
Abstract
Objective:
There is evidence that over time health outcomes of people with schizophrenia are deteriorating rather than improving both in terms of mortality rate and levels of morbidity, even in Australia where service resourcing is substantial. Our objective was to examine the evidence of whether poor outcomes reflect decreases in treatment effectiveness and, if so, what are the barriers to improving standards of care. This review will argue that the confidence of clinicians to diagnose schizophrenia early, and provide assertive and long-term care, may be being undermined by a series of controversies in the published literature and discrepancies in clinical practice guidelines.
Method:
A critical review was conducted of the evidence regarding six issues of high clinical relevance to the treatment of schizophrenia formulated as questions: (1) Is schizophrenia a progressive disease? (2) Does relapse contribute to disease progression and treatment resistance? (3) When should the diagnosis of schizophrenia be made? (4) Should maintenance antipsychotic medication be discontinued in fully remitted first-episode patients? (5) Do antipsychotic medications cause deleterious reductions in cortical grey matter volumes? and (6) Are long-acting injectable antipsychotics more effective in reducing relapse rate compared to oral formulations?
Results:
There is reliable evidence for schizophrenia being a progressive disease with emergent treatment resistance in most cases, that relapse contributes to this treatment resistance, that maintenance antipsychotic medication should not be discontinued in remitted first-episode patients, that antipsychotic medication does not appear to cause deleterious grey matter volume changes, that maintenance antipsychotic medication reduces the mortality rate in schizophrenia and that long-acting injectable antipsychotics are more effective in preventing relapse than oral formulations.
Conclusion:
There is an urgent need to re-engineer the early management of schizophrenia and to routinely evaluate this type of innovation within practice-based research networks. A proposal for an assertive treatment algorithm is included.
Introduction
The standard index of progress being made in a disease field at a population level is mortality rate (MR) – greater treatment effectiveness indicated by reductions in the MR of patients over time. Other metrics used to compare outcomes across disease areas, which capture both fatal and non-fatal health losses, are quality-adjusted life years (QALYs) or disability-adjusted life years (DALYs); however, rarely are sets of time series data on these indices collected: certainly they do not exist for mental disorders (Doessel et al., 2010). Despite the partial nature of MR as a health outcome measure, it has been informatively applied to mental disorders, where there is a clear trend for mental disorder–related MR to be increasing in Australia over time (Doessel et al., 2010), this trend being particularly marked for people with schizophrenia (Saha et al., 2007). Meta-analysis of MRs of people with schizophrenia show that in the 1970s standardised MRs were increased 1.84-fold over those of the general population, in the 1980s they were increased 2.98-fold and in the 1990s they were increased 3.20-fold (Saha et al., 2007). These high MRs appear likely to have continued into the last decade (Reininghaus et al., 2015; Torniainen et al., 2015). That is, mental illness is the only broad disease field in the Australian healthcare system that has not shown at least numeric improvement in MRs in recent decades (Doessel et al., 2010), with people with schizophrenia showing a large deterioration in MRs (Saha et al., 2007).
Complementing studies of MR are morbidity data suggesting that low treatment effectiveness for people with schizophrenia should be of concern. First, there is evidence that the overall recovery rate in schizophrenia is very low, when strictly defined as it was in the most recent meta-analysis of longitudinal studies of schizophrenia (Jaaskelainen et al., 2013). This meta-analysis, which included 8994 patients from 20 different countries including Australia, estimated the median recovery rate to be 13.5% – that is, for every 100 patients with schizophrenia, only 1 or 2 will meet recovery criteria per year. As Jaaskelainen et al. note, their most ‘sobering’ finding was that studies from recent decades reported numerically the lowest recovery rates. Second and also consistent with reduced or at least non-improving treatment effectiveness are the two recent Australian national surveys of people living with psychosis carried out 10 years apart in 1997–1998 and 2010 (Morgan et al., 2012). In the 10 years between the two national surveys of people living with psychosis, there were no measurable improvements in major indicators of disability. Specifically, these surveys (Morgan et al., 2012) show that pension rates had not changed (86.9% in 1997–1998 vs 87.4% in 2010), and there was a numeric increase in rates of deterioration from premorbid level of function (80.2% in 1997–1998 vs 93% in 2010) despite there being equivalent relatively high rates of good premorbid work/social adjustment prior to first presentation (68.0/65.6% in 1997–1998 vs 69.0/64.9% in 2010). Also, there was almost a doubling of rates of lifetime co-morbid drug abuse/dependence (30.4% in 1997–1998 vs 56.4% in 2010). Considering that government expenditure on Australian public mental health services more than doubled across the same period of time (Department of Health and Ageing, 2013: Figure 5), the figures above indicate a need for change in clinical practice if additional investment is to show measurable improvements in health outcomes for people with schizophrenia.
