
Abstract
Objective:
This study aimed to investigate the help-seeking behaviours among children and young people (CYP) from culturally and linguistically diverse (CALD) backgrounds for mental health (MH) needs in a multicultural Australian population.
Methods:
We analysed the electronic medical records (eMR) of 8135 MH-related emergency department (ED) encounters of CYP aged up to 18 years across six public hospitals in the South Western Sydney Local Health District, Australia, from January 2016 to April 2022. Urgency of MH care was grouped into high priority (triage categories 1 and 2, needing to have treatment within 10 minutes) and low-to-moderate (triage categories 3–5, needing to have treatment within 30–120 minutes) presentations. Multilevel logistic regression models adjusted for key covariates and patient level clustering examined the relationship between CALD status and urgency of MH care. We also assessed the combined effects of gender and CALD status, as well as CALD status and residential area socioeconomic status, on urgent ED care.
Results:
About 8.3% of all MH-related ED presentations during the 6-year period were classified as high priority. The odds of high-priority MH ED care were 2.03-fold higher for CALD CYPs compared to non-CALD CYPs (adjusted odds ratio (AOR): 2.03, 95% confidence interval [CI] = [1.46–2.82]). Furthermore, an added increase in the odds of seeking urgent MH care for CYPs who belong to multiple risk groups was observed among CALD male CYPs (AOR: 2.96, 95% CI = [1.81–4.85]) and those living in disadvantaged areas (AOR: 2.36, 95% CI = [1.59–3.49]).
Conclusion:
The findings of this study highlight the need for culturally appropriate services aimed at prevention and early intervention targeted at CYP from CALD backgrounds to avoid crisis presentations.
Keywords
Background
The increasing prevalence of mental disorders among children and young people (CYP) is a significant challenge to both the health and health care systems in Australia and worldwide (Australian Institute of Health and Welfare, 2022; GBD Mental Disorders Collaborators, 2022). In Australia, 14% of children and adolescents aged between 4 and 17 years reported experiencing mental illness (Lawrence et al., 2015) with 42% aged between 15 and 24 years experiencing psychological distress (Roger et al., 2024). Furthermore, the National Study of Mental Health and Wellbeing survey indicated that more than one in three (38.8%) people aged 16–24 years had a 12-month mental disorder (Australian Bureau of Statistics (ABS), 2023). The onset of mental illness during childhood and adolescence not only poses immediate challenges for affected individuals but also has far-reaching implications for their future health, social functioning, and overall quality of life (Celebre et al., 2021; Otto et al., 2021). The total cost associated with healthcare utilisation and medications for CYP with mental disorders in Australia has been estimated to amount to US$234 million annually, of which approximately 16% was attributed to out-of-pocket costs (Le et al., 2021). Moreover, the impact of the COVID-19 pandemic has further exacerbated the rates of mental illness among CYP due to reasons of school closures, lack of social gatherings, family stress, and domestic violence (Araújo et al., 2021; Cowie and Myers, 2021). This has been clearly reflected in the higher than usual visits to primary care and emergency departments (EDs), and increased hospitalisation rates, as evidenced by our previous studies (John et al., 2023; Khan et al., 2023). While the aforementioned studies have reported on the general population, specific risk factors that negatively influence mental health (MH) among CYP from culturally and linguistically diverse (CALD) communities have not been explored in detail, thus warranting further investigation.
Previous research has shown that migrants, refugees, and asylum seekers experience mental illness and suicidal behaviour at significantly higher rates than the general population due to reasons of traumatic pre- and peri-migration experiences such as family separation and loss, violence, and immigration detention (Australian Research Alliance for Children and Youth (ARACY), 2007; Tomasi et al., 2022). However, studies have also shown lower service utilisation, especially for MH needs, among those from CALD communities, due to reasons of cultural beliefs, stigma, and other structural barriers (Pham et al., 2023; Wohler and Dantas, 2017). While there is a scarcity of research documenting service utilisation among CALD communities and the risk factors that contribute to low service utilisation, available findings report on all ages combined, hence potentially overlooking the distinct risk factors that pertain to the CYP within these communities. In addition, there has been no research conducted examining whether CYP from CALD communities are seeking more urgent MH-related ED care or are accessing MH services late in their health journey.
