
Abstract

Introduction
The mental health of young people is declining globally (Benton et al., 2021). Australian national survey data show an approximate 50% increase in mental disorders among young people over the past two decades (Australian Bureau of Statistics [ABS], 2023), alongside an average annual rate of 3.6% increase in expenditure on child and adolescent mental health services (CAMHS) between 2015–2016 and 2019–2020 (Brazel et al., 2023). Adolescent mental illness and suicidality are strongly associated with child maltreatment (Angelakis et al., 2020; Baldwin et al., 2023), and self-harm and/or suicidal ideation are often recorded by child protection services prior to health services (O’Hare et al., 2023). Children exposed to severe maltreatment are more likely to be placed in out-of-home care (OOHC) and are at the highest risk of a range of poor outcomes in adulthood, including physical and mental health problems, homelessness and unemployment (Brännström et al., 2017). Here, we estimated the cumulative incidence of adolescent-onset mental disorders among youth aged 10–18 years who had been in contact with child protection services before age 10 years, and according to the highest level of child protection response which served as an indicator of the severity of maltreatment experienced (Mathews and Bross, 2015).
Methods
Study cohort
Participants were 85,368 youth (48% female, mean age 18.25 [SD = 0.37] years) drawn from a total population cohort of 91,597 youth in the New South Wales Child Development Study (NSW-CDS) (Green et al., 2024). These youth had available data from the NSW or ACT Admitted Patient Data Collections (APDC; 2002–2021) or Emergency Department Data Collections (EDDC; 2005–2021) and/or the NSW Mental Health Ambulatory data collection (MH-AMB; 2002–2020) and were alive at the end of the observation period on 31 December 2021. Ethics approval was provided by the NSW Population and Health Services and ACT Health Human Research Ethics Committees under a waiver of consent (HREC/18/CIPHS/49) for the linkage of health, education, justice and child protection records.
Outcome measures
Mental disorder indicators
Binary indicators of mental disorders diagnosed from 10 years of age were derived from any primary or secondary diagnoses of mental disorder (i.e. any F-code in Chapter V) and/or self-harm or suicidal ideation in any health record, according to the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification (ICD-10-AM). An indicator of any mental disorder was derived alongside seven additional indicators of (mutually exclusive) categories of mental disorders (Green et al., 2024): (1) anxiety disorders, (2) depressive disorders, (3) developmental disorders, (4) personality disorders, (5) psychotic disorders, (6) substance-use disorders and/or (7) suicidal ideation or self-harm; an individual could be diagnosed with multiple types of mental disorders. An indicator of any mental disorder <10 years was used as a covariate in adjusted analyses.
Exposures
Child protection response level
Young people known to child protection services were hierarchically allocated to mutually exclusive subgroups based on the highest level of child protection response they received <10 years of age: 1912 youth (2.2%) had at least one placement in OOHC; 2552 youth (3.0%) had at least one substantiated report of ‘Risk of Significant Harm’ but no OOHC placement; 11,769 youth (13.8%) had a ‘Risk of Significant Harm’ report which had not been substantiated and 2809 youth (3.3%) had reports that did not reach the ‘Risk of Significant Harm’ threshold.
Sociodemographic covariates
Covariates included the child’s sex (determined via consensus across records); Australian standard indices of socio-economic disadvantage (using the Socio-Economic Index For Areas: Index of Relative Socio-economic Disadvantage) and geographical remoteness (according to the Australian Standard Geographical Classification system) were derived from residential postcodes attained via cross-sectional assessments conducted at age 5 or 11 years (Green et al., 2024).
Analyses
Analyses were performed in RStudio v.1.3.1093 using R v.4.0.3. Univariable logistic regression analyses estimated associations between exposure to the child protection system and mental disorder outcomes. Multivariable logistic regressions adjusted for the three sociodemographic covariates and a binary index of ‘any mental disorder’ diagnosed before age 10 years. Cell sizes with frequencies less than 15 were suppressed, with secondary suppression implemented to prevent derivation of suppressed values via subtraction.
Results
Greater than one in five (22.3%) youths in the cohort were known to child protection services prior to age 10 years and around one in ten participants were diagnosed with at least one mental disorder between ages 10 and 18 years (Table 1). Greater than two in five (43.1%) individuals with adolescent mental disorder were previously known to child protection services; approximately half of youth with specific diagnoses of developmental disorders, personality disorders, psychotic disorders, substance-use disorders and/or suicidal ideation/self-harm were known to child protection services. Among youth with a mental disorder, almost one in two (46.5%) were diagnosed with multiple disorders.
