
Abstract
Objective:
Art therapy offers a predominantly non-verbal form of creative self-expression for people experiencing mental health issues. This systematic review aims to investigate the effectiveness and acceptability of art therapy for children and adolescents experiencing acute or severe mental health conditions.
Methods:
Following PRISMA guidelines, five electronic databases were searched (Embase, MEDLINE, Web of Science Core Collection, PsychINFO, CINAHL) using the search terms (‘art therap*’ OR ‘art psychotherap*’) AND (‘child*’ OR ‘adolescen*’ OR ‘youth’ OR ‘young’ OR ‘teen*’). Study quality was assessed based on methodological rigour, and narrative synthesis of findings was undertaken.
Results:
Of 3529 identified articles, 90 (23 original research papers and 67 case studies) met criteria. Art therapy delivery method, dose and intervention duration varied across studies. Nonetheless, synthesis of the 23 original research studies indicated high acceptability. Randomised control trials demonstrated effectiveness in reducing the severity of symptoms of post-traumatic stress disorder, depression and suicidal ideation. Quasi-experimental, cohort and cross-sectional studies also showed reductions in anxiety symptoms and improvements in emotion regulation, self-awareness, distress tolerance, confidence, communication and self-expression across various mental health conditions.
Conclusion:
Art therapy is an effective and acceptable treatment for young people experiencing acute or severe mental health conditions, with a preponderance of evidence for post-traumatic stress disorder. Effectiveness across conditions, settings and art therapy intervention type suggests the capacity of art therapy to adapt to needs of young people. Enhanced access to art therapy for young people navigating acute distress will support the provision of engaging and effective mental health treatments.
Introduction
Mental health conditions are a major public health challenge for children and adolescents (Benton et al., 2021). The prevalence of mental health conditions in young people (Sara et al., 2023) and their significant impact on both functioning (Wille et al., 2008) and quality of life (Weitkamp et al., 2013) underscore the imperative for effective and acceptable therapeutic interventions (Kieling et al., 2011). While many young people respond positively to talk-based psychotherapies, some may not have the inclination or capacity to engage in these interventions owing to symptom severity, situational mutism or past negative experiences with talk-based therapies (Coholic et al., 2020; Versitano et al., 2024b).
Art therapy is a creative psychotherapeutic approach utilising art-making with visual and/or tactile media. Conducted within a therapeutic relationship with a trained therapist, it can support improved cognitive, physical and emotional well-being (American Art Therapy Association [AATA], 2023; Australian, New Zealand and Asian Creative Arts Therapies Association, 2024; British Association of Art Therapists [BAAT], 2024). Art therapy offers a non-verbal form of expression, which can be particularly useful for people who have difficulty articulating their emotions or experiences verbally (Chong, 2015; Rubin, 2005). Furthermore, art therapy can provide a safe and structured environment in which young people can explore overwhelming emotions, process traumatic experiences and establish coping mechanisms (Braito et al., 2022).
Art therapy has been used with children and adolescents experiencing mental health challenges such as depression, anxiety, post-traumatic stress disorder (PTSD), among other mental health conditions (Braito et al., 2022). Art therapy is also increasingly integrated into mental health services (Bosgraaf et al., 2020; Braito et al., 2022; Scope et al., 2017), warranting rigorous assessment of its effectiveness and acceptability. Clear assessment and evaluation of the effectiveness of art therapy with young people can be translated into advocacy for implementation in mental health services (Cornish, 2013).
Case studies have long supported the use of art therapy in mental health settings (e.g. Atlas et al., 1992; Diamond-Raab and Orrell-Valente, 2002; Naumburg, 1945) and reviews which explore the spectrum of art therapy practices and approaches have also been undertaken (Potash et al., 2016; Van Lith, 2016). Effectiveness has been demonstrated in reviews of art therapy with adult populations, highlighting improved mental health outcomes, beneficial psychosocial effects, as well as reductions in trauma and depression symptoms (Maujean et al., 2014; Schouten et al., 2015; Shukla et al., 2022). The effectiveness of art therapy with children has also been reviewed (Braito et al., 2022; Cohen-Yatziv and Regev, 2019; Moula, 2020) and improvements in quality of life, anxiety, self-concept, problem-solving skills, attitudes towards school, and emotional and behavioural difficulties have been shown, with evidence suggesting it is particularly beneficial for children who have experienced trauma, or who have PTSD symptoms (Braito et al., 2022). However, reviews which focused on art therapy for children and adolescents did not examine acceptability, and excluded non-English publications (Braito et al., 2022; Cohen-Yatziv and Regev, 2019; Moula, 2020). Further to this, previous reviews have also placed limitations on outcome measures used, excluding case studies and qualitative studies (Cohen-Yatziv and Regev, 2019; Moula, 2020); however, our current review will include both qualitative and quantitative research with no restriction regarding outcome measures used.
Our systematic review will address these gaps by including non-English publications, placing fewer limitations on outcome measures and exploring both effectiveness and acceptability of art therapy interventions, with a focus on young people experiencing acute or severe mental health conditions. Discerning acceptability is critical when considering the use of therapeutic interventions in mental health settings (Sekhon et al., 2017). This is particularly salient with young people, as engagement and sustained participation are often challenging, yet essential for positive outcomes (Shin and Ahn, 2023). Increased understanding of art therapy acceptability and effectiveness will assist in delineating efficacious treatments for young people in acute or severe phases of mental health care, which is relevant to the current growing mental health crisis (Benton et al., 2021).
Methods
The protocol for this systematic review was registered on PROSPERO (CRD42024468934) and follows the guidelines for Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) (Page et al., 2021).
Search strategy
Existing peer-reviewed research published from database inception up until November 2023 was searched on Embase, MEDLINE, Web of Science Core Collection, PsychINFO & CINAHL. Search terms were (‘art therap*’ OR ‘art psychotherap*’) AND (‘child*’ OR ‘adolescen*’ OR ‘youth’ OR ‘young’ OR ‘teen*’). A secondary search was conducted before final analysis to include additional articles published up until 17 September 2024.