To address this critical knowledge gap, this study was conducted to determine the relationship between CALD status and urgency of care for MH needs in a multicultural community of South Western Sydney Local Health District (SWSLHD). As one of the most ethnically diverse regions in Australia, SWSLHD (2022) is home to a substantial number of CALD residents compared to the rest of New South Wales (NSW; 43% of SWS residents are born overseas compared to the NSW state average of 34%), speaking diverse languages and adhering to distinct cultural practices and beliefs. The findings of this study will provide insights into MH-related help-seeking behaviours, and MH service access among CYP from CALD communities and explore effective strategies for prevention and intervention.
Methods
Study design, data source and cohort selection
We analysed routinely collected de-identified electronic medical records (eMRs) of ED presentations between January 2016 and March 2022. This study comprised encounter-level information of CYP aged up to 18 years who presented to the ED for a MH problem, in the six SWSLHD public hospitals (Liverpool, Bankstown-Lidcombe, Bowral, Camden, Campbelltown, and Fairfield) covering a population of 1.04 million residents from Bankstown to Bowral, over the 6-year period.
The de-identified eMRs were securely accessed via the CEDRIC (Comprehensive Epidemiological Dataset for Research, Innovation and Collaboration) platform that draws data from the eMR system captured during service interactions, with opportunities to track their service use (South Western Emergency Research Institute (n.d.)). The CEDRIC platform comprises detailed data including demographic information, dates/times of ED visit, triage classification, and discharge diagnosis. ED discharge diagnosis was coded in Systematised Nomenclature of Medicine-Clinical Terminology Australian Extension (SNOMED CT-AU) and was converted into the corresponding International Classification of Diseases, 10th Division, Australian Modification (ICD-10-AM) codes using the snoMAP-Starter AU (Lawley et al., 2017). We classified an encounter as an MH-related presentation based on the relevant ICD-10-AM code for a MH condition (Lawley et al., 2017). A list of ICD-10-AM codes used to classify encounters with MH disorders in this database was reported in earlier research (John et al., 2024).
Outcome measure, exposure, and covariates
The primary outcome variable of interest was the perceived emergency level of care as defined by the Australasian Triage Scale (ATS), a tool that ensures that patients presenting to the ED are treated as per their clinical urgency and are assigned to the assessment and treatment area that best suits their needs (Australasian College for Emergency Medicine, 2016). For the purposes of this study, the five categories (categories 1–5) were dichotomised into ‘high priority’ (triage category 1 and 2, that is, needing to have treatment within 10 minutes and categorised as having an imminently life-threatening condition) and ‘low to moderate priority’ (triage categories 3–5, that is, needing to have treatment between 30 and 120 minutes) presentations priority.
In accordance with the nationally consistent indicators for CALD status (ABS, 2022), we identified a patient’s CALD status using three approaches: (1) if the patient’s preferred language was non-English, (2) if the patient’s country of birth was a non-English-speaking country and (3) if the patient’s preferred language was non-English and/or the country of birth was a non-English-speaking country (composite CALD status). In addition, key covariates that were considered in this study as potential confounding factors included: age at presentation to the ED (in years); gender (male, female, undisclosed); day of arrival (weekday, weekend); time of arrival (0:00–7:59, 8:00–17:59, 18:00–23:59); residential area (i.e. postcode); SES quartiles (least advantaged, second least advantaged, second most advantaged, most advantaged); residential area remoteness classification (major cities and inner or outer regions); mode of arrival (ambulance, others); and COVID-19 period (pre-COVID-19 from January 2016 to February 2020, COVID-19 from March 2020 to March 2022). The SES of patients’ residential postcode was calculated using the Australian Bureau of Statistics (ABS) (2006b) Index of Relative Socioeconomic Disadvantage (IRSD) for the 2016 census population. The ABS also contains the Accessibility and Remoteness Index of Australia (ARIA) to measure access to services, which was used in this study to classify each patient’s residential postcodes into major cities, inner or outer regional Australia (ABS, 2006a).
