
Abstract
Objective:
Women living with mental health conditions have lower cervical cancer screening rates and higher mortality. More evidence is needed to target health system improvement efforts. We describe overall and age-specific cervical cancer screening rates in mental health service users in New South Wales.
Methods:
Cervical cancer screening registers were linked to New South Wales hospital and community mental health service data. Two-year cervical screening rates were calculated for New South Wales mental health service users aged 20–69 years (n = 114,022) and other New South Wales women (n = 2,110,127). Rate ratios were compared for strata of age, socio-economic disadvantage and rural location, and overall rates compared after direct standardisation.
Results:
Only 40.3% of mental health service users participated in screening, compared with 54.3% of other New South Wales women (incidence rate ratio = 0.74, 95% confidence interval = [0.74, 0.75]). Differences in age, social disadvantage or rural location did not explain screening gaps. Screening rates were highest in mental health service users aged <35 years (incidence rate ratios between 0.90 and 0.95), but only 15% of mental health service users aged >65 years participated in screening (incidence rate ratio = 0.27, 95% confidence interval = [0.24, 0.29]).
Conclusion:
Women who use mental health services are less likely to participate in cervical cancer screening. Rates diverged from population rates in service users aged ⩾35 years and were very low for women aged >65 years. Intervention is needed to bridge these gaps. New screening approaches such as self-testing may assist.
Introduction
Cervical cancer screening programmes are an important strategy for reducing preventable cancer deaths. Australia’s free national screening programme has contributed to a halving of cervical cancer mortality over the past three decades (Australian Government Department of Health, 2022). There have been significant recent changes in cervical cancer prevention, screening methods and awareness (James et al., 2017; Nagendiram et al., 2020; Woodhead et al., 2016), including a shift from cytology-based screening every 2 years to the human papilloma virus (HPV) every 5 years (Hall et al., 2019). However, only around 62% of eligible women participating in screening (Australian Institute of Health and Welfare, 2022) and cervical cancer remains an important cause of mortality, with 2 deaths per 100,000 Australian women annually (Australian Institute of Health and Welfare, 2018, 2022). Barriers to cervical screening participation include practical and cost issues as well as the intimate nature and discomfort of screening procedures (Brown et al., 2019).
Australian women with serious mental health conditions are 27% more likely to die from cervical, uterine or ovarian cancer than other women of the same age, despite having similar incidence of these cancers (Kisely et al., 2013). Reduced screening participation is one likely cause of this increased mortality (Kisely et al., 2016; Solmi et al., 2020).
A recent meta-analysis (Solmi et al., 2020) identified 23 studies of cervical screening rates in women with mental illness. In pooled estimates from those studies, mental illness was associated with reduced cervical screening (odds ratio [OR] 0.89, 95% confidence interval [CI] = [0.84, 0.95]), and studies examining schizophrenia or affective psychoses reported the lowest rates. However, screening rates were not significantly reduced in studies which also adjusted for personal or demographic risk factors for reduced screening participation (OR for adjusted studies 0.91, 95% CI = [0.82, 1.01]).
Only two previous studies have examined cervical cancer screening rates in Australian mental health service users. An unadjusted survey of 100 hospital and community mental health service users (Owen et al., 2002), found that 76% self-reported cervical screening in the previous 2 years. A recent national linkage study (Tuesley et al., 2019) used prescription of second-generation antipsychotics or Lithium as a marker of severe mental illness. The study found that after adjusting for state or territory of residence and past general practitioner (GP) visits, women with mental illness were 17% less likely to have had recent cervical screening compared with other Australians. That study did not adjust for socio-economic disadvantage or urban–rural location within states or territories.