Unadjusted (uOR) and adjusted (aOR) odds ratios (and 95% confidence intervals) for associations between (A) any contact with child protection services and (B) the highest level of child protection response and indices of mental disorder diagnoses.

col.: column; Subs.: substantiated; ROSH: risk of significant harm; OOHC: out-of-home care.
Adjusted models include covariates: sex, area-based socio-economic disadvantage, geographical remoteness and any mental disorder age < 10 years; Reference Category for all models is ‘No Child Protection contact’.
Figure 1 presents the cumulative incidence of mental disorder diagnoses according to the highest level of child protection response. From age 15 years, the cumulative incidence of psychosis rose sharply in those with substantiated maltreatment and OOHC placements. Unadjusted and adjusted odds of mental disorder diagnoses according to the highest level of child protection response are presented in Table 1. Youth known to child protection services were three times as likely to be diagnosed with a mental disorder in adolescence relative to non-maltreated peers (uOR = 3.04; 95% confidence interval [CI] = [2.91, 3.19]); this effect was marginally reduced in the adjusted model (adjusted odds ratio [aOR] = 2.88; 95% CI = [2.75, 3.02]). There was a dose-dependent pattern of associations between any mental disorder diagnoses and escalating levels of child protection service.
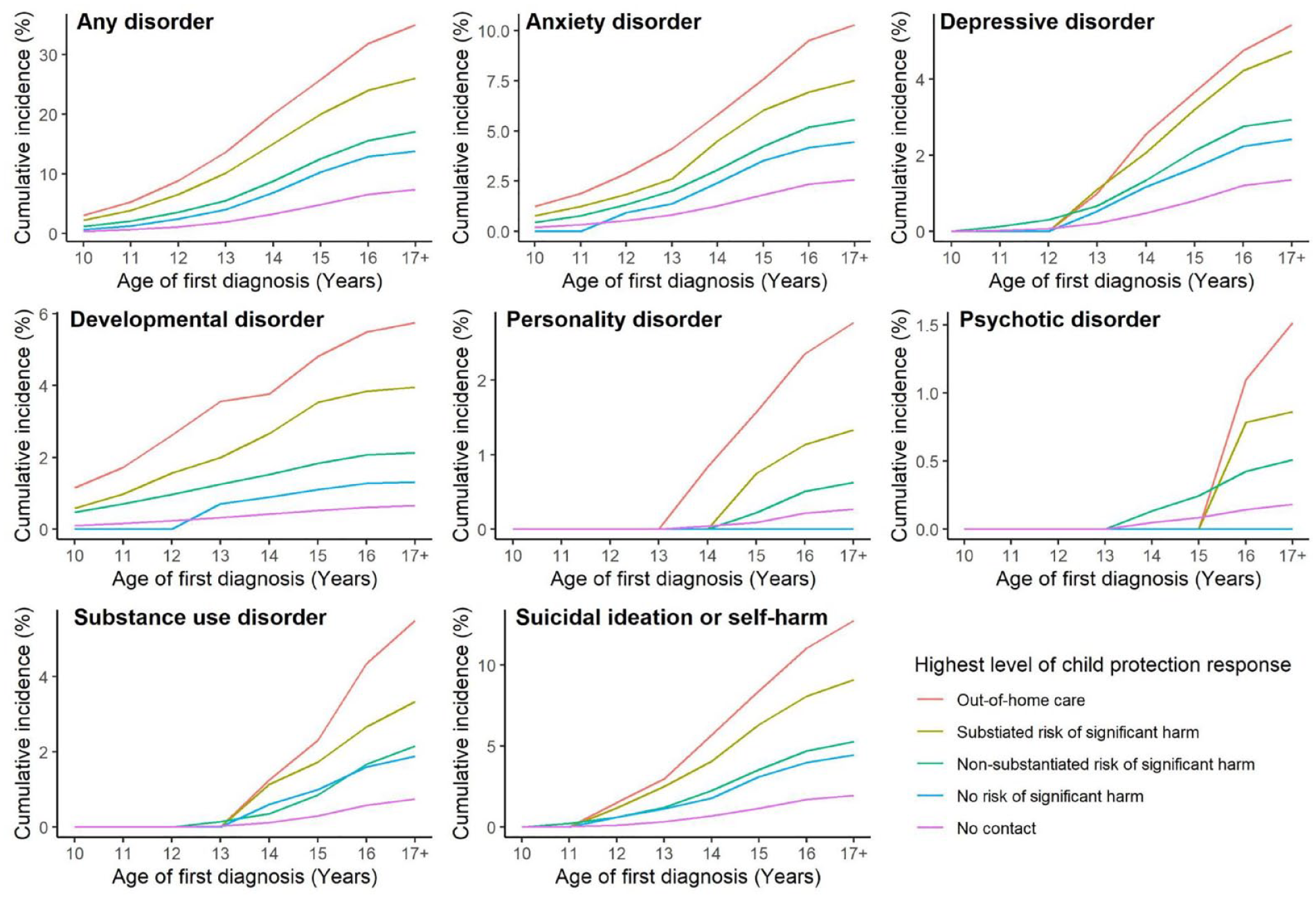
Cumulative incidence (%) of adolescents with different types of mental disorder between ages 10 and 18 years, according to the highest level of child protection response prior to age 10 years.