Inclusion and exclusion criteria
Peer-reviewed articles reporting original research on art therapy for individuals aged 0–24 years during an acute and/or severe mental health phase were included. For non-English language articles which met all other inclusion criteria, Google translate software was used to facilitate data extraction (Jackson et al., 2019). Individuals in an acute phase of care were defined as those who were (1) admitted in an inpatient mental health setting; (2) experiencing active psychotic, manic or suicidal symptoms and/or (3) experiencing severe, extreme or sudden onset symptoms of any other psychiatric disorders, e.g., depression or anxiety (American Psychological Association [APA], 2018). Unless stipulated, all Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5-TR) psychiatric conditions, plus disorders reported in earlier DSM versions or the International Classification of Diseases 11 (ICD-11), were considered for inclusion based on symptom severity and/or acuity, e.g., obsessive compulsive disorders, functional neurological disorders, eating disorders or mood disorders. Pervasive neurodevelopmental conditions such as intellectual disability and autism spectrum disorder (ASD) were included where there were intercurrent severe or acute mental health challenges.
If mental health diagnosis and illness severity were ambiguous regarding the above criteria, then social and environmental factors were also considered: for instance, if participants had a confirmed or probable history of complex trauma and/or if they were in a high-risk group such as out-of-home care or juvenile justice. Such clinically ambiguous cases were considered for inclusion in consultation with a child and adolescent psychiatrist (I.P.). When available, pre-test scores were examined to gauge symptom severity according to scoring and clinical cut-offs. Both qualitative and quantitative research were included, with no restriction regarding outcome measures. Studies where art therapy was conducted in combination with other therapeutic interventions were included (e.g. art therapy and mindfulness), given an art therapist or qualified health professional facilitated them. Articles were excluded when (1) young people were not experiencing an acute or severe mental health condition and/or (2) an arts-based intervention was not identified by authors as ‘art therapy’ or ‘art psychotherapy’.
Study selection and data extraction
Data from the searches conducted were imported and de-duplicated in EndNote. Remaining citations were imported into Covidence, where removal of duplicates was undertaken again by the first author (S.V.). Two authors (S.V., S.T.) screened titles and abstracts to identify relevant studies. Two authors (S.V. and C.L.) then undertook full-text review of the remaining studies. Discrepancies were resolved by consensus. Consultation with a co-author child and adolescent psychiatrist was undertaken as required to discern eligibility, particularly when symptom acuity was unclear (I.P.). Three authors extracted data from the included studies in Excel (S.V., C.L. and S.T.). The first author (S.V.) summarised information from the original research studies relevant to study aims, effectiveness and acceptability, and a co-author (S.T.) summarised case study findings separately.
Quality assessment
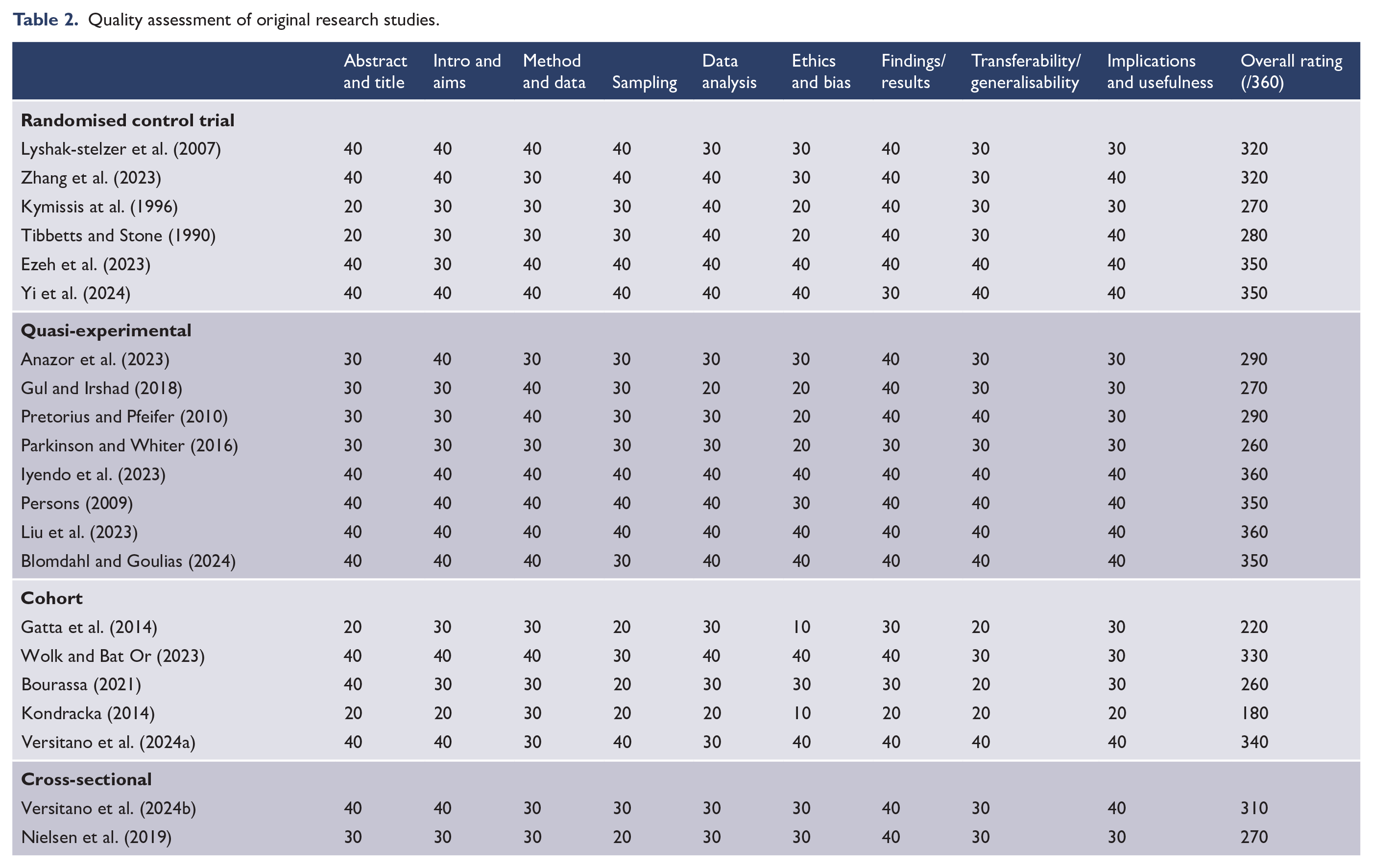
Hawker et al.’s (2002) critical appraisal tool was used to assess research quality, scoring methodological rigour based on nine categories: (1) abstract and title, (2) introduction and aims, (3) method and data, (4) sampling, (5) data analysis, (6) ethics and bias, (7) findings/results, (8) transferability/generalisability, (9) implications and usefulness. Categories were independently scored by two authors (S.V. and C.L.), and discrepancies were resolved by consensus. For each category, quality ratings were assessed as either ‘good’ (score of 40), ‘fair’ (30), ‘poor’ (20) or ‘very poor’ (10), demonstrating the strengths and weaknesses within each study (Hawker et al., 2002). A total score was calculated to illustrate overall quality, ranging from 90 to 360, where higher scores indicate higher quality.
