
Abstract
Globally, youth mental health services are evolving, with Australia’s headspace services presented as a leading exemplar. headspace services were designed as enhanced primary care-based entities and were expected to collaborate with local acute, and specialist clinical and psychosocial services. The lack of large-scale health services trials necessitates understanding their impact through systematic monitoring and evaluation. This paper compares data from differing sources that describe the demographic and clinical features, and functional outcomes, of young people presenting to various headspace services. headspace National reports that care is provided largely to youth with transient distress, minimal clinical disorders, suicidality or comorbidities and limited functional impairment. Almost 50% of clients are reported to have no significant psychological symptoms or risk factors, and less than 30% to have a clinical disorder. Consequently, 36% receive only a single session of care and the median number of clinical sessions provided is three. By contrast, empirically derived estimates, utilising data from an academic centre and its affiliated centres, other independent agencies and more refined analyses of headspace national data variously portray 50–60% of youth as presenting with at least moderate clinical complexity (including at least 20% with high complexity), and with another 27% requiring active clinical intervention. Together, these data suggest approximately 75% of attendees require substantive clinical care. Clinical outcomes data from all sources indicate limited impacts on functional outcomes, with less than a third achieving significant improvement. These data support the original intent of headspace services to focus on equitable access to multidimensional and clinical assessment, evidence-based early interventions for early stages of major anxiety, mood or psychotic disorders. As demand for youth services continues to rise, there is an urgent need to reconfigure our national youth service networks to address the unmet clinical and psychosocial needs of youth presenting in the early stages of major mental disorders.
Many countries, including Australia, are engaged in building new models of youth mental health care (McGorry et al., 2022, 2024). These are appropriate responses to the epidemiology of adolescent-onset mental disorders (McGrath et al., 2023), and they reflect global recognition of the long-term neglect of indicated prevention, early intervention and secondary prevention by traditional mental health services in this age group (McGorry et al., 2022, 2024; Uhlhaas et al., 2023).
Australia is at the forefront of these new models due largely to the pioneering work from Orygen, the National Centre of Excellence in Youth Mental Health (McGorry et al., 2022; Uhlhaas et al., 2023). In the 1990s, Orygen developed and evaluated early intervention for first-episode psychosis (McGorry et al., 2002, 2008). This led to the global transformation and revitalisation of early intervention services for young people with emerging and first episodes of psychosis (Uhlhaas et al., 2023).
In 2007, with the establishment of headspace, Australia committed to developing a national network of enhanced primary care-based mental health assessment and brief intervention centres for any young person experiencing psychological distress. This central goal was embedded within other community-based activities to promote mental health literacy and early help-seeking by youth aged between 12 and 25 years of age, and link youth with a broader variety of psychological and psychosocial (not just medical) interventions. This followed extensive evidence about the mismatch between the typical age-of-onset of common anxiety, depressive and other comorbid disorders (Kessler et al., 2005) and the provision of appropriate youth-specific health services (McGorry et al., 2007). The deficits in clinical care, particularly with a lack of access to appropriate psychological services, had been well documented (notably in primary care settings) in Australia (Hickie et al., 2001, 2007).
As of 2020, 16% of Australians (4.1 million individuals) were aged 12–24 years, with the most recent evidence indicating that 39% of those aged 16–24 years had a 12-month mental disorder (Australian Bureau of Statistics, 2023), up from 26% in 2007 (Australian Bureau of Statistics, 2008). Correspondingly, in 2021, 32% of youth aged 12–24 years received a Medicare-subsidised mental health service (this includes general medical and specialist psychological and psychiatric services), up from 28% in 2019. In addition, state-based mental health expenditure on youth aged 16–24 (largely hospital-based) has grown substantially in recent years ($3.64 per capita in 2010–2011 to $43 per capita in 2019–2020), with emergency department (ED) presentations for 18–24 year olds now reaching 209.3/10,000 in 2019–2020 compared with 121.61 for all ages. So, as psychological distress among young people continues to rise, and the demand for mental health services continues to grow rapidly, providing equitable and affordable access to high-quality care is increasingly challenging. These trends are clear in Australia, and globally (McGorry et al., 2024).