More evidence is needed to understand these screening gaps and target improvement efforts. No studies have examined how cervical screening rates vary with age in mental health service users, or the extent to which differences in screening rates may be explained by differences in socio-economic disadvantage or rural location. In this study, we used linked data from the National Cervical Screening Program to estimate screening participation rates in women using specialised mental health services in New South Wales (NSW), Australia. We compared rates for individual strata of age, socio-economic disadvantage and rural location, and estimated overall rate differences using direct standardisation. This study is part of the NSW Health Mental Health Living Longer project (Sara et al., 2019), an ongoing population-wide data linkage which aims to build data to understand and reduce premature mortality in people using NSW public mental health services.
Method
Setting and context
NSW has a current population of approximately 8.1 million people. Australia’s National Cervical Screening Program (Australian Institute of Health Welfare, 2013) offers free screening to people aged 20–69 years. The programme targets all people with a cervix, including women, transgender men, intersex people and non-binary people. During the period covered by this study, screening by Papanicolaou (Pap) test was offered 2 yearly. The NSW Pap Test Register recorded test results and personal details for all NSW screening participants undergoing Pap tests, cervical histology tests or HPV tests from public or private health providers (NSW Cancer Institute, 2015).
Mental health service users in this study were defined by contact with public (state operated) community mental health services or any (public or private) hospital admission for mental health care. Mental health care in NSW is mainly government funded or subsidised. Approximately two-thirds of hospital admissions for mental health care occur in state government funded (public) hospitals. Public community mental health services provide longer-term care for people with severe or enduring mental health conditions as well as emergency and acute community mental health care, and are accessed by approximately 2% of the NSW population each year (Australian Institute of Health and Welfare, 2023). Our study does not include data on Commonwealth-government or privately funded services provided in primary care and office-based specialist settings, which are accessed by approximately 11% of the NSW population each year.
Study design and data sources
We used NSW Pap Test Register data from 1 July 2015 to 30 June 2017 to estimate cervical cancer screening rates for all NSW women aged 20–69 years in that period. Population denominators were corrected for the proportion in each age group estimated to have an intact cervix ( ‘hysterectomy fraction’) (Taylor and Rushworth, 1998), using Australian national reference data (Australian Institute of Health and Welfare, 2021). We excluded residents of other states or countries at the time of screening, and individuals with four or more screening results recorded within the 2-year period because these may have reflected data linkage error.
We linked screening records with NSW Hospital and Community Mental Health data collections to define people who had at least one in-scope mental health contact during the study period or in the 2 years prior. NSW Health data collections for this period record sex and not gender: only records where sex was recorded as female were included. In scope contacts were defined as either (1) admission for mental health care to any NSW public or private hospital, or (2) contact with any NSW government-funded (public) community mental health services.
Analysis
Data assembly and statistical analysis were conducted in SAS v9.4. We defined cervical cancer screening rates per 100,000 for mental health service users and compared these with other NSW residents by calculating adjusted Incidence Rate Ratios (aIRR) and 95% confidence intervals after standardisation for age (in 5-year bands), rurality and socio-economic disadvantage. Disadvantage was estimated from the person’s area of residence, using the Index of Relative Socioeconomic Disadvantage (IRSD) (Australian Bureau of Statistics, 2006). This index is calculated using census-derived variables measuring income, government welfare support, education, home ownership, employment, household structure and English language proficiency. For analysis of disadvantage, regions were divided at the quintiles to create five groups of roughly equal population size. Rurality was defined based on the Accessibility/Remoteness Index of Australia Plus (ARIA) index (Australian Bureau of Statistics, 2018), which divides Australia into five levels of remoteness. ‘Remote’ and ‘Very Remote’ levels were grouped together for analysis because of low population and service-user numbers in ‘Very Remote’ areas.
Ethics and governance
The study was approved by the NSW Population and Health Service Research Ethics Committee (HREC/17/CIPHS/48.CINSW Refs 2017/|HRE1105, 2019/UMB0208). The programme is governed by a Steering Committee with includes peak organisations representing NSW health consumers, mental health service users and carers.
