
Abstract

Introduction
Surveillance is a crucial part of suicide prevention, for identifying suicide trends, risk groups, suicide clusters (World Health Organization (WHO), 2014) and frequently used locations for suicide. Suicide sites are usually public, natural or man-made objects known for their use for suicidal behaviour (e.g. bridges or cliffs) (Ross et al., 2020). Some suicide prevention activities to prevent jumping at common sites are more effective than others. For example, a 2020 systematic review found that physical barriers reduced jumping suicides by 93% compared to a 46% reduction for jumping means restriction interventions delivered in combination with other interventions (Okolie et al., 2020). Furthermore, a recent economic analysis of installing barriers at bridge sites in Australia found that barriers installed at multiple bridge sites are cost-saving and cost-effective in the short term (5 years) and long term (10 years) (Bandara et al., 2022).
The Story Bridge is a heritage-listed 74-m-high bridge in Brisbane City across the Brisbane River. Suicides from the Story Bridge have received attention over many years and preventive actions have been recommended (e.g. Law et al., 2014). After the media attention on Story Bridge murder-suicides in 2011 and 2012, the interim Queensland Suicide Register (iQSR), a real-time surveillance system, showed that suicides at the site increased from 7 in 5 years (2006–2010) to 16 in 2012 alone. Informed by the Australian Institute for Suicide Research and Prevention, in consultation with Queensland Health and Brisbane City Council, the Story Bridge Suicide Prevention Reference Group was established and different preventive actions were adopted, including installing Lifeline phones and surveillance cameras in 2012 and barriers at the Story Bridge by December 2015. This analysis examines the impact of these activities on suicides from the Story Bridge and the potential substitution effect by comparing changes in nearby locations.
Methods
We used data from the Queensland Suicide Register (QSR) from 2001 to 2018 and the interim QSR for 2019 to 2021. The QSR records all suicides in Queensland since 1990 including information from police reports to coroners, post-mortem autopsy reports, toxicology reports and coroners’ findings.
The iQSR, established in 2011, is part of the QSR, but information comes solely from police reports of suspected suicides. These reports inform coroners of the circumstances of the death and characteristics of decedents, to help coroners determine the cause of death.
iQSR staff use a decision tree (Leske et al., 2022: 44) to classify all deaths received as confirmed, probable or possible suicides. This study only includes confirmed and probable suicides. Possible suicides might be due to accident, illness or homicide. Further details about the QSR and iQSR procedures can be found elsewhere (Leske et al., 2022). Ethical approval for the QSR and iQSR comes from the Department of Justice and Community Safety Human Research Ethics Committee (HREC; CF/18/12771) in Victoria and the Griffith University HREC (CSR/02/10/HREC).
We examined suicide numbers from the Story Bridge, jumping from other bridges and cliffs, and jumping from other man-made constructions (e.g. residential buildings, carparks) in Inner Brisbane City (Statistical Area Level 4; SA4), and all suicides in suburbs neighbouring the Story Bridge from 2001 to 2021. This time period enabled us to divide suicides into 3-year blocks (to avoid small numbers) including four blocks before any interventions, one block (2013–2015) between two interventions (installing Lifeline phones in 2012 and barriers in 2015) and two blocks after (one using QSR and the last using iQSR data). We used Joinpoint regression analysis to identify changes in the trends of suicide numbers from 2001 to 2021. Joinpoint regression enabled the identification of the best-fitting points where a statistically significant change in a trend occurred, without the need to pre-specify when it would occur. We analysed data with Joinpoint Regression Program 4.9.1.0 (National Cancer Institute, 2022) and present the annual percentage change (APC) in suicides with their 95% confidence intervals (95% CIs).
