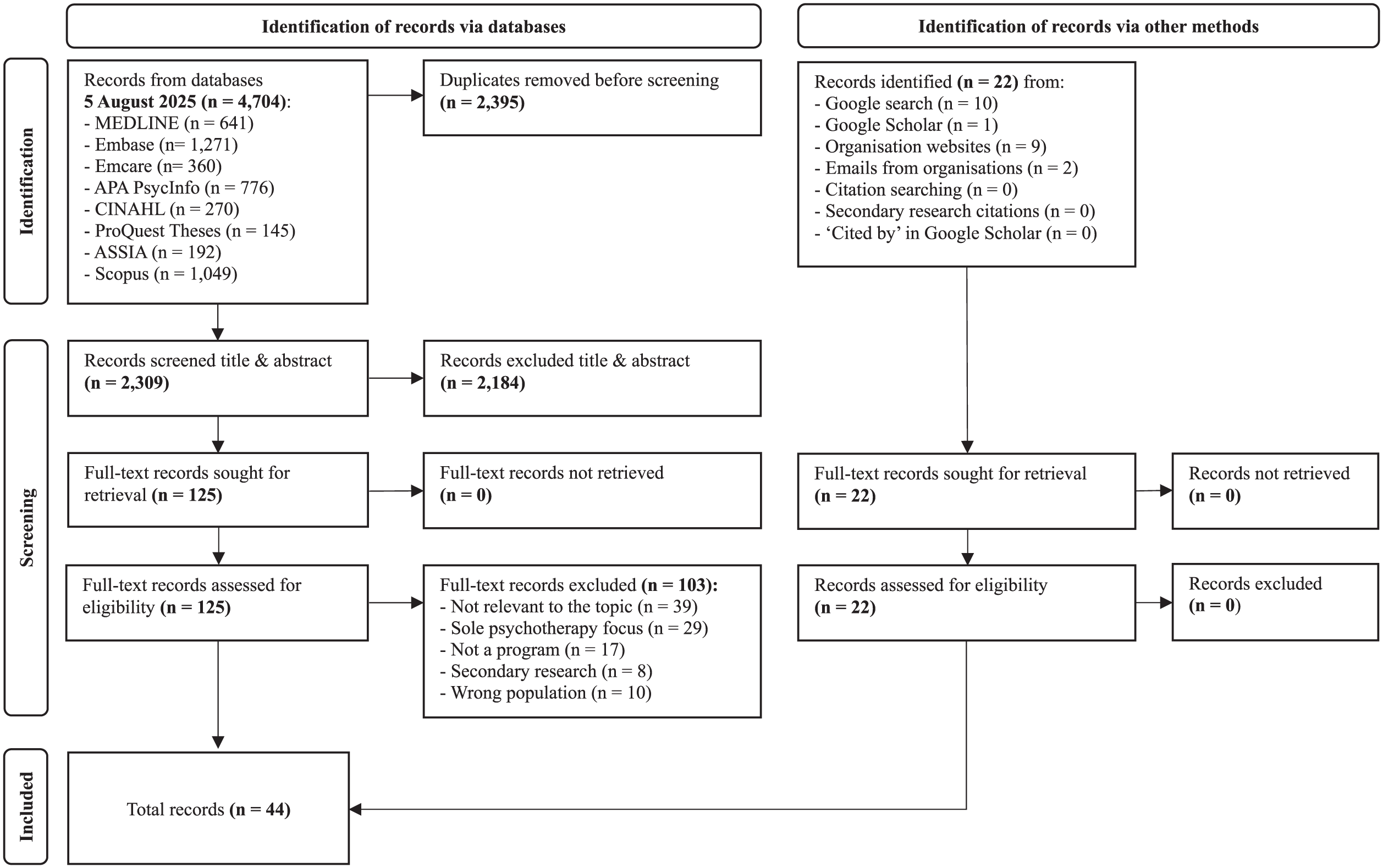
Flowchart of search and screening results.
