
Abstract
There has been recent discussion in Australia and New Zealand concerning the utility of Clinical Practice Guidelines (CPGs) and the role of the Royal Australian and New Zealand College of Psychiatrists (RANZCP) in their development. The College Board therefore established a Steering Group (SG) to oversee an exploration of options and produce recommendations about contemporary approaches to the development of high-quality evidence-based clinical practice guidance for psychiatry. This paper outlines the SG’s conclusions and recommendations, as well as the underlying methods and reasoning. In particular, we discuss best practice and recent developments in the synthesis of research evidence. Account has been taken of the opportunities offered by digital technologies, the proliferation of clinical evidence and awareness of the gains to be made by increased inclusion of lived-experience perspectives. It is recommended that the broader concept of best practice resources (BPRs) as now emphasised in so many fields of service is the most appropriate starting point for the College’s role in this area especially as the expertise of the College and its fellows lends itself to the development of a range of BPRs. In conclusion, contemporary guidance needs to be tailored to the requirements of the practitioners seeking it, to articulate the real-world needs and experiences of patients, and to be delivered in a contemporary format that is responsive to rapidly emerging evidence. The experience in Australia and New Zealand may have implications elsewhere for the development of CPGs and BPRs more broadly.
Keywords
Introduction
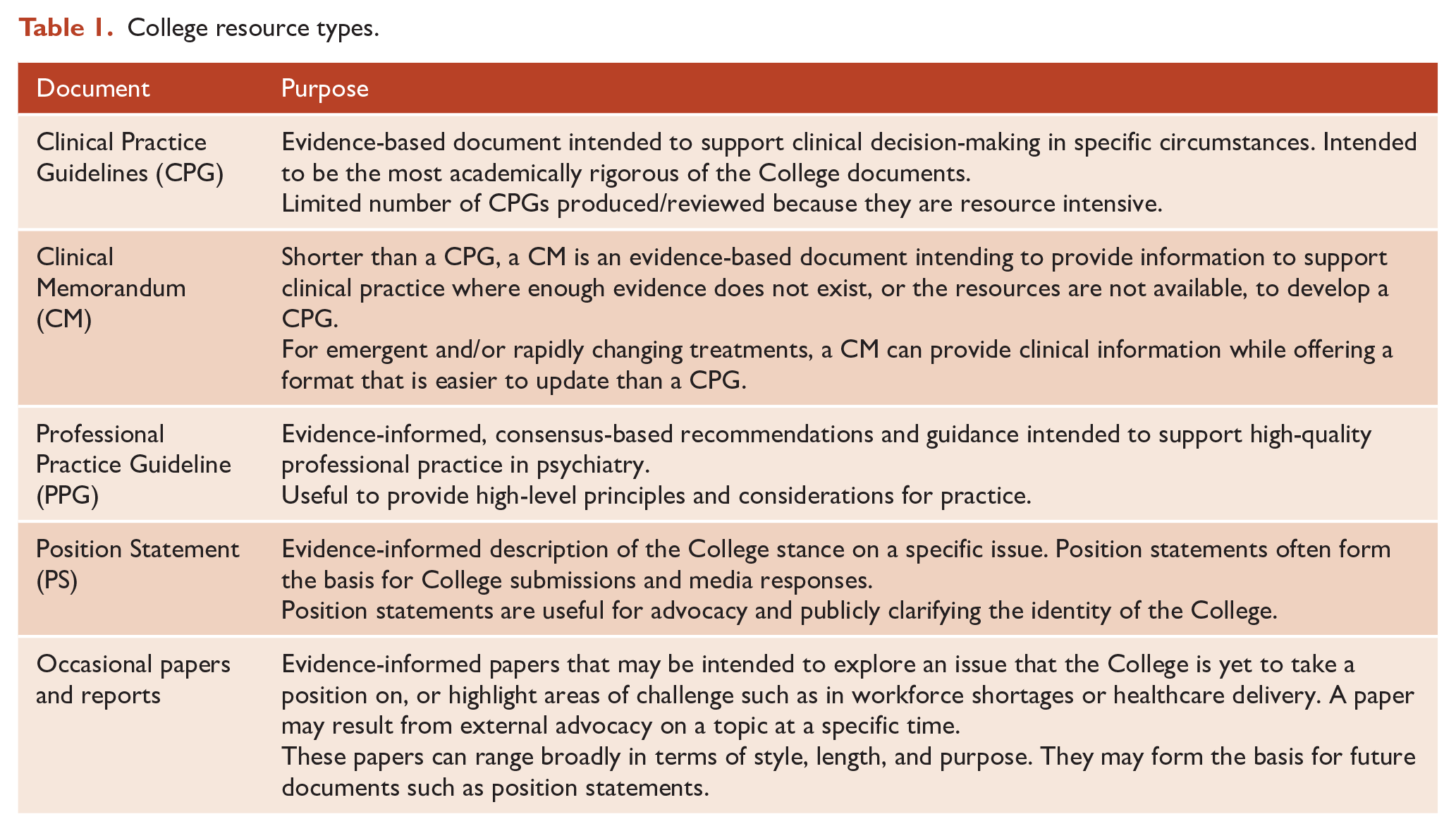
The Royal Australian and New Zealand College of Psychiatrists (RANZCP) has a long history of developing clinical guidelines dating back to the Quality Assurance Programme in 1983, led by Professor Gavin Andrews, which was followed by the Clinical Practice Guideline (CPGs) Project (Boyce et al., 2003). Six CPGs have been developed as part of the Project: anorexia nervosa; bipolar disorder; deliberate self-harm; depression; panic disorder and agoraphobia and schizophrenia (Boyce et al., 2003). CPGs represent one form of best practice resource (BPR) from the College on professional or clinical issues, others being Clinical Memoranda, Professional Practice Guidelines, Position Statements and occasional papers or reports. Table 1 gives comprehensive descriptions of each.