Statistical analysis
Descriptive statistics were used to compare the proportion of high priority or urgent ED presentations across key variables. A multivariable multilevel logistic regression model was used to evaluate the association between CALD status and high-priority ED presentation while controlling for covariates and patient level clustering. Five models were developed: Model 1 – Preferred language + covariates; Model 2 – Country of birth + covariates; Model 3 – composite CALD status (based on preferred language and/or country of birth) + covariates; and cumulative risk Models 4 and 5 – combined CALD and gender/area SES + covariates. The cumulative risk model quantified the combined effects of gender and CALD status, as well as CALD and area SES, on urgent ED care. The model-based results are presented as adjusted odds ratios (AORs) with 95% confidence intervals (95% CIs). All analyses were performed in R version 3.6.3.
Results
Descriptive characteristics of the sample
The descriptive characteristics of CYP with MH-related encounters by urgency of ED care are shown in Table 1. This study identified and analysed 8135 MH-related ED presentations made by 4979 unique CYPs during the study period. The average age of the participants was 14.5 years with higher presentations made by females compared to males (62% vs 37%) and majority of CYPs born in Oceania compared to other regions (93% vs 7%). Of the 8135 MH-related ED encounters, 676 (8.3%) encounters were reported as high-priority MH presentations. CYP from CALD background (composite CALD status) represented 9.2% of the overall MH-related