Record characteristics
The characteristics of the 44 included records are outlined in Table 1. The records dated from 1987 and spanned across 12 countries, with the highest representation from Australia and New Zealand (Borderline in the ACT, 2025; Department of Health and Aged Care, 2024; Healthtalk Australia, 2025; Lee et al., 2014; National Disability Insurance Scheme [NDIS], 2025; Orygen, 2024; Project Air, 2018, 2020; Royal Australian & New Zealand College of Psychiatrists [RANZCP], 2017; Sane, 2022; Scanlan et al., 2017; Sekharan et al., 2021) and the United States (Brogan et al., 2020; Emotions Matter, 2020; John Hopkins Medicine, 2025; Life Adjustment Team, 2025; McAlpine, 1991; McLean Hospital, 2024; Mehl, 1997; National Alliance on Mental Illness [NAMI], 2017; Nelson and Condrin, 1987; Pacific Teen Treatment, 2024; Tomasi et al., 2019; verywell mind, 2023), with 12 records each, followed by the United Kingdom (Clark et al., 2006; Lamont et al., 2017; Lee and Harris, 2010; Mind, 2022; National Health Service [NHS], 2022; Priory, 2025; Rehab 4 Addiction, 2025), Spain (Gabarda-Blasco et al., 2024; Ortega, 2004; Torres-Soto et al., 2021), Canada (Oke and Kanigsberg, 1991; St-Amour et al., 2024), Sweden (Enoksson et al., 2021; Helleman et al., 2018), Germany (Sayk et al., 2025), Iran (Soleimani et al., 2024), Italy (De Girolamo et al., 2024), Netherlands (Helleman et al., 2014), Portugal (Lima, 2008) and Switzerland (Bromundt et al., 2013).
Record characteristics.
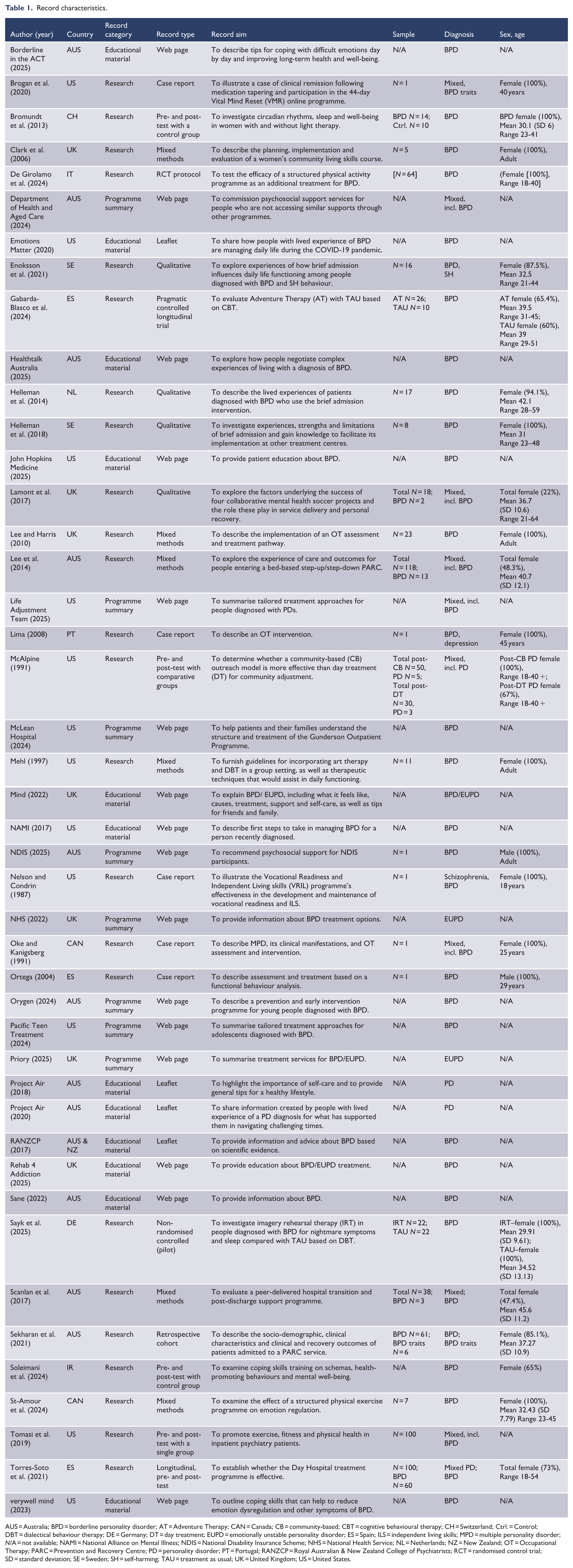
AUS = Australia; BPD = borderline personality disorder; AT = Adventure Therapy; CAN = Canada; CB = community-based; CBT = cognitive behavioural therapy; CH = Switzerland; Ctrl. = Control; DBT = dialectical behaviour therapy; DE = Germany; DT = day treatment; EUPD = emotionally unstable personality disorder; ES = Spain; ILS = independent living skills; MPD = multiple personality disorder; N/A = not available; NAMI = National Alliance on Mental Illness; NDIS = National Disability Insurance Scheme; NHS = National Health Service; NL = Netherlands; NZ = New Zealand; OT = Occupational Therapy; PARC = Prevention and Recovery Centre; PD = personality disorder; PT = Portugal; RANZCP = Royal Australian & New Zealand College of Psychiatrists; RCT = randomised control trial; SD = standard deviation; SE = Sweden; SH = self-harming; TAU = treatment as usual; UK = United Kingdom; US = United States.
