
Abstract
Objective:
To review publications addressing suicidal behaviour in the Australian and New Zealand Journal of Psychiatry, 1967–2012.
Method:
A PubMed/MEDLINE search using the words suicide, attempted suicide (and their synonyms) and Aust NZ J Psychiatr was carried out, and an examination of all tables of contents of the journal for the years 1967–2012 was performed.
Results:
In 342 (7.4%) of 4599 articles there was reference to suicidal behaviour. This ratio was consistent over time, although the nature of their content changed from broader epidemiological and clinical review studies to more focused reports.
Conclusions:
Papers addressing suicidal behaviour have been published consistently in the Australian and New Zealand Journal of Psychiatry since its inception in 1967. Early clinical reviews remain pertinent to the present time.
As the Royal Australian and New Zealand College of Psychiatrists approached the 50th anniversary of its establishment in 1963, an editorial initiative was to invite a number of reviews of important aspects of psychiatric practice that had been published in the Australian and New Zealand Journal of Psychiatry. This review is of publications about suicidal behaviour and its prevention.
Suicidal behaviour is associated with the majority of psychiatric disorders. Although they are not a necessary prerequisite for suicide, an area which is riven with claim and counterclaim (usually with an underlying theme of denigrating the medical model on which psychiatry is based), we cannot escape the responsibility of ensuring that any associated disorder that may be present is adequately diagnosed and treated optimally.
It is beyond the scope of this brief review to examine all aspects of change in academic and clinical psychiatry pertaining to suicide in the last half century – suffice to say that interest in the subject has expanded exponentially, and, in contrast to the mid-1960s, there are now three internationally recognised journals devoted to the subject (Crisis, the Suicide & Life-Threatening Behavior and Archives of Suicide Research), as well as a number of less influential national publications. Naturally, such journals, just as general medical journals available before the Australian and New Zealand Journal of Psychiatry was launched in 1967, have been the repository of much Australian and New Zealand research. Nevertheless, it is instructive to examine what Parker et al. (1984) have designated as publishing in the parish.
An initial search of PubMed/MEDLINE using the words suicide and attempted suicide (and their synonyms) and Aust NZ J Psychiatr was undertaken and then the tables of contents for all years were examined, which resulted in the retrieval of additional articles, particularly for the pre-1969 journals which PubMed/MEDLINE did not access. Table 1 presents the numbers identified and their percentage of total entries for the journal in 5-year time periods, except for the initial period which is for 6 years.
Publications related to suicidal behaviour in the Australian and New Zealand Journal of Psychiatry, 1967–2012.
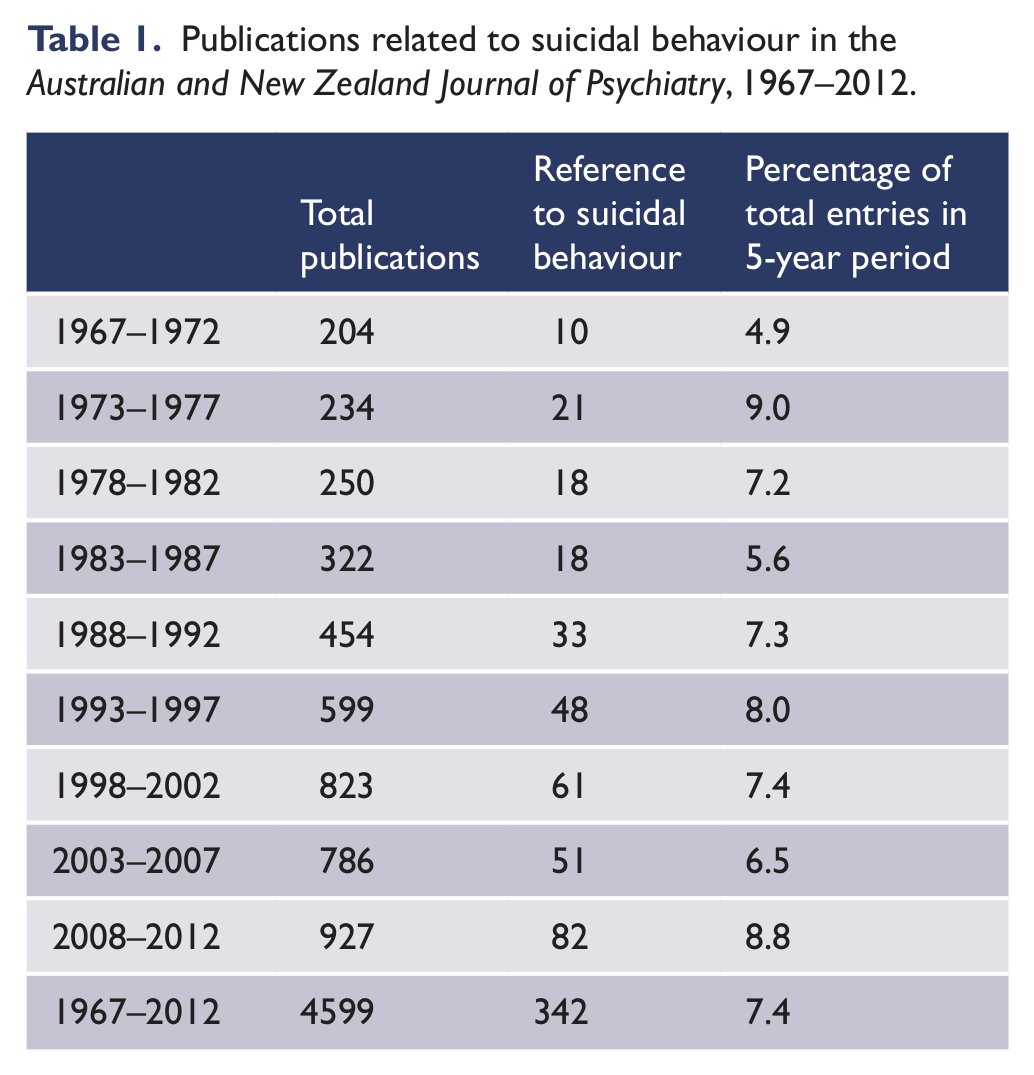
