
Abstract
Objective:
We conducted a data linkage study in Victoria, Australia, to determine the proportion of young females who are treated in hospital for self-harm who go on to die by suicide within 5 years and to identify factors associated with increased suicide risk in this same cohort.
Method:
We undertook a cohort study following 3689 female patients aged 10–24 years, who were initially treated in hospital for self-harm during the 2-year period January 2011 to December 2012. We followed each patient for 5 years unless they died first, in which case, they were followed until their date of death. We used inpatient admissions from the Victorian Admitted Episodes Dataset and emergency department presentations from the Victorian Emergency Minimum Dataset linked to death data from two sources, the Victorian Suicide Register and the National Death Index.
Results:
Twenty-eight individuals (0.76% of the total cohort) died by suicide within 5 years of their index admission. In multivariate survival analysis, only suicide ideation at the time of self-harm (hazard ratio = 4.59; 95% confidence interval: 1.70, 12.38) and a decreasing time between successive self-harm episodes (hazard ratio = 4.38; 95% confidence interval: 1.28, 15.00) were associated with increased suicide risk.
Conclusion:
Although the vast majority of young females who present to hospital for self-harm do not die by suicide within 5 years, our results suggest young females expressing suicide ideation and those presenting frequently with decreasing time between successive episodes should be prioritised for suicide-prevention efforts.
Introduction
Suicide is the leading cause of death for Australian females aged 10–24 years, accounting for approximately one-third of deaths in 2020 (Australian Bureau of Statistics, 2021). Before the COVID-19 pandemic, there was some evidence that suicide rates were increasing in young females in Australia (Stefanac et al., 2019) and in several other countries (Curtin, 2020; O’Neill and O’Connor, 2020; Ruch et al., 2019; Skinner and McFaull, 2012; Stallard, 2016; Twenge et al., 2019). In addition to increasing rates of suicide, there was evidence that rates of hospital-treated self-harm were increasing across many Australian states before COVID-19 (Clapperton, 2017; Leckning et al., 2016; Perera et al., 2018; Sara et al., 2023), particularly among young females. Since the onset of the COVID-19 pandemic, emergency department (ED) presentations for self-harm or suicidal ideation in one large Australian state have continued to increase, particularly among young females where a 47% per annum increase has been identified (Sara et al., 2023). Self-harm (including self-injury without intent to die as well as suicide attempts) is a known risk factor for suicide (Cooper et al., 2005; Hawton et al., 2015; Van Orden et al., 2010) and while the absolute risk of suicide following hospital-treated self-harm has been found to be greater in males compared to females, the risk relative to that in the general population has been found to be higher in females (Cooper et al., 2005; Hawton et al., 2015). The risk of suicide is particularly elevated for people who repeatedly self-harm (Haw et al., 2007; Mendez-Bustos et al., 2013; Zahl and Hawton, 2004), and this is especially true for young females (Zahl and Hawton, 2004), suggesting that repetition might be an important risk factor in this population.
Various explanations have been proposed for the increasing trends in young female suicide and self-harm rates. Some have suggested that the increases in this population are likely to be a result of social determinants, given the increases have occurred over a relatively short period (Luby and Kertz, 2019). Young females use social media more frequently than young males (Kelly et al., 2018) and are also more likely to experience cyberbullying (Kim et al., 2018). Relatedly, one suggestion is that increased social media use among adolescents in particular, is leading to a rise in interpersonal stress (Luby and Kertz, 2019), and mental health conditions (e.g. mood disorders) (Twenge et al., 2018, 2019), and these rises may be influencing suicide and self-harm rates. Other explanations relate to evidence that adolescent females are shifting to using more lethal means when attempting suicide (Roh et al., 2018; Ruch et al., 2019). Method escalation (i.e. when individuals switch from one method of self-harm to another method which is associated with more lethal outcomes) could also be influencing suicide rates in this population, although studies regarding method escalation and suicide risk have produced mixed findings (Witt et al., 2018, 2021).