There were three types of records: research, educational materials and programme summaries. The research records were controlled studies (Bromundt et al., 2013; De Girolamo et al., 2024; Gabarda-Blasco et al., 2024; McAlpine, 1991; Sayk et al., 2025; Sekharan et al., 2021; Soleimani et al., 2024), mixed methods (Clark et al., 2006; Lee et al., 2014; Lee and Harris, 2010; Mehl, 1997; Scanlan et al., 2017; St-Amour et al., 2024), descriptive studies (Brogan et al., 2020; Lima, 2008; Nelson and Condrin, 1987; Oke and Kanigsberg, 1991; Ortega, 2004), qualitative studies (Enoksson et al., 2021; Helleman et al., 2014, 2018; Lamont et al., 2017) and uncontrolled studies (Tomasi et al., 2019; Torres-Soto et al., 2021). The educational materials were web pages (Borderline in the ACT, 2025; Healthtalk Australia, 2025; John Hopkins Medicine, 2025; Mind, 2022; NAMI, 2017; Rehab 4 Addiction, 2025; Sane, 2022; verywell mind, 2023) and leaflets (Emotions Matter, 2020; Project Air, 2018, 2020; RANZCP, 2017). The programme summaries were web pages (Department of Health and Aged Care, 2024; Life Adjustment Team, 2025; McLean Hospital, 2024; NDIS, 2025; Orygen, 2024; Pacific Teen Treatment, 2024; Priory, 2025).
The BPD diagnosis sample size (n = 340) was derived from records describing people with the diagnosis only (Brogan et al., 2020; Clark et al., 2006; Enoksson et al., 2021; Gabarda-Blasco et al., 2024; Helleman et al., 2014, 2018; Lee and Harris, 2010; Lima, 2008; Mehl, 1997; NDIS, 2025; Nelson and Condrin, 1987; Oke and Kanigsberg, 1991; Ortega, 2004; Sayk et al., 2025; Sekharan et al., 2021; St-Amour et al., 2024) or records that reported the cohort separately (Bromundt et al., 2013; Lamont et al., 2017; Lee et al., 2014; McAlpine, 1991; Scanlan et al., 2017; Torres-Soto et al., 2021). This BPD diagnosis sample excludes the educational materials (outlined above), one record that did not report the cohort separately (Tomasi et al., 2019) and one record outlining a study protocol (De Girolamo et al., 2024). The sex distribution of the BPD diagnosis sample was 84% female and 16% male, calculated either from direct reporting (Brogan et al., 2020; Bromundt et al., 2013; Clark et al., 2006; Enoksson et al., 2021; Gabarda-Blasco et al., 2024; Helleman et al., 2014, 2018; Lee and Harris, 2010; Lima, 2008; McAlpine, 1991; Mehl, 1997; NDIS, 2025; Nelson and Condrin, 1987; Oke and Kanigsberg, 1991; Ortega, 2004; Sayk et al., 2025; Sekharan et al., 2021; St-Amour et al., 2024) or conservatively estimated using whole-sample proportions applied to the BPD diagnosis subset (Lamont et al., 2017; Lee et al., 2014; Scanlan et al., 2017; Torres-Soto et al., 2021). The age range of the participants in the directly reported BPD diagnosis sample was 18 to 59 years.
Programme aims, setting and structure
Programme aims
Thirty-two records described 34 facilitator-led programmes that addressed daily living functioning, as outlined in Table 2. The educational materials were removed from this table because they lacked a programme structure and facilitator. Programmes addressed daily living functioning through independent living skills development (Clark et al., 2006; Department of Health and Aged Care, 2024; Life Adjustment Team, 2025; McAlpine, 1991; NDIS, 2025; Nelson and Condrin, 1987), exercise and nutrition (De Girolamo et al., 2024; Lamont et al., 2017; St-Amour et al., 2024; Tomasi et al., 2019), residential facilities (Lee et al., 2014; NHS, 2022; Pacific Teen Treatment, 2024; Priory, 2025; Sekharan et al., 2021), brief admission to hospital (Enoksson et al., 2021; Helleman et al., 2014, 2018), outpatient treatment (McLean Hospital, 2024; Priory, 2025; Torres-Soto et al., 2021), occupational therapy (Lee and Harris, 2010; Lima, 2008; Oke and Kanigsberg, 1991), adventure-based therapy (Gabarda-Blasco et al., 2024), art therapy (Mehl, 1997), coping skills (Soleimani et al., 2024), early intervention (Orygen, 2024), functional behaviour analysis (Ortega, 2004), imagery rehearsal therapy (Sayk et al., 2025), light therapy (Bromundt et al., 2013), promotion of lifestyle changes (Brogan et al., 2020) and transition from hospital to home (Scanlan et al., 2017).