Results
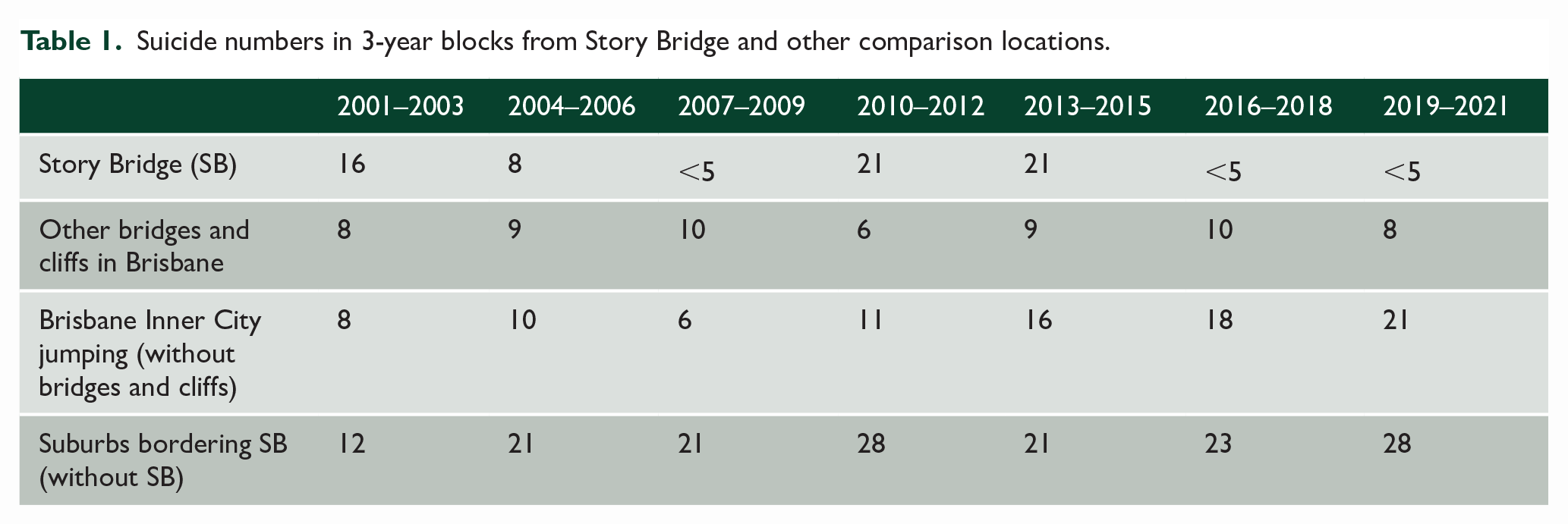
There were 72 suicides from the Story Bridge from 2001 to 2021; at autopsy, most suicides were death caused by jumping (87.5%), followed mainly by drowning after jumping (9.7%). Table 1 presents suicides from Story Bridge and other comparison locations in 3-year blocks. We observed declines in the first 3-year blocks until 2007 to 2009 (n < 5), followed by an increase to 21 suicides from 2010 to 2012. After phone booth installation in 2012, suicides in the 3-year block afterwards remained unchanged from 2013 to 2015 (n = 21); however, suicides dropped below 5 in the following 3-year blocks after barrier installation in December 2015. Joinpoint regression analyses identified two joinpoints in the Story Bridge suicide trend (due to some small annual numbers, Figure 1 only shows estimates). Story Bridge suicides dropped significantly (p = 0.02) from 2001 to 2009 (APC = −26.7%, 95% CI = [−43.4%, −5.1%]), followed by a rapid increase until 2012; since then, suicide numbers decreased significantly, declining to close to 0 (APC = −31.6%, 95% CI = [−44.9%, −15.1%], p = 0.002).
Suicide numbers in 3-year blocks from Story Bridge and other comparison locations.
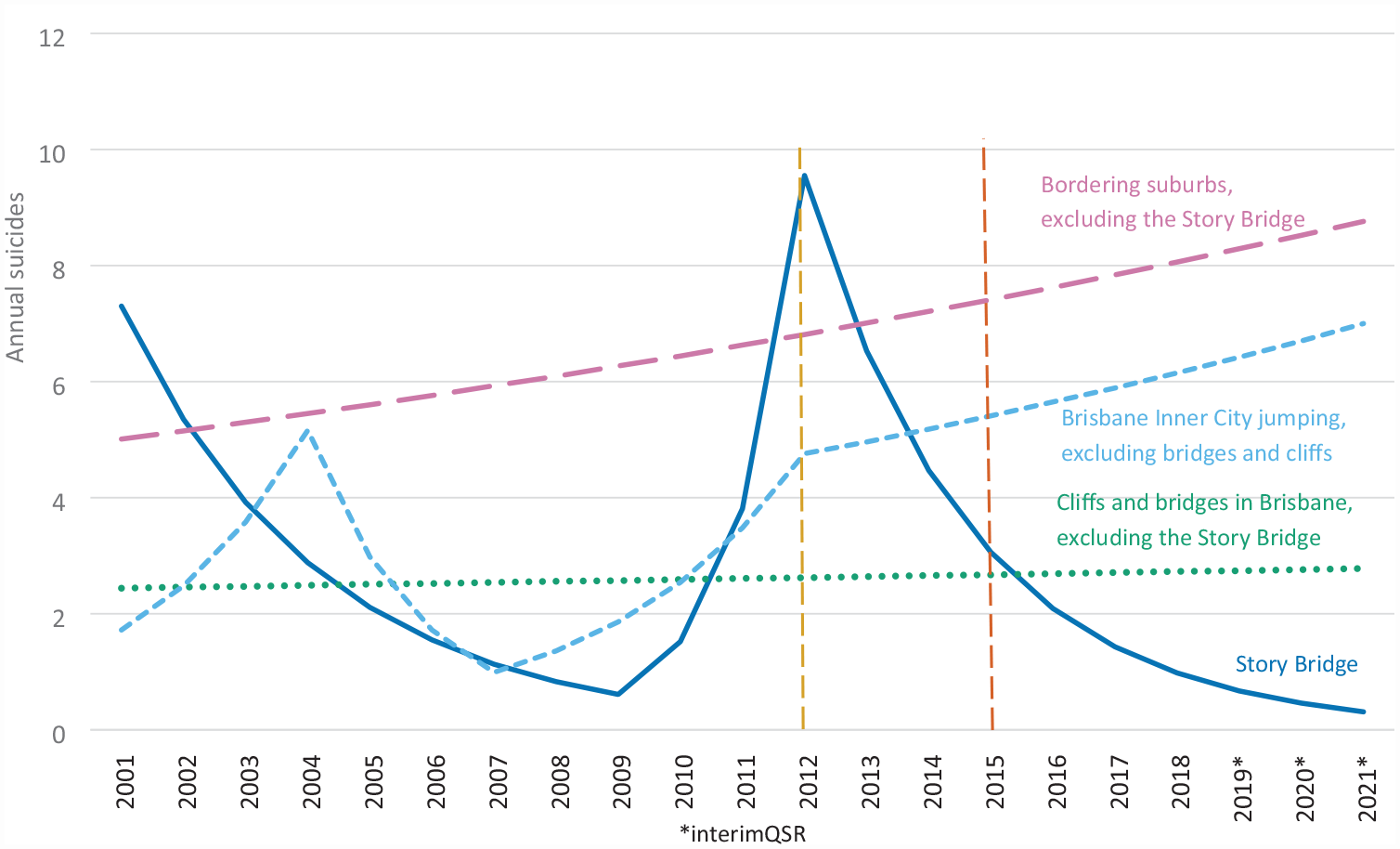
Joinpoint regression modelled suicide trends from the Story Bridge and compared locations.
Analysing suicide numbers from other cliffs and bridges in Brisbane did not identify any joinpoints and there were no changes in the trend during the observation period (APC = 0.6%, 95% CI = [−3.0%, 4.4%]; Figure 1). Similarly, there were no joinpoints in suicide numbers in Brisbane suburbs surrounding Story Bridge; however, the trend was somewhat increasing (APC = 2.8%, 95% CI = [−0.1%, 5.9%]). Jumping suicides from other man-made constructions in Brisbane Inner City SA4 showed more fluctuations with three joinpoints; nevertheless, all trends were not significant (Figure 1). Although the suicide trend increased rapidly from 2007 to 2012 (APC = 36.8%, 95% CI = [−0.2%, 87.5%]), it slowed from 2012 onwards (APC = 4.4%, 95% CI = [4.0%, 13.5%]).
