
Abstract

Introduction
Initial evidence in 2020 suggests that the COVID-19 pandemic did not result in an increased suicide rate in Australia (Clapperton et al., 2021). However, many surveillance systems for suicide using coroner’s records or hospitalisation data might not well represent actual suicide rates due to prolonged time in determining suicide intent (De Leo et al., 2010). In addition, these data also overlooked the non-hospitalised cases, which might underestimate the disease burden.
Mental health crises often need ambulance services (Lloyd et al., 2013). Ambulance attendance (AA) data might, hence, capture data on suicide missed from coroner’s records (Lubman et al., 2020). Recent evidence indicates that the lockdown might trigger increased mental health–related AAs in New Zealand (Dicker et al., 2020). The current study aims to examine whether AAs related to suicide attempt/self-injury increased during the pandemic in Australia.
Methods
We extracted 1-month per quarter data on AAs related to self-injury, suicidal ideation and suicide attempts in Australia from March 2018 to March 2021 from the National Ambulance Surveillance System (NASS) (Australian Institute of Health and Welfare, 2021).
Independent-samples t-tests were used to compare the differences in the numbers of AAs related to the three conditions between pre-COVID and post-COVID phases. Interrupted Time Series (ITS) analysis was used to determine whether the trajectories of AAs changed in response to the pandemic. The regression model is expressed as Y = β0 + β1T + β2D + β3P, where Y, T, D and P denote the outcome variable, the time since March 2020, the period (pre-pandemic vs pandemic periods) and the time since the first COVID-19 quarter, respectively; β1, β2 and β3 denote the trajectory before the pandemic, the immediate effect that occurs right after the outbreak and the sustained effect of the pandemic, respectively. The observed values of the rates of the three conditions, compared with their corresponding counterfactual values (i.e. events had the pandemic not occurred), were evaluated. Delayed effect was also assessed. All analyses were conducted using the R software (Version 4.1.2). We also compared the COVID-19 responses between different states by examining the data on the stringency of governments’ responses to COVID-19 from the Australian Bureau of Statistics (https://www.abs.gov.au/articles/state-economies-and-stringency-covid-19-containment-measures).
Results
The key findings of the ITS analysis are shown in Table 1. Overall, the trajectories of AAs for the three conditions increased substantially (p < 0.05) during the first wave immediately (β2) after the outbreak. However, the sustained effect (β3) did not differ significantly between pre- and post-outbreak periods (Figure 1). The data in the second quarter of 2021 were only available for Victoria, ACT and Tasmania, and adding the recent data of the second quarter of 2021 did not change the trend of increased AAs.
Interrupted Time Series analysis of overall self-injury, suicidal ideation and suicide attempts related to ambulance attendances.
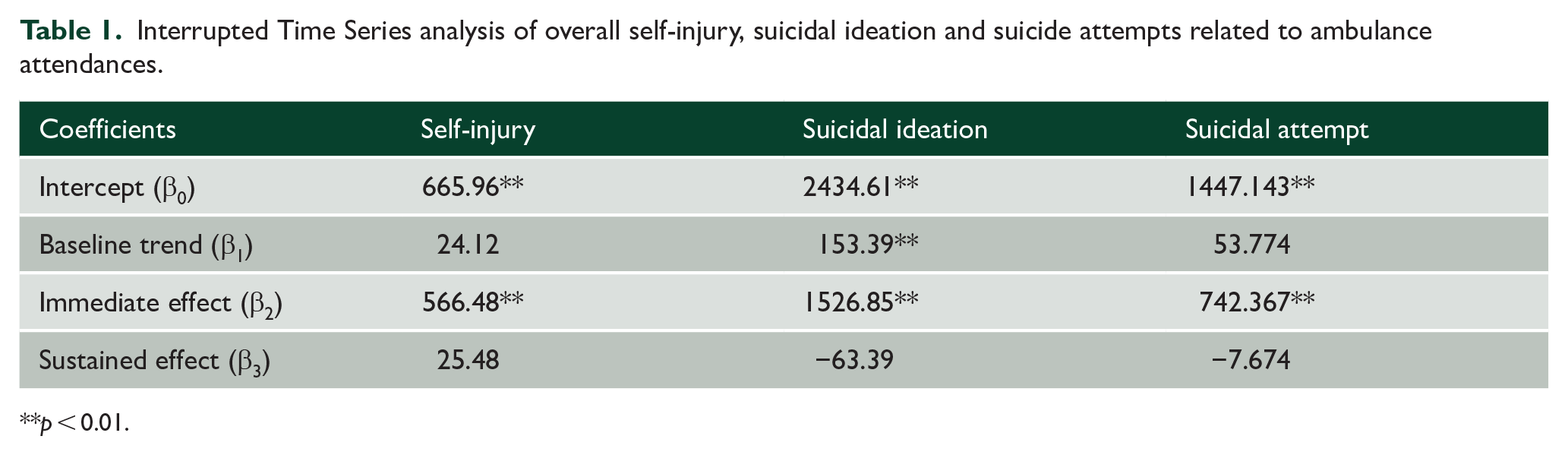
**p < 0.01.

Trends of ambulance attendances related to (a) self-injury, (b) suicidal ideation and (c) suicide attempts.
The average stringency index values of the government’s response in 2020 for NSW, ACT and Tasmania were between 35.8 and 39.8, while the stringency index value for Victoria was 79.3 – which was significantly higher than the other three states/territories. However, the variation in the stringency of the government’s response to the pandemic did not correlate with a substantial difference in the increase in AAs across different states/territories.
Discussion
The abrupt increase in AAs in March 2020 implies that demands in ambulance calls associated with suicidal ideation/attempts and self-injury escalated substantially soon after the COVID-19 containment measures commenced. Note that the increase did not subside over at least 15 months. This phenomenon may not be entirely attributable to increased distress in the population in response to the pandemic (Butterworth et al., 2022) since some of the demands might be shifted to ambulance services due to interruptions in other clinical services.
The primary limitation of this study is the availability of only quarterly snapshots has limited the ability to examine state-level lockdowns that may have occurred at different periods within a reporting quarter. Furthermore, the AA numbers alone may under-represent the actual rates of suicide behaviours, especially mild cases in the community.
Our findings provide a different perspective from previous cross-country evidence focused on fatal suicides (Pirkis et al., 2021), which may be biased towards more serious cases (Williams, 2015). Difficulties in confirming suicidal ideation in some deaths may contribute to the underestimated fatal suicide rate. Therefore, continuous monitoring of the trends is needed to clarify the possibility of delayed recognition of the rise of deaths by suicide since the time trend of fatal suicides does not necessarily correlate with the time trend of suicidal ideation/attempts. The impact of the pandemic on the capacity of clinical services, hence, needs to be re-evaluated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethics approval
The study involves anonymous aggregate data available in the public domain and does not require ethics approval.