
Abstract

Introduction
There is considerable overlap in the clinical, genetic, and neuroanatomical features of non-affective (e.g. schizophrenia) and affective (e.g. manic/depressive/bipolar) psychotic disorders (Cattarinussi et al., 2022; Pearlson, 2015). However, evidence of clinical differences prior to the onset of non-affective and affective psychoses suggest greater neurodevelopmental deficits among those who develop non-affective psychosis (Parellada et al., 2017). Prior psychiatric diagnoses may be distinct from a period of subclinical symptoms immediately preceding the onset of psychosis (typically considered the ‘prodromal phase’), or indeed, antecedent psychiatric diagnoses may represent the start of an ‘initial prodrome’ for psychotic disorders (Ortiz-Orendain et al., 2023). Previous studies have produced mixed findings, with some suggesting that the initial prodromes of non-affective and affective psychoses are indistinguishable (Olvet et al., 2010), while other studies suggest higher rates of depressive and anxiety disorders in the initial prodrome of affective psychosis (Ortiz-Orendain et al., 2023; Rietdijk et al., 2011). However, few studies have examined antecedent diagnoses of neurodevelopmental disorders such as autism and attention-deficit/hyperactivity disorders (ADHD), and previous samples have been relatively small. Here, we used administrative data for a large, population study to examine differences between groups of individuals diagnosed with affective or non-affective psychoses in terms of (1) the number and type of psychiatric diagnoses prior to the first psychosis diagnosis, (2) the average age of onset of antecedent and psychosis diagnoses, and (3) the length of time between the first antecedent (non-psychotic) diagnosis and first psychosis diagnosis.
Methods
Participants
Participants were 3176 young people (mean age = 20.70 years [SD = 0.40] at follow-up) with a diagnosis of non-affective or affective (manic/depressive) psychosis, drawn from the New South Wales Child Development Study (NSW-CDS) population cohort of 91,597 individuals born between 2002 and 2005 (Green et al., 2024). Record-linkages combining health and social service records from the time of the child’s birth until June 2020/2024 were performed by the NSW Centre for Health Record Linkage (http://www.cherel.org.au; false-linkage rate ~0.5%) and Australian Institute of Health and Welfare (AIHW) Data Integration Service Centre. Ethical approval was provided by the NSW Population and Health Services and the Australian Capital Territory (ACT) Health Research Ethics Committees (HREC/18/ciphs/49) and the AIHW Human Research Ethics Committee (EO2020/4/1026) under the ‘waiver of consent’ provision outlined in the National Statement of Ethical Conduct in Human Research (National Health and Medical Research Council, 2023).
Diagnoses of affective or non-affective psychoses
A binary indicator of non-affective (e.g. schizophrenia) or affective psychosis (e.g. bipolar disorders) was derived from the most recently recorded indicator of psychosis, according to International Classification of Diseases: 10th Edition, Australian Modification (ICD-10-AM) F-codes (Supplementary eTable 1) recorded in the NSW & ACT Admitted Patient Data Collections (APDC, 2002-2021), the NSW & ACT Emergency Department Data Collections (EDDC, 2005–2021) the NSW Mental Health Ambulatory Data Collection (MH-AMB, 2002–2020), or antipsychotic prescriptions (ATC: N05A) recorded in the AIHW’s Pharmaceutical Benefits Scheme data collection (PBS, 2002–2024) with a streamlined authority code indicating treatment for schizophrenia or bipolar disorder/mania. Supplementary eTable 2 provides information about the consistency of diagnoses across time and data collections.
Antecedent psychiatric diagnoses
Using the health records described above, binary indicators of psychiatric diagnosis recorded prior to the first episode of psychosis were derived for: (1) depressive, (2) anxiety, (3) eating, (4) conduct, (5) cluster B personality, (6) substance use (non-psychotic), (7) developmental, (8) and ADHD (formally known as hyperkinetic disorders in ICD-10), as well as (9) self-harm/suicidal ideation, and (10) any mental disorder (see Supplementary eTable 1). The length of the ‘initial prodrome’ was estimated as the number of days between first psychiatric diagnosis of any kind and the first diagnosis of any psychosis. In addition, the total number of antecedent (non-psychotic) presentations to health services was derived from primary or secondary diagnoses in APDC, EDDC, and MH-AMB records.
Statistical analysis
Analyses were performed in R v.4.0.3. Differences between psychosis groups in initial prodrome duration were evaluated using t-tests. A series of univariable and multivariable (accounting for age and sex) log binomial regression analyses determined the relative risk of affective psychosis (compared to non-affective psychosis as the reference group) associated with each antecedent psychiatric disorder.