Results
During the study period the NSW population averaged 2,224,149 women aged 20–69 years, of whom 114,022 (5.1%) had at least one in-scope mental health contact; 30% of mental health service users had no diagnosis recorded, 17% had at least one recorded diagnosis of psychosis and a further 10% had received more than 2 years of continuous mental health care. Psychosis diagnoses were more common in older service users: 25% of women aged 55–69 years had a recorded diagnosis of psychosis, compared with 10% of women aged 20–34 years. Table 1 shows the proportion of women who participated in cervical cancer screening during the study period after adjusting for hysterectomy fractions and duplicate tests. Cervical cancer screening rates were lower in mental health service users for all age groups and regions. Only 40.3% of mental health service users had participated in the National Cervical Screening Program in the past 2 years, compared with 54.3% of other NSW women (IRR = 0.74, 95% CI = [0.74, 0.75]) (Table 2). Standardisation for age alone or in combination with socio-economic status or rurality produced only negligible changes in estimated rates or relative risk ratios.
Cohort characteristics and stratum-specific cervical cancer screening rates for NSW mental health service users compared to other NSW residents, 2015–2017.
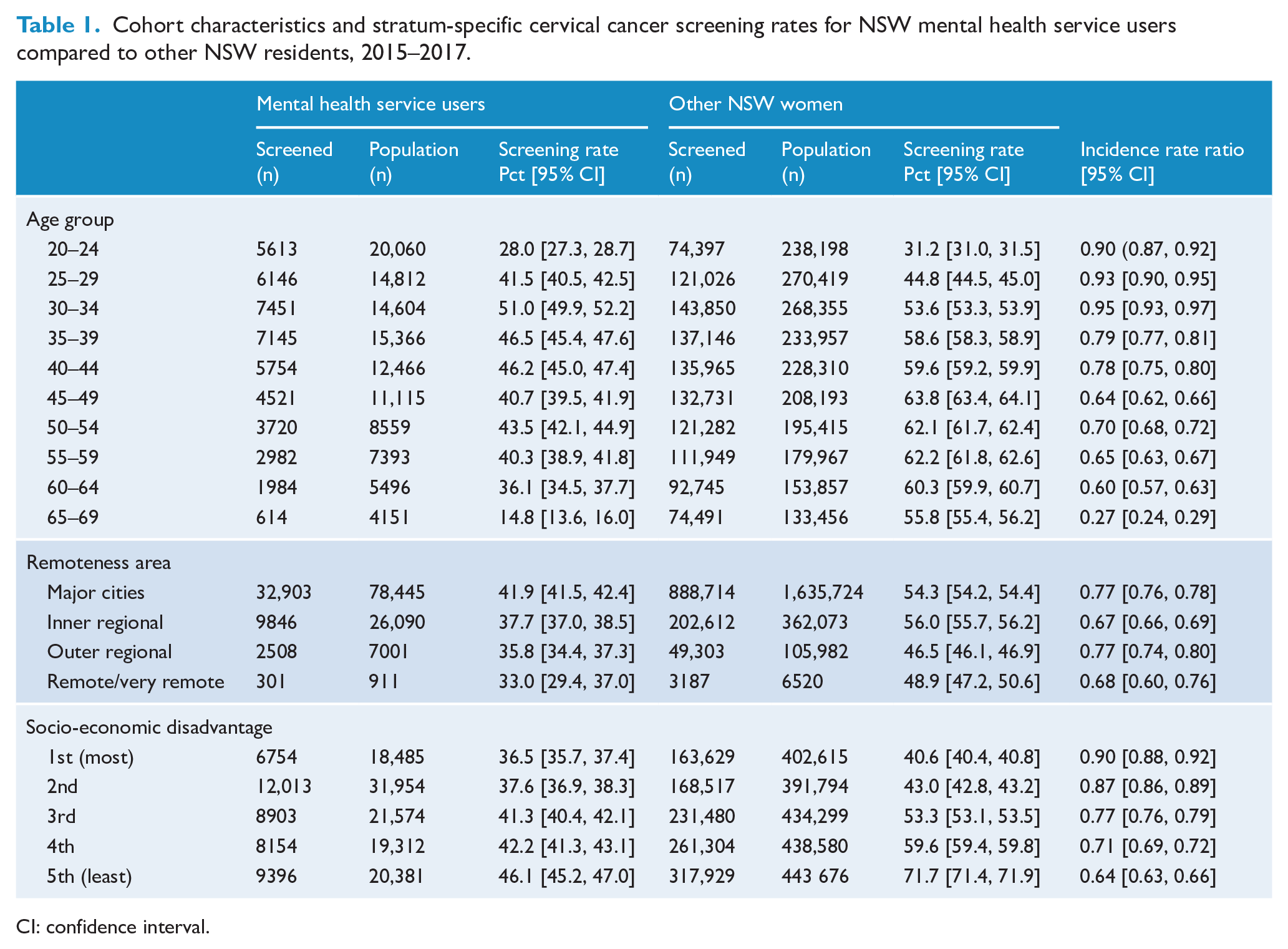
CI: confidence interval.