Results
A total of 3529 articles were extracted from all databases (Figure 1). After removal of 612 duplicates, and screening against inclusion and exclusion criteria, a total of 90 studies were included in the final synthesis. This comprised 67 case studies and 23 original research studies.
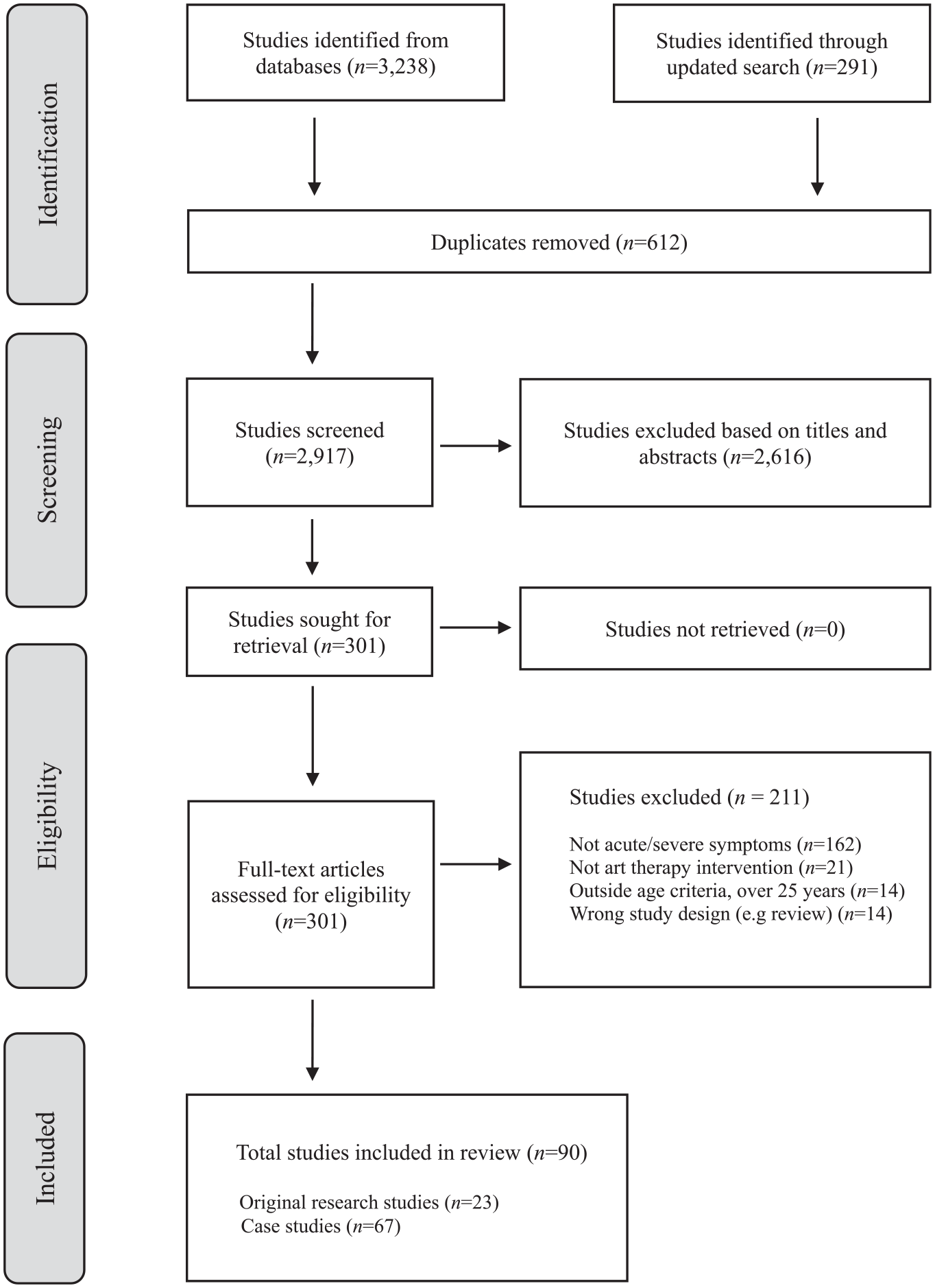
PRISMA flow diagram (Page et al., 2021).