While the vast majority of people treated in hospital for self-harm do not go on to die by suicide (Carter et al., 2017; Carter and Spittal, 2018), and there is acknowledgement in the suicide-prevention field that predicting future suicide risk is difficult and imprecise (Carter et al., 2017; Carter and Spittal, 2018), incidents of hospital-treated self-harm still represent opportunities for suicide prevention. In Victoria, a yearly average of 1800 ED presentations and 1000 hospital admissions for self-harm in young females aged 15–24 years occurred over the 10-year period 2006/07–2015/16 (Clapperton, 2017). These types of hospital contacts provide opportunities for linking people into ongoing community-based care (Spittal et al., 2017), and this may be particularly true for young females, given a recent Victorian study showed hospital contact for self-harm in the year prior to suicide was 3.5 times more likely for young females aged 10–24 years than for males aged 25–49 (the reference category) (Clapperton et al., 2021a).
A meta-analysis found active contact and follow-up type interventions were effective in preventing suicide in patients admitted to EDs for a suicide attempt (Inagaki et al., 2015). One such intervention currently being implemented in Victoria is the Hospital Outreach Post-suicidal Engagement (HOPE) initiative which provides enhanced support for people who present to the ED for intentional self-harm (Williamson et al., 2021). Key interventions delivered as part of the HOPE programme include, but are not limited to, assertive outreach, family support, clinical risk assessment and management, safety planning and substance use intervention (Williamson et al., 2021). A preliminary assessment of the HOPE initiative demonstrated promising results, showing improved subjective well-being and connection with supports in participants (Williamson et al., 2021). Despite these promising results, given the sheer volume of people, especially young females, being treated in Victorian hospitals following self-harm, it is likely still difficult for health services to follow-up adequately all individuals. For this reason, any information that can be provided regarding who is at greatest risk of suicide following hospital-treated self-harm should prove useful for targeting individuals who may benefit most from more active follow-up. Linkage studies using hospital administrative data show promise for this purpose and have been increasingly used to attempt to identify factors that might be associated with increased risk for suicide following hospital-treated self-harm (Bergen et al., 2012a, 2012b; Carter et al., 2005; Christiansen and Jensen, 2007; Cooper et al., 2005; Haw et al., 2007; Hawton et al., 2015; Kapur et al., 2015; Lilley et al., 2008; Owens et al., 2015; Reith et al., 2004).
Given the increasing suicide rate among young Australian females and the known high levels of hospital contact prior to suicide within this same population, we conducted a data linkage study in Victoria with two aims. The first aim was to determine the proportion of young females who are treated in hospital for self-harm who go on to die by suicide with 5 years, and the second was to identify factors associated with increased suicide risk in this same cohort.
Method
Study design and participants
We undertook a cohort study following patients who were initially treated in hospital for self-harm during a 2-year period (January 2011 to December 2012). From this index admission, we followed each patient for 5 years unless they died first, in which case they were followed until their date of death. Patients were eligible for inclusion in the study if they were aged between 10 and 24 years at index admission and were female.
Data sources
We used inpatient admissions from the Victorian Admitted Episodes Dataset (VAED) and ED presentations from the Victorian Emergency Minimum Dataset (VEMD) linked to death data from two sources, the Victorian Suicide Register (VSR) and the National Death Index (NDI).
The VAED is a unit record data file maintained by the Department of Health and Human Services on all public and private hospital admissions in Victoria, which consists of patient demographics and morbidity information and is coded to the World Health Organization (WHO) International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM). The VEMD comprises demographic, administrative and clinical data detailing presentations at Victorian public hospitals with designated 24-hour EDs, and data are coded to the relevant VEMD User Manual published by the Victorian Department of Health and Human Services (Department of Health & Human Services, 2017–2019). The VSR is an ongoing register established by the Coroners Court of Victoria and contains information on all suspected and coroner-determined suicides reported to the Victorian Coroners Court (Sutherland et al., 2018). Detailed information regarding deaths that are included in the VSR can be found in Sutherland et al.’s study (2018) under the ‘Case identification’ heading. The NDI contains all death records for Victoria and is maintained by the Registrar of Births, Deaths and Marriages in Victoria.