The crude odds of diagnosis with specific mental disorders in adolescence, among youth with a history of child protection contact, were moderate to very large (significant ORs ranging from 1.76 to10.48), with effect sizes marginally reduced in adjusted models (Table 1). Youth with an OOHC placement were at the greatest odds of being diagnosed with personality disorders (aOR = 9.29; 95% CI = [6.66, 12.75]), developmental disorders (aOR = 5.65; 95% CI = [4.45, 7.11]) and psychotic disorders (aOR = 6.81; 95% CI = [4.36, 10.30]). The magnitudes of effect were reduced in the adjusted models for specific disorders, but the statistical significance remained for all associations except that between personality disorders and reports below the threshold for risk of significant harm.
Discussion
Approximately one in five young people known to child protection services before age 10 years were diagnosed with a mental disorder by late adolescence; this rose to 26% of youth with substantiated maltreatment, and 35% of youth placed in OOHC. Youth placed in OOHC prior to age 10 years showed a crude >9-fold increase in risk of diagnosis with personality disorders, >8-fold increase in risk of developmental disorders, >7-fold increase in risk of psychosis and >6-fold increase in risk of self-harm or suicidal thoughts/behaviours, or substance-use disorders. The cumulative incidence of specific disorders across adolescence shows an earlier onset of many disorders with increased severity of maltreatment. The use of administrative data likely underestimated the extent of mental disorders and child maltreatment in this cohort, despite our higher cumulative incidence rates compared to annual incidence findings (ABS, 2023). Furthermore, this study cannot disentangle the potential genetic and/or environmental effects of parental mental disorders on maltreatment or mental disorders experienced by their offspring. The use of escalating child protection responses to index the severity of maltreatment is a coarse representation of the severity of maltreatment but reflects international practice and policy (Mathews and Bross, 2015). These findings highlight the potential role of child protection services at the forefront of mental illness prevention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The research was conducted with financial support from the National Health and Medical Research Council (NHMRC) Project Grant (APP1148055) and Investigator Grant (APP1175408 awarded to KD); Australian Research Council (ARC) Discovery Project (DP230101990) and Discovery Early Career Researcher Award (DE210100113 awarded to ST); Department of Health and Aged Care Medical Research Future Fund Million Minds Mental Health Grant (APP2006436) and a Postdoctoral Fellowship from Suicide Prevention Australia (awarded to OW). This research used population data owned by the NSW Department of Education; Australian Curriculum, Assessment and Reporting Authority (ACARA), managed by the NSW Education Standards Authority; NSW Department of Communities and Justice; NSW Ministry of Health; ACT Health; NSW Registry of Births, Deaths and Marriages; the Australian Coordinating Registry (on behalf of Australian Registries of Births, Deaths and Marriages, Australian Coroners and the National Coronial Information System); Australian Bureau of Statistics; NSW Bureau of Crime Statistics and Research; NSW Department of Justice and NSW Police Force. This research used data from the Australian Early Development Census (AEDC). The AEDC is funded by the Australian Government Department of Education. The findings and views reported are those of the authors and should not be attributed to these Departments, or the NSW, ACT or Australian Governments. Record linkages were conducted by the Centre for Health and Record Linkage (CHeReL). The funders had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. M.J.G. and O.J.W. had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Data Sharing Statement
Data used in this project have been provided by government custodians for research purposes of the NSW Child Development Study and are unable to be shared with third parties or deposited into data repositories. Collaborative research activities may be possible depending on scope and resources; alternatively, researchers wishing to access these data sets can apply directly to the relevant data custodians.