Given the emphasis in Australia on increasing access through enhanced primary care-based mental health services, the aim of this article is to present a variety of data sources, and analytic approaches, that report the differing demographic characteristics, clinical features and functional outcomes of young people who present across the network of headspace services. We aim to capture a detailed picture of the existing situation for those in early stages of major mental disorders. Hopefully, this detailed analysis will benefit the future design of a broader and more comprehensive network of youth mental health services.
headspace as the national primary care platform for youth mental health services
The original intentions of headspace services as set out in multiple reports (McGorry et al., 2007; Muir et al., 2009) were to:
develop a national network of enhanced primary care-based mental health services that could provide diagnostic assessment and a clear pathway to the range of medical and psychological services relevant to early stages of anxiety and depression;
facilitate access to appropriate specialist or emergency care for those with more advanced, complex or enduring mood or psychotic disorders, through appropriate partnerships with local state-funded or Medicare-supported services;
facilitate access to other health services for young people, notably for sexual health and alcohol and other substance misuse; and
link young people to appropriate education, employment, training and other relevant psychosocial or welfare services.
Enacting this last point was never going to be easy given Australia’s historic lack of investment in psychosocial services (i.e. funding being at around 6% of total mental health expenditure) (Rosenberg and Harvey, 2021). Prior to headspace, a range of non-clinical youth services, typically funded by local government or state-based health and welfare authorities, addressed some of the psychosocial needs of young people (e.g. welfare, housing, education and employment support).
While other networks of alcohol and substance misuse and sexual health services existed, many lacked capacity for mental health assessment or interventions for young people. headspace as a mental health and clinical service was intended to collocate, not compete, with the complementary primary care-based clinical and other psychosocial service partners provided by state and territory governments. Some available evidence suggests that initially headspace did add to earlier schemes that were also designed to provide brief psychological care (Bassilios et al., 2017). However, over time, the much-expanded Better Access Scheme (Rosenberg and Hickie, 2019) has come to be the dominant method by which the Commonwealth Government supports access to psychological care for all ages, including young people.
headspace national reporting of who attends, clinical characteristics, services delivered and outcomes achieved
The development of regionally based headspace services has been strongly supported by successive national governments, with rapid expansion from the initial 10 sites in 2007 to the operation of 154 sites by May 2022 (KPMG, 2022). The number of young people seen annually was reported to be 98,270 in 2018–2019 (113 sites, 870 young persons/site) and 90,110 in 2019–2020 (118 sites, 764 young persons/site). This represents a remarkable achievement in terms of providing direct and affordable access for young people to mental health services (Rickwood et al., 2014). The extent to which this has facilitated a substantial increase in absolute access for young people to psychological care is unknown, as headspace still appears to provide a relatively small proportion of the total number of Federal Government-subsidised mental health care services to young people.
The most recent independent review, published in June 2022 by KPMG (2022), notes that headspace services are still expected to operate across the domains of mental health and wellbeing, physical and sexual health, work and study (vocational) support and alcohol and other drug services. However, that analysis notes that, overwhelmingly, services are provided in the mental health and wellbeing domain (57.5%), with little activity for physical and sexual health, work and study (vocational) support and alcohol and other drug services (1.8%, 2.2% and 0.4%, respectively). That is, headspace operates primary care-based mental health care and not a wide variety of other services.
Of all episodes of care, 36% entail just a single occasion of service, and only 19% are associated with six or more occasions of service. This is consistent with the emphasis on expanding access via the provision of very brief psychological support, rather than more comprehensive medical, psychological, sexual health, alcohol or drug or psychosocial services.
