
Abstract
Objective:
Engagement with secondary mental health services after an emergency department presentation with suicidal behaviours may be an important strategy for reducing the risk of repeat attempts. Our aim was to examine secondary mental health service contact following a presentation to emergency department with suicidal behaviours.
Methods:
A systematic review of papers published between 2000 and 2020 was undertaken. This identified 56 papers relating to 47 primary studies. Data were extracted and summarised separately by age group: (1) young people, (2) older adults and (3) adults and studies with participants of ‘all ages’.
Results:
Studies in young people (n = 13) showed, on average, 44.8% were referred and 33.7% had contact with secondary mental health services within 4 weeks of emergency department discharge. In comparison, in adult/all ages studies (n = 34), on average, 27.1% were referred to and 26.2% had mental health service contact within 4 weeks. Only three studies presented data on contact with mental health services for older adults, and proportions ranged from 49.0% to 86.0%.
Conclusion:
This review highlights poor utilisation of secondary mental health service following emergency department presentation for suicidal behaviours, and further research is needed to identify the reasons for this. Crucially, this information could assist in the allocation of resources to facilitate the timely implementation of suicide prevention services.
Keywords
Introduction
Each year in Australia, over 3000 people die by suicide, and it is the leading cause of death for people aged 15–44 years (Australian Bureau of Statistic [ABS], 2021). Despite several decades of national suicide prevention initiatives, between 2012 and 2021, the suicide rate increased from 5.6 to 6.1 deaths per 100,000 for women and from 17.0 to 18.2 deaths per 100,000 for men. However, since 2019, the data show a downwards trend in rates for men from a high of 20.1 deaths per 100,000 (ABS, 2021). A recent systematic review found that 44% of people attempting suicide had been in contact with primary care health services and 21% with mental health services (Stene-Larsen and Reneflot, 2019) in the 1 month before the attempt. Although not everyone who has suicidal thoughts or who makes a suicide attempt will seek medical help (Jollant et al., 2022; Madge et al., 2008), the number of people presenting to a hospital emergency department (ED) following a suicide attempt has been increasing (Stapelberg et al., 2020; Ting et al., 2012), and in 2020–2021, there were almost 30,000 hospitalisations in Australia for intentional self-harm (Australian Institute of Health and Welfare, 2023). Evidence shows that the risk of repeated suicide attempts and death in the 12 months after ED presentation is substantially increased (Geulayov et al., 2019; Goldman-Mellor et al., 2019; Kapur et al., 2006; Olfson et al., 2021). Findings suggest that the majority of people who make a repeat suicide attempt will do so within the first 6 months; however, a small proportion makes a second attempt within the first few weeks (Esmaeili et al., 2022; Fedyszyn et al., 2016; Irigoyen et al., 2019; Kapur et al., 2006; Suárez-Pinilla et al., 2020).
National and international clinical guidelines (Alderdice et al., 2010; Carter et al., 2016; National Institute for Clinical Excellence, 2004) recommend that people presenting to hospital with suicidal behaviour should receive a psychosocial assessment by a trained health professional and be offered or have appropriate mental health aftercare arranged. Early access to and engagement with mental health services after an ED presentation with suicidal behaviours may be an important strategy for reducing the risk of repeat attempts and suicide mortality (Inagaki et al., 2015; Turecki and Brent, 2016). We undertook a comprehensive systematic review of the literature to determine whether people who present to an ED with suicidal behaviour are receiving secondary mental health aftercare services following ED discharge. As not everyone will accept the offer of mental health aftercare (Lin et al., 2014; Miller et al., 2020), we also examined referral to secondary mental health treatment services and admission from ED to a mental health bed (referred to in this paper as a mental health admission).
Methods
The study protocol is registered in PROSPERO, the international prospective register of systematic reviews of the University of York (www.crd.york.ac.uk/prospero/) and is accessible under ID no. CRD42022320512.
Eligibility criteria
Published studies were considered eligible if participants had presented at an ED expressing suicidal ideation or following an act of intentional self-injury irrespective of the intent and whether they were referred to or had contact with secondary mental health services. Only papers in English and those published from 2000 to December 2020 were included. The authors decided to restrict the review to a 20-year date range with the upper date (2020) chosen to limit the possible impact of COVID-19 on ED contact and aftercare provisions, given that access to ED care has been reported to be impacted by the pandemic (Dragovic et al., 2020). Randomised control trials (RCT) were excluded as interventions implemented were not ‘usual care’ such as active contact and follow-up interventions after ED discharge.
Study selection
Potentially eligible records were identified by searching electronic databases (PubMed, PsycINFO, MEDLINE, CINAHL Plus and Embase) for search terms in the title, abstract or text (see Supplemental Table 1 for search terms). After duplicate records had been removed, the titles and abstracts of identified records were screened to determine initial eligibility. The full text of eligible papers was then assessed in a second screening process. When papers were identified as having overlapping data, all papers were retained but were considered to be one study. The reference lists of all papers retained after the second screening were reviewed for missed eligible studies. Both stages of screening were conducted by two independent reviewers, and any differences were resolved through discussion (A.W. and G.M.V.).
Data management
Data extraction was conducted separately by two researchers (A.W. and Y.R.F.) and recorded on a spreadsheet. Data and information extracted included source of data, period of observation, sample size and the proportion of participants who, on ED discharge, had a secondary mental health service contact, a mental health service referral or a mental health admission. Proportions were manually calculated if not reported. We summarised and presented the data separately by three age groups: (1) children/young people aged 24 years and under (referred to as young people), (2) older adults 55 years and over and (3) adults 18 years and over and studies with participants of ‘all ages’.