This paper is predicated on the view that health outcomes and therefore treatment effectiveness are deteriorating over time for people with schizophrenia, although this view may be contrary to the position adopted in the recently published revision of the Royal Australian and New Zealand College of Psychiatrists (RANZCP) Clinical Practice Guidelines (CPG) for the Management of Schizophrenia and Related Disorders (Galletly et al., 2016; hereafter referred to as the 2016 RANZCP CPG). This review is also based on the assumption that confidence of clinicians to diagnose schizophrenia early, and provide assertive and long-term care, may be being undermined by a series of uncertainties and controversies in the published literature, which include discrepancies in CPG. These controversies are the subject matter of this review.
Approach to the reviewing process
The six clinical issues reviewed were selected because (1) the authors considered them highly relevant to the clinical practice of psychiatrists treating schizophrenia and likely to be impactful on health outcomes, (2) they have been the subject of extended and unresolved debate in the published literature and (3) their controversial nature is reflected in discrepancies across influential sets of CPG. Six questions that confront clinicians are as follows: (1) Is schizophrenia a progressive disease? (2) Does relapse contribute to treatment resistance? (3) When should the diagnosis of schizophrenia be made? (4) Should maintenance antipsychotic medication be discontinued in fully remitted first-episode patients? (5) Do antipsychotic medications cause deleterious reductions in cortical grey matter volumes? (6) Are long-acting injectable antipsychotics (LAIAs) more effective in reducing relapse rate compared to oral formulations?
This critical review results from a series of focused literature searches on each of the six questions. Although a systematic review would have been desirable, a critical review approach was the only feasible way to integrate the vast literature and to advance an understanding of the issues arising. Selection of material was strongly weighted by relevance, after fatally flawed studies were excluded. The review suggests that a re-engineering of the first hospital admission might substantially raise the standard of care. The word ‘patients’ with schizophrenia is used with the aim of conveying a sense of doctor responsibility for leading practice reform. The review is presented under the six question subheadings.
Is schizophrenia a progressive disease?
The notion of disease progression in schizophrenia is often conceptualised as involving neurodegenerative cell loss as Kraepelin initially proposed, but obvious cell loss has not been confirmed in post-mortem brain tissue studies of schizophrenia (Joshi et al., 2015). In a recent paper titled ‘The myth of schizophrenia as a progressive disease’, leading researchers (Zipursky et al., 2013) argued that schizophrenia is not inherently progressive at all, despite the well-established finding of progressive magnetic resonance imaging (MRI)-indexed grey matter volume loss occurring following the first episode, a finding not disputed by these researchers. Although Zipursky et al. concur with us that ‘the majority of people with schizophrenia have the potential to achieve long-term remission and full recovery’, logically they appear to call into question the value of assertive early intervention because it can be argued that a non-progressive disease does not require specialised early intervention as a major priority and that indeed early and sustained treatment may represent a serious risk as these researchers propose that antipsychotic medication exposure rather than disease progression accounts for much of the accelerated brain volume loss after the first episode (see Question 5 below), loss that has been linked to a worse prognosis (Van Haren et al., 2008). The 2016 RANZCP CPG endorsement of a staged model for schizophrenia appears to give tacit support for schizophrenia being a progressive disease, as this review concludes.
Progression could be a more subtle molecular level process, yet still cause persistent or irreversible effects such as progressive emergence of treatment resistance. Most patients (65–69%) have a good premorbid function (Morgan et al., 2012) consistent with the possibility that they may have the prospect of a good long-term outcome (Wiersma et al., 1998). Antipsychotic drug treatment is extremely effective in the first episode of schizophrenia with at least 70–80% of patients achieving a full remission in the short term (Lieberman et al., 1993; Malla et al., 2006; Zipursky et al., 2013). Put another way, at illness onset only 20–30% of patients show significant treatment resistance when first treated with antipsychotic medication. After two trials of antipsychotics, one of which should preferably be an LAIA (2016 RANZCP CPG), this subgroup of patients is immediately eligible for clozapine and other effective treatment strategies and should receive these in a timely manner. Irrespective of the favourable outcomes at the first episode, overall the rate of recovery for the total population of patients with schizophrenia declines to 13.5% (Jaaskelainen et al., 2013). This decline in treatment responsiveness appears to occur during the 5 years after the first episode (Robinson et al., 2004). In the seminal Hillside Hospital first-episode schizophrenia study, 84% of patients recovered (i.e. 16% did not remit) from the first episode (Lieberman et al., 1992). However, within 5 years of first presentation, 86.3% of patients failed to meet full criteria for recovery (Robinson et al., 2004). That is, in this study, 70.3% (i.e. 86.3%–16%) of the patients who achieved full remission after the first episode developed treatment resistance by the 5-year time point (Robinson et al., 1999, 2004). The major treatment history events that interceded between the high recovery rates at first episode and the low recovery rates 5 years later were repeated episodes of non-compliance and relapse, with at least 80% of patients in this expert treatment study relapsing in the intervening period (Robinson et al., 1999). This leads to the question of whether relapse has a mediating role in the emergence of treatment resistance after the first episode.
Does relapse contribute to disease progression and treatment resistance?