Regarding outcomes, the KPMG report describes a shift away from the initial clinical focus on early intervention and secondary prevention for the early stages of major mental disorders. It now lists alternative ‘intermediate outcomes’ including increased mental health literacy, increased early help-seeking, increased access to required services and a focus on delivering each of these outcomes for ‘hard-to-reach’ groups (Aboriginal or Torres Strait Islander, culturally and linguistically diverse, LGBTQIA+, those with disability). These ‘intermediate outcomes’ are then differentiated from service system outcomes (e.g. advocacy, reducing stigma, improving care pathways), user experience outcomes (e.g. culturally appropriate and inclusive, family support, youth participation) and psychosocial outcomes (e.g. improving mental health and wellbeing, considering clinical outcomes and improving psychosocial outcomes).
The report concludes that these intermediate goals (e.g. improved mental health literacy) have been achieved to varying degrees. However, key challenges remain for achieving effectiveness in area-level outcomes, managing wait times, connecting with ‘hard-to-reach’ groups, connecting with the wider mental health service systems or achieving reliable or clinically significant improvements in most clients. Importantly the report concludes that ‘for those young people . . . who met clinical thresholds (moderate or above), the majority do not see a clinically significant change to their [psychosocial] outcomes’ (KPMG, 2022: 19).
Elsewhere in the same report, there is the following statement ‘young people who go on to access at least six to eight occasions of service achieve the greatest improvement in outcomes’ which seems to suggest that there is a relationship between the duration of clinical care provided and enhanced outcomes. This is consistent with the more general notion that for those with clear clinical syndromes, the provision of very brief interventions is insufficient to meet their needs. It is also in line with our previously reported data on the positive relationship between a longer duration of care and better clinical outcomes in those presenting to our headspace services (Cross et al., 2016).
The headspace national data set: cross-sectional and longitudinal reports
There are several academic reports of the headspace national data set. The cross-sectional data (Rickwood et al., 2014) provide limited information regarding key clinical features such as diagnosis, clinical stage, patterns of physical or mental health comorbidity, prior use of other primary care or specialist services, prior or concurrent use of psychotropic medications or levels of functional impairment.
In the most comprehensive data now available on 58,223 clients, 23.57% are reported to have no significant psychological symptoms and no risk factors, and a further 25.64% are reported to have risk factors only (Rickwood et al., 2023). This means that headspace staff are recording almost half of those young people attending as not requiring clinical interventions, while only 29.78% are recorded as reaching a threshold for a clinical disorder.
Of the presenting psychological symptoms (reported in n = 47,447), anxious and depressive features were most common (42% and 33%, respectively). For diagnosis, the most common were anxiety and depressive disorders (21.7% and 18.5%, respectively). Regarding the range of services provided, these reports only include data on psychological treatments, being largely of the cognitive-behavioural type (31%) followed by general or supportive counselling (12.5%). No data on concurrent use of medical therapies are presented.
By contrast, another academic report on 76,021 individuals accessing 113 different services in 2018–2019 has recently appeared (Gao et al., 2024). It provides a somewhat different perspective on the needs of those who attend, while also suggesting that there may be important differences between sites. Over 50% of persons were rated as having very high levels of distress (Kessler Psychological Distress Scale [K10] >30) and 46% had significantly impaired function (Social and Occupational Functioning Assessment Scale [SOFAS] <61). Using a data-driven approach, the authors conclude that at least 60% of attendees have at least moderate levels of complexity, with 20% being rated as highly complex. However, the dataset on which these analyses were based has limitations, particularly with regard to the extent that they relied on ratings of clinical staging and formal diagnoses by site staff.
Instruction to staff by headspace national as to how to apply clinical staging differed significantly from the initial research criteria (Hickie et al., 2013) and no specific training for site staff, or inter-rater reliability, has been established. Independently, the Brain and Mind Centre (BMC) has provided clinical staging training to multiple sites and, consequently, it has been clear that local application has resulted in both significant under-ratings (due to the belief that those with clinical stages 2 and above should be referred onto more specialised services) and over-ratings (where exposure to previous trauma, taking medication for an anxiety or depressive disorder or duration of symptoms of more than 12 months automatically results in a rating of stage 3 or 4). Similarly for clinical diagnoses, these were often not assigned in services that lacked access to clinical psychologists or psychiatrists. Consequently, the variations in the ratings of complexity across sites in the report by Gao et al. (2024) are much more likely to reflect major variations in the validity of data collected, as distinct from actual differences in the clinical characteristics of youths presenting.