Discussion
This analysis aimed to identify the impact of suicide prevention activities on the Story Bridge in Brisbane. When compared in 3-year blocks, installing Lifeline phones, signs and surveillance cameras in 2012 did not seem to reduce suicides compared to the 3-year blocks before (2010–2012) and after (2013–2015). However, a more fine-grained analysis using data from individual years in the joinpoint regression analysis identified 2012 as the start of the decline in Story Bridge suicides. There was a reduction in suicides after barrier installation, completed in December 2015. Our result adds to the evidence that restricting access to means is effective in reducing suicides from common jumping sites, such as bridges, and reinforces that other interventions are less effective (Okolie et al., 2020; Pirkis et al., 2015). Nevertheless, it is also important to consider the impact of media, which may reduce the potential impact of less restrictive activities (Ross et al., 2020).
Yet, a substitution effect is possible. Although there was no increase in suicides in other bridges and cliffs in Brisbane, there were some ongoing increases observed in surrounding suburbs and jumping from other man-made constructions in the Inner City SA4 of Brisbane.
Some limitations should be considered. Although the QSR and iQSR are comprehensive suicide surveillance systems, the last 3-year block (2019–2021) comes from the iQSR which is based on police reports only and coronial findings have not been scrutinised yet.
In conclusion, our study highlights how real-time suicide mortality surveillance can inform effective means restriction interventions that ultimately reduce suicides.
Footnotes
Acknowledgements
We thank the Coroners Court of Queensland for real-time access to police reports and the Department of Justice and Community Safety for proving access to the National Coronial Information System (NCIS).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The Queensland Suicide Register is funded by the Queensland Mental Health Commission.