Results
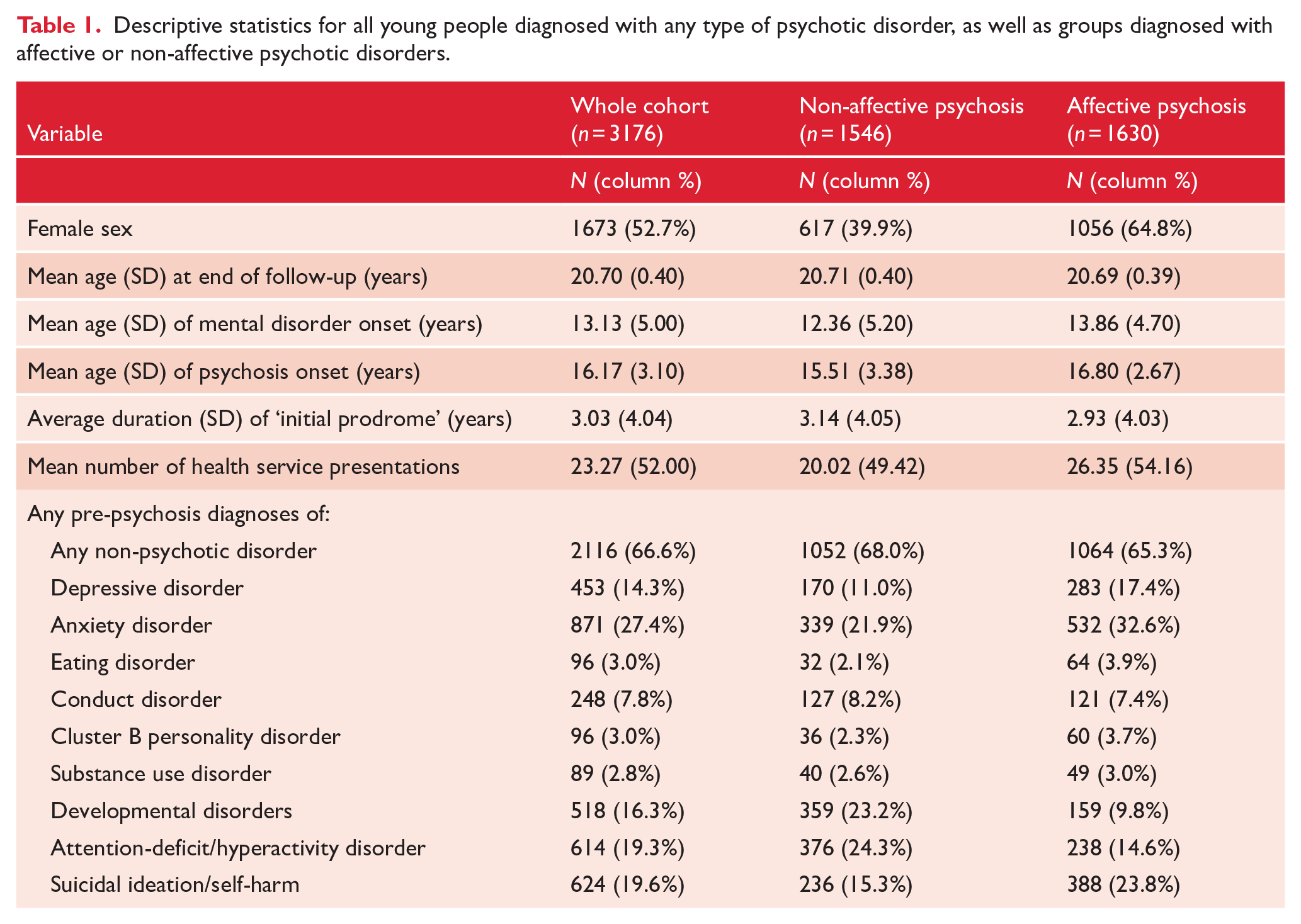
Descriptive statistics are displayed in Table 1. Individuals with non-affective psychosis were significantly younger at the time of their first mental disorder diagnosis (t = 8.52, df = 3101.6, p < .001, Cohen’s d = 0.303) and their first episode of psychosis (t = 11.88, df = 2942.1, p < .001, Cohen’s d = 0.424), and had fewer antecedent mental health presentations (t = 3.44, df = 3169.3, p < .001, Cohen’s d = 0.122), relative to youth with affective psychosis. The average time between the first antecedent (non-psychotic) diagnosis and first psychotic diagnosis was similar across the affective and non-affective psychoses groups (t = −1.480, df =3163.0, p = .139, Cohen’s d = 0.052). Females were more likely to be diagnosed with affective psychosis (relative risk (RR) = 1.65, 95% confidence interval (CI) = 1.54–1.78).