On the basis of the complexity score developed by Gao et al. (2024), the proportion of youth rated as having low complexity (for whom a brief intervention or indicated prevention approach may be most appropriate) was recognised as 40% (range: 21–64% across centres), meaning that 60% had more complex needs (range: 36–79%) and were likely to require more substantive clinical interventions. This estimate (but not the range) is consistent with earlier work by the BMC group (Capon et al., 2023a) which also used an empirically based approach, and found that 49% of attendees had more complex needs, while another 27% were in need of significant early intervention. Using a standardised and reliable data collection method, we have estimated the range across headspace services for those in need of substantive interventions to be 44–81% for severe distress, 35–67% for previous trauma, 36–57% for low functioning and 12–37% for those receiving government benefits (Capon et al., 2023b).
The longitudinal data reported by headspace national are limited to those attending on more than one occasion (median of three occasions of service), with a focus on changes in symptoms, functioning or self-reported quality of life. For those in whom at least two of three outcome measures were collected, 63% came from the ‘no diagnosis’ subgroup compared with 37% from the diagnostic group. Due to limited response rates, no data were reported on medium-term outcomes.
Those followed in the short-term comprised 38% (22,349 of 58,223) of presenting clients. When considering how many had positive outcomes from service engagement, ‘reliable change’, indicative of ‘improvement’, was reported in 24.5% for psychological distress (self-reported K10), 29.9% for functioning (clinician-rated SOFAS) and 30.1% for self-reported quality of life (measured by MyLifeTracker). Clinically significant improvement on these same three measures was reported in 22.4%, 37.8% and 29.9%, respectively. Correspondingly, clients with ‘no change’ on these measures made up 69.5%, 56.2% and 64.9%; and deterioration occurred in 5.9%, 13.8% and 5.0%, respectively (Rickwood et al., 2023). In summary, in the short term, about one-third of clients improve and two-thirds largely remain the same or deteriorate.
These data were interpreted as demonstrating the effectiveness of headspace, noting that, From presentation to last service rating, over one-third [of young people] had significant improvements in psychological distress and a similar proportion in psychosocial functioning; just under half improved in self-reported quality of life. Significant improvement on any of the three outcomes was shown for 70.96% of headspace mental health clients. (Rickwood et al., 2023: 1)
The BMC experience and evidence from 2007 to 2022
Our first academically affiliated centre was established in Campbelltown in 2007 and the second in Central Sydney from 2012. From the outset, these centres have been committed to continuous reporting on who is seen at these sites, their demographic and clinical characteristics (Capon et al., 2023b; Hamilton et al., 2011; Scott et al., 2012) and their clinical and functional outcomes (Burton et al., 2022; Iorfino et al., 2022a; Scott et al., 2019). Consistent with the BMC Youth Model (Hickie et al., 2019), these centres have been supported by academic and more specialised infrastructure since their inception. In addition, the BMC has supported clinical training and data collection and analyses from other urban and regional centres (Capon et al., 2023a, 2023b). Consequently, compared with most other headspace sites, there has been a greater emphasis on comprehensive clinical assessment, consistency of application of clinical staging and diagnostic criteria, continuing care and structured short and longer term outcome assessment. The insights gained from this intensive and academically supported work permit comparison between the aggregated national data set and clinically focused and multidimensional outcome data reported by an academic centre.
While these data are distinct from that reported by headspace national, it does not mean that the young people presenting to our services, or those we support academically, are markedly dissimilar to those seen at many other headspace services. In fact, we have consistently reported the extent to which the Sydney-based (BMC) cohort closely resembles those seen at other urban sites on basic demography, symptom severity and functional impairment (Table 1; Capon et al., 2023a, 2023b; Carpenter et al., 2020; Iorfino et al., 2022b). As now derived from the headspace national data (Gao et al., 2024), it is likely that many other headspace services have a similar cohort profile. What is likely to be different about the young people seen at BMC is not their baseline characteristics but rather their experiences of care. Services are arranged (within the headspace centres or through continuing care partnerships with various public and private, and more specialised, services) according to their need, rather than focusing care on single sessions or limiting care to brief psychological interventions only.