It is appreciated that there will have been articles missed. This will be partly because of reviewer neglect, but also because unwanted outcomes related to suicidal behaviour would undoubtedly have been referred to in some papers that have been omitted. Nevertheless, this crude assessment can give one a feel for the frequency with which the journal addressed issues pertaining to suicide – being consistently in about 6–8% of publications, with no time period dominating.
Indeed, there was no sequence of years that could be manipulated for making a case for such research being either ignored or given favourable consideration for publication. This is unexpected, as I have personal recollection of a new editor stating that there was too much suicide research published and that he would reverse the trend! On the other hand, one may have anticipated an increase in publications on research into suicidal behaviour, as it received a considerable boost in funding after the belated political realisation of the magnitude of the problem in the mid-1990s. However, there has also been much Australian and New Zealand work published elsewhere in speciality journals.
It is pertinent to reflect on the state of what is now termed suicidology in Australia and New Zealand in the 1960s. In an editorial brief in the journal in 1969, presumably written by Stoller, the then editor, it was noted that ‘We are fortunate in Australia in having a wide variety of recent publications from all States relative to the topics of suicide and attempted suicide …’ (1969: p. 361). Most such publications had been in the Medical Journal of Australia, and it is curious, though those in New Zealand may not be surprised, that the editorial did not specifically mention New Zealand, as the work of Ironside (1969), in his influential paper about iatrogenic contributions to suicide published in the New Zealand Medical Journal, was referenced.
Further perusal of early volumes reveals that in the very first edition there were at least four mentions of suicide, although two were in a section devoted to brief abstracts of Australasian psychiatry published elsewhere and are not included in this analysis. It is of note that the profession’s responsibility with regard to suicide prevention was referred to in the very first article in the journal, the 1966 presidential address of Dr Bill Dibden (1967). Also in the original edition was reference to no cases of suicide in an Aboriginal community by Kidson (1967), and it is of interest that a year later a report from New Zealand of Maori adolescents did not refer to suicidality at all (Gluckman, 1968). However, as a harbinger of what was to come, in 1968 Cawte drew ‘attention to the emergence of depression, suicide, and attempted suicide – comparative rarities in traditional culture’ (1968: p. 4). Cawte also asked ‘whether an evolution of mental illness patterns is taking place during the rapid acculturation of Australian Aborigines and if so, what is its nature.’ (1968: p. 3) This has become a matter of great concern for Indigenous communities in both Australia and New Zealand, and has been explored further in recent journal publications (e.g. De Leo et al., 2011; Hunter, 2011; Beautrais et al., 2006).
Other influential early work included the comprehensive review of epidemiological studies by Hetzel (1971) and the review of Australasian suicidology by Lindsay (1978). More general overviews were provided by Henderson and Williams (1974), on the prevention of parasuicide, and by Goldney and Burvill (1980), on the trends in suicidal behaviour and its management.