Original research studies
Of 23 original research studies reviewed (Table 1), 9 took place in hospital-based mental health care settings. Most of these were inpatient child and adolescent psychiatric units (n = 7), in addition to a residential rehabilitation centre (n = 1), and a youth partial hospitalisation unit supporting transition out of hospital-based psychiatric care (n = 1). Nine studies took place in school environments, including a school set up within camps for internally displaced people, a post-psychiatric hospitalisation boarding school and an alternative schooling environment for ‘seriously emotionally disturbed’ young people. Other settings included community mental health care (n = 2), juvenile justice (n = 2) and out-of-home care (n = 1).
Effectiveness and acceptability of art therapy interventions.

N/R: Not reported; N/A: Not applicable.
Participant demographics
There were a total of 4053 participants within 23 studies. Of these, 1400 were male, 2508 were female, 3 participants were non-binary or agender and 142 participants were uncategorised. Participants presented with a range of severe and/or acute mental health challenges. Seven studies focused specifically on young people with PTSD or severe post-traumatic stress symptoms. Ten studies included participants with various mental health conditions including mood disorders, personality disorders, anxiety disorders, eating disorders, conduct disorders, schizophrenia or psychotic spectrum disorders, or neurodevelopmental disorders (co-occurring with a mental health condition). The remaining studies focused on a single diagnosis or presentation, including severe depression, anorexia nervosa, first episode psychosis, personality disorders and suicidal ideation. Studies were conducted across diverse geographic locations, predominantly Africa (n = 7), Europe (n = 5), the United States (n = 4) and Australia (n = 3).
Art therapy interventions
The art therapy interventions offered varied substantially. Most interventionists were art therapists (n = 18) with minor variation in terminology such as ‘art psychotherapist’, ‘certified art therapist’, ‘qualified art therapist’, ‘registered art therapist’ or ‘professional art therapist’. Five studies reported on art therapy interventions facilitated by other health professionals such as psychologists, psychiatrists or psychotherapists.
Most studies delivered art therapy interventions in a group format (n = 16). Four focused specifically on individual art therapy sessions, while three provided both group and individual interventions. Study duration ranged from two half-day workshops, up to 2 years of art therapy service delivery. The length of participant engagement varied, and often depended upon their length of stay, particularly within inpatient and juvenile justice settings. Session frequency varied from one to five times per week, and sessions ranged from 45 minutes, to a half day in duration. Longer sessions were often group-based, while briefer interventions tended to be individual sessions. Some studies utilised an open studio approach (n = 4), wherein participants could come and go from the artmaking space with the art therapist always present to provide support (Finkel and Bat Or, 2020).
Intervention structure also varied. Many interventions could broadly be categorised as either directive (n = 11) – guided by specific themes or structured activities – or non-directive (n = 6) – client-led exploration of organically emerging themes or ideas (Kottman and Dickinson, 2016). Some studies utilised a mixture of directive and non-directive components (n = 6), often structuring sessions responsively based on participant need. Art therapy practices can occur across a continuum, at times incorporating guiding elements, as well as opportunities for self-directed exploration (Kottman and Dickinson, 2016). Intervention descriptions are outlined in Table 1.
Control groups
Eleven studies utilised a control group, five of which were waitlist control and two which received no treatment. Of the remaining three control groups, one was an arts-and-crafts activities group (Lyshak-Stelzer et al., 2007), another was a freeform discussion group (Kymissis et al., 1996). The other involved a mixture of recreational activities and conversation (Tibbetts and Stone, 1990).
Effectiveness of art therapy
With substantial variation in research design and methodology, effectiveness was challenging to assess across the original research studies. The most definitive measure of effectiveness was the reduction of PTSD symptoms, as demonstrated across six studies. Most studies measured PTSD symptom severity using the International Trauma Questionnaire (Anazor et al., 2023; Ezeh et al., 2023; Iyendo et al., 2023; Zhang et al., 2023), while other studies used the UCLA PTSD Index (Lyshak-Stelzer et al., 2007) or PTSD Evaluation Scale Children and Adolescent Questionnaire (Gul and Irshad, 2018). Art therapy was effective in significantly reducing PTSD symptom severity for young people across all six studies (Anazor et al., 2023; Ezeh et al., 2023; Gul and Irshad, 2018; Iyendo et al., 2023; Lyshak-Stelzer et al., 2007; Zhang et al., 2023). Gains were maintained at 3 months (Iyendo et al., 2023; Zhang et al., 2023) and 6 months post-intervention (Ezeh at al., 2023) in follow-up studies. One study demonstrated that while both trauma-focused art therapy and an arts-and-crafts control group reduced PTSD symptoms (Lyshak-Stelzer et al., 2007), the art therapy intervention was comparatively more effective. Another study also found that the art therapy intervention was associated with a reduction in trauma symptoms related to sexual abuse history, as compared to the control (Pretorius and Pfeifer, 2010). One study showed that a dance therapy group and an art therapy group were both significantly effective in reducing PTSD symptoms compared to the control, but that dance therapy was marginally more effective (Ezeh et al., 2023). However, another study (Iyendo et al., 2023) demonstrated that art therapy was more effective in reducing PTSD symptoms compared to music therapy and poetry therapy interventions. Art therapy was also more effective than music therapy in reducing suicidal ideation (Liu et al., 2023) and depression (Yi et al., 2024).