Key characteristics of Brain and Mind Centre and headspace youth cohorts.
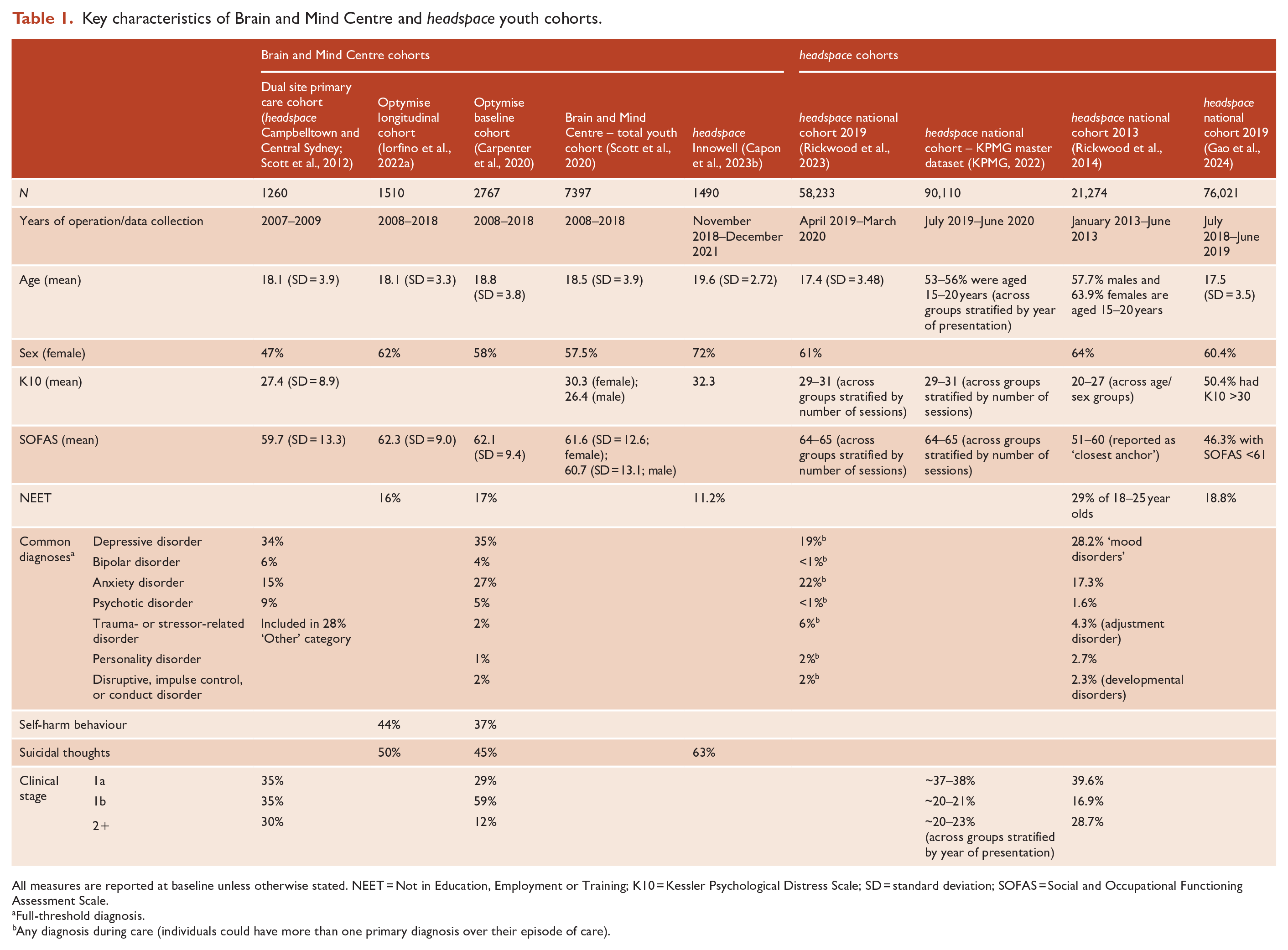
All measures are reported at baseline unless otherwise stated. NEET = Not in Education, Employment or Training; K10 = Kessler Psychological Distress Scale; SD = standard deviation; SOFAS = Social and Occupational Functioning Assessment Scale.