An obvious conundrum is that schizophrenia goes from being a relatively treatment-responsive disorder at first presentation to one that is treatment resistant in almost all multi-episode patients. Robustly supporting the likelihood that relapse is directly associated with progressive emergence of treatment refractoriness and psychosocial deterioration is the body of literature that shows (1) there are step-wise increases in the number of patients who do not recover (i.e. who do not respond well to medication if received) after successive relapses (Bleuler, 1978 [1972]; Ciompi, 1980; Emsley et al., 2012, 2013; Shimazono, 1973; Watt et al., 1983; Wiersma et al., 1998); (2) there is increased time to antipsychotic treatment response for recurrent episodes versus first-episode schizophrenia (Emsley et al., 2012, 2013; Lieberman et al., 1996; Wyatt, 1991); (3) the dose of medication needed to achieve remission in first-episode patients is lower than that recommended for multi-episode patients (McEvoy et al., 1991; Merlo et al., 2002; Oosthuizen et al., 2004); and (4) un-medicated patients who are allowed to relapse and subsequently placed on medication do not achieve the same level of remission compared with patients maintained on medication who do not relapse (Gopal et al., 2011; McEvoy et al., 1991; Merlo et al., 2002; Oosthuizen et al., 2004; Wyatt, 1991). Duration of relapse, defined as the sum of the duration of all relapse episodes that occurred between MRI scans, has been reported to be related to the extent of brain volume changes (Andreasen et al., 2013). In a cohort study in which 80% of patients deteriorated over a 7-year follow-up period, there was a highly significant correlation between the number of relapses and degree of social deterioration (Curson et al., 1985).
These studies are clinical cohort studies and only offer evidence of an association between relapse and emergent treatment resistance. They raise the question of whether the treatment resistance emerging after the first episode would have happened irrespective of what treatment the patient received. That is, are relapses simply a manifestation of a pre-existing genetic and developmental proneness to treatment resistance that is hard-wired into the brain prior to the first episode in poor prognosis patients? Or in 70–80% of patients is emergent treatment resistance induced by long periods of non-adherence to antipsychotic medication and multiple prolonged relapses (similar to the relationship between duration of illness/number of relapses and evidence of disease progression/poorer outcomes in major depression and bipolar disorder [Bora et al., 2010; Sheline et al., 2003; Treadway et al., 2015]). The main argument for relapse as the cause of treatment resistance in schizophrenia is the temporal relationship between the two: relapses occur before treatment resistance emerges. Particularly compelling studies are those of un-medicated patients who are allowed to relapse and who are subsequently placed on medication. These patients do not achieve the same level of remission compared with patients maintained on medication who do not relapse (Gopal et al., 2011; McEvoy et al., 1991; Merlo et al., 2002; Oosthuizen et al., 2004; Wyatt, 1991). In studies of patients with disease onsets occurring substantially before the discovery and introduction of antipsychotic medication, the greater duration of untreated illness is associated with greater gross functional deterioration (Scully et al., 1997; Waddington et al., 1995), suggesting in these patients that the delay in treatment contributed to poor prognosis independently of constitutional predisposition. However, is the converse true: Is avoidance of relapse associated with better long-term outcomes? We are aware of only one first-episode study with long-term follow-up (up to 9 years) in which adherence was very high and relapse rate was very low (Girgis et al., 2011). In this study of 160 Chinese patients living in China randomised to either clozapine or chlorpromazine for up to 2 years and thereafter given naturalistic treatment, adherence was objectively monitored using pill counts, and remission/relapse status was the primary outcome measure. Patients took medication most days over the 9-year follow-up (77% for clozapine and 66% for chlorpromazine), and there were few relapses (about 10% of patients relapsing over the 7-year period). In contrast to long-term follow-up studies of patients with poor adherence, high relapse rates and poor outcomes, Girgis et al. found that high levels of adherence and low relapse rate were associated with maintenance of remission status 9 years after the first episode (78% for both groups). Regrettably, there is not a single biological study that directly assesses the pathophysiological consequences of relapse and whether some of the brain changes associated with relapse are permanent and cause emerging treatment resistance. This type of study would require a large multi-centre sample, long-term follow-up and repeated biomarker assessment in and out of relapses, and on and off medication. Currently, such a clinically important study is not likely to happen in Australia under current research funding processes.
Clinicians are reminded that CPG only offer guidance: they are not based on certainty; all treatment recommendations have only a probability of being correct. Clinical judgement remains the final arbiter. Until there is absolute adequacy of research, clinicians are individually left to decide whether or not to prioritise relapse prevention as the most powerful modifiable risk factor for long-term poor outcome in schizophrenia. Most experienced acute care clinicians know too well that keeping remitted first-episode patients on maintenance medication avoids the worst aspects of the otherwise almost inevitable deterioration in psychosocial function that currently occurs in most patients (Robinson et al., 1999, 2004). The main problem clinicians confront in keeping first-episode patients well is how to maintain long-term medication adherence. Irrespective of gaps in direct evidence about the damaging effects of relapse, one might think that the deteriorating outcomes for schizophrenia associated with our current system might stimulate urgent innovation and evaluation of assertive approaches to the prevention of relapse right from the first episode, approaches that may also be effective in reducing rates of suicide, co-morbid substance misuse and physical health co-morbidity and for these approaches to be considered best practice. But these approaches require that the diagnosis of schizophrenia be made as early as possible.