Aims and structure of programmes.
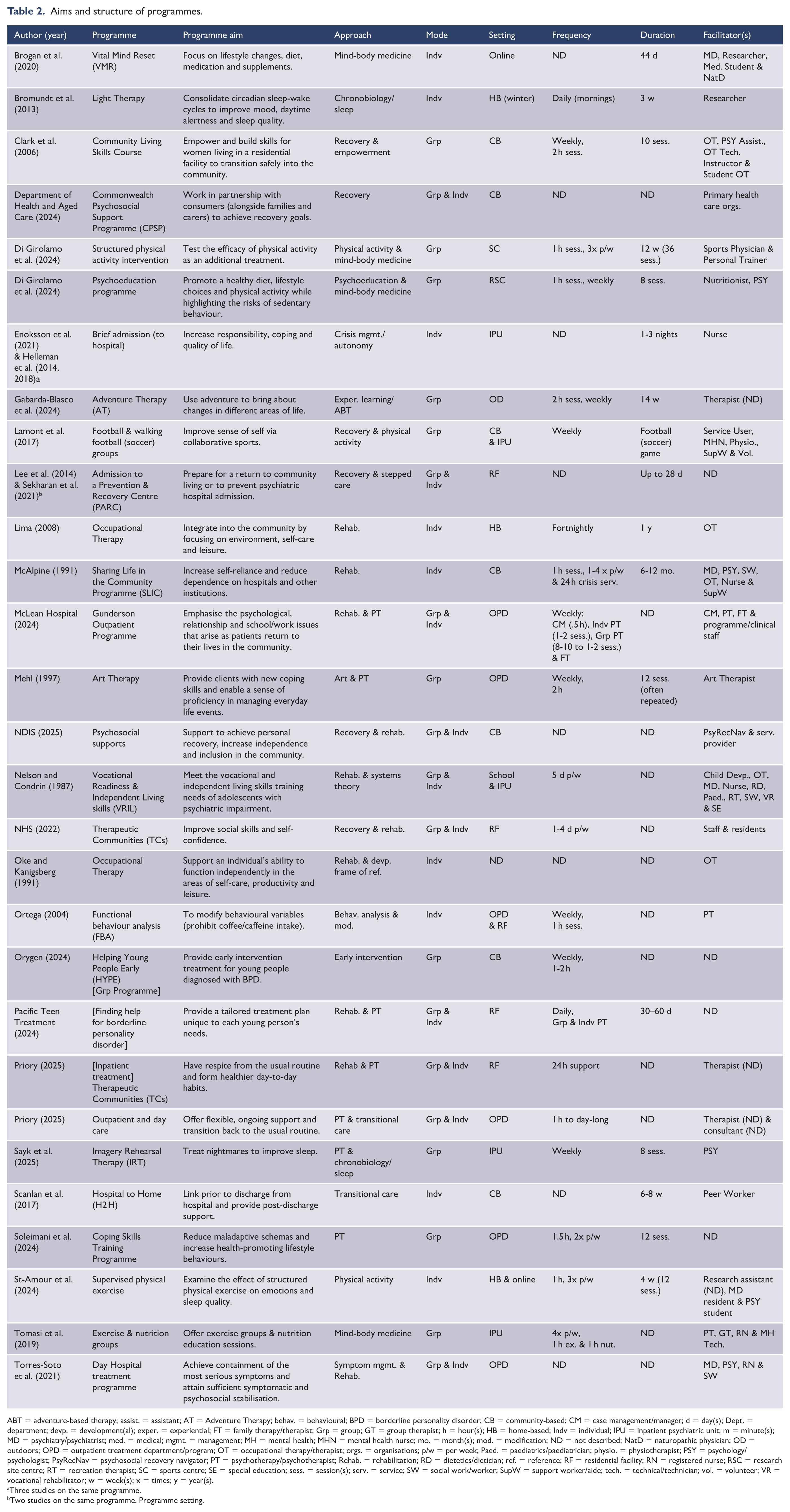
ABT = adventure-based therapy; assist. = assistant; AT = Adventure Therapy; behav. = behavioural; BPD = borderline personality disorder; CB = community-based; CM = case management/manager; d = day(s); Dept. = department; devp. = development(al); exper. = experiential; FT = family therapy/therapist; Grp = group; GT = group therapist; h = hour(s); HB = home-based; Indv = individual; IPU = inpatient psychiatric unit; m = minute(s); MD = psychiatry/psychiatrist; med. = medical; mgmt. = management; MH = mental health; MHN = mental health nurse; mo. = month(s); mod. = modification; ND = not described; NatD = naturopathic physician; OD = outdoors; OPD = outpatient treatment department/program; OT = occupational therapy/therapist; orgs. = organisations; p/w = per week; Paed. = paediatrics/paediatrician; physio. = physiotherapist; PSY = psychology/psychologist; PsyRecNav = psychosocial recovery navigator; PT = psychotherapy/psychotherapist; Rehab. = rehabilitation; RD = dietetics/dietician; ref. = reference; RF = residential facility; RN = registered nurse; RSC = research site centre; RT = recreation therapist; SC = sports centre; SE = special education; sess. = session(s); serv. = service; SW = social work/worker; SupW = support worker/aide; tech. = technical/technician; vol. = volunteer; VR = vocational rehabilitator; w = week(s); x = times; y = year(s).