Cervical cancer screening rates in NSW mental health service users aged 20–69 years compared with other NSW residents, overall and adjusted for (1) age, (2) age and socio-economic status or (3) age and remoteness, using direct standardisation.
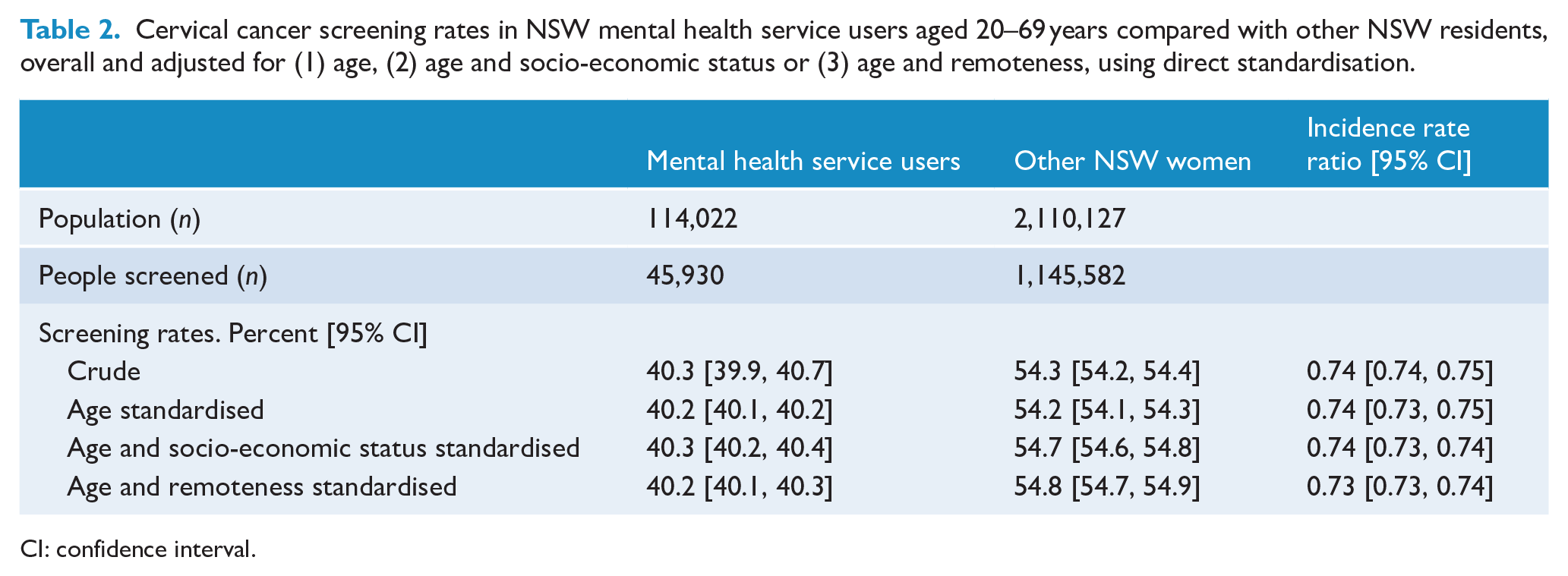
CI: confidence interval.