When should the diagnosis of schizophrenia be made?
An unfortunate by-product of the early psychosis intervention paradigm has been the encouragement of delayed and imprecise diagnosis, especially in the case of schizophrenia. There are explicit statements discouraging clinicians from making and telling patients about the diagnosis of schizophrenia in early psychosis training manuals:
An early and definitive diagnosis of schizophrenia, for example, may damage the patient and family, by stigmatising them and affecting the way that they are viewed and managed by healthcare professionals. In addition, such a diagnosis does not contribute anything positive in terms of guiding treatment. (McGorry and Edwards, 1997)
This advice has persisted into the second edition of the Australian Clinical Guidelines for Early Psychosis (ACGEP; Early Psychosis Guidelines Writing Group, 2010):
the traditional pessimism associated with the diagnosis of schizophrenia has permeated professional and popular culture to some extent. Making a rigid and too specific diagnosis may therefore not only be unreliable but have iatrogenic effects on both the clinician and client optimism and the potential for recovery.
As far as the authors are aware, schizophrenia is the only disease for which CPG encourage delayed diagnosis. Delay appears to be justified on two grounds. One purported reason is the belief that the diagnosis of schizophrenia is unstable over time, despite this view not being supported by empirical evidence (Farooq et al., 2016). On occasion, the initial diagnosis of schizophrenia will be wrong, so regular diagnostic review especially in the first 6–12 months is essential. The other reason appears to relate to the belief that disclosure of bad news will cause anguish and deny patients hope: this old fashioned view has been addressed by communication training for clinicians in physical medicine (Farooq et al., 2016).
Not making the diagnosis of schizophrenia as early as possible may have serious consequences if it leads to a less assertive approach to medication adherence and relapse prevention, and not urgently providing psychoeducation about the need for long-term maintenance antipsychotic therapy as soon as the diagnosis is made. Currently, advice against early diagnosis appears to be coupled with giving medication adherence a lower priority by proponents of early psychosis services. That is reflected in an absence of recommendations about evidence-based objective adherence monitoring (e.g. electronic medication event monitoring, pill counts or checking pharmacy refill records). There is no reference to evidence-based adherence improvement interventions (e.g. multi-component interventions combining unit-of-use packaging, patient motivational counselling and family psychoeducation [Dolder et al., 2003; Valenstein et al., 2011; Velligan et al., 2008; Zygmunt et al., 2002]) when oral antipsychotic formulations are prescribed, in either the 2016 RANZCP CPG or the ACGEP.Compounding this issue is the inclusion of highly ambivalent or negative statements about the use of LAIA, e.g., in the 2005 RANZCP CPG Team for the Treatment of Schizophrenia and Related Disorders (2005) it is stated that ‘Excessive use of depot antipsychotics as a crude response to the widespread lack of adherence to oral medications had been another unfortunate feature of the landscape of care, especially in Australia’. This sentiment dilutes advice against early use of LAIAs in the 2016 RANZCP CPG: ‘Oral SGAs should be prescribed as first- and second line treatments for people with FEP’. These recommendations may be affecting the practice of early psychosis clinicians who appear to typically use oral formulations without implementing evidence-based adherence monitoring and improvement interventions (Brown and Gray, 2015; Farooq and Farooq, 2014). If the diagnosis of schizophrenia is made, objective adherence monitoring and improvement interventions are arguably essential in all cases where oral antipsychotic medications are prescribed because patient self-report of their adherence to antipsychotics and the doctor’s opinion about which of their patients are adherent or non-adherent with oral antipsychotics are completely unreliable (Byerly et al., 2007; Velligan et al., 2007), and because of the high rates of service disengagement and non-adherence particularly in first-episode patients (see Question 6 below and the ACGEP). Given the major treatment implications of the diagnosis of schizophrenia for early and sustained care, it is in the patient’s interest to make this diagnosis as early as possible.
Should maintenance antipsychotic medication be discontinued in fully remitted first-episode patients?