Three studies on the same programme.
Two studies on the same programme. Programme setting.
Programmes were delivered in the community (Clark et al., 2006; Department of Health and Aged Care, 2024; Lamont et al., 2017; McAlpine, 1991; NDIS, 2025; Orygen, 2024; Scanlan et al., 2017), inpatient units (Enoksson et al., 2021; Helleman et al., 2014, 2018; Lamont et al., 2017; Lee and Harris, 2010; Sayk et al., 2025; Tomasi et al., 2019), outpatient treatment centres (McLean Hospital, 2024; Mehl, 1997; Ortega, 2004; Priory, 2025; Soleimani et al., 2024; Torres-Soto et al., 2021), residential facilities (Lee et al., 2014; NHS, 2022; Pacific Teen Treatment, 2024; Priory, 2025; Sekharan et al., 2021), at home (Bromundt et al., 2013; Life Adjustment Team, 2025; Lima, 2008; St-Amour et al., 2024), online (Brogan et al., 2020; St-Amour et al., 2024), research facilities (De Girolamo et al., 2024), special schools (Nelson and Condrin, 1987), sports centres (De Girolamo et al., 2024) and outdoors (Gabarda-Blasco et al., 2024). One record did not describe the programme setting (Oke and Kanigsberg, 1991).
Programme structure
Programmes were implemented individually (Brogan et al., 2020; Bromundt et al., 2013; Enoksson et al., 2021; Helleman et al., 2014, 2018; Life Adjustment Team, 2025; Lima, 2008; McAlpine, 1991; Oke and Kanigsberg, 1991; Ortega, 2004; Scanlan et al., 2017; St-Amour et al., 2024) and in groups (Clark et al., 2006; De Girolamo et al., 2024; Gabarda-Blasco et al., 2024; Lamont et al., 2017; Lee and Harris, 2010; Mehl, 1997; Orygen, 2024; Sayk et al., 2025; Soleimani et al., 2024; Tomasi et al., 2019). Programmes also combined individual and group components (Department of Health and Aged Care, 2024; Lee et al., 2014; McLean Hospital, 2024; NDIS, 2025; Nelson and Condrin, 1987; NHS, 2022; Pacific Teen Treatment, 2024; Priory, 2025; Sekharan et al., 2021; Torres-Soto et al., 2021). Programme facilitators were diverse, including consumers (service users), nurses, nutritionists, occupational therapists, peer workers, personal trainers, physiotherapists, psychiatrists, psychologists, researchers, social workers, students and support workers. Programme duration varied greatly, ranging from eight sessions to 12 months.