Studies also reported improved emotion regulation, with participants managing difficult emotions through the artmaking process (Parkinson and Whiter, 2016) and feeling a greater sense of calm (Bourassa, 2021). Another study within a juvenile justice setting reported that participants who undertook the art therapy intervention had reduced anger, felt more in control and were getting into less ‘trouble’ (Persons, 2009). One study demonstrated a significant association between art therapy interventions and a reduction in seclusion, restraint and intramuscular injected sedation on an acute inpatient child and adolescent mental health unit (Versitano et al., 2024b). Improved emotional regulation and distress tolerance were further evidenced by a significant reduction in suicidal ideation (Liu et al., 2023) and a reduction in self-injurious behaviour (Persons, 2009). Cognitive improvements and regulation were also reported in relation to improved concentration (Persons, 2009), attention span (Tibbetts and Stone, 1990) and organisation of thoughts (Parkinson and Whiter, 2016).
Synthesis of findings across the remaining studies revealed several key themes. Studies demonstrated effectiveness of art therapy interventions in improving self-efficacy and empowerment, demonstrated by increased levels of self-confidence (Nielsen et al., 2019; Parkinson and Whiter, 2016; Persons, 2009), assertiveness (Kymissis et al., 1996) accomplishment (Parkinson and Whiter, 2016) and self-esteem (Coles and Harrison, 2018; Kondracka, 2014).
Art therapy interventions were also effective in increasing self-awareness (Parkinson and Whiter, 2016; Wolk and Bat Or, 2023), helping young people to understand how their thoughts related to their feelings (Nielsen et al., 2019) and improving their sense of identity (Tibbetts and Stone, 1990). Art therapy also improved self-expression (Coles and Harrison, 2018; Nielsen et al., 2019) and increased hope and resilience (Collins et al., 2023).
Two studies identified significant reductions in depressive symptoms for young people engaging in art therapy (Blomdahl and Goulias, 2024; Yi et al., 2024). While art therapy, music therapy and cognitive behaviour therapy (CBT) were all significantly effective in reducing depression (Yi et al., 2024), CBT was deemed most effective, followed by art therapy and finally music therapy. At 3 months post-intervention, CBT and art therapy groups demonstrated similar outcomes, sustaining a significant reduction in depression scores when compared to the control (Yi et al., 2024). A further three studies reported lower levels of depression and anxiety (Persons, 2009; Pretorius and Pfeifer, 2010; Tibbetts and Stone, 1990). Studies also demonstrated that art therapy enhanced overall well-being (Coles and Harrison, 2018; Kymissis et al., 1996; Nielsen et al., 2019).
Improvements in interpersonal effectiveness were demonstrated by improved communication (Kondracka, 2014), reduction in group conflict (Gatta et al., 2014) and participants feeling less anxious around others (Coles and Harrison, 2018). There were also reported improvements in participants’ relationships with others, including feeling more tolerance and acceptance (Persons, 2009).
While predominantly positive outcomes were reported, one study found an increase in avoidance within the group climate post-intervention (Gatta et al., 2014). However, authors indicated this avoidance appeared to enhance group cohesion, providing greater structure to participation and reducing conflict (Gatta et al., 2014).
Acceptability of art therapy
Acceptability of art therapy interventions was demonstrated in the majority of original research studies (n = 20/23), though the quality of evidence varied. Survey responses gathering direct feedback from young people indicated high enjoyment and satisfaction ratings for art therapy interventions across several studies (Blomdahl and Goulias, 2024; Bourassa, 2021; Collins et al., 2023; Kondracka, 2014; Nielsen et al., 2019; Versitano et al., 2024a). Within a multidisciplinary group programme on an acute inpatient unit, art therapy was one of the most consistently attended and enjoyed groups, compared to other therapeutic and diversional interventions offered (Versitano et al., 2024a). Young people also requested increased art therapy services (Versitano et al., 2024a). Similarly, within a long-stay inpatient setting, participants unanimously indicated their experience of art therapy was positive, rating it as excellent (37%), great (37%) or good (26%), with many young people wanting to continue art therapy post-discharge (Nielsen et al., 2019). Within an inpatient mental health setting for young people diagnosed with anorexia nervosa (Kondracka, 2014), participants had a unanimously positive response to the intervention, reporting being ‘satisfied’ (50%) or ‘very satisfied’ (50%), and feeling ‘safe’ (60%) or ‘very safe’ (40%), in art therapy workshops. In a youth justice programme (Collins et al., 2023), all participants reported high intervention satisfaction ‘strongly agreeing’ or ‘agreeing’ that art therapy sessions were a good fit for them and that they looked forward to sessions (Collins et al., 2023). In a study utilising manual-based phenomenological art therapy for depression (Blomdahl and Goulias, 2024), acceptability was indicated by no cancellations or programme dropouts and a high overall client satisfaction score.
Qualitative data also demonstrated acceptability of the art therapy interventions. In one study undertaken in a psychiatric unit within a juvenile correctional centre (Persons, 2009), participants shared that receiving positive recognition and encouragement in the art therapy programme were important factors contributing to their engagement and enjoyment. Furthermore, these young people were eager to participate in this voluntary art therapy programme, often continuing their artworks in their rooms at night, and spending up to 10 hours per week in group and/or individual art therapy sessions (Persons, 2009). Another study exploring a museum-based art therapy intervention (Coles and Harrison, 2018) found that participants formed positive social connections, and some continued to meet as a group several months post-intervention. Participants also stated the non-intrusive nature of art therapy accommodated for different paces and ways of engagement in an early intervention psychosis programme (Parkinson and Whiter, 2016).
Where studies made no specific reference to intervention acceptability, attrition was considered as a proxy indicator. Three studies reported no attrition (Anazor et al., 2023; Gul and Irshad, 2018; Pretorius and Pfeifer, 2010), while a further three reported very high study completion rates (all >92%) (Ezeh at al., 2023; Iyendo et al., 2023; Liu et al., 2023; Yi et al., 2024). However, one study of an inpatient mental health setting mentioned relatively high attrition due to patients being discharged prior to completing the 16-session treatment protocol (Lyshak-Stelzer et al., 2007). Another study indicated an 80% study completion rate in an alternative education environment, due to participant expulsion, absconding or a suicide attempt (Tibbetts and Stone, 1990). One study reported 44% attendance to a group art therapy programme offered in an inpatient mental health unit (Gatta et al., 2014). However, authors described attendance patterns as typical of the stability and continuity of participant engagement in that particular setting. When exploring anything participants did not like about art therapy workshops offered in an inpatient psychiatric setting (Kondracka, 2014), criticism of verbal components within the workshops was raised by some participants.