Included studies
The database search identified a total of 926 records after duplicates had been removed (see Figure 1). After screening the titles and abstracts of these records and reviewing the reference lists of the relevant papers, a total of 142 papers were retained for full-text screening. Of these, 3 papers were not able to be retrieved and 83 papers were excluded: n = 10 study participants did not meet inclusion criteria; n = 11 had an ineligible study design (e.g. RCT); n = 14 did not provide a breakdown of data for participants with suicidal behaviours; n = 44 did not report outcome data relevant or useable for this review and n = 4 reported duplicate data.
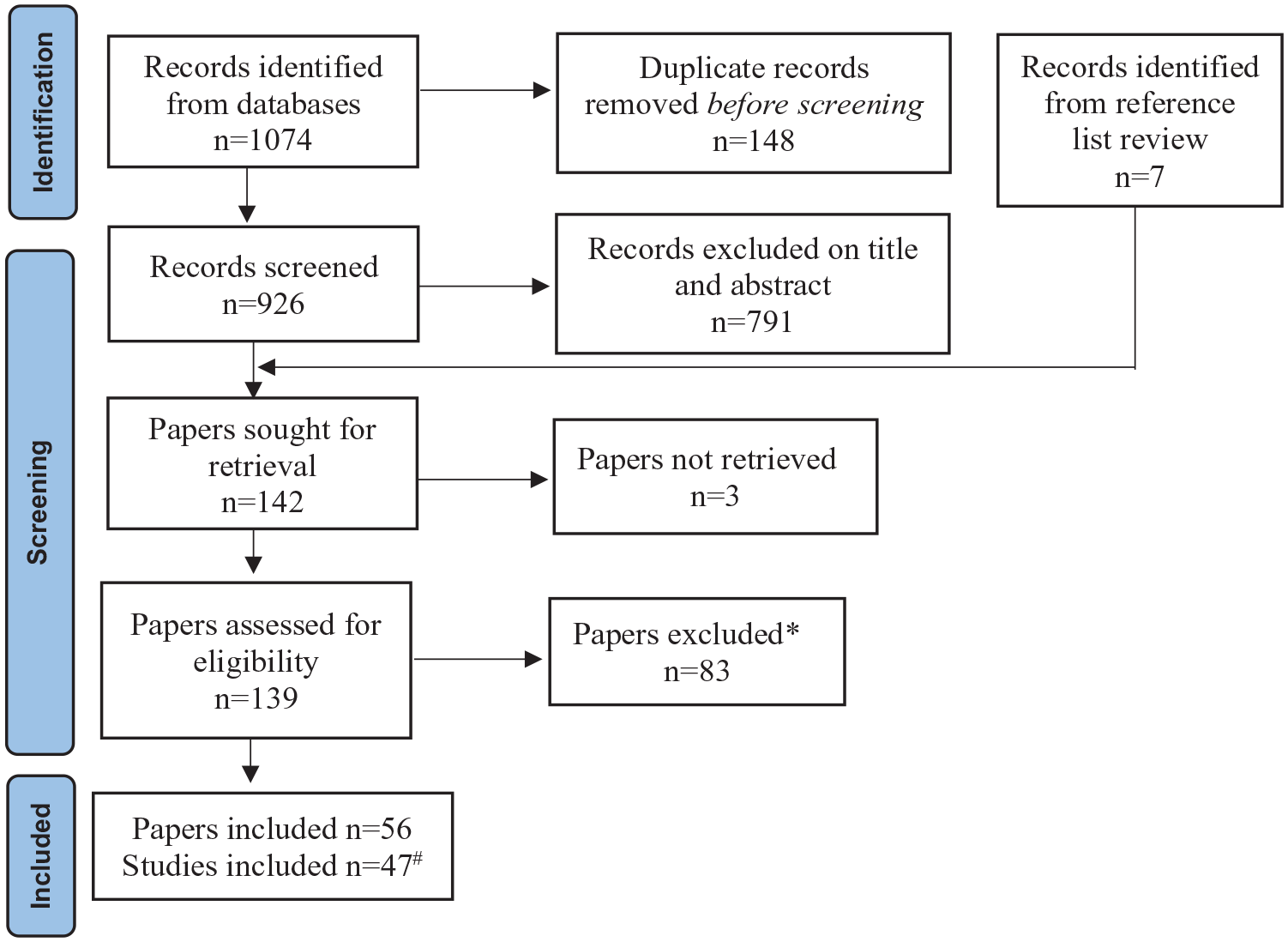
Flow chart of study identification and selection.
Results
A total of 56 papers relating to 47 primary studies presented data on mental health service contact, referral or admission following an ED presentation with suicidal behaviours and were included in this review (Table 1). There were 32 studies (68.1%) which had an observation period prior to 2010, 13 studies (27.7%) with the observation period in 2010 or after and two studies (4.3%) which did not report the dates of their observation period.
Characteristics of the 47 included primary studies.