encounters. While the rate of repeated presentations to the ED was lower among those from a CALD background (1.37 per CYP) compared to non-CALD (1.67 per CYP) CYPs, the proportion of high-priority MH encounters among CYP from CALD background was double that of CYP from a non-CALD background (13.4% vs 7.8%). This higher rate was similar using different definitions of CALD status, e.g. preferred language (non-English) and the country of birth (non-English-speaking country). Furthermore, a breakdown of ED encounters by MH diagnosis and by CALD status is shown in Supplementary Table 1 and the overall number and percentage of MH-related ED presentations by CALD status (country of birth and language spoken) are shown in Supplementary Table 2.
Characteristics of CYP patients by all mental health-related ED encounters and by type of priority encounters.
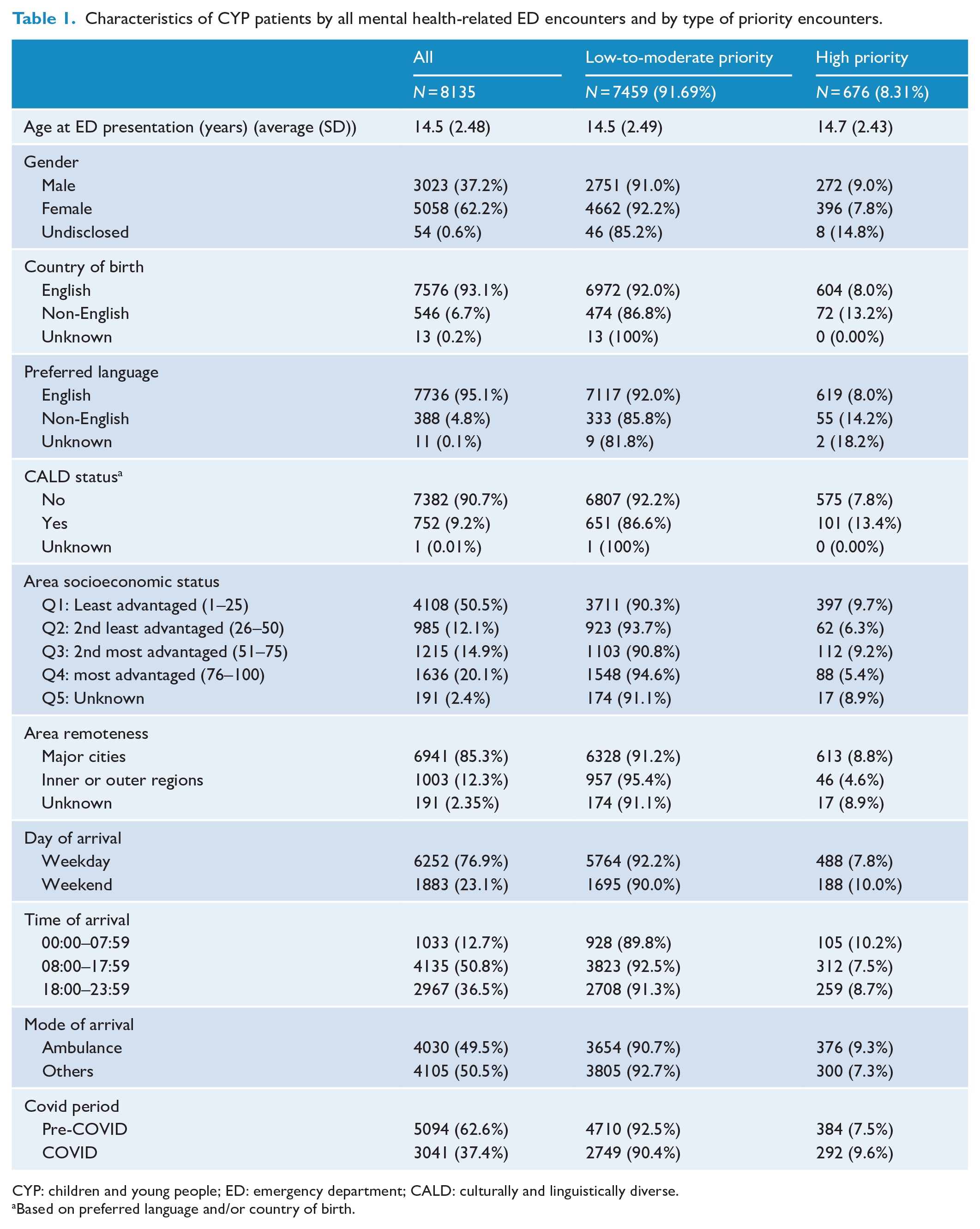
CYP: children and young people; ED: emergency department; CALD: culturally and linguistically diverse.
Based on preferred language and/or country of birth.
Findings from the multivariable multilevel logistic regression model
CYP with CALD backgrounds (irrespective of the specific indicators used to define the CALD populations) had increased odds of requiring urgent MH ED care compared to non-CALD CYPs, accounting for potential confounding factors. The odds of ED presentation with urgent MH need were 2.03 times higher in CYP from a CALD background compared to those from a non-CALD background (AOR: 2.03, 95% CI = 1.46–2.82) model 3. Results were again comparable across definitions of CALD status (models 1–3; see Table 2).