The Coroners Court of Victoria supplied VSR data to the Centre for Victorian Data Linkage Unit (CVDL) via the secure data exchange portal. The only VSR variables included were name, date of birth, age, sex and local government area of residence. CVDL linked the hospital data sets to the NDI and VSR and all data were then de-identified. Only the de-identified data sets, containing a linkage ID, were transferred to researchers using the secure data exchange portal.
Data selection and definitions
Death data (from the VSR and the NDI) and hospital data (from the VAED and the VEMD) were supplied to the researchers for the period 1 January 2011 to 31 December 2017. VSR data included all suspected and coroner-determined suicides. To avoid double counting of episodes we (1) considered hospital inpatient admissions with an admission source indicating a transfer from another hospital or statistical separation (change in care type within the same hospital) in consecutive records to be part of the same episode and recoded them to be the one inpatient admission; (2) excluded any ED presentation coded as being admitted to a ward (as the episode would also be recorded in the inpatient admissions data set); and (3) excluded any hospital episode (ED presentation or hospital admission) that ended in ‘death’. We considered a hospital contact to be for self-harm if the hospital record included ICD-10-AM diagnosis codes in the range X60–X84 (intentional self-harm) in the VAED or the ‘human intent’ variable in the VEMD-indicated self-harm. Hospital-treated self-harm in this study comprises all incidents where hospital coders determined that the injury or poisoning was purposely self-inflicted, meaning self-harm both with and without intent (the latter, sometimes termed non-suicidal self-injury) are also included. We retained all self-harm episodes if they occurred among the cohort of females aged 10–24 years who were identified as having an index hospital contact for self-harm in the 2-year period 1 January 2011 to 31 December 2012.
We used the Socio Economic Index For Areas (SEIFA; Australian Bureau of Statistics, 2011) to source an area-level measure of socioeconomic circumstances. The measure we used was the Index of Relative Socio-economic Advantage and Disadvantage (IRSAD). A low score indicates relatively greater disadvantage and a lack of advantage in general whereas, a high score indicates a relative lack of disadvantage and greater advantage in general (Australian Bureau of Statistics, 2011). We applied the SEIFA index at the Statistical Local Government Area (SLA) level by place of residence recorded in each hospital record.
We coded the presence of mental health conditions based on ICD-10-AM codes (range F00–F99) in the hospital records of each episode, and we coded methods based on ICD-10-AM codes (range X60-X84) in the VAED and on ‘cause of injury’ categories in the VEMD. We coded VEMD categories to match VAED categories then aggregated them to match those reported in a recent systematic review (Cai et al., 2021).
We defined method escalation based on known lethality of eight methods as published in the same systematic review (Cai et al., 2021). For each individual, we flagged an episode as ‘increasingly lethal trajectory of method’ if the method used had a higher lethality than the method used in a previous episode. Similarly, we flagged an episode as ‘decreasing time between episodes’ if there was a decrease in the number of days between successive episodes.
All variables were coded as time-varying variables, meaning that for people with multiple episodes of self-harm, the values correspond to their changing circumstances over time. Clinical variables (number of prior self-harm episodes, suicide ideation, method of self-harm, escalation of lethality, time between episodes and mental health conditions) were set to the values of the most recent episode.
Outcome variable
Our outcome variable was death by suicide. Only suicides occurring within the 5-year study window were included.
Predicting suicide
We used survival analysis to identify the characteristics of young females at risk of suicide. Time at risk was defined as from the date of the index admission until death or until the censoring date which was 5 years after study entry. Our models were fit using a Cox proportional hazards model. Because the time-vary nature of many predictors meant a patient could have multiple rows of data, we used cluster-adjusted standard errors to account for this. All models were fit in Stata, version 16.1.
Ethics
The study was reviewed and approved by the University of Melbourne’s Human Research Ethics Committee (Reference Number: 2056962.1). The research received a waiver of consent in accordance with Section 2.3.9 of the National Statement.
Results
Cohort characteristics
The cohort consisted of 3689 females who were aged 10–24 years at the time of their index admission (Table 1). At the time of their index admission, 10% were aged 10–14 years, 53% aged 15–19 years, and 37% were aged 20–24 years. Over the study period, the majority of participants (68%) had a single episode of hospital-treated self-harm, 25% had between one and four episodes, and 7% had five or more episodes.