Full-threshold diagnosis.
Any diagnosis during care (individuals could have more than one primary diagnosis over their episode of care).
More recently, we have been able to access data directly from 11 other urban and regional sites. Generally, these non-academic sites are connecting with very similar cohorts, though with the trend towards regional sites having a higher proportion of younger clients and clients with more psychotic-like symptoms and risk of suicidal behaviour (Capon et al., 2023b). Interestingly, those from urban areas were more likely to have used other services previously and had higher rates of alcohol misuse.
Furthermore, it is clear that a large proportion of young people attending our centres do have formal diagnoses of anxiety, depression or other complex disorders, well-established functional impairment, and other neurocognitive impairments and neurodevelopmental difficulties (Crouse et al., 2020), elevated genetic risk for severe mood and psychotic disorders (Crouse et al., 2021) and prior presentations for care and experiences of other interventions (Table 1). Importantly, the data we have collected across various centres indicate that almost 50% of attendees have complex clinical needs (Capon et al., 2023a).
Longitudinal data sets and longer term multidimensional outcomes
Longer term data linkage studies have confirmed that this ‘early intervention’ youth cohort is at risk of premature death from all causes (notably suicide and accidents and injuries), with a five-times increased risk found for males and two-times increased risk for females (McHugh et al., 2023). In addition, over a 10-year follow-up period, the median number of presentations to state-based EDs for mental or physical health crises is three (Iorfino et al., 2023a). Almost a third (31%) had an ED presentation directly associated with mental illness or substance abuse. Furthermore, short-term studies of the brief interventions provided indicate that those with greater functional impairment do not improve to the same extent as those who present with little impairment (Cross et al., 2016).
In the most significant long-term study of those entering care through our headspace services (median follow-up time [days] = 490, range = 101–3580), only a third of those presenting for care had a good functional outcome (Iorfino et al., 2022a). Although those responsible for headspace have asserted that such poor outcomes from our centres cannot be considered representative of the national programme (Rickwood et al., 2022), as detailed in our response to that critique (Iorfino et al., 2022b) and above, we attract a very similar cohort and our results are entirely consistent with the proportion (30%) that headspace national itself has reported with regard to improved short-term functioning.
While there was significant individual variation in illness course in our long-term outcomes, several different trajectories were clear. These included early improvement followed by later deterioration, pre-existing impairment which does not change despite clinical interventions and pre-existing impairment which is then associated with progressive impairment. For two-thirds of this cohort, the brief psychological intervention model does not result in significant change to either illness course or functional outcomes. More recent work evaluating causal effects has demonstrated the importance of functional impairment as a direct and specific target for intervention with potential impacts not only on functioning, but also on suicide ideation, self-harm, suicide attempts and psychosis-like experiences (Iorfino et al., 2023b).
The use of clinical staging has been an important tool for understanding the risks of young people presenting to these services (Hickie et al., 2013). With regard to illness progression, 3% of those presenting as stage 1a as compared with 13% of those presenting as stage 1b (i.e. sub-threshold syndromes) progress to stage 2 (full threshold) of a major mood, psychotic or comorbid disorder (Iorfino et al., 2019). So, these cohorts likely contain a subgroup who are at significant risk of progression to major mental disorders.