CALD status indicators associated with high-priority triage presentations adjusting for key covariates (outcome variable 0 = low-to-moderate priority, 1 = high priority).
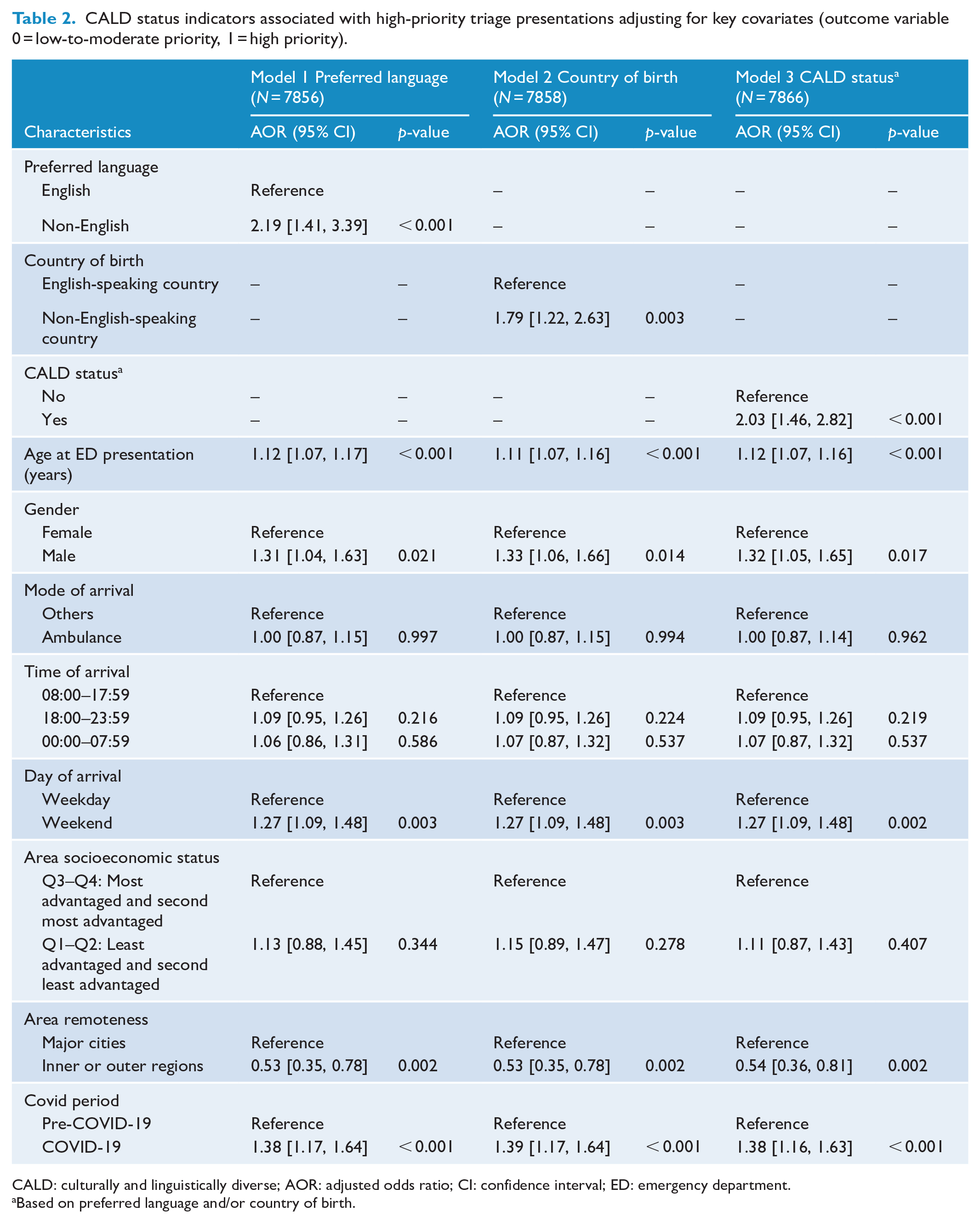
CALD: culturally and linguistically diverse; AOR: adjusted odds ratio; CI: confidence interval; ED: emergency department.
Based on preferred language and/or country of birth.
Other key covariates were also significantly associated with higher priority triage presentation (urgent MH presentation). These included older age (AOR: 1.12, 95% CI = [1.07–1.16]); males compared to females (AOR: 1.32, 95% CI = [1.05–1.65]); and weekend presentations (AOR: 1.27, 95% CI = [1.09–1.48]). Furthermore, the COVID-19 period was also significantly associated with higher odds of urgent MH presentation in both models (AOR: 1.40, 95% CI = 1.18–1.66). Finally, area remoteness (inner or outer regions) was significantly associated with lower odds of urgent MH presentation (AOR: 0.54, 95% CI = [0.36–0.81]) compared to CYPs living in major cities.
Being in multiple risk groups increased the likelihood of urgent MH-related ED care (see Table 3). For example, the odds of high-priority MH-related ED care were 2.96-fold higher for male CYPs from a CALD background compared to females from a non-CALD background (AOR: 2.96, 95% CI = [1.81–4.85]). In addition, CYPs from a CALD background living in disadvantaged areas also had 2.36-fold higher odds of high priority ED care compared to CYPs without these risk factors (AOR: 2.36, 95% CI = [1.59–3.49]).
Cumulative risk model based on gender, CALD and SES.