Screening rates differed substantially with age (Table 1, Figure 1). In women aged ⩽34 years, screening rates in mental health service users were only 5–10% lower than in other NSW women (IRRs ranged from 0.90 to 0.95). However, screening rates diverged steadily from age 35 to 39 (IRR = 0.79, 95% CI = [0.77, 0.81]) to age 60–64 (IRR = 0.60, 95% CI = [0.57, 0.63]). There was a steep drop in screening rates in mental health service users aged ⩾65 years, who had a screening rate of only 15% compared with 56% in other NSW women of the same age (IRR = 0.27, 95% CI = [0.24, 0.29]). There was a strong socio-economic gradient to cervical cancer screening in the overall NSW population, with higher screening rates (72%) in more advantaged areas, and lower rates (41%) in the most disadvantaged areas. However, in mental health service users this gradient was much less evident, with screening rates ranging from 46% in the most advantaged regions to 37% in most disadvantaged regions. As a result, the gap in rates between mental health service users and other NSW women was widest in the most advantaged regions (IRR = 0.64, 95% CI = [0.63, 0.66]), and narrowest in more disadvantaged regions (IRR = 0.90, 95% CI = [0.88, 0.92]).
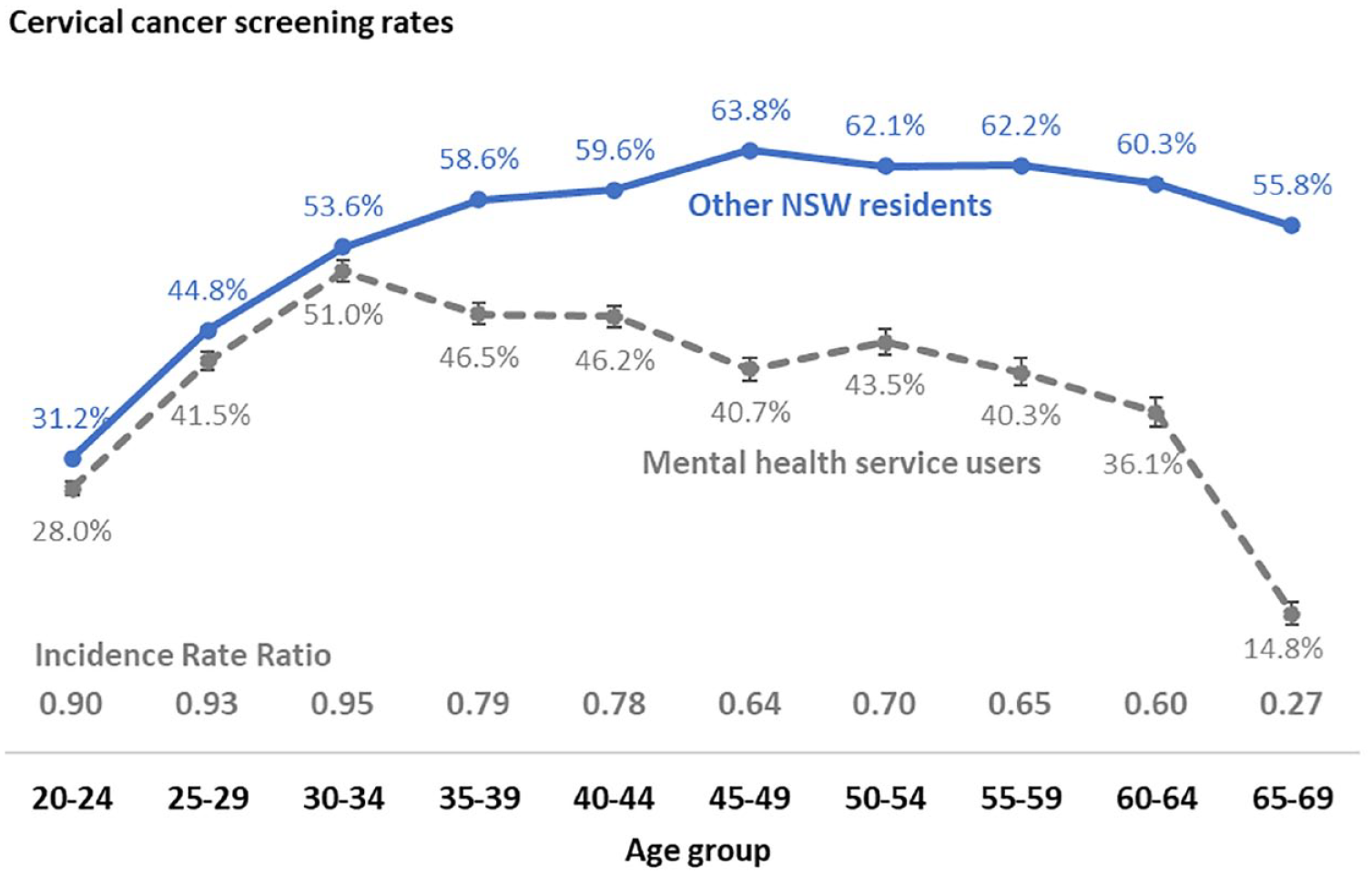
Cervical cancer screening participation rates by age group in NSW mental health service users and other NSW women (95% confidence intervals for other NSW residents are displayed but smaller than graph marker).
For the NSW population, cervical screening rates were slightly higher in metropolitan and inner regional areas, and lowest in the outer regional and remote areas. Mental health service users had lower screening rates in all parts of the state, with the lowest rate (33%) for mental health service users in remote and very remote regions.
Discussion
This study describes cervical cancer screening rates in 114,000 women who had received mental health care in the hospital or public community settings in NSW. Mental health service users were 26% less likely to participate in cervical cancer screening compared with 2.1 million other NSW women of the same age. We estimate that approximately 16,000 additional NSW mental health service users would have been screened in this period if participation rates matched those of the broader population. This screening gap has potentially serious impacts on cancer morbidity and mortality.