Approaches underpinning programmes
Programmes typically utilised multiple approaches, as shown in Table 2. The most frequently used approaches were rehabilitation (Lee and Harris, 2010; Life Adjustment Team, 2025; Lima, 2008; McAlpine, 1991; McLean Hospital, 2024; NDIS, 2025; Nelson and Condrin, 1987; NHS, 2022; Oke and Kanigsberg, 1991; Pacific Teen Treatment, 2024; Priory, 2025; Torres-Soto et al., 2021) and recovery (Clark et al., 2006; Department of Health and Aged Care, 2024; Lamont et al., 2017; Lee et al., 2014; NDIS, 2025; NHS, 2022; Sekharan et al., 2021), followed by psychotherapy (McLean Hospital, 2024; Mehl, 1997; Pacific Teen Treatment, 2024; Priory, 2025; Sayk et al., 2025; Soleimani et al., 2024), physical activity (De Girolamo et al., 2024; Gabarda-Blasco et al., 2024; Lamont et al., 2017; St-Amour et al., 2024), mind-body medicine (Brogan et al., 2020; De Girolamo et al., 2024; Tomasi et al., 2019), crisis management/autonomy (Enoksson et al., 2021; Helleman et al., 2014, 2018), stepped care (Lee et al., 2014; Sekharan et al., 2021), transitional care (Priory, 2025; Scanlan et al., 2017), chronobiology/sleep (Bromundt et al., 2013; Sayk et al., 2025), adventure-based therapy (Gabarda-Blasco et al., 2024), art therapy (Mehl, 1997), behaviour analysis/modification (Ortega, 2004), developmental frame of reference (Oke and Kanigsberg, 1991), early intervention (Orygen, 2024), empowerment (Clark et al., 2006), experiential learning (Gabarda-Blasco et al., 2024), psychoeducation (De Girolamo et al., 2024), symptom management (Torres-Soto et al., 2021) and systems theory (Nelson and Condrin, 1987).
Domains of daily living functioning addressed in records
Table 3 summarises the domains of daily living functioning addressed across all 44 records, including the self-directed educational materials. The most frequently addressed domain was ‘health’ (n = 189), followed by ‘relational’ (n = 84), ‘responsibility’ (n = 67), ‘personal’ (n = 61), ‘leisure’ (n = 53), ‘routine’ (n = 42) and ‘household’ (n = 30).
Domains of daily living functioning addressed in records.
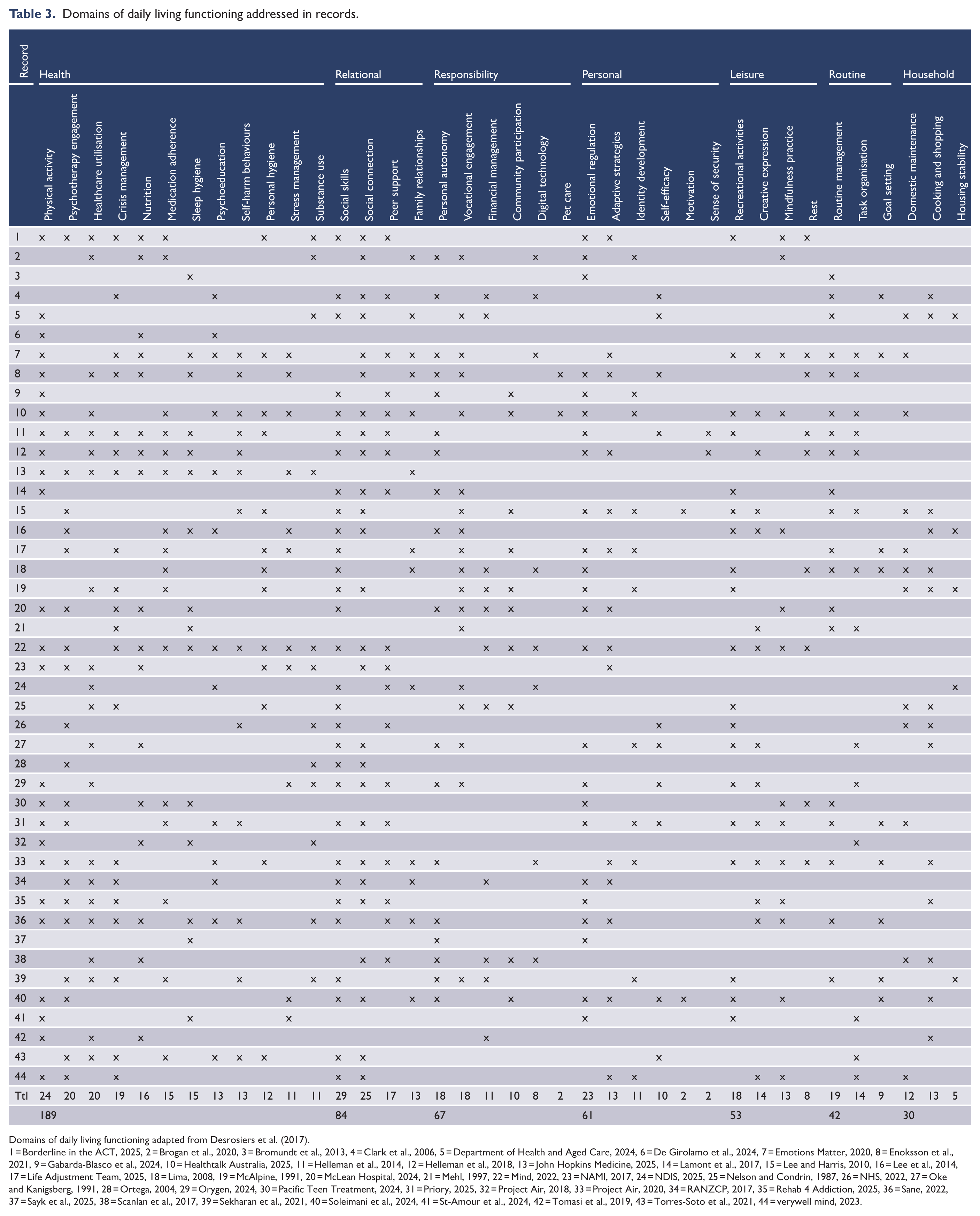
Domains of daily living functioning adapted from Desrosiers et al. (2017).
