
Abstract
Objectives:
The rate of mental health services provided to children and young people is increasing worldwide, including in Australia. The aim of this study was to describe patterns of hospital and ambulatory mental health service use among a large population cohort of adolescents followed from birth, with consideration of variation by age, sex and diagnosis.
Methods:
Characteristics of services provided for children with mental disorder diagnoses between birth and age 17.5 years were ascertained for a population cohort of 85,642 children (52.0% male) born between 2002 and 2005, from ‘Admitted Patients’, ‘Emergency Department’ and ‘Mental Health Ambulatory’ records provided by the New South Wales and Australian Capital Territory Health Departments.
Results:
A total of 11,205 (~13.1%) children received at least one hospital or ambulatory health occasion of service for a mental health condition in the observation period. More than two-fifths of children with mental disorders had diagnoses spanning multiple categories of disorder over time. Ambulatory services were the most heavily used and the most common point of first contact. The rate of mental health service contact increased with age across all services, and for most categories of mental disorder. Girls were more likely to receive services for mental disorders than boys, but boys generally had an earlier age of first service contact. Finally, 3.1% of children presenting to mental health services experienced involuntary psychiatric inpatient admission.
Conclusions:
The extent of hospital and ambulatory-based mental healthcare service among children emphasises the need for primary prevention and early intervention.
The number of young people seeking treatment for mental disorders is rising worldwide (Lawrence et al., 2015; Lipson et al., 2019; Nishi et al., 2019). In Australia, recent evidence indicates that expenditure on child and adolescent mental health services increased by an average of 3.6% per year between 2015 and 2016 and 2019 and 2020 (Brazel et al., 2023); between 1998 and 2013 and 2014, the proportion of young people who received treatment for mental health problems more than doubled (from 31.2% to 68.3%; Lawrence et al., 2015). Children with mental disorders in Australia most frequently visit general practitioners, psychologists and psychiatrists, with additional support obtained via school, telephone and online services for mental health problems, with only a small proportion (6.2%) accessing emergency or hospital-based services (Lawrence et al., 2015). Understanding which hospital-based services are most frequently accessed for mental health treatment by children in Australia, according to age, sex and diagnosis, could inform early intervention and prevention efforts.
Hospital- (including inpatient, outpatient and emergency services) and ambulatory-based treatment of mental disorders increases with age during childhood and adolescence (Bardach et al., 2014; Segal et al., 2017; Torio et al., 2015; Williamson et al., 2018). Young people with mental illness tend to experience longer episodes of care during emergency department presentations (relative to physical health issues) and have a higher rate of re-presentation, especially when presenting with self-harm or suicidal ideation (Nash et al., 2021; Patricia et al., 2022). More broadly, there has been an increase in mental health presentations to emergency departments over time (Hiscock et al., 2018; Tran et al., 2019), alongside increasing rates of hospitalisation for suicidal ideation and self-harm in young people (Plemmons et al., 2018). Psychotic and eating disorders especially, have been linked to extended periods of care in inpatient settings (Stewart et al., 2014; Tulloch et al., 2011). Individuals with comorbid mental disorders are also more likely to use services more frequently and over a longer period of time (Burgess et al., 2009; Yong et al., 2013), while people with psychotic disorders (particularly men) are most likely to be admitted to a psychiatric unit involuntarily (Feeney et al., 2019; Hotzy et al., 2019). However, there has yet to be a comprehensive investigation of the characteristics and cumulative incidence of children receiving hospital- and ambulatory-based mental healthcare in Australia. Most research to date has focused on presentations to a single health service (usually the emergency department), for a single type of disorder, or among specific subpopulations (e.g. Aboriginal and/or Torres Strait Islander peoples). Various studies also cover different date or age ranges, making it challenging to compare mental health service use across studies. Evidence-based allocation of resources for mental health treatment of children and adolescents would be aided by an integrated epidemiological overview of hospital and ambulatory mental health service use.
The goal of this study was therefore to describe patterns of hospital and ambulatory-based healthcare provided for the treatment of mental disorders during childhood and adolescence, for a population-based cohort of >85,000 children followed from birth to 17–18 years of age. Specific aims were to determine (1) the cumulative incidence of mental disorders according to sex, diagnosis and the type of health service contact, (2) the days of healthcare received for mental disorder according to age, diagnosis and the type of health service accessed, (3) the average age and point of first contact with mental disorder, (4) the rates of comorbidity among the different psychiatric disorders treated and (5) the rate and duration of involuntary hospital admissions according to age, sex and diagnosis.
Method
Study cohort
Participants were 85,642 children with data available from New South Wales (NSW) or Australian Capital Territory (ACT) health records (described below) in the Wave 3 linkage of the NSW Child Development Study (Green et al., 2024). Health records subsequent to each participant’s 18th birthday were excluded, as not all children had reached 18 years of age at the time of record-linkage on 31 March 2021 (median age at this date = 17.5 years). Ethical approval was provided by the NSW Population and Health Services and ACT Human Research Ethics Committees (HREC/18/CIPHS/49), with relevant data custodian approvals. This research was conducted under the ‘waiver of consent’ provision of the National Statement of Ethnical Conduct in Human Research (National Health and Medical Research Council, 2023).
Measures
Mental health service use
Health service contacts for primary mental disorder diagnoses were recorded in any one of the following three record sets: the Admitted Patient Data Collection (APDC; records from January 3 2002 to 31 March 2021 supplied by NSW and ACT), Emergency Department Data Collection (EDDC; records from 8 January 2005 to 31 March 2021 supplied by NSW and ACT), or the NSW Mental Health Ambulatory (MH-AMB) data collection (records from 27 November 2002 to 31 December 2020, which include care provided to non-admitted patients, including mental health day programs, psychiatric outpatient and community outreach services).
Demographics
Each child’s sex was determined via consensus across all available records in the NSW-CDS (Child Development Study). The child’s age was determined using the month and year of birth available in the NSW Registry of Births, Deaths and Marriages (or other records where available) and separated into four time periods between birth and 17 years: 0–5 years, 6–11 years, 12–14 years and 15–17 years.
Mental disorder indicators
Twelve binary indicators, corresponding to the chapter blocks of the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification (ICD-10-AM) Chapter V, were created to signify health service contact in relation to specific mental disorders occurring on at least one occasion during the observation period in addition to a single indicator for self-harm (X60-X84, T14.19, Y87.0) and/or suicidal ideation R45.851 (R45.81 for ICD-10-AM). The 12 ICD-10-AM chapter blocks included organic disorders (F00-F09); substance use disorders (F10-F19); schizophrenia, schizotypal and delusional disorders, hereafter referred to simply as ‘schizophreniform disorders’ (F20-F29); mood disorders (F30-F39); neurotic disorders (F40-F48); physiological disturbance (e.g. eating) disorders (F50-F59); personality disorders (F60-F69); intellectual disability (F70-F79); developmental disorders (F80-F89); behavioural (childhood onset) disorders (F90-F98) and mental disorders not otherwise specified (NOS; F99). These indicators were generated from primary diagnoses and were not mutually exclusive (i.e. a child could be recorded as having contact for more than one type of mental disorder in each observation period).
Number of mental disorders
The number of mental disorder categories for which each child received a diagnosis was derived by summing 11 of the 12 binary indicators for the ICD-10 C-AM chapter (V) blocks (omitting ‘mental disorders not otherwise specified’) plus suicidal ideation/self-harm. For children with at least one primary diagnosis of a mental disorder in the observation period, both primary and secondary diagnoses were included in the calculation of this variable to capture concurrent disorder comorbidity.
Days of care
The number of days receiving inpatient and ambulatory mental health care for all primary diagnoses of mental disorder (including NOS) was derived across all health service record sets, and separately for each type of mental disorder diagnostic category. For APDC and EDDC records, this reflected the cumulative number of days between each admission and discharge (inclusive) date, for each child. For MH-AMB records, the number of days in care was derived from the number of unique dates on which mental health services were accessed. In combining days of care received across datasets (APDC, EDDC and MH-AMB), only unique dates of care were counted. Days spent in involuntary care (available in APDC records only) were derived by summing the number of days spent in involuntary care for each person, across presentations.