Many factors may contribute to low cervical screening participation in mental health service users. Socio-economic disadvantage and rural residence are associated with increased risk of mental health disorders (Isaacs et al., 2018), lower cervical cancer screening rates (Australian Institute of Health and Welfare, 2022) and reduced access to range of preventive and primary health care (Olver et al., 2011). Australians with private health insurance are also more likely to participate in health screening such as pap smears (Rana et al., 2020). However, our findings showed that mental health service users did not have the same socio-economic gradient in screening rates as seen in other NSW residents, so that the largest ‘screening gap’ occurred in more advantaged areas where population rates are highest. We also found that adjusting for rural residence and socio-economic disadvantage had negligible impact on estimates of comparative screening rates. The relative rate of screening in our study was very similar to that found by the only other large Australian linkage study (Tuesley et al., 2019), despite the two studies examining different periods, using different mental health cohort definitions and adjusting for different risk factors.
To our knowledge, this is the first study to describe age-specific differences in cervical cancer screening in mental health service users. We found smaller screening gaps in mental health service users aged <35 years, a steadily widening gap from age 35 to 65 years and a very low screening rate (14.8%) in service users aged ⩾65 years. There are several potential explanations for these findings. First, this may be a cohort effect, reflecting changes in awareness and acceptance of cervical screening in the decade following Australia’s implementation of a national, school-based HPV vaccination programme in 2007 (Patel et al., 2018). Second, this may reflect differences between younger and older women in the type or severity of mental health conditions: among NSW mental health service users in our cohort, a higher proportion of older women had a diagnosis of psychosis. Further study is planned to understand these age-specific patterns.