There are marked discrepancies across influential CPG and medication algorithms about the recommended period of maintenance antipsychotic medication and if and when to discontinue it (Takeuchi et al., 2012). Takeuchi et al. identified 14 CPG and medication algorithms and found that only 5 had clear definitions of the maintenance phase and its treatment; 6 of them did not argue against antipsychotic discontinuation after 1–2 years of treatment in patients with first-episode schizophrenia, while in chronically ill patients, 10 of the 11 recommended continuation of medication for 5 years but not indefinitely. The 2016 RANZCP CPG do not recommend against discontinuation or for indefinite maintenance antipsychotic medication in patients with schizophrenia: ‘The person should have made a full recovery and been well for at least 12 months before cessation of medication is considered’. The ACGEP also do not give recommendations for long-term (indefinite) medication for schizophrenia: ‘There is no clear evidence in FEP as to the period of time following remission that an individual should stay on an antipsychotic medication’, but later states, ‘This suggests maintenance treatment as a rule of thumb if remission has been achieved for six months or less; at least one year following remission would be recommended on current practice and previous placebo controlled trials …’. Reinforcing a permissive attitude towards medication discontinuation has been the prominence given to a recent multi-flawed study (Wunderink et al., 2013), prominence added to by its citation in the 2016 RANZCP CPG. Wunderink et al. concluded but did not demonstrate that long-term recovery rates might be higher in remitted first-episode patients with schizophrenia who discontinue medication 6 months after remission. Because of the unacceptable quality of the study (the 2016 RANZCP CPG list fiveserious flaws in the study, but there were others including the following: highly questionable blinding in the first 2 years of the study, and no blinding whatsoever from 2 to 7 years; selective exclusion of patients likely to be uncooperative; and low power making any finding unreliable),this is an invalid conclusion, and flies in the face of the overwhelming evidence of the benefits of maintenance medication, especially in remitted first-episode patients (see below; Gaebel et al., 2016). Antipsychotic medication is highly effective in preventing relapse. A recent systematic review of antipsychotic discontinuation studies in remitted first-episode patients with a schizophrenia-related diagnosis who had been stabilised on medication for an average of 15 months (range: 12–24 months) showed that discontinuation of medication was associated with a 77% relapse rate by the end of the first year and 90% relapse rate by the end of the second year, while the 1-year relapse rate in patients who continued maintenance mediation was 3% (Zipursky et al., 2014).
Apart from relapse prevention, what else has the patient to gain from maintenance antipsychotic medication? Even if you question whether maintenance medication prevents emergent treatment resistance, there are other major benefits. First and foremost, maintenance medication is a life-saving intervention, especially in first-episode patients (Torniainen et al., 2015). In first-episode schizophrenia patients who do not receive antipsychotic medication, the relative MR is 10 times that of the general population, whereas the relative MR only shows a twofold increase in those taking average doses of antipsychotic medication (Torniainen et al., 2015). One of the saddest results of how we currently treat schizophrenia is the 20-fold increase in suicide rate in first-episode patients during the first 10 years of their illness compared to region-matched general population controls (Reininghaus et al., 2015). Relapse (and chronic residual psychotic symptoms) has many distressing consequences, especially for young people who have multiple socially and vocationally disastrous relapses (Ascher-Svanum et al., 2006), but the risk that overshadows all others is the risk of suicide. Although the life-saving benefits of antipsychotics are apparent at all stage of the illness (Torniainen et al., 2015), they are most obvious in the early years after first presentation. Despite evidence of adverse metabolic effects of antipsychotics, these effects were not found to contribute at all to the raised MR in schizophrenia in this large (involving an entire national Swedish sample of 21,492 patients with schizophrenia and 1230 patients with first-episode schizophrenia prospectively followed up) methodologically sound study (Torniainen et al., 2015), clearly implicating unhealthy life style behaviours (e.g. smoking) and poor preventive medical care as the major culprits in relation to cardiovascular-related mortality in patients with schizophrenia. For unknown reasons, this high-quality pivotal study containing critically important findings for clinical practice was not cited in the 2016 RANZCP CPG.
Our review strongly supports an early intervention approach to treatment of schizophrenia: making the diagnosis early and initiating assertive long-term care as soon as possible. The difficulty in finding the right language to initially inform patients and their families that long-term care is indicated so early in their treatment should not be under-estimated: nor the difficulty in overcoming insight deficits with the effective use of psychotherapeutic frameworks that have been developed in relation to the cognitive treatment of delusions, motivational interviewing or narrative therapy (see Table, Supplementary Material). However, effective early intervention implies these efforts are critical, and one aim of this review is to increase clinician confidence in presenting the case for long-term maintenance medication: discontinuation of medication early or late in the illness denies the patient a life-saving intervention. It is most effectively started at the first episode (Torniainen et al., 2015), an intervention that may offer the patient the best chance of maintaining long-term recovery.
Do antipsychotic medications cause deleterious reductions in cortical grey matter volumes?