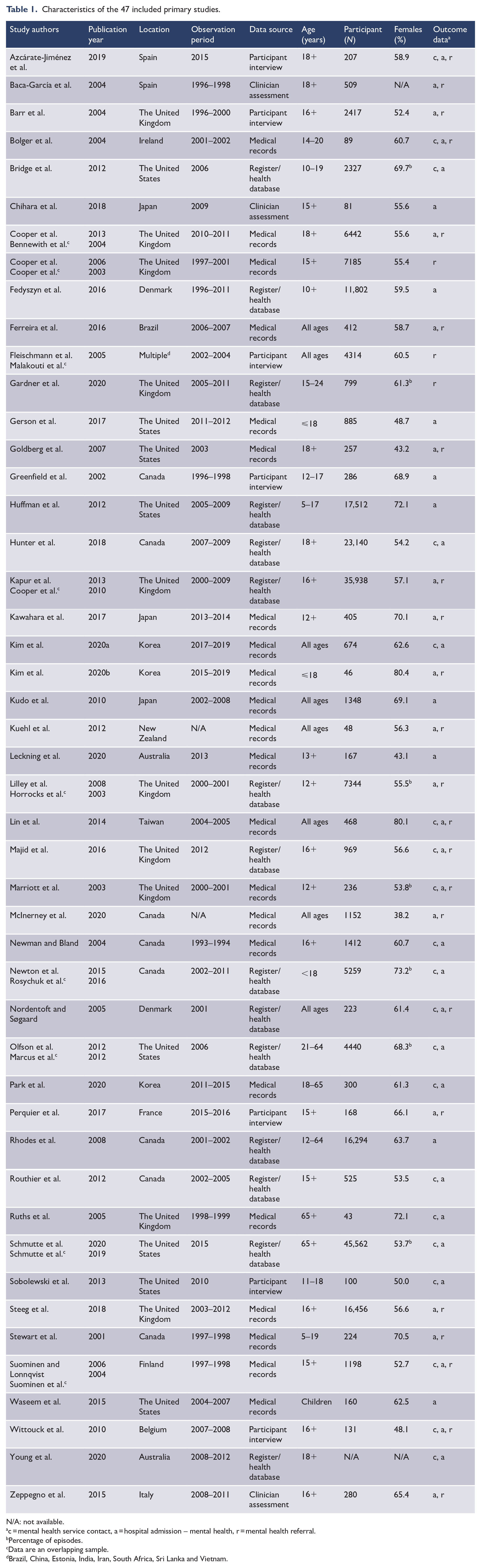
N/A: not available.
c = mental health service contact, a = hospital admission – mental health, r = mental health referral.
Percentage of episodes.
Data are an overlapping sample.
Brazil, China, Estonia, India, Iran, South Africa, Sri Lanka and Vietnam.
Characteristics of included studies and participants
The included studies were undertaken in 24 countries, of which 37% were European, 30% North American, 20% Asian and 13% from other countries. Two main sources of data were used in the included studies: medical records (46.8%) and register or linked administrative health databases (31.9%); a further 14.9% undertook participant interviews and 6.4% conducted clinical assessments. Most (72.3%) studies reported outcomes for unique individuals, although 25.5% reported on the outcome for each episode of ED contact. Consequently, in those studies, an individual could contribute to more than one ED contact. Almost all (91.5%) studies selected their cohort from all people presenting to ED with suicidal ideation or any suicidal behaviours, irrespective of the intent. One study restricted inclusion to people with schizophrenia or depression who were hospitalised after ED presentation (Routhier et al., 2012) and a second followed up adults released from prison (Young et al., 2020). In addition, two studies limited inclusion to people who presented to ED after a self-poisoning attempt (Rhodes et al., 2008) or after self-wrist cutting (Park et al., 2020).
The number of study participants ranged from 43 to 45,562, with an overall mean of 4788 (median = 600). On average, females made up 58.4% of all participants (range = 38.2–80.4%). Of the 47 primary studies included in the review, 34 (72.3%) studies were conducted on adult (n = 8) or all age (n = 25) participants, 11 (23.4%) studies restricted inclusion to children or young people up to the age of 24 years and two (4.3%) studies only included people aged 65 years and over. However, a total of five studies (10.6%) reported data separately for older participants aged 55 years and over, and 13 studies reported data separately for participants aged 24 years and under.
Age-specific outcomes
Children and young people
A total of 13 (27.7%) studies provided data for young people ranging in age from 2 to 24 years (Table 2). The mean age of participants in these studies was 15.3 years (standard deviation [SD] = 2.2). Seven papers reported on contact with mental health services between 7 days and 12 months after an ED presentation. The four papers which reported on mental health service contact within 4 weeks showed that one-third (33.7%) of young people had contact with mental health services (range = 14.3–47.0%). Twelve studies reported on the proportion of young people with a mental health admission from ED, and six studies reported on referral to mental health services. On average, 43.0% were admitted (range = 13.9–54.4%), and 44.8% were referred to mental health services (range = 25.9–75.4%).
Studies reporting contact with mental health services for children and young people 24 years and under.