Low cervical cancer screening rates may reflect broader gaps in primary and preventive health care due to factors including differences in access, cost, perceived stigma and health literacy (Solmi et al., 2020; Thornicroft, 2011). Women living with mental health conditions may also face additional specific barriers to participation in breast and cervical cancer screening (Owen et al., 2002). Women who report a history of childhood sexual trauma are less likely to participate in cervical cancer screening (Olesen et al., 2012), and the intimate nature of cervical cancer screening may pose a substantial barrier to participation. In July 2022, Australia introduced a self-collection test as an option in the National Cervical Cancer Screening Program. This may provide a more acceptable choice for some women (Smith et al., 2016); however, more work is required to understand possible anxieties and barriers which may also limit the uptake of self-collection (Nagendiram et al., 2020).
Limitations
Our study accessed NSW Pap test screening data to 2017. Since that time there have been changes to national data collections; the Pap test has been replaced by HPV testing as the preferred screening method, and recommended screening frequency has reduced to 5-yearly (Australian Institute of Health and Welfare, 2021). The COVID-19 pandemic also caused significant disruptions to primary-care attendance and cancer screening participation in NSW (Sutherland et al., 2020). This study cannot describe the impact of these changes but may provide baseline data to understand their impact as linked screening data become available in future years.
A high rate of missing diagnoses in our public community mental health service records prevented detailed subgroup analysis of specific mental health conditions such as psychosis. This is a common limitation of studies using linked administrative data in clinical research (Bohensky et al., 2010), and there is little data comparing the diagnostic profile of people accessing Australian private and public mental health services. More than one-quarter of our cohort met an operational definition of severe or persistent mental illness (having a diagnosis of psychosis or more than 2 years of mental health care); however, in other studies of our cohort (Lambeth et al., 2023; Sara et al., 2023), public mental health service users without severe or persistent illness also had very substantial gaps in screening or outcomes when compared with the broader NSW population. This may reflect that, regardless of diagnosis, Australian public mental health services primarily see people with severe conditions. Our findings may not generalise to the broader population of Australian women who receive mental health care only in primary care or private outpatient settings.
The current study did not aim to identify subgroups of service users at particularly high risk due to low screening rates. Further work is planned to look at predictors of screening participation in all mental health service users, and to identify combinations of personal, clinical, service and regional factors associated with low screening rates.
Finally, our measures of socio-economic disadvantage were estimated from each person’s local region of residence rather than on individual circumstances and so may underestimate contributions of disadvantage to screening gaps. We do not have reliable data on differences in cultural background, which may also contribute to screening differences.
Conclusion
Early detection through screening is an essential step in reducing morbidity and mortality from cervical cancer. Recent developments in understanding and prevention have the potential to further reduce cervical cancer mortality. Our results highlight the inequalities that mental health service users face in cancer prevention. Older mental health service users may be particularly at risk. The causes of these gaps are likely to be complex and involve shared risk factors, personal vulnerabilities, education and awareness, and system factors in primary care and mental health services. Ongoing study is needed to understand whether mental health service users are benefitting from recent changes in screening, to identify groups of mental health service users at greatest risk and to target health system improvement efforts.
Footnotes
Acknowledgements
This work was completed while K.B. was employed as a trainee on the NSW Biostatistics Training Program, NSW Ministry of Health, on placement with the System Information and Analytics Branch, NSW Ministry of Health. The authors thank Dr Richard Walton, Cancer Institute NSW, for advice on the draft manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the NSW Population and Health Service Research Ethics Committee (HREC/17/CIPHS/48.CINSW Refs 2017/|HRE1105, 2019/UMB0208). The programme is governed by a Steering Committee with representation from peak organisations representing NSW health consumers, mental health service users and mental health carers, and by an Aboriginal Sovereign Steering Committee.