Characteristics of the cohort of young Victorian females who had hospital contact for self-harm in the 2-year period 2011–2012 (n = 3689).
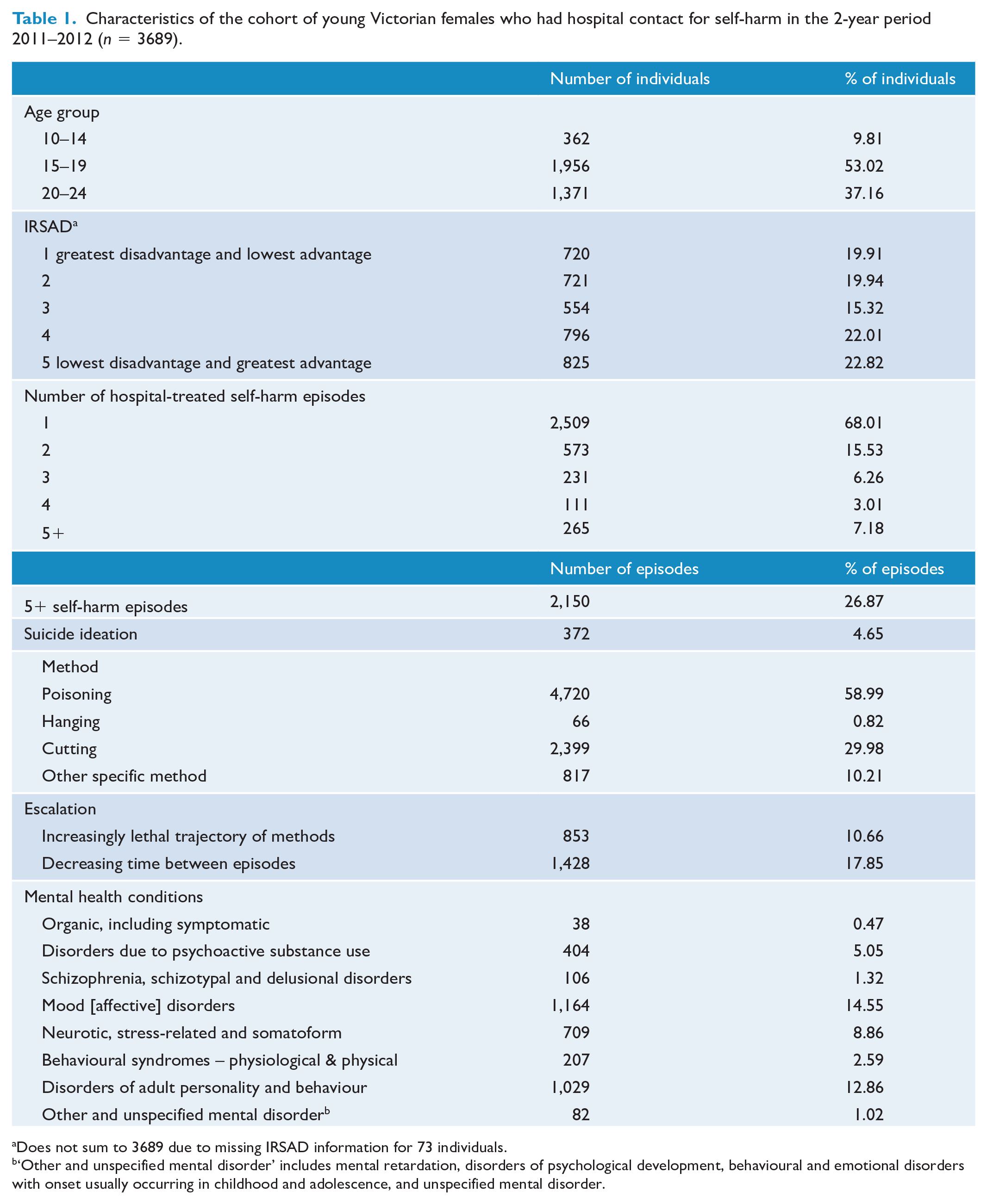
Does not sum to 3689 due to missing IRSAD information for 73 individuals.