Quality assessment of included studies
Quality assessment details are included in Table 2. Almost all studies demonstrated ‘fair’ to ‘good’ introduction, method and results sections. Overall, randomised controlled trials (RCTs) exhibited strengths in areas of methodology, data analysis and results, with some studies achieving consistently high ratings across all assessed components, such as methodological rigour, ethical consideration and generalisability of findings (Ezeh et al., 2023; Yi et al., 2024). However, certain RCTs received lower scores in areas of ethics, bias and sampling, exposing potential limitations in their methodological execution and sample representativeness (Kymissis et al., 1996; Tibbetts and Stone, 1990). Although sampling details regarding age, gender, race and context were generally adequate, sample size emerged as a recurrent limitation, likely reducing generalisability of findings and diminishing statistical power. It is noteworthy that the assessment tool used (Hawker et al., 2002) did not allow for a comprehensive evaluation of sample size. Several cohort and cross-sectional studies exhibited weaknesses in sampling, ethical considerations and data analysis, affecting the reliability and generalisability of their results.
Quality assessment of original research studies.
Case studies
Of 90 identified eligible studies, the remaining 67 used case study methodology to examine art therapy interventions (Supplementary Table 1). Similar to the original research studies, most took place within inpatient child and adolescent psychiatric units (n = 34), in addition to outpatient community mental health settings (n = 14), residential treatment centres (n = 4), schools (n = 4), juvenile justice and forensic facilities (n = 2), private practice (n = 2) and specially designed programmes or camps for young people (n = 2).
Case study methodology most often entailed descriptive analysis of a single young person (n = 35) or multiple case study participants (n = 19), as compared with a group analysis (n = 13). Most studies (n = 45) focused on young people with comorbid mental health conditions, such as adjustment disorder, mood and anxiety disorders, eating disorders, conduct and behavioural disorders, personality disorders, schizophrenia or psychotic spectrum disorders, and neurodevelopmental disorders (co-occurring with a mental health condition). Fewer case studies focused on a single diagnosis or presentation (n = 22), most commonly conduct or behavioural disorders (n = 5) or developmental trauma (n = 5).
Art therapy interventions again varied substantially in type, format and duration. Most interventions were delivered on an individual basis (n = 42). Theoretical frameworks or guiding principles were unclear or unspecified in many interventions. Overall, older studies utilised predominantly psychoanalytic or psychodynamic approaches to intervention and interpretation (e.g. Allie, 1981; Naumburg, 1945). More recent studies have continued to utilise psychodynamic approaches to art therapy (e.g. Hanvey and Tepper-Lewis, 2019), alongside more modern and alternative theoretical frameworks including attachment-informed art therapy (Cunningham and Page, 2001; Kozlowska and Hanney, 2001), ecopsychology (Wardle, 2023), land art (Bourry and Barbe, 2012), somatic experiencing (Hetherington and Gentile, 2022) and trauma processing methods (Howie et al., 2002; Mallay, 2002), as well as transcultural family therapy (Roijen, 1991).
Most interventions took a multidisciplinary and multimodal intervention approach, particularly within hospital-based settings. Art therapy interventions were frequently delivered by a trained art therapist alongside other health professionals including psychiatry, psychology, social work, case management intervention and educational therapy (e.g. Kozlowska and Hanney, 2001; McGann, 1999; Rupa et al., 2014). Provision of art therapy often took place in conjunction with family-based treatments, medication management and talk-based psychotherapies such as CBT (Coşkunlu et al., 2018; Kozlowska and Hanney, 2001; Mazloomian and Moon, 2007). Some interventions also offered additional treatment components such as bullying intervention (e.g. Buchan, 2009), behaviour management strategies (Hetherington and Gentile, 2022; Potash, 2009) and other creative therapies such as music therapy, play therapy and psychodrama (Diamond-Raab and Orrell-Valente, 2002; Mazloomian and Moon, 2007; Sikes and Kuhnley, 1984). Session frequency ranged from 3 to 4 times per week to monthly, with session duration from 30 to 90 minutes. The longest case study was conducted over a 3-year period (Steinhardt, 1995).
Outcome measures were heterogeneous, precluding clear synthesis. Qualitative measures were most commonly used, involving clinical observations undertaken by the art therapy interventionist. Only three case studies used validated qualitative coding methods or frameworks; all of which used a phenomenological coding approach focused on identifying themes in participant artwork, verbal dialogue and semi-structured interviews (Bourry and Barbe, 2012; Van Lith, 2008; Wyder, 2019). Four studies used art-based assessment measures to examine efficacy of art therapy. This included the Levels of Emotional Awareness Scale (Barth and Klosinski, 2007) to measure emotional awareness, an Observation Grid to identify mental activity and pictorial mediation in childhood psychosis (Calestrémé et al., 2016), the Body Image Projective Drawing Test to assess unconscious internal processes (Kim and Ki, 2014) and the Face Stimulus Assessment Task, a projective drawing assessment (Robb, 2002). Quantitative methodologies were rarely used to evaluate outcomes of art therapy interventions. Only four case studies used validated questionnaires to assess self-reported mental health outcomes, all of which reported benefits of art therapy. This included reductions in depressive symptom severity (Child Depression Inventory, Coşkunlu et al., 2018), post-traumatic stress symptoms (Impact of Events Scale-Revised, Wyder, 2019), alexithymia and somatisation symptoms (Alexithymia Scale Questionnaire and Symptom Checklist Revised, Kim and Ki, 2014) and improved self-esteem (School Form of Coopersmith Self-Esteem Inventory, Stanley and Miller, 1993).