What has the patient to lose by continuing maintenance antipsychotic medication? There are researchers (e.g. Zipursky et al., 2013) who attribute much of the progressive grey matter volume loss seen after the first episode to antipsychotic medication and not the disease process itself. Given that volume loss is related to poor prognosis (Van Haren et al., 2008), one might reasonably assume that the loss is deleterious. Therefore, this controversy creates a quandary faced by proponents of long-term antipsychotic medication, who may have to make the opposing case in discussions with patients and their families, requiring a full understanding of the relevant findings. While three meta-analyses have reported a statistical association between higher antipsychotic medication dose and increased grey matter volume reduction (Fusar-Poli et al., 2013; Haijma et al., 2013; Vita et al., 2015), all of the studies included in these meta-analyses were not experimentally designed to test the hypothesis that antipsychotic medication causes grey matter volume loss and are confounded by indication; i.e., poor prognosis patients who lose brain volume faster are likely to be given higher doses of medication by indication. In an attempt to control for this type of confounding, researchers statistically ‘partial out’ the effect of prognosis using ad hoc measures of prognosis they may have collected. However, satisfactory measures of illness prognosis were not collected a priori. Indeed, measurement of prognosis is not currently possible as the pathophysiology of schizophrenia remains unknown. That is, these meta-analyses are of clinical interest but do not provide proof that medication causes grey matter volume loss, leaving the alternative more probable explanation for the loss being related to disease processes. The view that volume loss is related to antipsychotic medication rather than disease progression is also challenged by evidence from studies of medication-naïve schizophrenia patients in the prodromal phase (Pantelis et al., 2003), at first episode (Ren et al., 2013) and with chronic long-term illness (Zhang et al., 2015), clearly showing sequential brain volume changes.
However, if weight is given to any aspect of these meta-analyses, it should be given to the most recent and largest meta-analysis of cohort studies assessing the effect of medication on grey matter volume changes (Vita et al., 2015), which not only refuted the idea that second-generation (atypical) antipsychotic medications are associated with loss of grey matter volume but also reported that these medications, if they do anything to grey matter volume, either slow or reverse the accelerated rate of grey matter volume loss observed in first-episode schizophrenia patients. Importantly, this association is unlikely to be confounded by indication because patients with less volume loss tend to have better prognosis and not have an indication for higher doses of medication. This interpretation is consistent with evidence of neurotropic actions of these drugs (Fernandes et al., 2015; Kusumi et al., 2015). Also, there are studies showing second-generation antipsychotics either prevent loss (Lieberman et al., 2005) or reverse it (Van Haren et al., 2007). There are antipsychotic challenge studies in healthy non-human primates that show cortical volume loss, but again none of these studies should be given any weight in the clinic because whether there was dopamine D2 receptor occupancy in the treated animals comparable to that associated with human therapeutic use was not determined. Antipsychotic dosing in animal studies tends to be in substantial excess of what induces therapeutic levels of D2 occupancy in humans, as we found in a rodent study (Naiker et al., 2006). In summary, the clinician should have confidence in recommending long-term use of antipsychotic medication for schizophrenia in the knowledge that grey matter volume reductions seen in schizophrenia are almost certainly disease-related and that second-generation antipsychotic medication, if anything, protects against these volume changes.
Are LAIAs more effective in reducing relapse rate compared to oral formulations?
This question challenges the belief that LAIAs are no more effective than oral formulations. This belief is based on meta-analysis of randomised controlled trials (RCTs) of oral versus injectable medications (Kishimoto et al., 2014; Leucht et al., 2011), which find little advantage for LAIAs over orals. The view that RCT methodology is always the best design to test intervention effectiveness, promoted by the Cochrane Reviews, on occasion may have the potential to mislead schizophrenia CPG designers. For certain interventions, RCTs can result in completely invalid conclusions (Catts et al., 2010; Kane et al., 2013). This is because totally inappropriate patients, who can comply with an experimental protocol over long periods of time, are recruited to such studies providing no useful information about the treatment of real-world patients. Because eligible patients for RCT studies of interventions such as LAIAs and community treatment orders are rare and completely atypical, samples sizes are very often unacceptably low, a methodological fault hidden by agglomerating data in meta-analysis. But the faults remain – in a recent meta-analysis of LAIA versus oral formulations (Leucht et al., 2011), the median sample size of included RCTs was 55 patients – unacceptable in any other field of medicine. For this type of intervention, large-scale epidemiologically sound studies that include complete samples of real-world patients are far superior. There is a landmark study of this calibre assessing the effectiveness of LAIAs involving the total national population (avoiding ascertainment bias) of schizophrenia patients in Finland, with unbiased methods for determining medication use and rates of re-admission to hospital (Tiihonen et al., 2011). This study found that real-world patients with schizophrenia taking LAIA medication had one-third the rate of re-hospitalisation. Although this methodologically sound study is much more applicable to clinical practice than the 10–20 small RCTs bundled into meta-analysis, it was not cited in the 2016 RANZCP CPG for schizophrenia. Additionally, a systematic review of mirror-image studies found similarly large benefits in favour of LAIAs (Kishimoto et al., 2013), another study not cited in the 2016 RANZCP CPG. We believe these observational studies should leave no doubt in the clinician’s mind that LAIAs are best practice as first-line treatment in all patients as soon as the diagnosis of schizophrenia is made, when there is no obvious contra-indication. Logically, their prescription should begin at the first hospital admission and be continued indefinitely for three main reasons: (1) non-adherence with oral antipsychotics occurs early – within 60 days post-hospitalisation in first-episode patients – in about 60% of patients (Tiihonen et al., 2011); (2) this high level of non-adherence with oral antipsychotics persists into the chronic phase of the illness (Dolder et al., 2002; Gilmer et al., 2004; Lacro et al., 2002; Velligan et al., 2003); and (3) psychiatrists are completely unreliable in determining which of their patients are non-adherent (Byerly et al., 2007; Velligan et al., 2007). We are not alone in recommending LAIAs as best practice: there are highly respected CPG that recommend LAIAs as maintenance treatment from the first episode of schizophrenia (Llorca et al., 2013), contrary to the recommendations in the 2016 RANZCP CPG.