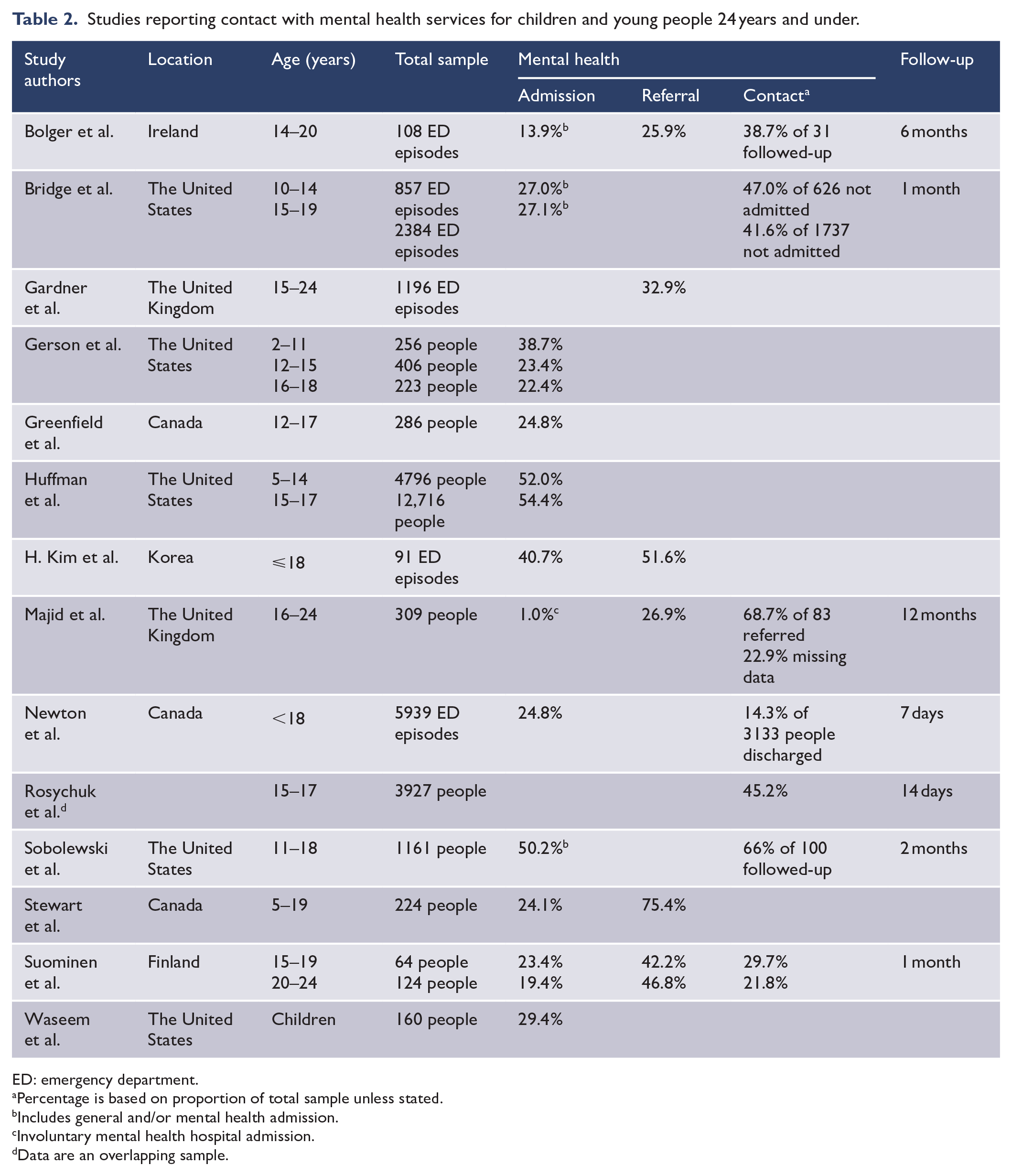
ED: emergency department.
Percentage is based on proportion of total sample unless stated.
Includes general and/or mental health admission.
Involuntary mental health hospital admission.
Data are an overlapping sample.
Older adults
Of the five (10.6%) studies which presented outcome data for older adults, three studies were conducted in the United Kingdom (Table 3). Four of the five studies had sample sizes of less than 150 people, while the one US study had over 45,000 people with more than 50,000 episodes of ED care. Contact with mental health services following an ED presentation with suicidal behaviour was reported in three papers and rates ranged from 49.0% to 86.0%. Four papers reported on the proportion of older people who were admitted to a mental health bed from ED. In the three UK studies, the average proportion admitted was 24.6% (range = 14.0–28.6%), and in the US study, 62.8% were admitted. Three papers presented data on referral to mental health services, and the proportions referred ranged from 28.6% to 66.0%.
Studies reporting contact with mental health services for older adults 55 years and over.