Descriptive statistics for all young people diagnosed with any type of psychotic disorder, as well as groups diagnosed with affective or non-affective psychotic disorders.
Individuals who went on to develop affective psychosis were more likely to have been previously diagnosed with depressive and anxiety disorders and to have experienced suicidal ideation/self-harm, relative to young people with non-affective psychoses in multivariable models (see Figure 1). In contrast, individuals with non-affective psychosis were 81% (58% adjusted) more likely to have antecedent diagnoses of developmental disorder and 41% (22% adjusted) more likely to have antecedent diagnoses of ADHD, relative to those with affective psychosis. There were no differences between affective and non-affective psychosis in antecedent diagnoses of externalising disorders.
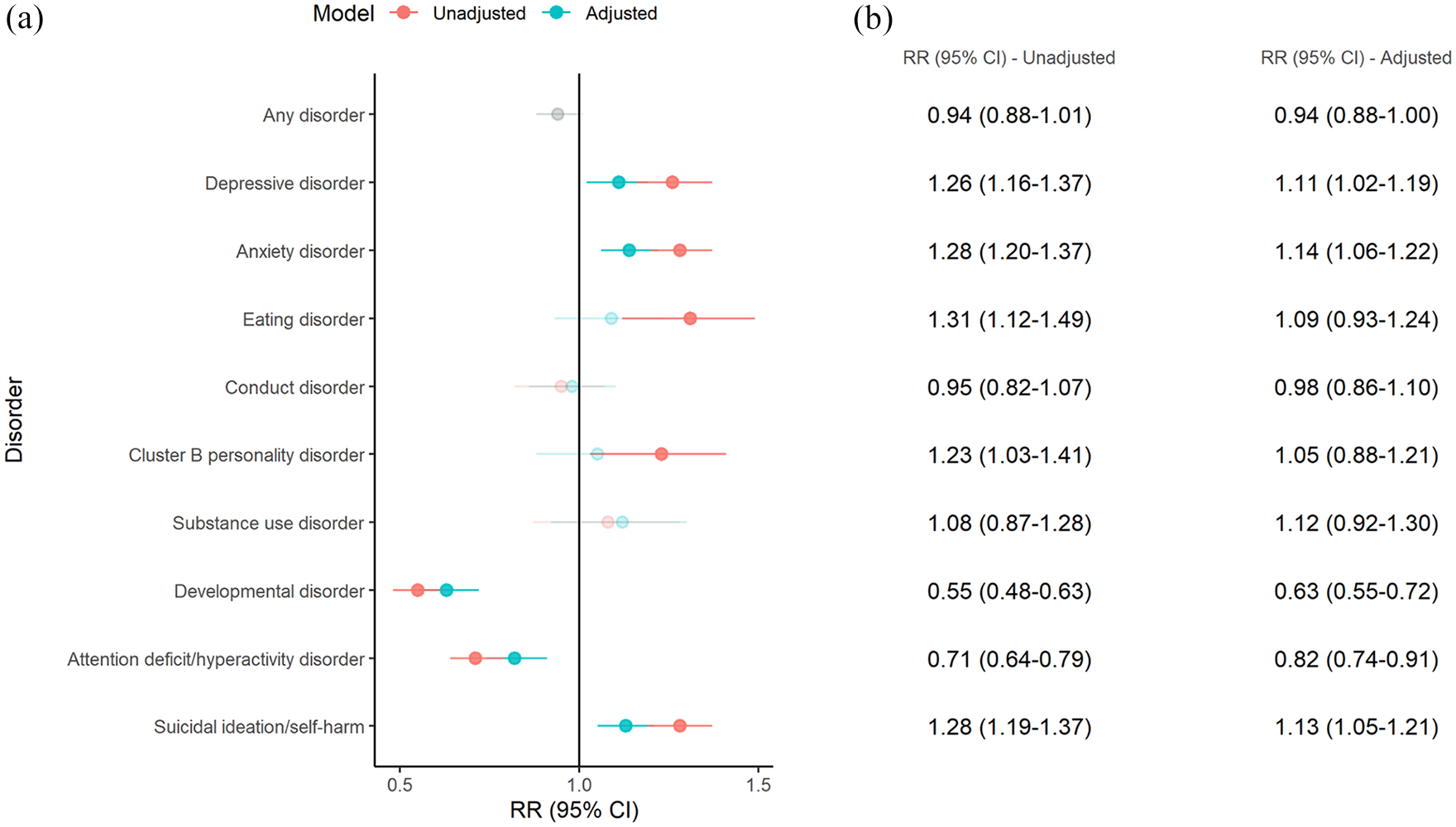
Relative risk of mental disorder diagnoses prior to the first diagnosis of affective psychosis (relative to non-affective psychosis).