1 = Borderline in the ACT, 2025, 2 = Brogan et al., 2020, 3 = Bromundt et al., 2013, 4 = Clark et al., 2006, 5 = Department of Health and Aged Care, 2024, 6 = De Girolamo et al., 2024, 7 = Emotions Matter, 2020, 8 = Enoksson et al., 2021, 9 = Gabarda-Blasco et al., 2024, 10 = Healthtalk Australia, 2025, 11 = Helleman et al., 2014, 12 = Helleman et al., 2018, 13 = John Hopkins Medicine, 2025, 14 = Lamont et al., 2017, 15 = Lee and Harris, 2010, 16 = Lee et al., 2014, 17 = Life Adjustment Team, 2025, 18 = Lima, 2008, 19 = McAlpine, 1991, 20 = McLean Hospital, 2024, 21 = Mehl, 1997, 22 = Mind, 2022, 23 = NAMI, 2017, 24 = NDIS, 2025, 25 = Nelson and Condrin, 1987, 26 = NHS, 2022, 27 = Oke and Kanigsberg, 1991, 28 = Ortega, 2004, 29 = Orygen, 2024, 30 = Pacific Teen Treatment, 2024, 31 = Priory, 2025, 32 = Project Air, 2018, 33 = Project Air, 2020, 34 = RANZCP, 2017, 35 = Rehab 4 Addiction, 2025, 36 = Sane, 2022, 37 = Sayk et al., 2025, 38 = Scanlan et al., 2017, 39 = Sekharan et al., 2021, 40 = Soleimani et al., 2024, 41 = St-Amour et al., 2024, 42 = Tomasi et al., 2019, 43 = Torres-Soto et al., 2021, 44 = verywell mind, 2023.
Measures used to describe changes in functioning
Eighty-nine measures were used to describe changes in functioning across the included quantitative studies (Brogan et al., 2020; Bromundt et al., 2013; Clark et al., 2006; De Girolamo et al., 2024; Gabarda-Blasco et al., 2024; Lee et al., 2014; Lee and Harris, 2010; Lima, 2008; McAlpine, 1991; Mehl, 1997; Nelson and Condrin, 1987; Ortega, 2004; Sayk et al., 2025; Scanlan et al., 2017; Sekharan et al., 2021; Soleimani et al., 2024; St-Amour et al., 2024; Tomasi et al., 2019; Torres-Soto et al., 2021). Sixty-four of these were valid and reliable, such as the Borderline Evaluation of Severity Over Time (BEST) (Pfohl et al., 2009), Kohlman Evaluation of Living Skills (KELS) (Burnett et al., 2009) and Recovery Assessment Scale – Domains and Stages (RAS-DS) (Hancock et al., 2015). The Health of the Nation Outcome Scale (HoNOS) appeared in two separate studies of the Prevention & Recovery Centre (PARC) in Victoria, Australia (Lee et al., 2014; Sekharan et al., 2021), despite its lack of reliability and validity (Brooks, 2000). An overview of these measures is provided in Supplementary File 1. The wide array of measures demonstrates the lack of standardised assessment of daily living functioning.
Discussion
This scoping review synthesised literature describing programmes that address the daily living functioning of people diagnosed with BPD. Persistent functional impairment despite symptomatic remission represents a critical gap in current treatment (Álvarez-Tomás et al., 2019; Choi-Kain et al., 2020). The programmes found in this review were bespoke and service-specific, with considerable variability in aims, content and delivery. This ad hoc approach to addressing daily living functioning is in stark contrast to the theoretically informed and manualised psychotherapies (Choi-Kain et al., 2017; Storebø et al., 2020). Such variability in rehabilitation for daily living functioning indicates the need for a more systematic and evidence-based approach.