College resource types.
Advantages and challenges
Over the years, the College’s CPGs have been developed and updated according to recommendations from the National Health and Medical Research Council of Australia (NHMRC, 2016). Among others, these include the following:
The guideline is developed by a multidisciplinary group with expertise in clinical content, methodology, literature searches and the review of evidence, as well as lived experience.
Guidelines should be based on systematic reviews of evidence.
There should be transparency about the membership, decision-making and judgements of the group.
Each recommendation should be clearly linked to the supporting evidence, including an assessment of the underlying strength.
CPGs are produced in consultation with relevant College Committees, Working or Steering Groups (SGs). They are reviewed every 3–5 years to ensure currency and either rescinded or reviewed and updated as appropriate. Although the initiation, drafting and approval is time- and resource-intensive for both membership and staff, taking up to 3 years to complete, CPGs can be a valuable resource for psychiatrists, trainees and other health professionals. Advantages have included greater standardisation and consistency in patient care based on the best available evidence, better patient outcomes by promoting effective treatments and their use as educational or continuing professional development tools helping clinicians stay up-to-date with the latest research and treatments (Setkowski et al., 2021). The current suite of RANZCP CPGs are internationally valued as demonstrated by their high citation figures. However, recent discussions concerning global shifts in digital technology, practice and expectations regarding the provision of clinical guidance highlight differences in opinion on their continued utility and the College’s role in their development (Anaf et al., 2023; Malhi et al., 2023).
Currently, there is increasing discussion concerning the purpose of CPGs. Historically they are recommendations derived from research and other sources of information that are collated by experts with a combination of interest, education and experience in the subject matter, the ultimate aim being to guide others in their clinical practice. CPGs have also been used for other purposes, such as by clinical administrators and insurers who use them to monitor, control, direct or judge the execution of clinical best practice or in legal proceedings, such as negligence matters, where they may be used as evidence of peer-accepted practice.
As with all forms of evidence synthesis, there are limitations to CPGs. For instance, guidelines may not account for individual patient variations or reflect the most current research and treatments. Target audiences may be unclear, as CPGs are not necessarily tailored to the needs of practitioners with different levels of experience. For example, while a trainee psychiatrist may find the CPGs very useful for professional development, an experienced psychiatrist may wish to draw on other sources of information.
Another shortcoming is that they largely ignore the preferences and ‘expertise by experience’ of people with lived experience. This is because most CPGs have been developed by clinicians on behalf of those whom they treat rather than in conjunction or in partnership with them (Fonseka et al., 2020). As a result, they do not reflect lived experience and often use complicated medical language that is hard for a lay audience to understand. In the absence of a layperson summary, this adversely affects mental health literacy, impedes individuals’ ability to access and communicate health information and fails to fully inform decision-making (Fonseka et al., 2020).
Furthermore, the implementation of CPGs can be resource-intensive as it requires time, training and/or financial investment and can be influenced by conflicts of interest that potentially compromise their objectivity.
Finally, in a new era when evidence synthesis struggles to keep pace with an explosion in knowledge – especially given digital technologies or new approaches to synthesising evidence – what is the future of CPGs? Examples of the former include smartphone or web-based applications such as Medscape or Learn from Neuroscience Education Institute. New approaches to synthesising evidence include meta-reviews, umbrella reviews and overviews of systematic reviews (SRs) (Aromataris et al., 2015; Belbasis et al., 2022; Ortega et al., 2016). While exact definitions vary, all share common advantages of reproducibility, transparency and the possibility of greater standardisation in applying results to clinical practice.