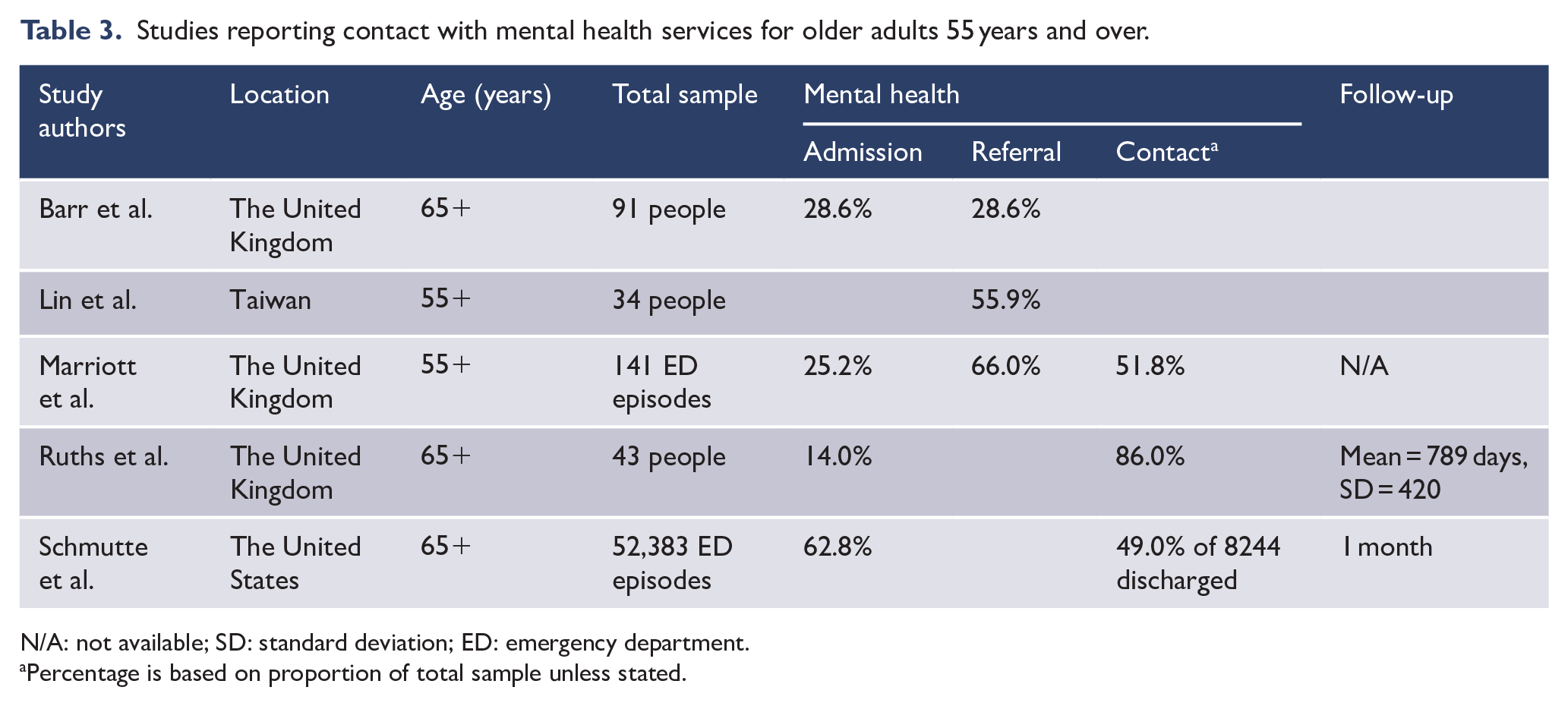
N/A: not available; SD: standard deviation; ED: emergency department.
Percentage is based on proportion of total sample unless stated.
Adult/all ages
Mental health service contact
Fourteen (30.0%) studies reported on contact with mental health services after presenting to ED with suicidal behaviours (Table 4). The types of secondary mental health services and health professionals which people had contact with included psychiatrists, psychologists, psychological counselling, mental health outpatients, group programmes, suicide prevention centre and community mental health services. Half (n = 7) the studies provided data on mental health service contact within 30 days following ED contact, and of these, on average, 26.2% (range = 20.7–61.1%) had a mental health service contact within this period. Two studies had a 3-month follow-up (see Table 4), with both showing that half the participants had a mental health service contact, and two studies had a 6- to 12-month follow-up. The study by Azcárate-Jiménez et al. (2019) found 78.7% had a mental health contact at 6 months and Majid et al. (2016) reported that 67% of those referred were seen by mental health services within 12 months. Three studies provided information on secondary mental health service contact, but not on the follow-up time period. We compared secondary mental health service contact following an ED presentation for those studies with an observation period prior to 2010 (n = 9) with those from 2010 and after (n = 5) and found that the average proportion with a mental health service contact increased from 26.8% (range = 20.7–61.1%) to 38.0% (range = 13.0–78.7%).
Studies reporting contact with mental health services for adults and people of all ages by length of follow-up time.