These epidemiological and review papers gradually gave way to more focused research.
The virtually insurmountable task of predicting suicide in the individual was noted by Goldney and Spence (1987).
The role of firearms in suicide was emphasised by Cantor and Lewin (1990), long before the Port Arthur massacre in Tasmania, in which 35 people were killed and 23 wounded.
The evidence, mechanisms and prevention of adolescent suicide clusters were addressed by Hazell (1993).
Litigation related to suicide was reviewed by Cantor and McDermott (1994).
Hazell and King (1996) presented arguments for and against teaching suicide prevention in schools.
A contribution to our theoretical understanding of suicide, the absolute misery hypothesis was posited by Barber (2001).
Suicide in rural communities was reported by Page and Fragar (2002).
There have been contributions addressing youth suicide (Burns and Patton, 2000), and more specifically suicide prevention in early psychosis (Power et al., 2003).
The Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines Team for Deliberate Self-Harm published its recommendations in 2004.
The controversy about the association of serotonin reuptake inhibitor antidepressants with suicidal behaviour was addressed by Hall and Lucke (2006) and by Goldney (2006).
The favourable influence of media reporting guidelines was noted by Niederkrotenthaler and Sonneck (2007).
The effectiveness of bridge barriers in preventing suicide was reiterated by Beautrais et al. (2009).
Skegg et al. (2010) contributed to the issue of controlling access to means in an analysis of suicide and occupation.
Having conducted this necessarily selective and limited historical review, the question is sometimes asked: Why study the history of psychiatry? Mulder (1993) has addressed this question and noted that not only was it necessary in a general intellectual sense, but also for us to appreciate the ambiguity of some of our concepts and also ‘more convincingly explain the reality and consequences of mental illness to a skeptical public’ (1993: p. 556). This is amply evident in this brief review of publications referring to suicidal behaviour in the Australian and New Zealand Journal of Psychiatry. There has been epidemiological documentation of change, for example, in the patterns of Indigenous illness in both Australia and New Zealand; there has been more focused research addressing specific aspects of suicidal behaviour; and, from a practical point of view, there has been a reaffirmation of what is sometimes considered to be an old-fashioned clinical approach. With regard to the latter, we can return to volume 1, issue 1 in 1967, when, in the previously noted first article by Dibden (titled: In the looking glass), Dibden stated that ‘It needs to be said … that suicide is a symptom of mental or emotional disorder … We must be clear and steadfast on matters such as these, if our public image is to reflect true’ (1967: p. 10). Furthermore, it remains pertinent to quote from Stoller’s editorial brief 2 years later (titled: On the prevention of suicide): ‘In regard to completed suicides, this resides to considerable degree in the management of the middle-aged and elderly depressive male, the alcoholic who has recently suffered an object loss and the younger schizophrenic with affective disturbance. Those who have attempted suicide are at greater risk of completing suicide if they are older, repeat attempts, exhibit psychotic features and have become depressed without adequate cause. It follows, therefore that early recognition of depression, adequate treatment (with sufficient doses of antidepressant drugs or electrocerebral therapy) and follow-up (including alerting of relatives and significant others) can make an impact on suicide figures. Practitioners need not only to recognize suicidal tendency but also to avoid unconscious collusion in a patient’s suicide.’(1969: p. 361)
Stoller also referred to the interpersonal component of attention seeking in some suicide attempts; the reduction of suicide following restriction of the availability of barbiturate sedatives; and emerging evidence about the effectiveness of lithium in reducing suicide.
With the additional comment that there is now good evidence for the effectiveness of lithium; that clozapine offers protection for those with severe schizophrenic illnesses; that not only barbiturates should be prescribed with caution; and that psychotherapeutic approaches have been refined, it is sobering, although perhaps reassuring, to reflect that in terms of a clinician’s individual approach to suicide prevention, there is really very little to add to what was well documented over 40 years ago. Perhaps this is the real benefit of a historical review; appreciating that the work of our founding clinicians and researchers, as documented over the years in the Australian and New Zealand Journal of Psychiatry, warrants appropriate recognition.
In concluding, although the discerning reader, or more probably those researchers and clinicians whose work has been omitted from this necessarily selective and limited overview, who will be well aware that other important work has also been published in the journal, it is amply evident that even this brief retrospective could well provide the basis for quite a comprehensive and authoritative textbook on the subject of suicidal behaviour.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The author reports no conflicts of interest. The author alone is responsible for the content and writing of the paper.