As a result of these considerations and a commitment to reviewing approaches in light of them, the RANZCP commissioned an independent review of the College’s approach to the future of CPGs in 2022. This was conducted by Health Research Consulting (hereco, 2023), supported by College staff and the Future Development of CPG SG (the Steering Group), of which this paper’s authors were members. The present paper describes the methods and reasoning behind the work and recommendations of the SG.
Considering alternative approaches
Initially, the SG examined the current understanding and usage of evidence in drafting College documents. It noted that the current understanding of evidence, preferably from quantitative sources and clinical studies, discounts or removes consumers’ perspectives and possibly restricts consumer choice and autonomy over their care. The SG also discussed and proposed that, where possible, the College should avoid duplication of high-quality resources by producing its own documentation if there were external resources that could be endorsed or repurposed.
Other considerations included advances in digital technologies, as well as target audience expectations with regard to the format and length in which information is provided. For instance, there has been a shift towards shorter-form, accessible (including digitally accessible), and targeted provision of information given increases in the amount and availability of research evidence. The differential needs of trainees, practitioners and the community in this regard were also important.
The SG also took into consideration the hereco report (the Report) (Health Research Consulting [hereco], 2023). This report was informed by consultations with key RANZCP members and stakeholders, an analysis of existing RANZCP CPGs and an environmental scan of CPG development across Australian and New Zealand Medical Colleges, peak bodies and international psychiatry organisations. The Report identified that the College was an outlier in creating its own CPGs. Most similar organisations did not engage in producing this kind of document unless commissioned and funded by an outside body, typically a government agency. The high level of expertise and intensive resourcing (up to one million dollars) associated with producing CPGs were deterrents, as were the potential risks to the organisation that creates them (hereco, 2023). These risks include reputational risk if a CPG is produced without appropriate rigour, division within the College if the content is contested and the use of significant organisational resources that could otherwise be directed elsewhere. The Report also highlighted that while existing CPGs had many strengths such as the involvement of a multidisciplinary working group, named authors, declarations of interest, SR methods, professional/lay recommendations, accessibility and extensive consultation, there were also limitations. These included the following: limited information on how consensus was achieved between authors; a lack of detail on the parameters of the literature search and included papers; the critical appraisal of included studies or how the included research was linked to the recommendations. The length and narrative style of CPGs were also noted to hinder navigation and potentially implementation, although it should be noted that some CPGs have been issued in abbreviated form for use by non-psychiatrists (Malhi et al., 2018a, 2018b). While the report acknowledged the expertise and effort involved in producing the existing CPGs over the past several years, only two of the five met the demanding contemporary criteria cited by the report of a high-quality, evidence-based CPG. These were the CPGs on anxiety and deliberate self-harm (Andrews et al., 2018; Carter et al., 2016).
During interviews conducted with key stakeholders, the Report found support for the recommendation that the College review its role in developing CPGs (hereco, 2023: 30). The SG subsequently recommended that the College consider alternative options, using the rubric of BPRs (Figure 1). Alternatives might entail the endorsement, adaptation or development of existing high-quality BPRs, such as guidelines from the UK’s National Institute for Health and Care Excellence (NICE), or other peak bodies, following the prioritisation and selection of topics by the College’s Committee for Evidence-Based Practice and other relevant stakeholders. Depending on the nature and scope of the topics, BPRs might include clinical memoranda, professional practice guidelines, position statements and systematic or umbrella reviews. Shorter-form, accessible modes of information communication could also include webinars, podcasts, short videos, fact sheets and emerging modes of knowledge and evidence transmission.