‘Other and unspecified mental disorder’ includes mental retardation, disorders of psychological development, behavioural and emotional disorders with onset usually occurring in childhood and adolescence, and unspecified mental disorder.
Including index episodes, the cohort totalled 8,002 episodes of hospital-treated self-harm. Poisoning was used in most episodes (59%). In 11% of episodes, the individual used a method of higher lethality than that used in their previous episode, and in 18% of episodes there was a decreasing time interval between successive episodes. Mood disorders (15% of episodes) and disorders of adult personality and behaviour (13% of episodes) were the most commonly recorded mental health conditions, and suicide ideation was recorded in just 5% of episodes.
Time to suicide
Twenty-eight individuals died by suicide. Of these, 15 occurred in year 1 (1-year suicide probability = 0.4%, 95% CI 0.2%, 0.7%) and 5 in year 2 (2-year suicide probability = 0.5%, 95% CI 0.3%, 0.8%). The 5-year suicide probability was 0.8% (95% CI 0.5%, 1.1%; Figure 1).
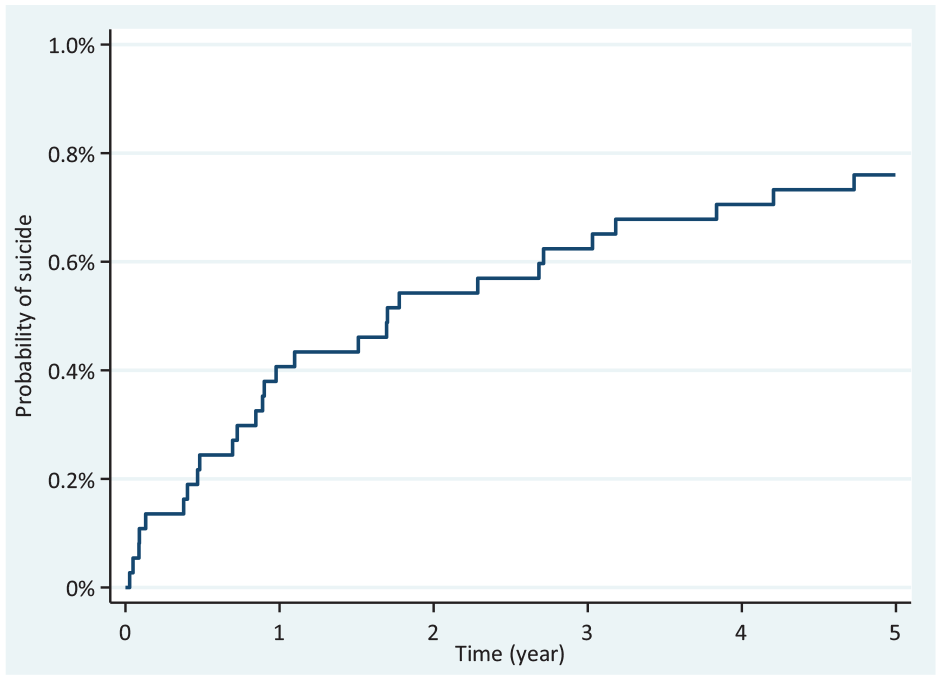
Probability of suicide after hospital-treated self-harm.
Factors associated with suicide
The overall suicide rate in this cohort of young females was 1.53 per 1000 person years. Rates of suicide ranged from 0.28 per 1000 person years for those residing in the lowest IRSAD quintile, to 9.82 per 1000 person years for those who used hanging as a method of self-harm. In univariate survival analysis, suicide ideation [hazard ratio (HR) = 5.39; 95% CI: 2.05, 14.18], five or more self-harm episodes (HR = 4.02; 95% CI: 1.17, 13.80) and decreasing time between self-harm episodes (HR = 6.23; 95% CI: 2.29, 16.93) increased the risk of suicide (Table 2). In multivariate survival analysis, after adjusting for other variables in the model, only suicide ideation at the time of self-harm (HR = 4.59; 95% CI: 1.70, 12.38) and a decreasing time between self-harm episodes (HR = 4.38; 95% CI: 1.28, 15.00) increased the risk of suicide.