The central notions of indicated prevention, or early intervention combined with secondary prevention, are that early access to effective strategies can reduce the transition rate from ‘sub-threshold’ or ‘early clinical stages’ to major mood or psychotic disorders. In our largest long-term cohort study (n = 2901), most full-threshold psychotic or bipolar disorders were already evident at first presentation (prevalence of 4.1% and 3.1%, respectively; Carpenter et al., 2022). Of those who did not have one of these disorders at baseline, there were relatively small numbers of new-onset bipolar (n = 100, 4.3%) or psychotic (n = 51, 2.2%) disorders, with most emerging in the first 2 years after presentation to care. This is despite a high prevalence of anxious and depressive syndromes, as well as moderately high rates of psychotic and mania-like experiences, circadian disturbance, deliberate self-harm, suicide attempts and alcohol, cannabis and stimulant use among this cohort (Carpenter et al., 2022).
In studies from this large youth cohort, we have detailed the extent to which physical illness or risk factors (notably metabolic dysfunction), as well as substance misuse, are not necessarily tied to clinical stage (meaning they often occur early in the course of illness; Capon et al., 2022; McKenna et al., 2024; Shin et al., 2024; Wilson et al., 2023). Further, some factors such as circadian disturbance and functional impairment are not only predictive of illness progression (Iorfino et al., 2019; Scott et al., 2022), but may also be a consequence of that progression (Capon et al., 2022). Altogether, this work illustrates the level of complexity already present among these cohorts.
Diverging narratives
Given the changing epidemiology of adolescent-onset mental disorders, the development of enhanced primary care-based ‘headspace’ services in Australia is of international significance (McGorry et al., 2024). These services respond directly to the historic neglect of indicated prevention, early intervention services and secondary prevention for youth, as well as the demonstrated failure of traditional general medical services to provide affordable or equitable access to quality care (Hickie, 2021).
As large-scale controlled trials of these new service platforms are unlikely, we must learn as much as possible about their effectiveness from systematic and detailed monitoring, as well as from selected but much more detailed evaluations (Hilferty et al., 2016; Muir et al., 2009). The data from the centres operated directly by the BMC, and affiliated networks, provide valuable insights that have not been readily available from the headspace national dataset. Together, more sophisticated analysis of the national dataset (Gao et al., 2024) and these detailed BMC studies provide the complementary evidence required to improve the quality of youth mental health services for young people in Australia and add to the international discourse about the further development of such services.
It is a concern, however, that two diverging narratives have developed over the life of the headspace programme. Various reports now present contrasting interpretations about who attends headspace centres, what their clinical needs are, to what extent are these services alone or in combination with other more specialised service partners genuinely enhancing our national capacity to provide effective indicated prevention, early intervention and secondary prevention services.
The headspace national narrative increasingly has put less emphasis on pathways to comprehensive service delivery, particularly for those with at least moderate clinical and psychosocial complexity. Instead, the emphasis is on single session or brief interventions for those with low levels of complexity, alongside related efforts to enhance other ‘intermediate’ and population-based outcomes. That is, an emphasis on improving mental health and wellbeing, promoting mental health literacy and supporting a better experience of care is now entwined with maximising ‘one-off’ encounters, providing limited clinical assessment, promoting brief psychological (and limited medical) interventions and tracking short-term outcomes. This focus may be a response to increasing demand or the challenges headspace faces in attracting and retaining skilled clinical staff.
This narrative may well be appropriate for young people experiencing largely transient distress, with very low rates of clinical disorders, self-harm or suicidal ideation, physical ill-health, other comorbidities (e.g. abnormal eating behaviour) and little evidence of functional impairment, estimated by headspace national to be 40% of attendees but as low as 25% across the centres surveyed by BMC. Importantly, when key clinical and functional impairment factors are formally assessed, a contrasting picture of much greater need is clear. In the headspace national data these are now estimated to be approximately 60% of attendees, while in the BMC network we estimate this to be at least 49%, with another 27% also needing clinical services (75% in total).