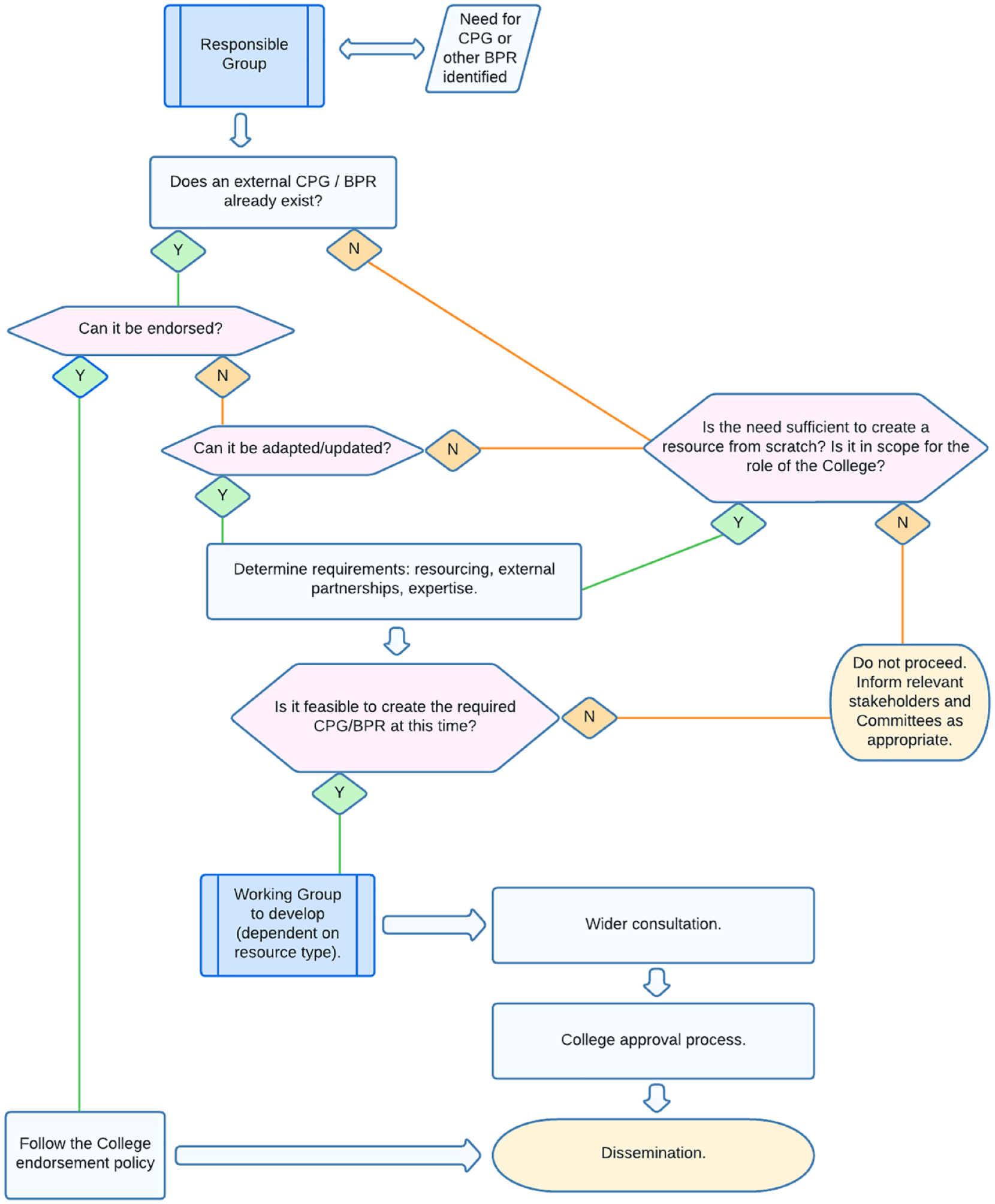
Best practice resources pathway.
In any instances where the College continues to develop CPGs, there should be external funding, wide consultation on priority setting and topic selection, transparency in decision-making and consideration of alternatives to dissemination in a lengthy primary document (as is already the case in mood disorders; Malhi et al., 2018a, 2018b). Wider community involvement is crucial, including the views of people with lived experience, to ensure that BPRs are tailored to the audience’s needs, at both individual and community levels, to maximise effective knowledge translation. Examples include lived-experience input into a protocol for responding to suicidal ideation, as well as guidelines from the NICE (Fonseka et al., 2020; Hawgood et al., 2023).
Next steps
The continued submission of CPGs developed independent of the RANZCP to the College’s journals continues to be of immense value. Our specific experience in Australia and New Zealand – for example, with regards to considerations around rurality and intergenerational trauma – is likely to have implications elsewhere for the development of CPGs and BPRs more broadly.
The SG also noted, in providing its recommendations and endorsing the Report, the importance of tailoring BPRs to the intended audience, a commitment to transparency in methodology and the need to incorporate qualitative and lived-experience perspectives as well as quantitative evidence. Following agreement by the Board, we envision the RANZCP can embark on a journey towards a future approach to advocating for, developing and adapting BPRs that are tailored to the nature and scope of the clinical topic, embrace new approaches to knowledge synthesis and evidence communication and consider lived experience perspectives and experiential knowledge (Salvador-Carulla et al., 2017).
Key future considerations need to include examination of who is seeking guidance, where, in what form and for what reason. These queries will determine the parameters of who delivers what guidance, in what form and based on what evidence. The present era of digital technology provides a unique opportunity for clinical guidance providers to build on existing knowledge while harnessing previously inaccessible modes of synthesis and communication. The SG is pleased to share a vision for how the College can adapt to changes in digital technology, target audience information expectations and thrive as a leader providing clinical guidance to future generations of psychiatrists. The experience in Australia and New Zealand may have implications elsewhere for the development of CPGs and BPRs more broadly.
Footnotes
Acknowledgements
We would like to acknowledge the substantial pro-bono contributions of RANZCP members and collaborators to the development of CPGs over the years, which is greatly appreciated.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All the authors were members of the Future Development of Clinical Practice Guidelines Steering Group, or assisting College staff.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.