Proposal for change: re-engineering the first hospital admission for schizophrenia
In this paper, we propose that the first psychiatric admission to hospital for psychosis, especially into public acute psychiatry wards, be radically re-engineered (see Figure 1). Rather than discharge the patient with an indefinite diagnosis of early psychosis or drug-induced psychosis, every effort is made to establish whether the patient has the typical developmental and prodromal trajectory of schizophrenia – and if so, the diagnosis of schizophrenia be made then and there. In accordance with the 2016 RANZCP CPG, this will involve comprehensive investigation to exclude non-psychiatric medical conditions (e.g. encephalopathies, including that mediated by N-methyl-D-aspartate [NMDA] receptor autoantibodies; temporal lobe epilepsy; cushing disease; thyroid disease; Vitamin B12 deficiency; ovarian/small cell lung cancer; diabetic hypoglycaemia; hyponatraemia; hypercalcaemia; hypocalcaemia; hypomagnesaemia; systemic lupus erythematosus; cytogenetic abnormalities; Wilson’s disease; porphyria) (Freudenreich et al., 2009; Griswold et al., 2015). Urine analysis and blood levels should be checked for substance- and medication-induced disorders (e.g. anticholinergics, digoxin, steroids, narcotics, cimetidine, anti-Parkinson’s disease drugs) (Freudenreich et al., 2009; Griswold et al., 2015). Occasionally, the initial diagnosis of schizophrenia will be wrong, and in fact the patient will have bipolar disorder or borderline personality disorder, so regular diagnostic review especially in the first 6–12 months is essential particularly in those patients who do not achieve a full remission with medication. Then, while still in hospital, in all patients who reach diagnostic criteria for schizophrenia (irrespective of their history of substance abuse), the key aspects of preventive intervention for psychotic relapse, suicide, and physical healthand substance use co-morbidity be initiated (see Table, Supplementary Material). This will involve engagement of the family and patient in comprehensive and optimistic patient-focused psychoeducation which includes giving reasons for the critical necessity of long-term maintenance medication. In particular, the patient and family need to be informed of the evidence for the superiority of LAIAs over oral formulations in preventing re-admission (Tiihonen et al., 2011). But if the doctor fails to convince the patient of the value of LAIAs (psychiatrists appear to be poor advocates for LAIAs [Weiden et al., 2015]), then an evidence-based adherence improvement intervention (Dolder et al., 2003; Valenstein et al., 2011; Velligan et al., 2008; Zygmunt et al., 2002) needs to be immediately initiated with all patients using oral medication. Assertive management of unsatisfactory response overall, or in terms of positive or negative symptoms, co-morbid depression, anxiety and substance abuse or in cognitive deficits, will increase rates of sustained recovery after the first episode (see Table, Supplementary Material). Risk assessments should not only trigger safety procedures but also focus treatment on preventive management of treatment resistance. By the time of first presentation, many patients have already moved towards an inactive life style, started to smoke and made unhealthy dietary choices, which render them highly susceptible to the pro-metabolic effects of antipsychotic medication. An assertive preventive physical healthcare programme (which includes dental health; Wey et al., 2016) must be immediately begun and sustained. The general practitioner can play a critical role in facilitating access to the many effective treatments and encourage the patient and their family to aim at a full recovery.