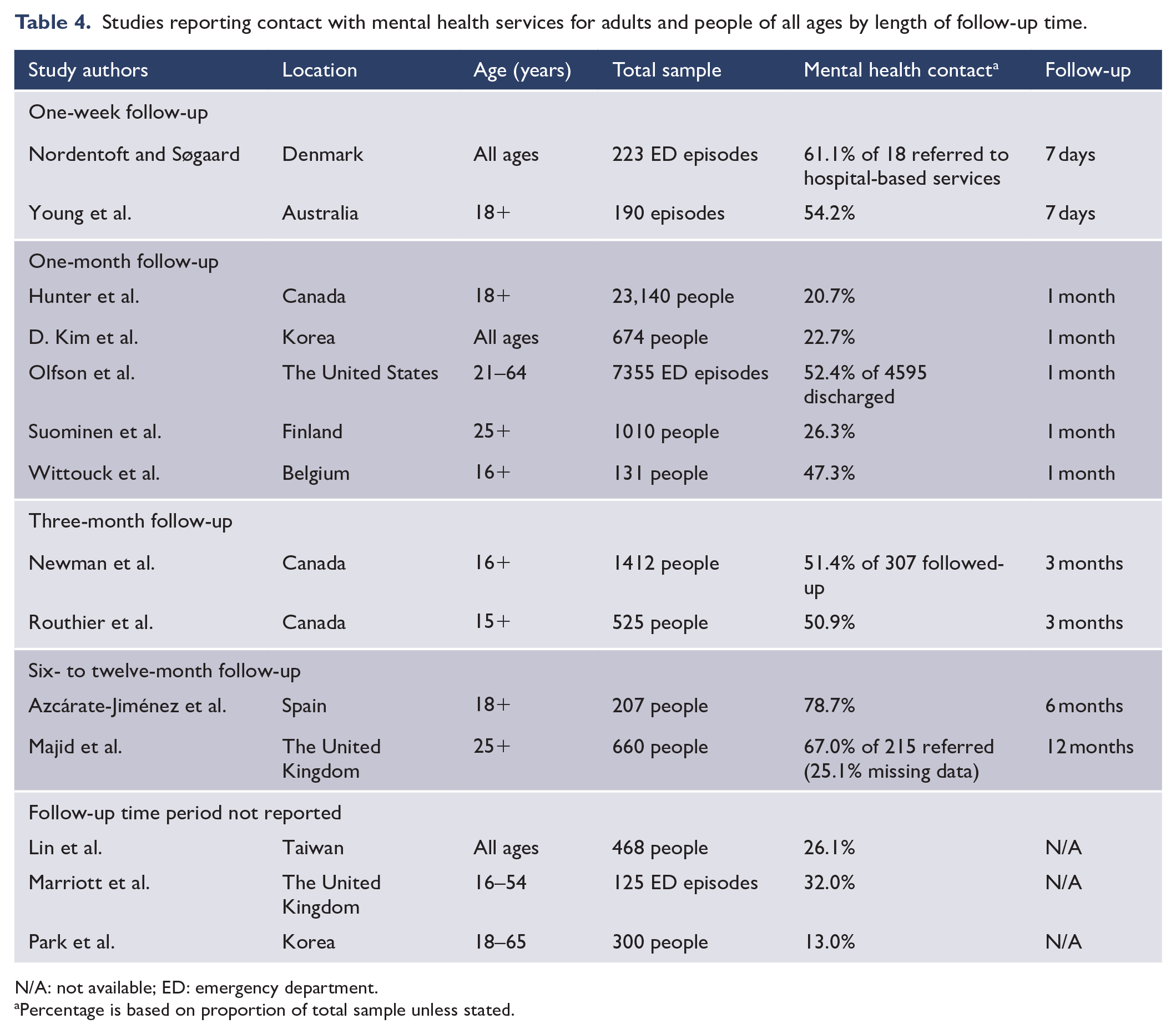
N/A: not available; ED: emergency department.
Percentage is based on proportion of total sample unless stated.
Mental health admissions and referrals
Thirty-one (66.0%) studies reported on mental health admission from ED in adult/all age participants, with the proportion ranging from 1.9% in Korea to 69.9% in the United States. Excluding the two studies which reported on involuntary mental health admission only, on average, 12.5% were admitted. Examining the seven studies conducted in the United Kingdom separately, the data showed that, on average, the proportion admitted was 5.9% (range = 3.2–12.8%). While in the six studies conducted in Asian countries (Japan, Korea and Taiwan), the average proportion admitted was 20.6% (range = 1.9–36.1%). A total of 29 (61.7%) studies reported on referrals to mental health services after an ED presentation with suicidal behaviours (Table 5). The mental health services and health professionals to which people were referred included suicide prevention clinics, community mental health services, outpatient mental health services, alcohol and drug treatment services, child and adolescent mental health services, hospital in the home, partial hospitalisation and day hospital programmes, case management, crisis services, group psychotherapy, psychiatrists and psychologists. Across these 29 studies, the average proportion referred was 27.1%, and this ranged from 1.7% in China to 85.2% in Brazil. Studies with an observation period from 2010 (n = 5) had a higher average proportion referred to mental health services (32.4%; range = 29.6–76.3%) compared to studies conducted prior to 2010 (n = 15, 26.5%; range = 5.7–85.2%).
Studies reporting on mental health admission and referrals after ED presentation for adults and people of all ages by region.