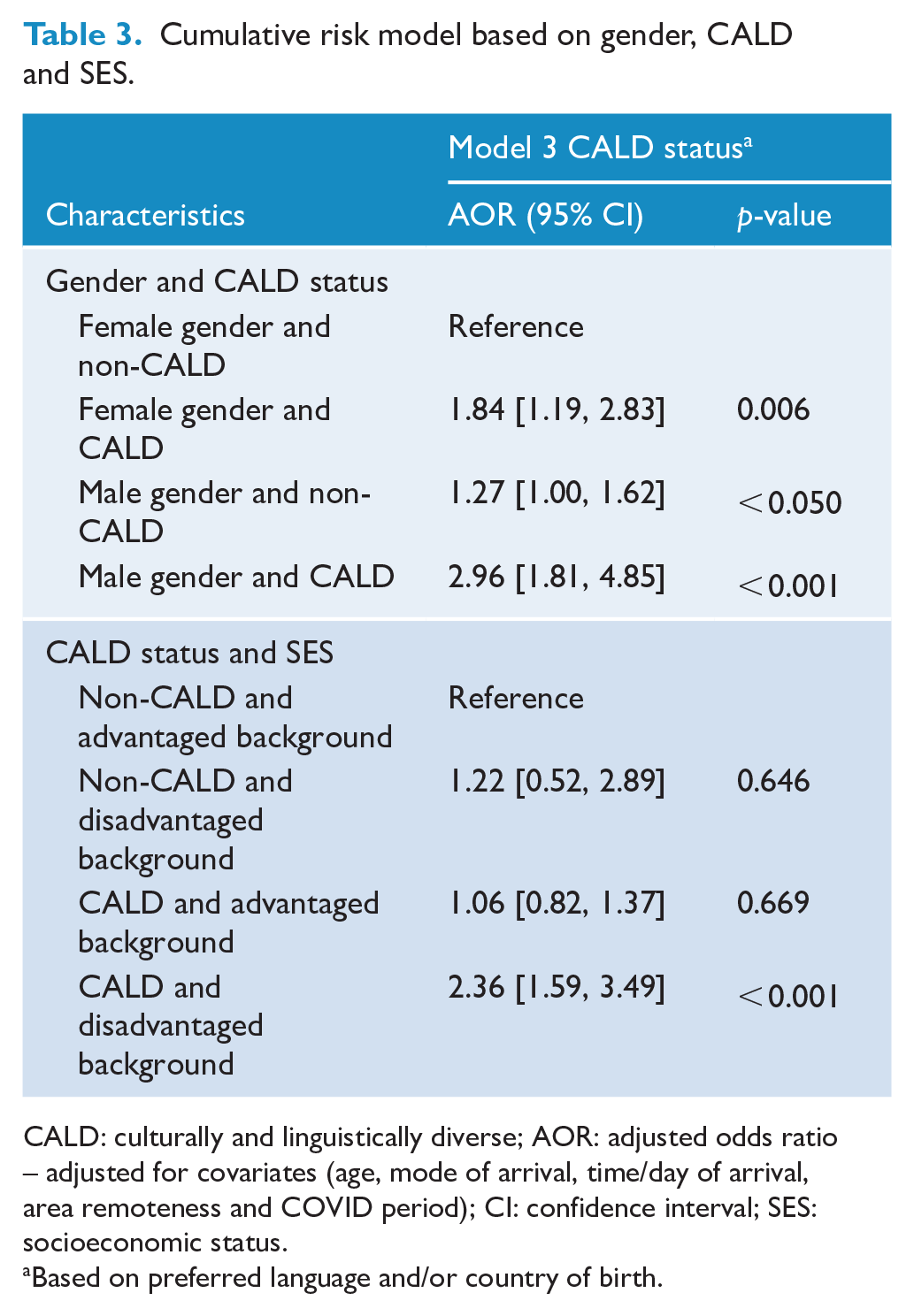
CALD: culturally and linguistically diverse; AOR: adjusted odds ratio – adjusted for covariates (age, mode of arrival, time/day of arrival, area remoteness and COVID period); CI: confidence interval; SES: socioeconomic status.
Based on preferred language and/or country of birth.
Discussion
Summary of the findings
In this study, we undertook an analysis of MH-related ED presentations among CYP aged up to 18 years in a multicultural community of SWSLHD. We found that, despite the low rates of MH-related ED service utilisation, CYP from a CALD background demonstrated twice the odds of presenting to the ED with urgent MH needs compared to those from non-CALD background. Furthermore, this risk was exacerbated among males from a CALD background as well as CYPs from a CALD background living in disadvantaged communities. Finally, we also found significant associations between high priority triage MH presentations and risk factors such as older age, male gender, weekend presentations, area remoteness, and the COVID-19 period.