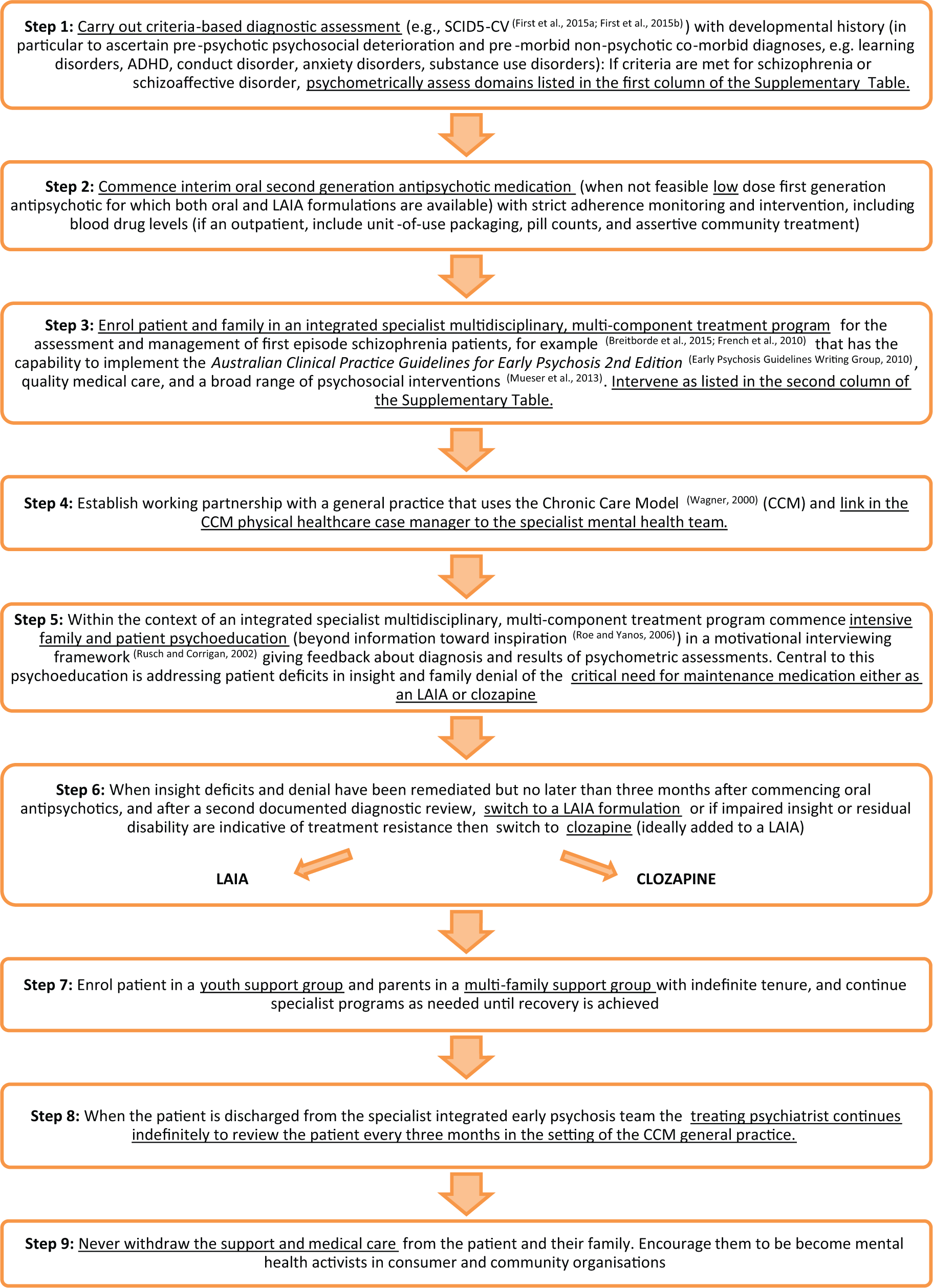
Proposal for a re-engineered treatment algorithm for first-episode schizophrenia.
Conclusion
Schizophrenia is a disease in which 80% of patients respond very well to standard antipsychotic drug treatment at first presentation, and there are effective treatment strategies including introduction of clozapine that could prevent further deterioration in the remaining 20%. Emergent treatment resistance, which occurs in 70% of remitted first-episode schizophrenia patients, is potentially avoidable. Relapse prevention is the strongest modifiable risk factor for emergent treatment resistance. The evidence reviewed indicates that a major reduction in the occurrence of emergent treatment resistance will involve more frequent use of LAIAs as maintenance medication from the first episode of schizophrenia, and early introduction of clozapine as soon as eligibility criteria are met. LAIAs appear to be particularly applicable in resource-constrained service settings (Chiliza et al., 2016). However, the application of the principles of personalised medicine to patients with schizophrenia will depend upon future research that directly studies the pathophysiology of relapse, remission and treatment resistance. This urgent research priority will be feasible only within the framework of health service – health practitioner – clinical researcher partnerships. Our mental health system needs to be held accountable. One way of doing this is to evaluate the impact of implementing best practice in services adopting it. This could be done either as a sub-study in the next national survey of people living with psychosis, or evaluation could be carriedout routinely by establishing Practice-Based Research Networks (McMillen et al., 2009). We can defeat the worst aspects of this disease now – by collaborating together, we can certainly manage it vastly better than we currently do.
Footnotes
Declaration of Conflicting Interests
S.V.C. has received funding for acting in the role of an advisory board member, as a sponsored educational speaker and for research projects from the following pharmaceutical companies: Janssen-Cilag Pty Ltd, Eli Lilly Australia Pty Ltd, Lundbeck Australia Pty Ltd, Novartis Pharmaceuticals Australia Pty Ltd, Pfizer Australia Pty Ltd, Bristol-Myers Squibb Pty Ltd, Sanofi-Aventis Australia Pty Ltd, Hospira Australia Pty Ltd and AstraZeneca Pty Ltd. He is a Trustee for the Psychosis Australia Trust and the Queensland Schizophrenia Research Foundation. He is a board member of Clearthinking Queensland Ltd. B.I.O has no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.