Analyses
All analyses were performed in RStudio v.1.3.1093 using R v.4.0.3. Odds ratios and 95% confidence intervals for the associations between female sex and diagnosis of mental disorders were examined using logistic regression analyses among all children (n = 85,642), accounting for age at time of record linkage (March 2021). Sex differences in age of first service contact for each mental disorder category were examined using Mann–Whitney tests. Mental health service contact was described in terms of the number of children receiving care, the total number of days of care, according to disorder category, age band and record set, for the subcohort identified with at least one mental disorder diagnosis (n = 11,205). The relationship between the type of first mental health contact and the median age at the time of first contact was assessed using a Kruskal–Wallis rank sum test using the psych package (Revelle, 2018), with post hoc analysis of each pairwise comparison evaluated using pairwise Wilcox tests, applying a Benjamini–Hochburg correction. The extent of cumulative comorbidity experienced by children with each category of disorder was reported as the number and percentage of children diagnosed with one, two, three or four or more disorders, for the subset of children who had at least one mental disorder diagnosis other than ‘Mental illness NOS’ (n = 8179). Finally, for the subset of children who experienced an involuntary admission for psychiatric care (n = 353), negative binomial mixed modelling was performed using the lme4 package (Bates et al., 2015) to evaluate the relationship between mental disorder type and the number of days spent in involuntary psychiatric care, treating each child as a mixed factor (as each individual may have had hospitalisations for multiple categories of mental disorders). Negative binomial analysis was implemented given the overdispersion (right-skewed distribution) of the number of days of involuntary care. A Wald chi-square test was used to evaluate the overall fixed effect of disorder type on the number of days of involuntary care received. Estimated marginal means and 95% confidence intervals were derived from the negative binomial model using the emmeans package (Lenth, 2022). Means were considered significantly different when their corresponding 95% confidence intervals did not overlap. All figures were generated using the ggplot2 package (Wickham, 2016).
Results
Descriptive statistics
There were 11,205 children (13.1% of the cohort; 5238 male) identified with a primary mental disorder diagnosis, for whom clinical and demographic characteristics are displayed in Table 1. Contact with more than one type of health service was evident for 36.5% (n = 4088) of these children, with 10.7% (n = 1198) having contact with all three types of service for mental health care (Figure 1). The most heavily utilised service was Mental Health Ambulatory (n = 9223). There was a subtle, yet significant, difference (t[df = 10,892]= 11.453, p < 2.2 × 10−16) in the average age of boys (M = 17.57, SD = 0.39) and girls (M = 17.49, SD = 0.37) at the time of record linkage, among the subcohort identified with at least one service contact for primary mental disorder.
Demographic and clinical characteristics for all children with a primary mental disorder diagnosis in health records (n = 11,205).
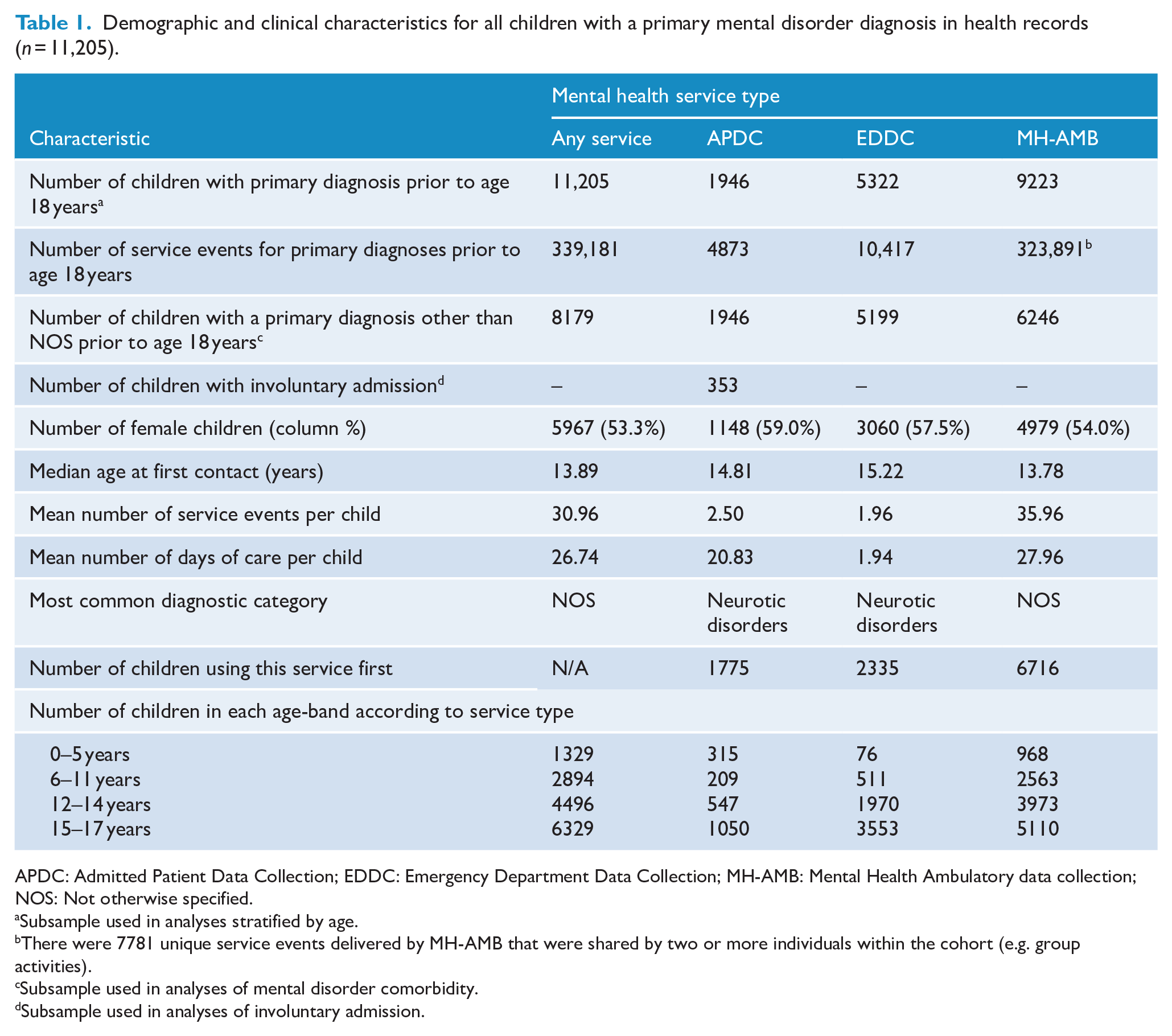
APDC: Admitted Patient Data Collection; EDDC: Emergency Department Data Collection; MH-AMB: Mental Health Ambulatory data collection; NOS: Not otherwise specified.
Subsample used in analyses stratified by age.
There were 7781 unique service events delivered by MH-AMB that were shared by two or more individuals within the cohort (e.g. group activities).
Subsample used in analyses of mental disorder comorbidity.
Subsample used in analyses of involuntary admission.