Discussion
Among 3176 Australian young people aged ~20 years with a psychotic disorder, those with non-affective psychoses were more likely to present with developmental disorders and ADHD in childhood, earlier in life, but presented to mental health services less frequently than those with affective psychoses. In contrast, those with affective psychoses were more likely to be diagnosed with an internalising disorder (i.e. depressive disorders, anxiety disorders, and suicidal ideation/self-harm) prior to their first episode of psychosis. Notably, the present results were demonstrated in a substantially larger and younger cohort relative to prior studies of diagnoses preceding psychosis (Ortiz-Orendain et al., 2023; Rietdijk et al., 2011). These findings are consistent with previous work suggesting that premorbid developmental deficits are more strongly associated with non-affective (relative to affective) psychoses (Parellada et al., 2017), while externalising (i.e. conduct) disorders are common antecedent diagnoses of both disorders (Ortiz-Orendain et al., 2023), at a rate substantially higher than that observed in the general population (Fairchild et al., 2019). Conduct problems, which have been shown to precede almost all forms of adult psychopathology (Kim-Cohen et al., 2003), thus represent an early point for preventive interventions.
The use of administrative health records likely underestimated the incidence of mental disorders, and raises issues of diagnostic instability (e.g. 28.7% of the sample received diagnoses of both affective and non-affective psychosis at different timepoints). We thus used the most recent diagnosis for classification purposes, but some individuals may eventually have their diagnoses revised. We could not ascertain lifetime diagnoses given the limited period of follow-up; some young people may yet develop psychosis in later life.
Knowledge of childhood clinical presentations prior to the first episode of psychosis may assist paediatricians and adolescent psychiatrists to more efficiently screen for psychosis in vulnerable young people, and provide earlier intervention for emerging psychosis. Children with anxiety, depression, and suicidal ideation/self-harm are somewhat more likely to eventually present with affective psychosis, while the opposite is true for children with neurodevelopmental disorders. These findings can inform targeted strategies to prevent psychosis in young people.
Supplemental Material
sj-docx-1-anp-10.1177_00048674251361768 – Supplemental material for Psychiatric diagnoses prior to the first onset of non-affective and affective psychoses
Supplemental material, sj-docx-1-anp-10.1177_00048674251361768 for Psychiatric diagnoses prior to the first onset of non-affective and affective psychoses by Oliver J Watkeys, Kirstie O’Hare, Kimberlie Dean, Kristin R Laurens, Stacy Tzoumakis, Felicity Harris, Vaughan J Carr and Melissa J Green in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This research used population data owned by the NSW Department of Education; Australian Curriculum, Assessment and Reporting Authority (ACARA), managed by the NSW Education Standards Authority; NSW Department of Communities and Justice; NSW Ministry of Health; ACT Health; NSW Registry of Births, Deaths and Marriages; the Australian Coordinating Registry (on behalf of Australian Registries of Births, Deaths and Marriages, Australian Coroners and the National Coronial Information System); Australian Bureau of Statistics; Australian Institute of Health and Welfare; Department of Social Services; NSW Bureau of Crime Statistics and Research; NSW Department of Justice, and; NSW Police Force. This research used data from the Australian Early Development Census (AEDC). The AEDC is funded by the Australian Government Department of Education. The findings and views reported are those of the authors and should not be attributed to these Departments, or the NSW and Australian Government. Record linkages were conducted by the NSW Centre for Health Record Linkage (CHeReL) and the Australian Institute of Health and Welfare Data Integration Service Centre.
Correction (November 2025):
This paper has been updated online to correct the term “non-affective” to “affective” in the sentence: In contrast, those with affective psychoses were more likely to be diagnosed with an internalising disorder (i.e. depressive disorders, anxiety disorders, and suicidal ideation/self-harm) prior to their first episode of psychosis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted by the University of New South Wales with financial support from the National Health and Medical Research Council (NHMRC) Project Grant (grant no. APP1148055), an Australian Research Council (ARC) Discovery Project (grant no. DP230101990), a Department of Health and Aged Care Medical Research Future Fund Million Minds Mental Health Grant (grant no. APP2006436), and a Postdoctoral Fellowship from Suicide Prevention Australia (awarded to O.W.).
Data Availability Statement
Data used in this project have been provided by government or other agencies for the research purposes of the NSW Child Development Study and are unable to be shared with third parties or deposited into data repositories. Researchers wishing to access these data need to apply in writing to relevant data custodians.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.