The BMC narrative that emphasises the more significant needs of the majority of those attending headspace services is also supported increasingly by the reporting of data by another independent research group. It too has focused on more detailed and reliable reporting of the clinical, psychosocial and complexity characteristics of those youth presenting for care at other headspace sites (Cotton et al., 2022; Gao et al., 2023). In this data, based on quality-of-life measures, only 26% of youth fall into the low needs group (Cotton et al., 2022).
These more detailed analyses have major implications for the future design of youth mental health services. The BMC model of care places a much clearer focus on highly personalised and skilled assessment on entry to services, followed by measurement-based care. That is, it prioritises detailed clinical and multidimensional assessment to facilitate the delivery of a range of appropriate evidence-based psychological, psychosocial and medical interventions. This service delivery model is not tied to the traditional primary-secondary or specialist care divide, or simple stepped-care (or ‘fail-first’) models, but instead leverages infrastructure that supports an alternative ‘right care, first time’ care model (Hickie et al., 2019; Rosenberg et al., 2020). Such rapid access to appropriately coordinated specialist care is also more likely to deliver significant population-level benefits, in cost-effective ways, as compared with our current stepped-care models (Crosland et al., 2024; Skinner et al., 2023; Vacher et al., 2023).
When established in 2007, headspace also promoted an ‘enhanced primary care’ model, with the expectation that young people would have ready access to skilled mental health staff. The goal of any youth mental health system needs to be that any time a young person seeks care, their needs are appropriately assessed and responded to in a personalised but standardised way, with equity and consistency. That assessment process (in person, or enhanced by new technologies) needs to consider complexity, future risks for illness progression and poor prognosis across a range of clinical, physical health and psychosocial outcomes.
Conclusion: ways forward
As the demand for more personalised and effective care options rises, and the limitations of a very narrow focus on low levels of complexity and indicated prevention rather than genuine early intervention and secondary prevention are recognised, a new range of service care models are urgently required. Much of the BMC-led clinical and population-based work has focused on the promotion of regionally focused service planning and the development of person-centred and organisationally relevant infrastructures to underpin effective triage, service prioritisation and short- and longer term tracking of clinical and functional outcomes (Crosland et al., 2024; Rosenberg et al., 2023). This requires the development of real partnerships with local youth and welfare services, maintaining and fostering clear partnerships with more specialised mental health services, so that a range of clinical and psychosocial needs can be met. Consequently, what we need is a national network of youth services that overtly respond to the unmet needs of young people in the early stages of major disorders, who already have moderate levels of clinical and psychosocial complexity. Providing early, effective, equitable, appropriate, evidence-based and affordable care to Australia’s young people surely ranks among our highest priorities for mental health reform.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: IBH is the Co-Director, Health and Policy at the Brain and Mind Centre (BMC) University of Sydney. The BMC operates an early-intervention youth services at Camperdown under contract to headspace. IBH is the Chief Scientific Advisor to, and a 3.2% equity shareholder in, Innowell Pty Ltd, which supports the transformation of mental health services internationally through the use of innovative technologies. EMS is Principal Research Fellow at the Brain and Mind Centre, The University of Sydney. EMS is Discipline Leader of Adult Mental Health, School of Medicine, University of Notre Dame, and a Consultant Psychiatrist. EMS was the Medical Director, Young Adult Mental Health Unit, St Vincent’s Hospital Darlinghurst until January 2021. EMS has received honoraria for educational seminars related to the clinical management of depressive disorders supported by Servier, Janssen and Eli-Lilly pharmaceuticals. EMS has participated in a national advisory board for the antidepressant compound Pristiq, manufactured by Pfizer. EMS was the National Coordinator of an antidepressant trial sponsored by Servier. All other authors declare no financial or non-financial competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funders played no role in study design, data collection, analysis and interpretation of data, or the writing of this manuscript. IBH is supported by a NHMRC L3 Investigator Grant (GNT2016346). JJC is supported by an NHMRC Emerging Leadership Fellowship (GNT2008197). WC is supported by an Australian Government Research Training Program (RTP) Scholarship. FI was supported by the Bill and Patricia Richie Foundation and an NHMRC EL1 Investigator Grant (GNT2018157).