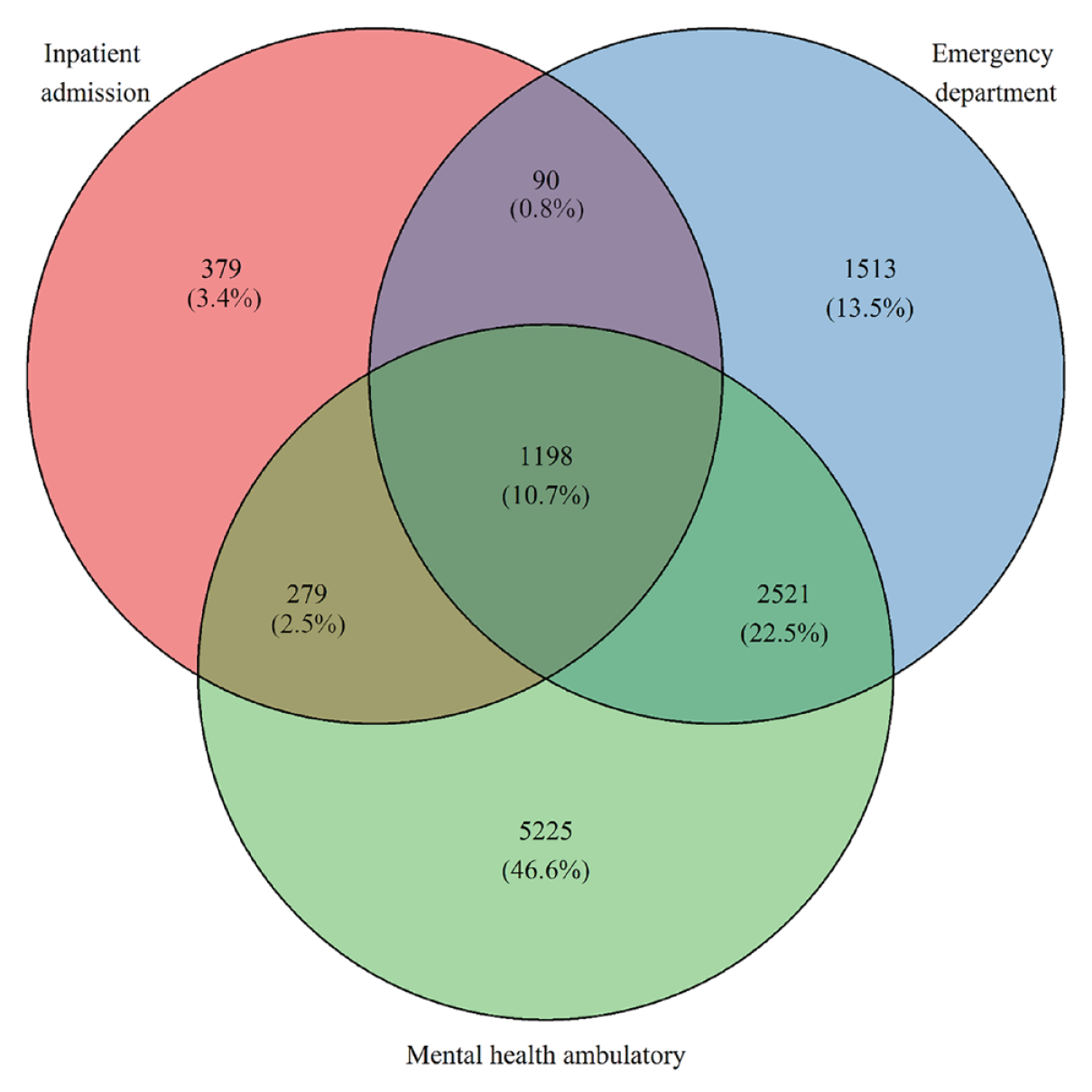
Number of children accessing single and multiple types of health services for mental health treatment between ages 0 and 17 years (n = 11,205).
Cumulative incidence of mental disorders
The cumulative incidence of recorded mental disorders according to type of health service is presented in Table 2. The most common confirmed diagnosis category across all service types was neurotic disorder, followed by self-harm and/or suicidal ideation, behavioural (childhood onset) disorders and mood disorders. There were notable differences in the most frequently recorded diagnoses in each type of health service. For example, diagnoses of ‘mental disorder NOS’, mood and behavioural (childhood onset) disorders were most common in MH-AMB data; whereas self-harm/suicidal ideation, organic and substance use disorders were most common in the EDDC; and developmental disorders were most common in the APDC.
Cumulative incidence of each category of primary mental disorder according to health service type among the cohort of 85,642 children followed from birth to ~17 years.
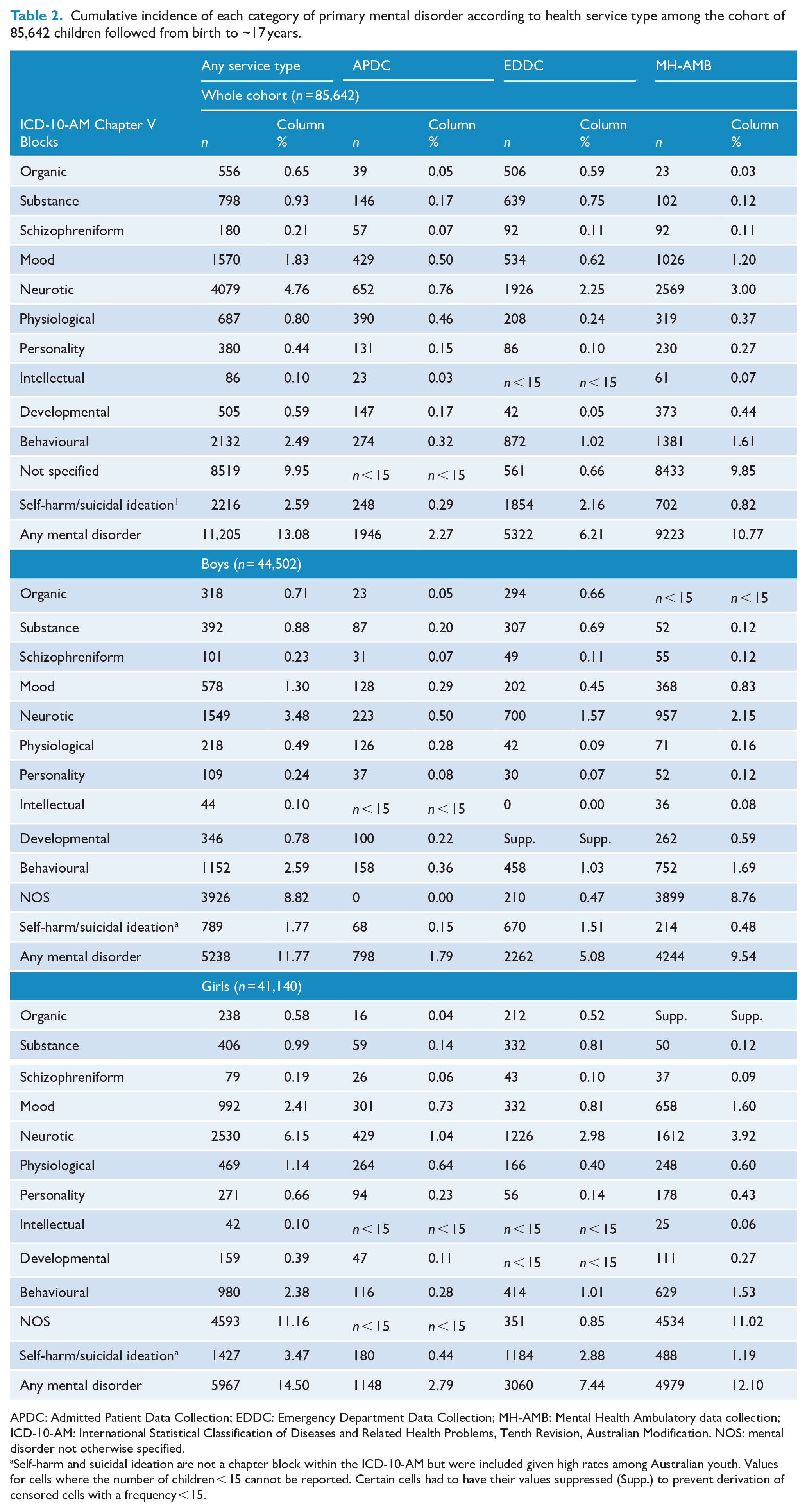
APDC: Admitted Patient Data Collection; EDDC: Emergency Department Data Collection; MH-AMB: Mental Health Ambulatory data collection; ICD-10-AM: International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification. NOS: mental disorder not otherwise specified.
Self-harm and suicidal ideation are not a chapter block within the ICD-10-AM but were included given high rates among Australian youth. Values for cells where the number of children < 15 cannot be reported. Certain cells had to have their values suppressed (Supp.) to prevent derivation of censored cells with a frequency < 15.