Factors associated with 5-year suicide among young Victorian females who had hospital contact for self-harm in the 2-year period 2011–2012 (n = 3689 individuals).
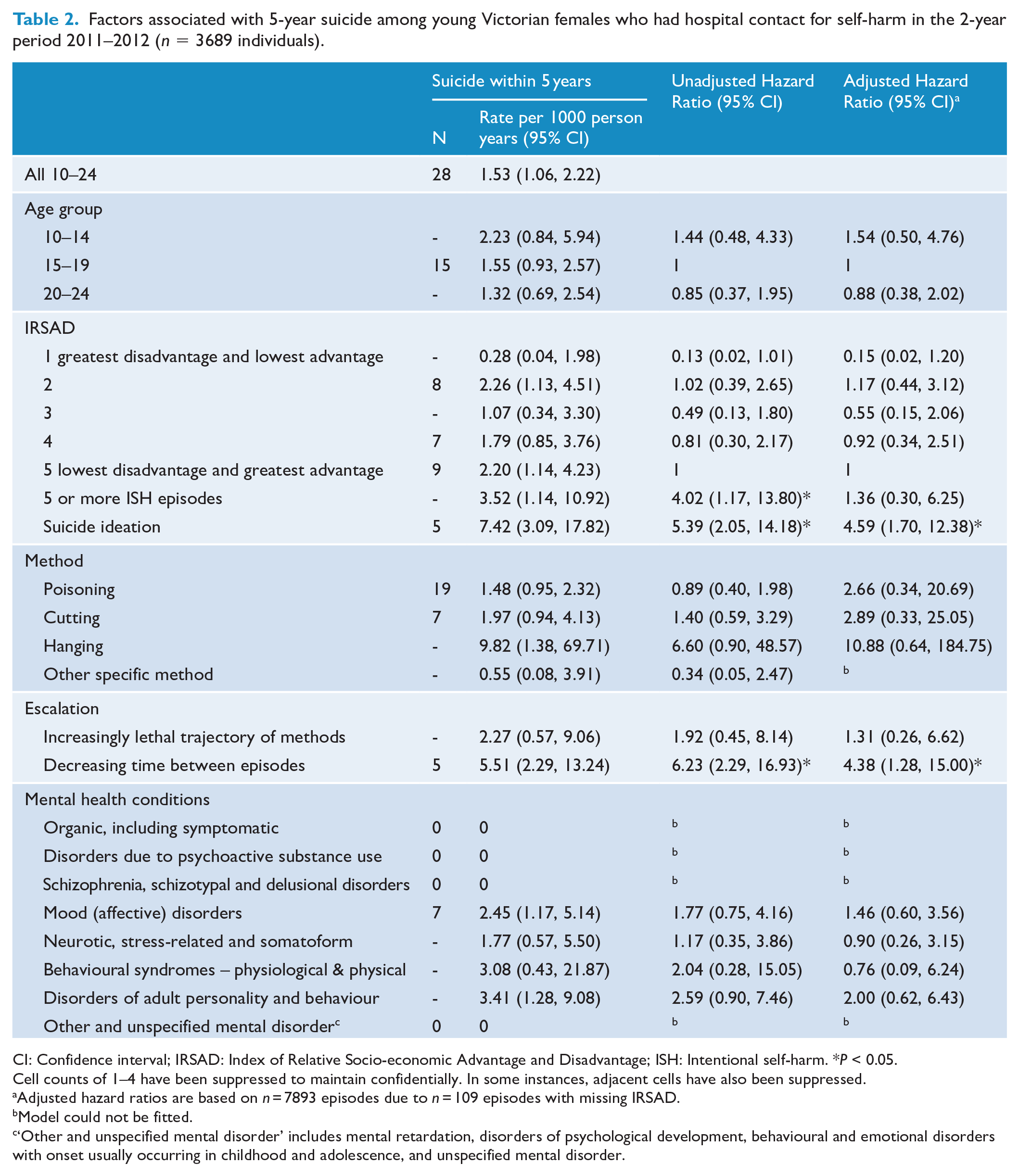
CI: Confidence interval; IRSAD: Index of Relative Socio-economic Advantage and Disadvantage; ISH: Intentional self-harm. *P < 0.05.