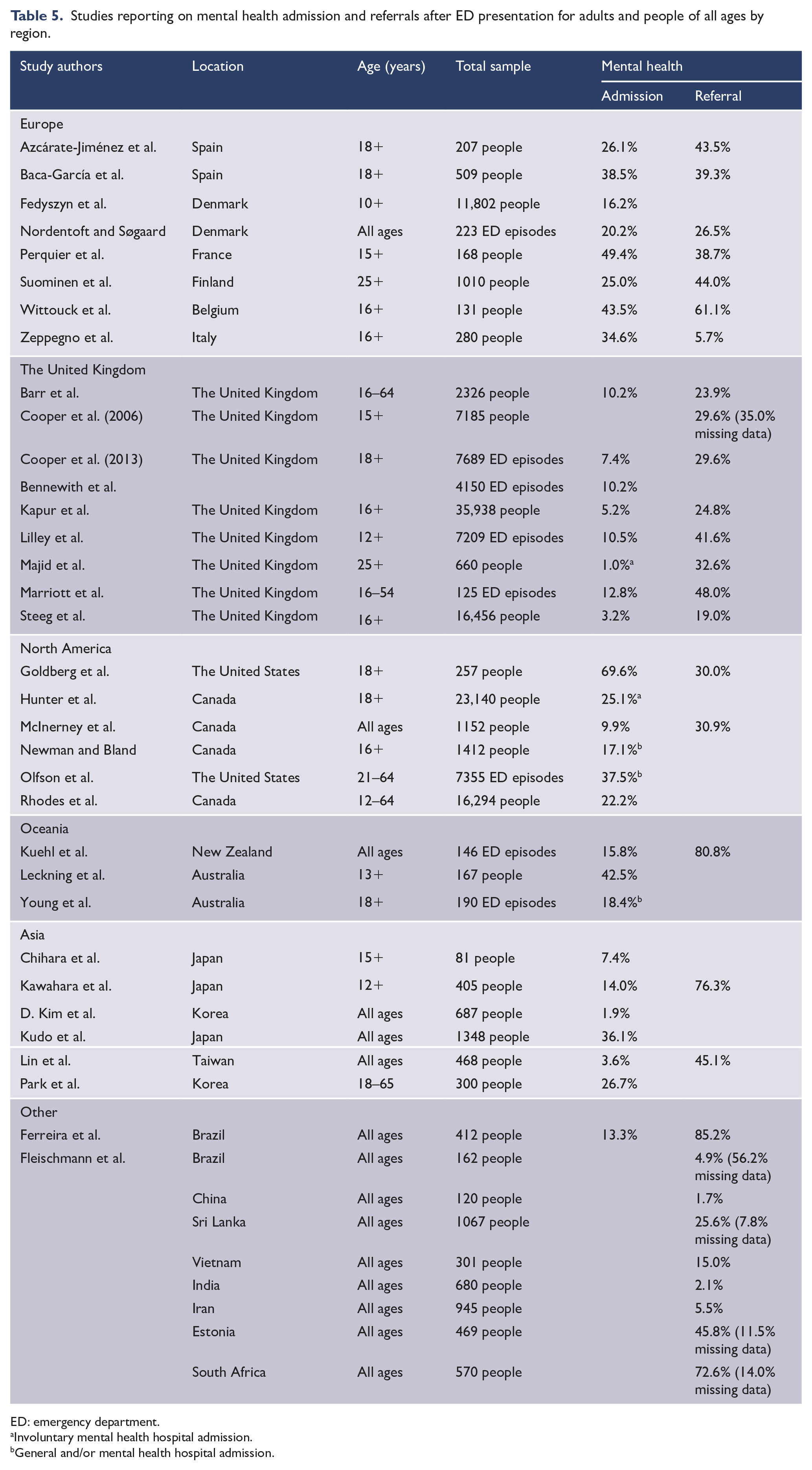
ED: emergency department.
Involuntary mental health hospital admission.
General and/or mental health hospital admission.
Sex differences in mental health service contact and referrals
Five studies (10.6%) provided data on sex differences and contact with mental health services within 1 month following an ED contact (Bridge et al., 2012; Kim et al., 2020a; Olfson et al., 2012; Rosychuk et al., 2016; Suominen et al., 2004). All five studies showed that, on average, the proportion of women who had a mental health service contact within 4 weeks following an ED presentation (47.3%; range = 24.4–53.6%) was higher than for men (43.0%; range = 20.9–49.8%). Seven studies presented data on referrals by sex (Azcárate-Jiménez et al., 2019; Bolger et al., 2004; Cooper et al., 2006, 2010; Ferreira et al., 2016; Lin et al., 2014; Malakouti et al., 2008). A comparison of males and females referred to secondary mental health services in these studies showed little difference in the average proportion referred (males 30.5% vs females 31.6%) with only two studies showing that the proportion of men referred was higher than for women (Cooper et al., 2010; Malakouti et al., 2008). However, between studies, there was wide variation. The lowest referral rates for both men and women were in the study by Malakouti et al. undertaken in Iran (6.1% and 5.1%, respectively). In contrast, 80% of men and 85.1% of women in the study by Ferreira et al. conducted in Brazil were referred to mental health services.
Discussion
Rapid and active support and care after a suicide attempt is critically important to reducing the risk of a subsequent suicide attempt (Inagaki et al., 2019; Stanley et al., 2018). This systematic review of 47 studies aimed to determine what proportion of young people, adults and older adults has contact with secondary mental health services following an ED presentation for suicidal behaviours and to examine referrals to mental health treatment services and mental health admissions after discharge from ED. We found that, on average, young people presenting to ED for suicidal behaviours were more likely than adults to have a secondary mental health service contact, to be admitted to hospital and to be referred to mental health services. For older adults, we found there was a paucity of studies (n = 5), despite evidence that suicide rates in older adults are increasing (Morgan et al., 2018; Wang et al., 2020). Four of the five studies had small sample sizes (less than 150 people or ED episodes), and there were methodological differences across these studies which restricted our ability to make meaningful comparisons. A comparison of studies based on the date of their observation period (prior to 2010 or from 2010 onwards) showed that, on average, studies conducted in the last 10 years had higher proportions referred to and in contact with mental health services than those undertaken prior to 2010. However, we found very few studies in young people or adults who had mental health service contact, admission or referral rates of 50% or more, irrespective of date. These findings suggest the opportunity to provide longer-term mental health treatment to people who present to an ED with suicidal behaviours is being missed.