Rates of mental health service use according to sex, age, diagnosis and service type
Girls (14.5%) were more likely to access health services for mental disorders overall, relative to boys (11.8%), and this was particularly evident for personality, mood, neurotic, physiological disorders and self-harm (Table 3). Conversely, boys were more likely than girls to receive health services for developmental and organic disorders. Girls were no more likely than boys to experience behavioural disorders, intellectual disability or schizophreniform disorders. In terms of age of onset, boys presented earlier than girls overall for mental health services, and, in particular for neurotic, physiological disturbance, behavioural and mental disorders not otherwise specified (Table 3).
Sex differences and average age of onset for different categories of mental disorder diagnoses. a
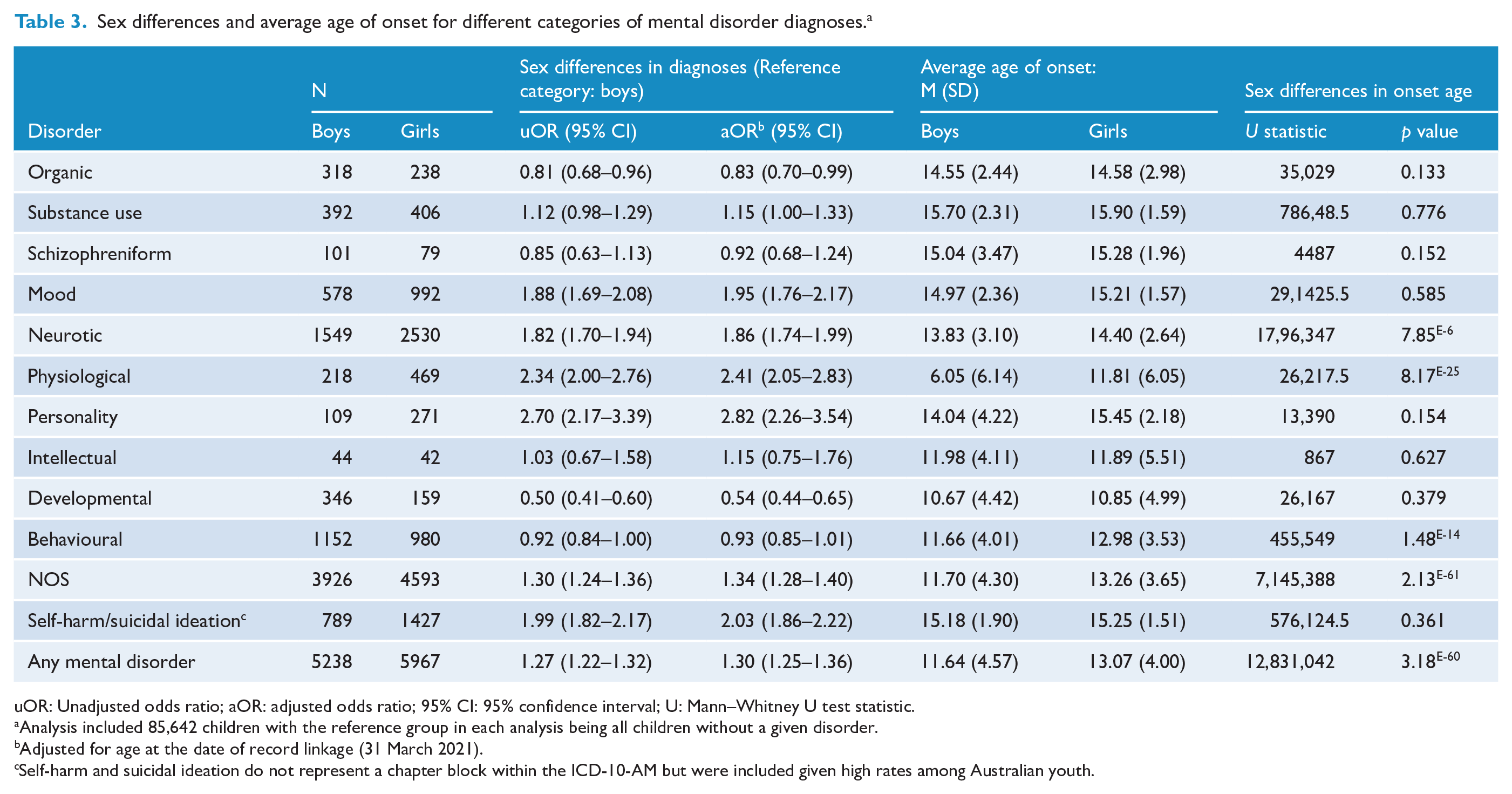
uOR: Unadjusted odds ratio; aOR: adjusted odds ratio; 95% CI: 95% confidence interval; U: Mann–Whitney U test statistic.
Analysis included 85,642 children with the reference group in each analysis being all children without a given disorder.
Adjusted for age at the date of record linkage (31 March 2021).
Self-harm and suicidal ideation do not represent a chapter block within the ICD-10-AM but were included given high rates among Australian youth.
Progressively more children presented for services with increasing age, evident in the number of days of care overall (Table 4, and Supplementary Figures 1 and 2). Adolescence (age 12–17 years) was marked by particularly rapid increases in the number of children admitted to hospital with self-harm/suicidal ideation, neurotic and mood disorders. In contrast, the number of children admitted to hospital (and the associated number of days of care) for physiological disturbance disorders (i.e. predominantly sleep and eating disorders) followed a quadratic trend characterised by a peak in early childhood (driven by sleep disorders, see Supplementary Table 1), a decline in middle childhood and an increase in adolescence (driven by eating disorders, see Supplementary Table 1). Treatment in the emergency department was, by contrast, distinguished by a sharp increase in the number of children presenting for neurotic disorders and self-harm in adolescence. Finally, ambulatory services had the highest rate of ‘mental disorders NOS’, which increased gradually over the course of childhood and adolescence.