Overall, outcomes were largely positive across the included case studies. Positive gains were reported in 54 of 67 studies, including improvements in emotional awareness and expression, interpersonal skills, cognitive skills and occupational functioning. Improvements in mental health outcomes were also reported, including most commonly reductions in post-traumatic stress symptoms (Harnden et al., 2004; Hetherington and Gentile, 2022; Kozlowska and Hanney, 2001; Peake, 1987; Potash, 2009; Stanley and Miller, 1993; Waller, 2006; Wardle, 2023). Reductions were also observed in symptoms of anxiety (e.g. Buchan, 2009; Calestrémé et al., 2016), disordered eating (Diamond-Raab and Orrell-Valente, 2002; Lindinger and Karwautz, 2016), depression (Coşkunlu et al., 2018; Rupa et al., 2014), oppositional and behavioural difficulties (e.g. Fliegel, 2000; McGann, 1999), psychotic spectrum symptoms (e.g. Atlas et al., 1992; Calestrémé et al., 2016), somatisation symptoms (Kim and Ki, 2014), self-harming behaviour (e.g. Briks, 2007; Coşkunlu et al., 2018) and suicidal ideation and attempts (e.g. Coşkunlu et al., 2018; Diamond-Raab, Orrell-Valente, 2002). Unclear or mixed outcomes were reported in the remaining 13 studies across varied outcomes. Heterogeneity in intervention components, frameworks and intervention dosage, duration and format preclude distinction of particular components of art therapy contributing to effectiveness. Multimodal interventions also limit disentangling impacts of art therapy intervention from broader systemic or contextual treatments.
Around half the studies reported on acceptability (n = 34). Most indicated high acceptability and of positive impressions and experiences of art therapy (n = 24). This was inferred from clinical observations of participant engagement and enthusiasm, self-reports of high satisfaction and enjoyment, staff feedback on increased engagement (e.g. Barth and Klosinski, 2007), improved self-regulation (e, g, Coşkunlu et al., 2018), positive interaction with varied art materials (e.g. Howie et al., 2002) increased independent art-marking time (e.g. Wolf, 1975) and strong therapeutic rapport (e.g. Moon, 1999). Ten case studies reported negative or mixed acceptability, most commonly relating to poor participant engagement or participation (McGann, 1999), limited parental capacity in family-based art interventions (Nielsen et al., 2021; Roijen, 1991), limited motivation, resistance or premature termination of participation (George and Kasinathan, 2014; Hanvey and Tepper-Lewis, 2019; Horovitz, 1983; Powers and Langworthy, 1978; Raghuraman, 2000; Robb, 2002) or ‘therapy-interfering behaviours’ such as disrupting peers or engaging in conflictual behaviour (Bennink et al., 2003). Overall, this supports original research studies demonstrating generally positive impressions and engagement with art therapy interventions.
Discussion
Clear patterns of effectiveness have emerged in art therapy interventions, despite variation in methodological approach and intervention structure. Multiple original research papers, predominantly randomised control trials, reported statistically significant reductions in PTSD symptom severity (e.g. Anazor et al., 2023; Ezeh et al., 2023; Zhang et al., 2023), with case study evidence mirroring this finding (e.g. Harnden et al., 2004; Hetherington and Gentile, 2022; Wardle, 2023). Studies also demonstrated effectiveness for emotional regulation and reducing acute distress. This was evidenced by reduced anger, greater emotional control (Persons, 2009), a statistically significant reduction in restrictive practices (Versitano et al., 2024b), as well as reductions in suicidal ideation (Liu et al., 2023), and self-injurious behaviour (Coşkunlu et al., 2018; Edan and Knecht-Favrod, 2011; Persons, 2009). Original research studies also indicated improved self-awareness (Parkinson and Whiter, 2016; Wolk and Bat Or, 2023), confidence (Nielsen et al., 2019; Parkinson and Whiter, 2016) and significantly reduced depression (Blomdahl and Goulias, 2024; Yi et al., 2024) and anxiety symptoms (Coles and Harrison, 2018; Pretorius and Pfeifer, 2010; Tibbetts and Stone, 1990).
Acceptability of art therapy interventions was consistently demonstrated, with high rates of attendance to art therapy sessions (Blomdahl and Goulias, 2024; Versitano et al., 2024a), and minimal attrition reported (e.g. Pretorius and Pfeifer, 2010; Yi et al., 2024). Many young people expressed enjoyment of art therapy interventions (e.g. Blomdahl and Goulias, 2024; Versitano et al., 2024a) and a preference for art therapy relative to verbal therapies (Diamond-Raab, Orrell-Valente, 2002; Gmitrowicz et al., 2012; Versitano et al., 2024a). Despite evidence predominantly supporting the acceptability of art therapy, some studies reported feasibility challenges regarding recruitment and retention in acute mental health settings where discharges were difficult to anticipate (Gatta et al., 2014; George and Kasinathan, 2014; Lyshak-Stelzer et al., 2007). Some case studies also reported challenges with participant engagement or motivation (e. g. McGann, 1999; Robb, 2002).
Art therapy was predominantly found to be effective in reducing symptom severity, while also being an enjoyable therapeutic modality with high levels of acceptability reported. These findings support those of a recent systematic review of the effectiveness of art psychotherapy for children and adolescents with mental health conditions (Braito et al., 2022) which found benefits for young people with PTSD symptoms. In addition, a scoping review of the use of visual arts in hospital environments, which included art therapy studies, found that arts and art therapy enhanced well-being and improved communication processes in health settings (Ullán and Belver, 2021). While both arts-and-health and art therapy interventions provide benefits, it is important to distinguish between the psychotherapeutic practice of art therapy and diversional arts-and-health activities, as they are frequently conflated, diminishing the strengths of each modality (Van Lith and Spooner, 2018).