Comparison with existing literature
Despite the significant proportion of the CALD population in SWSLHD, our study revealed that only 9.2% of MH-related ED presentations were made by CYPs from CALD backgrounds. This finding highlights the underrepresentation of CALD CYP among those seeking ED care for MH concerns. This is consistent with Hart’s (1971) description of ‘inverse care law’ and our previous work (Woolfenden et al., 2020) where we observed that those children from priority population groups (CALD or socioeconomically disadvantaged background) were least likely to access health services, despite having the greatest need. Nonetheless, among the limited number of CYP who presented to the ED with MH needs, we found that CYP from a CALD background had significantly higher odds of presenting to the ED with urgent MH needs. This is consistent with Hart’s (1971) description of ‘inverse care law’ and our previous work (Woolfenden et al., 2020) where we observed that those children from priority population groups (CALD or socioeconomically disadvantaged background) were least likely to access health services, despite having the greatest need. Moreover, we also found that the increased risk of high-priority triage in ED MH care is shaped by the intersection of multiple risk factors, such as being a male and residing in disadvantaged areas, in addition to being from a CALD background. In line with this, there is a growing body of evidence reporting this health service inequity among CYP from a CALD background as a result of structural barriers, as well as unique help-seeking patterns (Eapen et al., 2017). For instance, a scoping review of 64 studies reported low service utilisation due to key individual-, family- and community-level challenges including poor health literacy, cultural beliefs, language barriers, socioeconomic status, lack of understanding of appropriate healthcare pathways, and poor access to and cultural competency of providers, among many other factors (Khatri and Assefa, 2022).
Another systematic review of 62 studies, reporting on barriers to accessing and engaging with MH care among at-risk young people in Australia, found only one study investigating the role of CALD background in MH service utilisation, indicating that individuals with a CALD background tended to place a low-to-moderate priority on MH, have distrust of services, and keep emotional problems within the family, leading to barriers to access (Brown et al., 2016). In addition, there is evidence of research participation inequity, in that priority populations such as CALD groups are not represented in health systems research, and hence service type and delivery are not designed for their needs (Collings et al., 2016; Grace et al., 2019; Grace and Trudgett, 2012; Mei et al., 2020). Therefore, it is crucial to have systems in place to address equity in service access, as well as community and consumer engagement in health research, to ensure that CYPs’ needs are met, regardless of their background and circumstances.
We also found several other key risk factors that were associated with high priority MH presentations. Consistent with other studies (Say et al., 2021; Smith et al., 2019), we found that older age was significantly associated with high-priority MH presentations, which may suggest that adolescents are more likely to have severe MH problems or complex psychosocial situations requiring ED care compared to their younger counterparts. The findings of this study showed that, while female CYPs had higher rates of overall MH-related ED presentations, male CYPs were associated with higher odds of presenting to the ED for an urgent MH need. The increased rates of MH-related health service utilisation among female CYP are consistent with our previous findings (John et al., 2023; Khan et al., 2023); however, the higher rates of urgent presentations among male CYPs further underscore the help-avoidance pattern, and that they tend to seek assistance only when faced with an urgent MH need, as reported by other studies. For instance, a systematic review of help-seeking behaviour among individuals with major depression found that males tend to delay seeking help for MH issues until they become more severe (Magaard et al., 2017). Other potential reasons for help avoidance among male CYPs include traditional masculine ideals, self-medicating with alcohol, stigma and shame associated with cultural beliefs and personal challenges, among others (Lynch et al., 2018). Finally, we also found that weekend presentations were also associated with higher odds of high-priority MH presentations. This might be due to the limited availability of MH services, especially during weekends, making ED services the only option for urgent MH needs.