Number of children diagnosed and total days of care for each mental disorder recorded as a primary diagnosis, according to health service type and ICD-10 Chapter V blocks, by age band. a
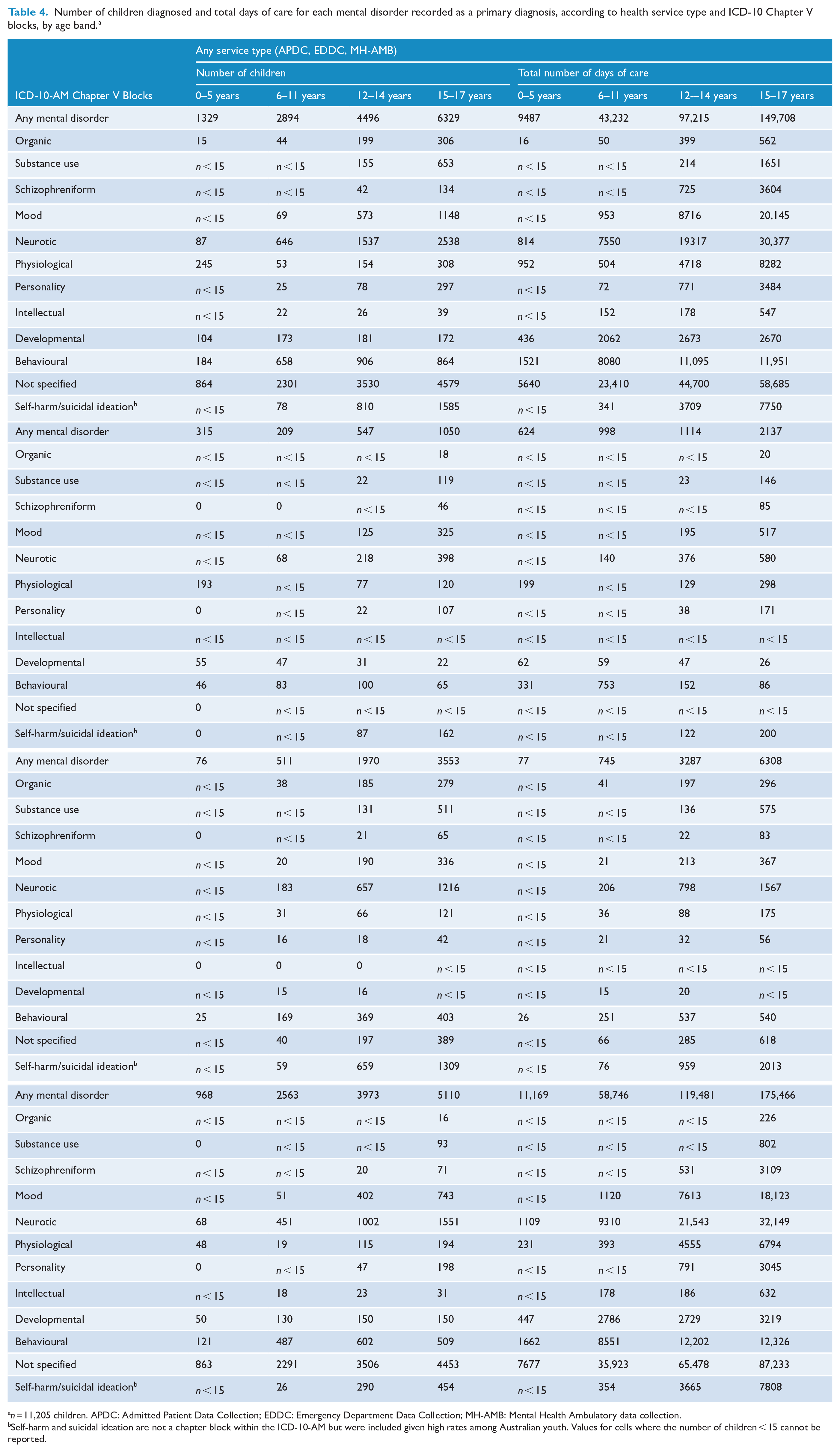
n = 11,205 children. APDC: Admitted Patient Data Collection; EDDC: Emergency Department Data Collection; MH-AMB: Mental Health Ambulatory data collection.
Self-harm and suicidal ideation are not a chapter block within the ICD-10-AM but were included given high rates among Australian youth. Values for cells where the number of children < 15 cannot be reported.
Type of health service at time of first contact for mental disorder treatment
Mental health ambulatory services was the type of health service most commonly accessed for a first mental disorder treatment, while hospital admissions were the least common (Table 5). Compared with children who first accessed multiple types of health services on the same day on the date of first contact for mental disorder treatment, the median age of first presentation was earlier among admitted patients and those in contact with mental health ambulatory services (Kruskal–Wallis chi-square = 1566.2, df = 3, p < 2.2e-16), but not among those who first presented to the emergency department (p = 0.10). Children whose first mental health service contact was as an inpatient tended to have their first contact at a younger age (prior to 2 years of age; Figure 2). Among children who presented to multiple services on the date of their first mental health service contact, attendance at the emergency department and mental health ambulatory services was the most common combination (n = 883), followed by emergency and admitted patient treatment (n = 158); a total of 111 children presented to all three services on the same day of their first treatment for mental disorder.
Frequency of children with first contact for mental health treatment recorded in each health service type, according to the number of services used overall. a
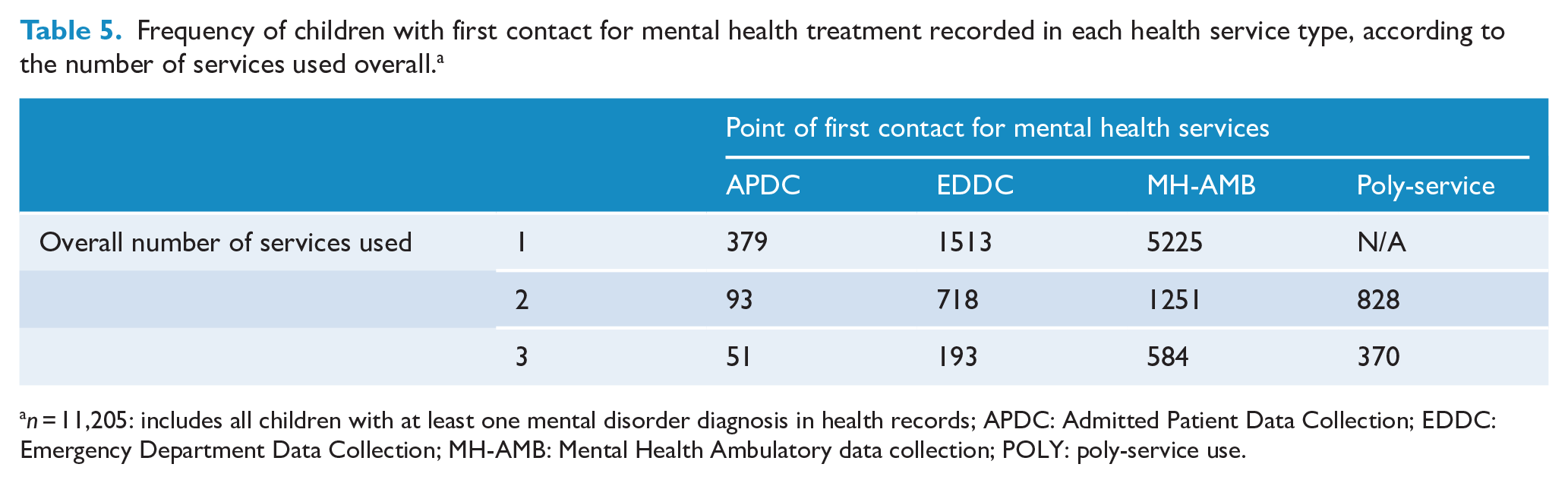
n = 11,205: includes all children with at least one mental disorder diagnosis in health records; APDC: Admitted Patient Data Collection; EDDC: Emergency Department Data Collection; MH-AMB: Mental Health Ambulatory data collection; POLY: poly-service use.
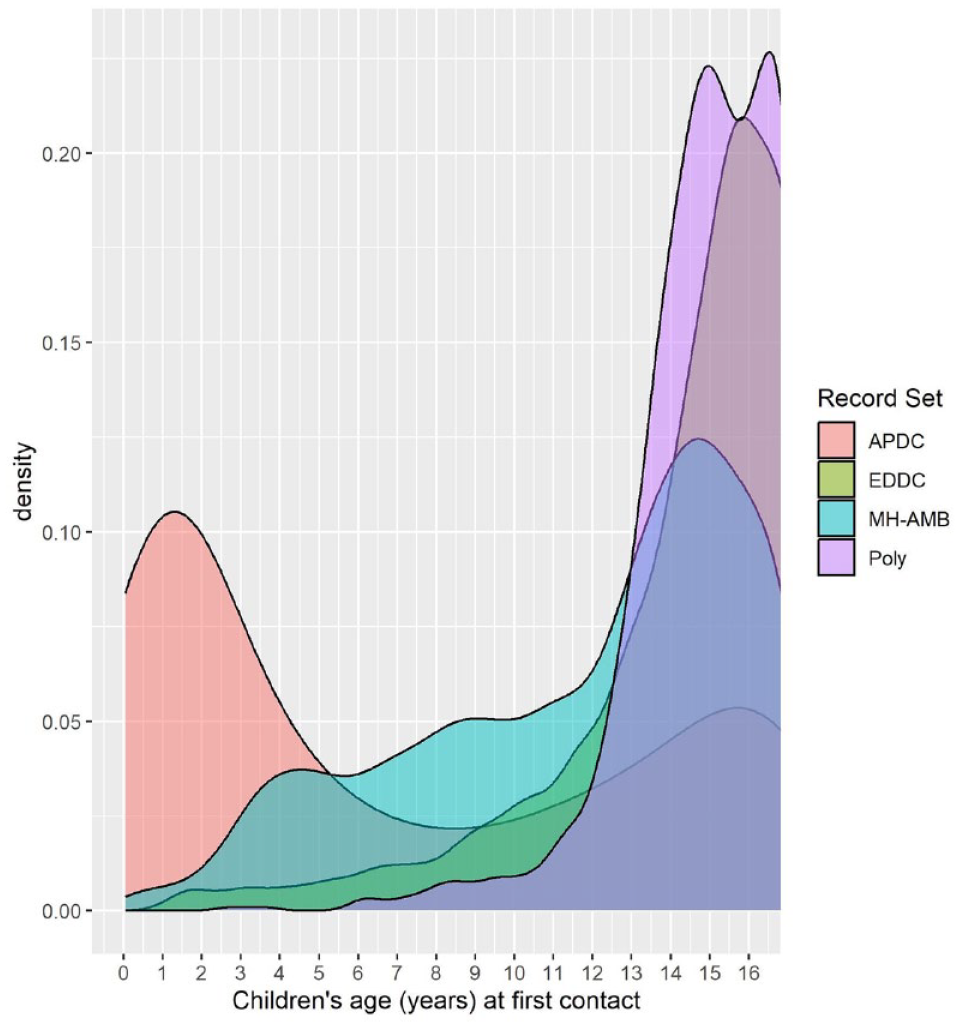
Distribution of children’s age (years) at time of first contact according to the type of health service that was the first-accessed service1.