Within the present systematic review, RCTs demonstrated that art therapy was a comparatively more beneficial intervention for young people than arts-and-crafts control groups (Lyshak-Stelzer et al., 2007), or freeform discussion control groups (Kymissis et al., 1996). This is particularly salient when working with young people experiencing severe or acute mental health challenges, as art therapists’ capacity to hold and contain complex, and often distressing, emotional and visual material in-session is supported by their specialised clinical training in the intersection of arts and psychotherapy (Rubin, 2011; Van Lith and Spooner, 2018). With 18 of the 23 original research studies conducted by trained art therapists, current findings are primarily applicable to art therapist-delivered treatments.
A systematic narrative review on art therapy for psychosocial problems in children and adolescents (Bosgraaf et al., 2020) found similar variations in art therapy interventions offered, as in our review. Bosgraaf et al. (2020) concluded that this represents a responsiveness of art therapists, and their capacity to flexibly adapt to the clinical needs and circumstances of young people, therefore providing positive outcomes. Art therapy is sometimes critiqued for its lack of manualised or structured (and therefore readily replicable) treatments. Art therapists are trained in client-focused work and deliver interventions tailored to specific client needs, requiring advanced therapeutic skills and sensitivities. This is a strength rather than deficit of the modality, consistent with evidence-informed practice that incorporates client perspectives and practice wisdom alongside scientific evidence (Alla and Joss, 2021; Psychotherapists and Counsellors Federation of Australia [PACFA], 2019).
Our review highlights the value of art therapy for young people experiencing severe or acute mental health conditions. Art therapy is sometimes misconceived as a diversional intervention or secondary treatment. However, current findings suggest it is an effective intervention which young people deem enjoyable and helpful. Therefore, art therapy services delivered by qualified art therapists could be established in more services which support young people who are experiencing severe or acute mental health challenges. This body of evidence is particularly strong in the treatment of PTSD symptoms. While this may not be possible in certain geographic locations due to workforce constraints, interactive media-based art therapy interventions have also demonstrated their effectiveness (e.g. Anazor et al., 2023; Liu et al., 2023; Zhang et al., 2023)
Several limitations warrant consideration. Non-English studies were included and translated using Google Translate which may affect the reliability of reported findings in those studies (Jackson et al., 2019). Furthermore, the review process included all forms of research including case studies. While qualitative research, particularly utilising case studies, has often been the preferred method of art therapy research historically, this poses challenges to generating evidence on effectiveness and acceptability, as cases are often selectively presented.
Future research on art therapy with young people experiencing severe and/or acute mental health conditions should aim to increase methodological rigour across the range of quantitative, mixed-method and qualitative approaches. This includes conducting further gold-standard evidence-based evaluations, particularly RCTs, which incorporate longitudinal follow-up assessments to discern intervention sustainability for a transdiagnostic cohort in acute mental health settings. Further research is also needed on the physiological effects of art therapy on mental health (Czamanski-Cohen and Weihs, 2016), examining potential mediators of effects including intervention structure, dose, delivery mode and outcomes assessed alongside confounding factors such as provision of multicomponent multidisciplinary interventions. A component analysis to identify the ‘effective ingredients’ of art therapy would provide further clarity. Future research may also examine condition-specific RCTs to strengthen evidence-based evaluations in areas with limited research to date, e.g., with obsessive compulsive disorder (Dyason et al., 2022). Future art therapy research should also ensure diversity representation, inclusivity and cultural sensitivity in its practice (Hughes et al., 2024), as this was under-reported or absent from many reviewed studies.
Conclusion
Art therapy has significant therapeutic effects for young people who may be experiencing severe emotional distress. The novelty of this review lies in its specific focus on severe and acute mental health conditions for children and young people. This is pertinent given increasing trends in acute mental health presentations including self-harm and suicidal ideation within this population (Sara et al., 2023). This review identified effectiveness of art therapy in reducing symptoms of PTSD, depression, anxiety and suicidal ideation. Art therapy was also found to improve emotional regulation, confidence, self-awareness, distress tolerance, self-expression, interpersonal effectiveness, hope and resilience. Effectiveness across a range of clinical diagnoses, settings and art therapy intervention types reflects the responsive capacity of art therapy to adapt to the specific needs of young people it supports (Bosgraaf et al., 2020). Art therapy was a widely accepted intervention, with young people reporting high enjoyment, engagement and satisfaction with this therapeutic modality. Previous reviews have not examined acceptability (Braito et al., 2022; Cohen-Yatziv and Regev, 2019; Moula, 2020) despite this being a key consideration in the design, evaluation and implementation of healthcare interventions (Sekhon et al., 2017), further enhancing the value of this review and of art therapy intervention for young people. Art therapy services were found to be in settings which provide mental health care for young people with acute or severe mental health conditions, including hospitals, schools, juvenile justice and community mental health settings. This review highlights a strong and growing evidence base to support the provision of art therapy in the context of acute or severe mental health conditions in children and young people.
Supplemental Material
sj-docx-1-anp-10.1177_00048674251361731 – Supplemental material for Art therapy with children and adolescents experiencing acute or severe mental health conditions: A systematic review
Supplemental material, sj-docx-1-anp-10.1177_00048674251361731 for Art therapy with children and adolescents experiencing acute or severe mental health conditions: A systematic review by Sarah Versitano, Stephanie Tesson, Chae-Weon Lee, Sheridan Linnell and Iain Perkes in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors acknowledge all the young people who participated in the studies which were reviewed for this research, and the Health Education and Training Institute (HETI) who provided funding to undertake this research as part of the Mental Health Research Award. We also wish to acknowledge Professor Neeraj Gill for his guidance and support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The first author was partially funded by the Health Education and Training Institute (HETI) Mental Health Research Award.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.