Cell counts of 1–4 have been suppressed to maintain confidentially. In some instances, adjacent cells have also been suppressed.
Adjusted hazard ratios are based on n = 7893 episodes due to n = 109 episodes with missing IRSAD.
Model could not be fitted.
‘Other and unspecified mental disorder’ includes mental retardation, disorders of psychological development, behavioural and emotional disorders with onset usually occurring in childhood and adolescence, and unspecified mental disorder.
Discussion
In a large cohort of young females initially treated for self-harm, we identified 28 suicides. This equates to a suicide rate of 1.53 per 1000 person years (almost 40 times higher than the rate of 0.04 per 1000 in the general population of Australian females aged 10–24 years (Stefanac et al., 2019)). While this discrepancy in suicide rates is alarming, it is also expected that the population who are treated in hospital for self-harm have a much higher suicide risk than the general population, given self-harm is a known risk factor for suicide (Cooper et al., 2005; Hawton et al., 2015; Van Orden et al., 2010). Twenty-eight individuals died by suicide after discharge from hospital for self-harm (0.8% of the total cohort), and consistent with previous research (Geulayov et al., 2019; Hawton et al., 2015), the highest incidence of suicide occurred in the first 12 months (1-year suicide probability = 0.4%).
Our analysis also identified two factors independently associated with increased risk of suicide in this cohort. Suicide ideation, recorded at the time of treatment, occurred in 5% of all included self-harm episodes and increased the risk of suicide 5-fold. Decreasing time between hospital-treated self-harm episodes, which was evident for 18% of episodes, increased the risk of suicide by almost four and a half times.
Approximately one-third of young Victorian females who die by suicide are seen in hospitals for self-harm in the year prior to their suicide (Clapperton et al., 2021a), suggesting that presentation to hospital for self-harm is a potential opportunity to initiate suicide-prevention initiatives targeting young females. Despite this high proportion who have contact and the high rate of suicide identified in this study, we found that the absolute risk of suicide following hospital-treated self-harm in our cohort was low (0.8%). Our finding is lower than the 3.9% estimate of 5-year suicide risk following hospital-treated self-harm published in a systematic review (Carroll et al., 2014). However, given our cohort consisted of young females, this discrepancy is not surprising as the authors stated that estimates of fatal repetition of self-harm were higher in males and older cohorts (Carroll et al., 2014). Although it has been acknowledged that a low absolute risk of suicide – such as we identified in this study – makes individual suicide risk prediction difficult (Carter et al., 2017; Carter and Spittal, 2018; Olfson et al., 2017), we believe our study has still identified factors associated with increased suicide risk in this population which can be used to inform high-priority groups for follow-up care after discharge.
The finding that suicide ideation was associated with increased risk of suicide at first seems intuitive; however, previous research about the association between suicide ideation and subsequent risk of suicide is equivocal. In outpatients treated for mental health conditions nearly daily suicidal ideation has been shown to be associated with greater risk of suicide attempts and suicide, the increased risk continues over the subsequent 2 years, and the relationships between suicidal ideation and suicide attempts and suicides were found to be similar across all age groups (Rossom et al., 2017). Similarly, a study involving four samples (i.e. adolescent psychiatric patients, adolescent high school students, university undergraduates and random sample of adults) that examined the associations of established suicide risk factors (including suicide ideation) to attempted suicide, identified the strongest association was with suicide ideation (Klonsky et al., 2013). In contrast, multiple other studies in varied populations have showed that current or recent suicide ideation has very little association with suicide attempts or suicide, see review by Silverman and Berman (2014). While all these studies are concerned with suicide ideation and its relationship with suicide attempts and suicide, they did not examine suicide ideation in the context of self-harm as we have in this study. Consequently, suicide ideation in combination with hospital-treated self-harm should be considered a risk factor for suicide in young females.