Cumulative comorbidity between mental disorders
There were 8179 children who had a mental disorder other than ‘mental disorders NOS’, and at least 3576 (43.7%) who received diagnoses in multiple categories, either across multiple presentations or within a single presentation as concurrent secondary diagnoses (Table 6 and Supplementary Figure 3). Children diagnosed with personality disorders had the highest degree of cumulative mental disorder comorbidity among categories (87.9), followed by children with schizophrenia (86.1%) and mood (79.5%) disorders. Only organic, physiological disturbance and substance-use disorder categories were more likely to occur in isolation (62.4%, 54.0% and 51.6%, respectively) than in combination with another type of mental disorder.
Number (%) of children1 with lifetime diagnoses of 1, 2, 3 or 4 or more primary or secondary mental disorder diagnoses grouped according to ICD-10 Chapter V blocks.
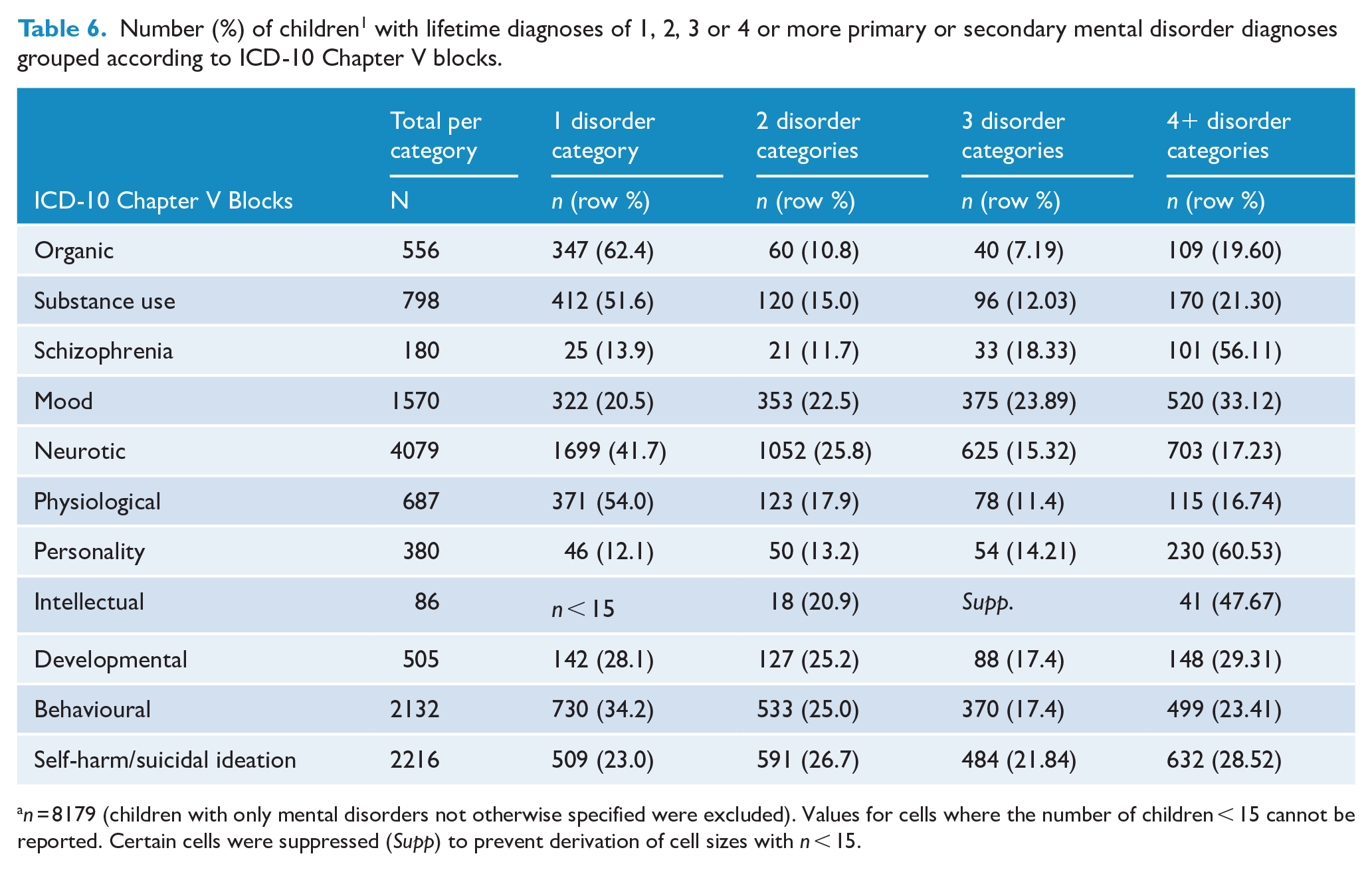
n = 8179 (children with only mental disorders not otherwise specified were excluded). Values for cells where the number of children < 15 cannot be reported. Certain cells were suppressed (Supp) to prevent derivation of cell sizes with n < 15.
Involuntary admissions to psychiatric facilities
There were 353 children who were involuntarily admitted to a psychiatric facility prior to 18 years of age, representing 3.1% of all children who received a primary mental disorder diagnosis. There were 568 involuntary admissions among these 353 children (Table 7), representing 11.7% of all admissions for a primary mental disorder (n = 4873). Negative binomial analysis indicated that the number of days spent in involuntary care was also influenced by diagnosis (χ2 = 117.82, df =6, p = 2.2 × 10−6). Comparison of the 95% confidence intervals between each diagnostic group for the number of days spent in care demonstrated that on average, young people with schizophreniform disorders spent significantly more days in involuntary care than children with other mental disorders (Supplementary Table 2 and Figure 3).