Interventions and strategies implemented in ED such as educating clients and their families about the importance of follow-up care, assisting with making appointments at convenient times, developing rapport and engaging people in treatment decisions may help improve initial attendance and ongoing engagement with mental health services (Asarnow et al., 2011; Kim et al., 2012; Sobolewski et al., 2013). Studies have shown that a prior mental health diagnosis and previous mental health treatment are both positively associated with receiving follow-up mental healthcare after a hospital presentation with suicidal behaviours which may suggest that positive experiences with mental health services may increase the willingness to re-engage with services in the future (Fontanella et al., 2020; Schmutte et al., 2022). Other factors shown to influence peoples willingness to engage with health services include the attitudes of ED healthcare professionals to people with suicidal behaviours, their level of training and their confidence in providing care to people presenting with suicidal thoughts and behaviours (Boukouvalas et al., 2020). Providing ED staff with specialised suicide education and training may translate to higher rates of referral and better mental health outcomes for patients.
The heterogeneity across the studies in this review made it difficult to compare and present the data in a consistent way. For example, the follow-up periods ranged from 7 to 365 days, and contact with mental health services was reported in a variety of ways including as a proportion of those: not admitted to hospital, discharged from hospital, given a referral, followed-up and of the total sample. Some studies included individuals with multiple ED contacts for suicidal behaviours but selected only one contact to be included, and others included each episode of ED care. We also observed a wide range in the contact, referral and admission rates between studies, which could in part be due to the 47 studies being conducted in 23 different countries and the variations in their healthcare systems. This may include differing thresholds for mental health admission, different models of care such as intensive crisis home treatment services, complexity of referral pathways, the availability of mental health aftercare services, including shortages of old age and child/adolescent psychiatrists and access to universal healthcare. Cultural differences may have also impacted the outcomes, with the authors of studies conducted in Asian countries (Chihara et al., 2018; Lin et al., 2014; Malakouti et al., 2008) noting that the stigma associated with mental illness may explain why patients and/or their family members intentionally misreported the intent of the injury, left hospital before receiving care, refused admission and/or referral to mental health treatment services and failed to attend follow-up appointments.
Almost one-third of the studies in this review used health registries or linked administrative health databases to identify: eligible participants, subsequent hospital admissions and contacts with secondary mental health services. These databases are a valuable tool for health services research, as they are a rich source of population-level data for utilisation of public health services. However, they were designed to collect data for administrative or billing purposes, and few will capture information on the comprehensive range of referral types such as general practitioners (GPs) and full fee-paying services, such as private psychiatrists or psychologists. Researchers need to be aware that this may lead to an underestimation of secondary mental healthcare service referral and contact. The accuracy of International Classification of Disease (ICD) codes from hospital discharge records to identify people with suicidal behaviours from self-injury with no suicidal intent can also present issues (Sveticic et al., 2020). Some studies in this review adopted strategies to minimise the known limitations of administrative databases. For example, Routhier et al. (2012) only included people who attempted suicide and were hospitalised after presenting at ED in an attempt to differentiate suicidal from non-suicidal injuries, while Park et al. (2020) classified a mental health contact as two rather than one outpatient visit, so as to exclude counting people who only attended once to ‘obtain medical documents needed for insurance claims’ rather than for aftercare.
Strengths and limitations
Several strengths and limitations of this systematic review need to be considered. The wide coverage of studies from low-, middle- and high-income countries make the findings more generalisable. However, as only studies where people who presented to ED were included, the findings may not be generalisable to people with suicidal behaviours who do not seek medical assistance from an ED or are admitted directly to hospital for inpatient care. Only referrals made to mental health services at the time of ED presentation were examined in this review. Consequently, referrals made to mental health services or to a GP after leaving hospital could not be determined. In some countries, ED referrals are made primarily to GPs (Fleischmann et al., 2005), and evidence shows that GPs are highly involved in the care of their suicidal patients (Boffin and Van Casteren, 2018). GPs are often the first health professional seen after a suicide attempt (Younes et al., 2020), and they frequently see people within 1 week of hospital discharge following a suicide-related admission (Gunnell et al., 2002). As most studies only documented if an individual had a health service contact, and not the number or types of health service contacts received, the overall level of support and aftercare people received could also not be determined. Finally, although two researchers independently screened the records, it is possible that relevant studies were excluded or missed in the review process.
Conclusion
This review highlights the high proportion of people, both young and old, who present to ED with suicidal behaviours but are not receiving timely follow-up specialist mental health support and aftercare, despite being at a higher risk of subsequent suicide attempts. We observed that referral to mental health services was generally low; however, this review did not examine the reasons underpinning the low rates of contact with secondary mental health service such as non-attendance. A better understanding of mental health service utilisation after an ED presentation with suicidal behaviours may help identify gaps in services. Crucially, this information could assist in the allocation of resources to facilitate the timely implementation of suicide prevention services.
Supplemental Material
sj-docx-1-anp-10.1177_00048674231172116 – Supplemental material for Secondary mental health service utilisation following emergency department contact for suicidal behaviour: A systematic review
Supplemental material, sj-docx-1-anp-10.1177_00048674231172116 for Secondary mental health service utilisation following emergency department contact for suicidal behaviour: A systematic review by YR Feng, GM Valuri, Vera A Morgan, DB Preen, Colleen M O’Leary, E Crampin and A Waterreus in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors acknowledge Megan O’Connor, A/Head of Psychiatric Services Library, North Metropolitan Health Service for her assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by funding from the Office of the Chief Psychiatrist, Western Australia. G.M.V. is being supported by an Australian Research Council Linkage Grant (LP190100968). A.W. is being supported by the Western Australian Future Health Research and Innovation Fund, which is an initiative of the WA State Government.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.