Strengths and limitations
Our study has several strengths and limitations. The data are drawn from a large clinical and administrative dataset from six public hospitals in SWSLHD, an area with a significant proportion of CALD communities as well as high rates of social and economic disadvantage. We presented an encounter-level analysis as opposed to a patient-level analysis, making it possible to explore the relationship between CALD status and high priority MH presentations and other key risk factors. However, several limitations to this study are also noted. First, the data extracted from the six public hospitals cannot be generalised to the populations in the community or ED presentations to other hospitals outside the SWSLHD. Second, the findings demonstrate an association rather than a causative relationship between predictors and outcomes. Although we defined the CALD status using the minimum core set of cultural and language indicators such as preferred language and country of birth, other key factors such as the reason for migration (e.g. skilled migration versus refugee/asylum seekers) and type of ethnic groups might have provided richer information. Hence, there is opportunity for future research to further explore in detail, health service use by reason for migration and by different ethnic groups. In addition, further research should include better data on underlying population prevalence of MH issues, and ED presentation rate per 100,000 people, by CALD/non-CALD status in a CYP population both in Australia and within each relevant geographic region.
Implications of the findings
The findings of this study have important implications for policy at patient (CYP), practice/provider, and health care system levels. At CYP level, there is an urgent need to further promote MH awareness programs in culturally and linguistically sensitive and appropriate ways at a range of venues, including but not limited to schools and early childhood centres, multicultural and ethnic child and family or community groups, and youth work settings. At practice/provider level, services need to better consider the needs of CYP from a CALD background and consider strategies for adapting services to make them more culturally responsive. Cultural competence training among healthcare providers is essential for ensuring equitable and patient-centred care for CALD children. Training on diverse cultural norms and communication styles could help health care professionals in enhancing their ability to better understand the distinct needs of CYP from CALD communities. At health care systems level, resources could be redirected to further meet the needs of CYP from CALD communities by embedding multicultural worker/interpretation services, which has proven to be effective in increasing uptake/engagement among CYP from CALD communities (Goris et al., 2013). This reiterates the need for more culturally appropriate MH awareness, cultural competence training for health care providers, as well as resources targeted to embed multicultural worker or interpreter services, to better manage this vulnerable cohort, so that their MH needs are identified and supported early. In this regard, an Integrated Continuum of Connect and Care (I-CCC) model has been proposed that would integrate all relevant services using a tiered care pathway proportionate to the needs of the CYP and their families/carers (Eapen et al., 2023).
Conclusion
The findings of this study show that CYP from a CALD background, while having low MH-related service utilisation generally, are also at disproportionately higher risk of crisis presentations to the ED with urgent MH needs. This suggests that they may postpone seeking assistance for their MH concerns until they reach a more critical stage. Furthermore, other key risk factors such as older age, male gender, area remoteness, weekend presentations, and the COVID-19 period were also associated with high-priority MH presentations. This emphasises the necessity of increased awareness about MH that aligns with various cultures, training healthcare providers to be culturally competent, and allocating resources specifically aimed at integrating multicultural workers or interpreter services. Directions for future research include quantitatively exploring health service use by reason for migration and by different ethnic groups as well as qualitatively ascertaining subjective experiences of CYP and their families about barriers and challenges and co-designing potential solutions for better access and engagement.
Supplemental Material
sj-docx-1-anp-10.1177_00048674241310702 – Supplemental material for Mental health help-seeking behaviours among children and young people from culturally and linguistically diverse communities in a multicultural urban Australian population
Supplemental material, sj-docx-1-anp-10.1177_00048674241310702 for Mental health help-seeking behaviours among children and young people from culturally and linguistically diverse communities in a multicultural urban Australian population by James Rufus John, Jahidur Rahman Khan, Paul M Middleton, Yao Huang, Ping-I Lin, Nan Hu, Bin Jalaludin, Paul Chay, Raghu Lingam and Valsamma Eapen in Australian & New Zealand Journal of Psychiatry
Footnotes
Author Contribution
J.R.J., J.R.K., R.L., and V.E. were involved in the conceptualisation of the study. J.R.J., J.R.K., P.M.M., Y.H., and N.H. contributed to the data curation and formal analysis. J.R.J. and J.R.K. drafted the original draft. All co-authors contributed to the review and editing. All authors have read and agreed to the submitted version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics and Patient Consent
The Australian Institute of Family Studies Ethics Committee reviewed and approved each wave of the LSAC study. The ethics committee is registered with the National Health and Medical Research Council (NHMRC) and has ensured that the LSAC project fulfils the Australian National Statement on Ethical Conduct in Human Research. The data custodians authorised this study, and as this study only utilised secondary de-identified data, no additional ethics approval was necessary.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.