Characteristics of involuntary admissions according to primary diagnosis. a
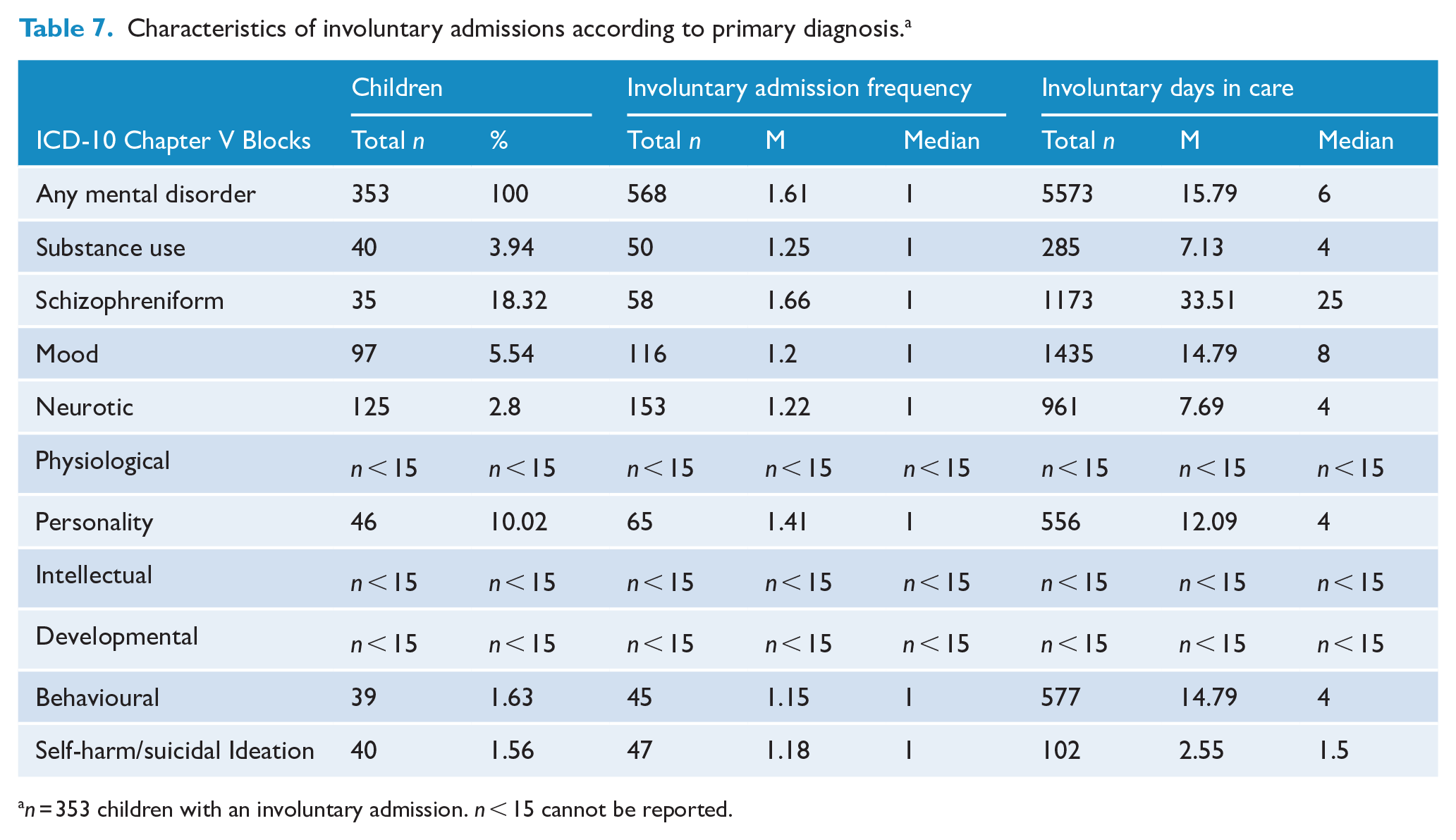
n = 353 children with an involuntary admission. n < 15 cannot be reported.
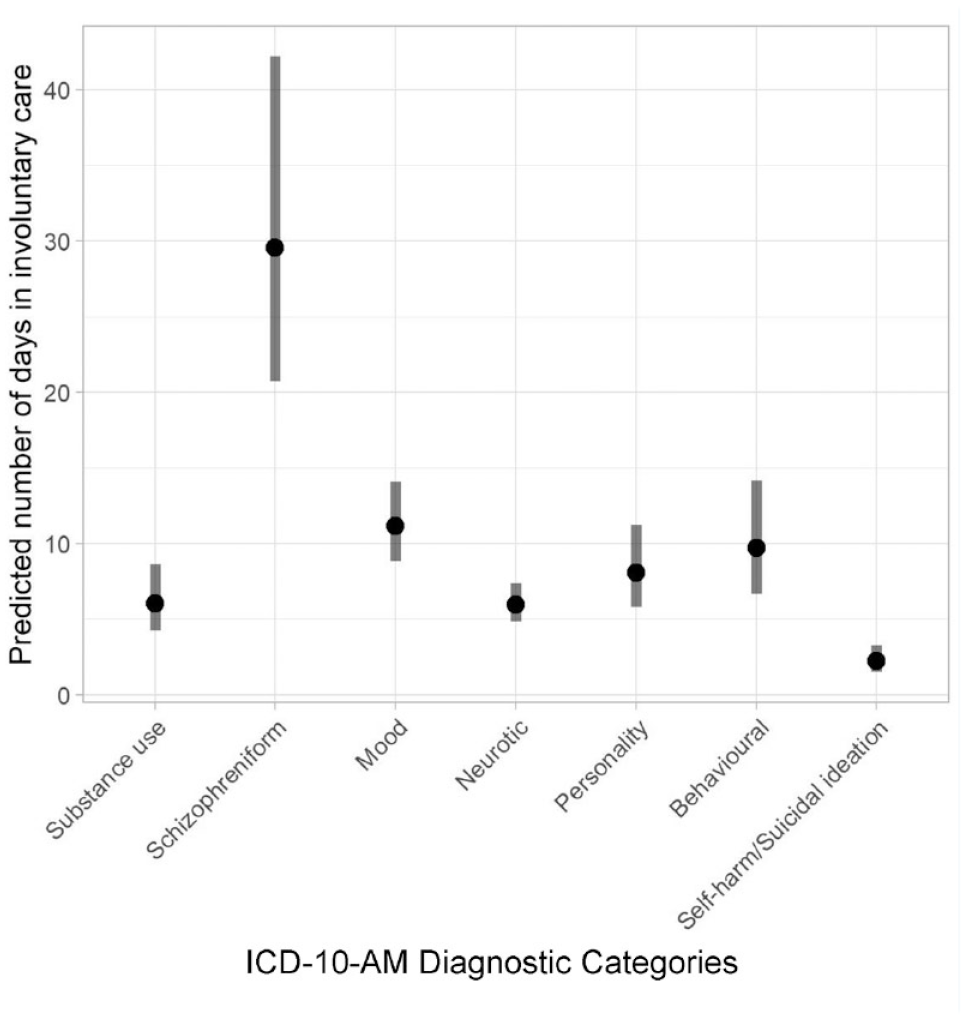
Estimated marginal means and 95% confidence interval for length of time in involuntary psychiatric care according to primary psychiatric disorder diagnostic category.a
Discussion
In a representative population sample of 85,642 Australian children growing up in NSW, 11,205 (13.1%) received at least one occasion of mental healthcare from admitted patient, emergency department or mental health ambulatory services between birth and age ~17.5 years (2002–2021). Among these children, ambulatory services were the most frequently accessed, and girls were more likely than boys to have contact with mental health services. Consistent with prior Australian studies (Lawrence et al., 2015; Segal et al., 2017), mental health service use increased with age. Here we were able to demonstrate, for the first time, how these patterns of mental healthcare service use by children varied according to mental disorder category and type of health service accessed. For example, young people with physiological (eating) disorders were most commonly identified in admitted patient data; children with organic disorders, substance use disorders and self-harm/suicidal ideation were most commonly identified in emergency services data; while children with all other types of mental disorders (mood, neurotic, personality, intellectual, developmental, behavioural and mental disorders not otherwise specified) except for schizophreniform disorders, were most frequently identified in mental health ambulatory services. Young people with schizophreniform disorders were just as commonly identified in emergency and mental health ambulatory services. This study also produced the novel finding that more than two-fifths of children receiving mental healthcare were diagnosed with more than one category of mental disorder prior to 18 years of age; cumulative comorbidity was greatest among youth with personality disorders and schizophreniform disorders. The presence of personality disorders among this cohort is interesting given historical controversies surrounding diagnosis with personality disorders prior to 18 years of age; nevertheless, such diagnoses appear to be reliable and useful to facilitate early intervention among adolescents (Kaess et al., 2014). Approximately 3% of children with a mental disorder were involuntarily admitted for psychiatric care: nearly one-fifth of the young people with schizophreniform disorders were involuntarily admitted at least once and spent more time in involuntary care than children with other disorders.