In addition to suicide ideation, we also identified a decreasing time interval between successive self-harm episodes as inferring increased risk of 5-year suicide in our cohort. Although we could not identify any studies that examined time between self-harm episodes and suicide risk in the same way we did, some studies of suicide attempts and suicide have related findings. A study of adolescents found the more suicide attempts an individual made, the shorter the average period of time before the next repeat suicide attempt (Goldston et al., 2015), but the relationship between the shorter time between attempts and suicide was not assessed. Also, a recent US population-based case–control study found an increase in mental health care visits in the quarter most proximal to suicide for cases but not controls (Chock et al., 2019). Although this US study examined visits for mental health conditions rather than self-harm, an increase in contacts could suggest that the time between episodes lessened in this study too. Our study finding suggests that hospital staff need to be aware that the intent to suicide associated with self-harm may increase as time between subsequent hospital-treated self-harm episodes decreases.
Strengths
The main strength of this study relates to the representativeness and comprehensiveness of the data we included. In contrast to other similar studies, we have included ED presentations as well as inpatient admissions, and we have included data sets that cover the population of the state of Victoria. Due to the comprehensiveness of the data sets included in our study, we were able to estimate suicide risk in a very specific population even though the absolute number of suicides was low. Relatedly, our study also provides estimates inherent to Victoria which can be used to inform locally applicable interventions.
Another strength is that our study is particularly timely, given that during the recent COVID-19 pandemic, it appears that young people have been disproportionately affected (Clapperton et al., 2021b; Yard et al., 2021). A recent systematic review found increased numbers of self-harm hospital presentations among adolescents, particularly females (Steeg et al., 2022) indicating that the identified trends in young female self-harm (Leckning et al., 2016; Perera et al., 2018) and suicide (Stefanac et al., 2019) rates could continue. Therefore, this study is opportune in that it provides clear guidance as to the young females who could be prioritised for intensive follow-up at this time of potentially heightened risk.
Limitations
Our study has a number of limitations that must also be acknowledged. First, the study period and data we used covered the period 1 January 2011 to 31 December 2017. Index episodes were identified as the first that occurred in the period 1 January 2011 to 31 December 2012; however, individuals may have had self-harm episodes prior to 1 January 2011.
Although the hospital-based data presented should be representative of most Victorian hospital-treated incidents of intentional self-harm, general data quality issues in hospital administrative data sets (including, specifically those used in this study) (Sheppard et al., 2022) suggest that the data presented in the study are likely to be an underestimate of the true incidence of hospital-treated self-harm. Consequently, our finding that 0.8% of the cohort died by suicide is likely an overestimate of the overall 5-year suicide risk associated with hospital-treated self-harm. In addition, it is possible that some factors we studied may be more likely than others to be recorded in these data sets which could have impacted the hazard ratios we calculated.
We found no evidence that increasing lethal trajectory of methods was associated with increased risk of suicide. While this is consistent with previous work in Victoria using ambulance data (Witt et al., 2021), it could also reflect the bluntness of our methods of self-harm categories. We based our definition of method escalation on the lethality of eight different methods (Cai et al., 2021) which required all poisoning cases to be considered to have the same lethality. It is probable that different methods of poisoning have very different lethality; however, these differences would not be reflected in our definition of method escalation.
Finally, we were unable to examine suicide risk in all young females who self-harm, only the population who are treated in hospital. As such, the associations identified here are specific to the cohort of young females treated in hospital and not the general population.
Conclusion
Although the vast majority of young females who present to hospital for self-harm do not die by suicide within the following 5 years, our results suggest young females expressing suicide ideation and those presenting frequently with decreasing time between successive episodes should be proactively encouraged to join assertive outreach programmes such as the current HOPE initiative in Victoria. This initiative has produced promising results so far (Williamson et al., 2021), although, whether participation in the programme is associated with decreased suicide risk remains to be seen. If this intervention is not shown to be effective for reducing suicide risk in young females, then developing different interventions, or tailoring the assertive outreach to better suit young females, should be prioritised.
Footnotes
Acknowledgements
The authors would like to thank the Centre for Victorian Data Linkage for providing linkage services and the custodians of the data collections (Coroners Court of Victoria and Victorian Department of Health and Human Services) for providing the data. The views expressed in this article are those of the authors and do not necessarily represent those of the Victorian Department of Health and Human Services or the Victorian Government of Australia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: A.C. is supported by an Australian Rotary Mental Health Research Grant.