The high frequencies of the ‘relational’ and ‘responsibilities’ domains of functioning found in this review reflect the well-documented challenges that people diagnosed with BPD face in employment and relationships (Grenyer et al., 2022; Miller et al., 2018; Zanarini et al., 2010b). The other frequently occurring domains seemed to highlight burgeoning areas of interest in research, including ‘sleep hygiene’ (King et al., 2024), ‘healthcare utilisation’ (Botter et al., 2021; Glass et al., 2024), ‘physical activity’ (Petersen et al., 2025), ‘nutrition’ (St-Amour et al., 2023), ‘crisis management’ (Warrender et al., 2020), ‘personal hygiene’ (Potvin et al., 2019), ‘routine management’ (Birken and Harper, 2017; Falklöf and Haglund, 2010) and ‘recreational activities’ (leisure) (Borovica et al., 2024). Importantly, greater focus on these ‘other’ domains of functioning could support people diagnosed with BPD in obtaining and maintaining work (Kernot et al., 2023; Larivière et al., 2025).
Measures used to describe changes in functioning were strikingly heterogeneous, with 89 measures identified, 25 (28%) of which were bespoke or lacked reliability and validity. This large number of measures reflects the disparate nature of the evidence base informing rehabilitation programmes for people diagnosed with BPD. The diversity of measures also reflects the broader challenge of assessing functional impairment in mental health (Üstün and Kennedy, 2009). The Global Assessment of Functioning (GAF) (Endicott et al., 1976) was not used to describe changes in functioning in any of the programmes, confirming its lack of clinical utility (Gold, 2014). Notably, while there is a measure of daily living functioning specifically designed for people diagnosed with BPD, it is currently only available in French (Desrosiers et al., 2017).
Recommendations for practice
Given persistent functional impairment, rehabilitation for daily living functioning should be offered alongside or re-centred within evidence-based psychotherapy for people diagnosed with BPD. Rehabilitation could involve greater emphasis on the domains of daily living functioning outlined in Table 3, including health (sleep hygiene, physical activity and nutrition), household management (cooking and shopping), routine management (task organisation), responsibility (financial management and community participation) and leisure (recreational activities and creative expression). This approach requires shifting focus to consider all domains of daily living functioning, rather than relying solely on relational and vocational domains as indicators of functional recovery. Practitioners can draw from the available rehabilitation programmes and measures found in this review to structure and evaluate service delivery. However, practitioners will need to rely on clinical judgement when choosing between options, as a robust and comparable research evidence base has not yet been established.
Recommendations for future research
Research is needed to strengthen the evidence base for rehabilitation programmes addressing the daily living functioning of people diagnosed with BPD. This involves developing and rigorously evaluating comprehensive programmes that address all domains of functioning. A validated English-language assessment tool for evaluating daily living functioning is urgently needed. The development of such a tool and future programmes addressing daily living functioning should be informed by both lived experience and clinical perspectives. Future research should evaluate whether addressing daily living functioning improves both psychotherapy and sustained work outcomes.
Strengths and limitations
A strength of this review is its comprehensive scope, with no date or language restrictions and incorporating grey literature across multiple countries. However, programmes reporting positive outcomes are more likely to be available, creating publication bias. The search terms were based on a Google Translate version of Desrosiers et al.’s (2017) assessment tool, potentially excluding programmes using different terminology to describe daily living functioning. The predominance of female participants (84%) in the sample may limit the generalisability of findings to males diagnosed with BPD (Larivière et al., 2023).
Conclusion
Rehabilitation for daily living functioning is critically important for people diagnosed with BPD given persistent functional impairment, yet a comprehensive search of existing programmes found only 44 records to guide service delivery. There were substantial inconsistencies in the aims, content and delivery of these programmes. Daily living functioning requires increased research attention and clinical focus to enable functional recovery. Future rehabilitation programmes must comprehensively address all domains of daily living functioning and be systematically evaluated using reliable and valid measures.
Supplemental Material
sj-docx-1-anp-10.1177_00048674251393159 – Supplemental material for A scoping review of programmes that address the daily living functioning of people diagnosed with borderline personality disorder
Supplemental material, sj-docx-1-anp-10.1177_00048674251393159 for A scoping review of programmes that address the daily living functioning of people diagnosed with borderline personality disorder by Dillon Tepper, Ben Sellar, Sheryl Shipley, Rachel Smith and Carolyn M Murray in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We express our gratitude to our consumer and carer consultants for their time, feedback and guidance. We would also like to acknowledge the academic librarian staff at the University of South Australia for their assistance with refining the search terms.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research is supported by an Australian Government Research Training Programme (RTP) Scholarship for Dillon Tepper’s PhD.
Data availability statement
All data for this scoping review is based on publicly available information.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.