To our knowledge, this was the first study to conjointly examine mental healthcare in young people across admitted patient, emergency and mental health ambulatory services, facilitating comparison of the patterns of mental healthcare accessed across these services, according to age, sex and disorder types. Mental health ambulatory care services, which were the primary source of mental health support among children both overall and as the point of first contact, include multiple outpatient services. The emergency department was the next most likely type of health service accessed by young people. The number of children presenting to the emergency department for self-harm and suicidal ideation was particularly high, especially for girls and increased with age, consistent with several other studies (Kim et al., 2020; Perera et al., 2018). Emerging evidence internationally suggests that emergency departments are often ill-equipped to attend to the needs of patients who present with self-harm and suicidal ideation (O’Keeffe et al., 2021; Rayner et al., 2019) and that people from socio-economically disadvantaged backgrounds are more likely to present to the emergency department (Ceniti et al., 2020). In Australia, presentations to the emergency department with mental health problems have been increasing over time (Hiscock et al., 2018; Tran et al., 2019), and have been associated with longer wait times and periods of care, a tendency to receive inadequate care, high re-presentation rates and a greater likelihood of prematurely discharging themselves against medical advice, relative to patients with physical health problems (Australian Institute of Health and Welfare, 2019; Duggan et al., 2020; Patricia et al., 2022). Emergency departments could be better equipped to deal with acute mental health presentations via improved design and increased resources, better trained staff in all aspects of mental health care, and better integration with emergency medical services, especially those of toxicology. That the receipt of mental healthcare as an admitted patient was the service type least frequently accessed is likely attributable to the fact that psychiatric admissions predominantly occur in the context of severe clinical presentations (Unick et al., 2011): perhaps not surprisingly, the number of children admitted with neurotic and mood disorders, and self-harm/suicidal ideation increased with age. Regardless of service type, physiological disturbance disorders were most likely to occur in early childhood (driven by sleep disorders), declined in middle childhood and resurged in adolescence due to the onset of eating disorders.
Consistent with prior research, this study observed that girls were more likely than boys to use mental health services for most types of mental disorders (most notably mood and neurotic disorders; Eaton et al., 2012; Kuehner, 2017), despite earlier service use among boys (relative to girls) overall and for several mental disorder categories. While this aligns with reported sex differences in propensities towards internalising vs externalising psychopathology (Eaton et al., 2012), there was little difference in the proportion of boys and girls who sought treatment for primary substance use issues. This may be because individuals with persistent externalising problems may come into contact with the criminal justice system (instead of secondary health services; Broidy et al., 2015; Rivenbark et al., 2018). Furthermore, males are less likely to seek treatment for mental health issues (Grace et al., 2018; Liddon et al., 2018; Rice et al., 2018a; Rice et al., 2018b). Consistent with the prior literature (Adak and Halder, 2017; Zeidan et al., 2022), developmental disorders were considerably more prevalent in males in the present study; research suggests that the diagnostic criteria and screening instruments for autism are biased towards detecting this disorder in males (McCrossin, 2022).
This study represents the first examination of mental disorder comorbidity among children presenting to hospital, emergency and mental health ambulatory services; overall, more than two-fifths of children who accessed mental health services presented with multiple mental disorders over the course of childhood and adolescence. This largely accords with rates of comorbidity reported previously (Barr et al., 2022; McGrath et al., 2020), extending these previously reported findings into the area of cumulative mental disorder comorbidity in childhood and adolescence. Personality disorders, schizophreniform disorders, intellectual disability, self-harm/suicidal ideation and mood disorders showed particularly high rates of cumulative mental disorder category comorbidity. Such findings emphasise the need to improve personalised assessment and care (Caspi et al., 2013; Insel et al., 2010; Kotov et al., 2017). While diagnostic uncertainty in childhood and adolescence may have contributed to comorbidity, the observed rates of comorbidity were similar to those previously reported among these children’s parents over only a 5-year period (Watkeys et al., 2022). If mental disorder comorbidity were wholly attributable to diagnostic uncertainty during childhood, elevated cumulative mental disorder comorbidity should have been evident in children relative to their parents, but it was not.
Among the approximately 3% of children who were involuntarily admitted for psychiatric care, diagnoses of neurotic or mood disorders accounted for almost two-thirds of involuntarily admissions, while schizophreniform disorders were associated with the greatest number of admissions and number of days in care per person. Several international studies have similarly reported an increased risk for, and length of stay in, involuntary care among people diagnosed with schizophreniform disorders (Hotzy et al., 2019; Hwang et al., 2020). Young people with a primary diagnosis of mood disorder also spent significantly longer in involuntary care compared with children who had a primary diagnosis of neurotic disorders, self-harm/suicidal ideation and substance-use disorders.
Limitations of this study include the use of records from only three types of health services which likely represent a fraction of services used by young people for the treatment of mental disorders (these records do not include contact with general practitioners, private psychologists or psychiatrists, counsellors or other mental health professionals); only 6% of young people with mental illness are estimated to use hospital-based mental health services each year (Lawrence et al., 2015). In addition, the EDDC does not obtain data from all emergency departments in the state of NSW, despite capturing a substantial proportion of the service provided (NSW Ministry of Health, 2022).
In sum, among a population cohort of >85,000 children followed from birth through adolescence, 13.1% of children accessed hospital- and ambulatory-based mental health services; most of these children accessed multiple services on repeated occasions, with service-use increasing with age. This whole-of-population, integrated overview of mental healthcare provision across different services among children and adolescents can inform future developments of mental health systems for this population. Future research should explore the intersection between these services and more common forms of mental healthcare (e.g. general practitioners, psychologists, etc.) to determine the extent to which children access these primary forms of care prior to engaging with more acute services to elucidate potential means of addressing mental health problems before they become severe enough to necessitate hospital care.
Supplemental Material
sj-docx-1-anp-10.1177_00048674241258599 – Supplemental material for Patterns of health service use for children with mental disorders in an Australian state population cohort
Supplemental material, sj-docx-1-anp-10.1177_00048674241258599 for Patterns of health service use for children with mental disorders in an Australian state population cohort by Oliver J Watkeys, Kirstie O’Hare, Kimberlie Dean, Kristin R Laurens, Stacy Tzoumakis, Felicity Harris MAClinEpi, Vaughan J Carr and Melissa J Green in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This research used population data owned by the NSW Department of Education; Australian Curriculum, Assessment and Reporting Authority (ACARA), managed by the NSW Education Standards Authority; NSW Department of Communities and Justice; NSW Ministry of Health; ACT Health; NSW Registry of Births, Deaths and Marriages; the Australian Coordinating Registry (on behalf of Australian Registries of Births, Deaths and Marriages, Australian Coroners and the National Coronial Information System); Australian Bureau of Statistics; Australian Institute of Health and Welfare; Department of Social Services; NSW Bureau of Crime Statistics and Research; NSW Department of Justice, and; NSW Police Force. This research used data from the Australian Early Development Census (AEDC). The AEDC is funded by the Australian Government Department of Education. The findings and views reported are those of the authors and should not be attributed to these Departments, or the NSW and Australian Government. Record linkages were conducted by the NSW Centre for Health Record Linkage.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was conducted by the University of New South Wales with financial support from the National Health and Medical Research Council (NHMRC) Project Grant (APP1148055), and Investigator Grant (APP1175408 awarded to K.D.) and Australian Research Council (ARC) Future Fellowship (FT170100294 awarded to K.R.L.) and Discovery Early Career Researcher Award (DE210100113 awarded to S.T.) and a Department of Health and Aged Care Medical Research Future Fund Million Minds Mental Health Grant (APP2006436). OW was supported by a Postdoctoral Fellowship from Suicide Prevention Australia.
Data availability statement
Data used in this project were provided by government or other agencies for the research purposes of the NSW Child Development Study and are unable to be shared with third parties or deposited into data repositories. Researchers wishing to access these data need to apply in writing to relevant data custodians.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.