
Abstract
Objectives:
Suicide is a leading cause of maternal mortality. Suicidality during and around the time of pregnancy can have detrimental impacts on a child’s development and outcomes. This paper examines prevalence, demographic characteristics, and timing of initial contact with first responders and health services for a cohort of women who experienced suicidality during and around the time of pregnancy.
Methods:
Findings are drawn from the Partners in Prevention (PiP) study, a population-wide linked data set of suicide-related attendances by police or paramedics in Queensland, Australia. A sub-cohort of women was identified, who were between 6 months preconception and 2 years postpartum at the time of a suicide-related contact with police or paramedics (PiP-Maternal). Findings are compared to other girls and women who had a suicide-related contact with police or paramedics (PiP-Female). Prevalence, demographic characteristics, timing of contact with first responders and health services, re-presentations, and mortality are reported.
Results:
The PiP-Maternal cohort comprised 3020 individuals and 3400 births. Women in the PiP-Maternal cohort were younger, more likely to be of Aboriginal and/or Torres Strait Islander descent and live outside of a major city than the PiP-Female cohort. There were high rates of out-of-hours calls to police and ambulance, and similar perceived seriousness of the call between women in the PiP-Maternal and PiP-Female cohorts. Women in the PiP-Maternal cohort were less likely to be admitted to an emergency department within 24 hours, even after matching on covariates. Prevalence of suicidality for women who were pregnant and up to 2 years postpartum was 1.32% (95% CI = [1.27, 1.37]).
Conclusion:
Vulnerabilities and high rates of contact with police or paramedics, coupled with lower levels of follow-up, highlight the critical need to improve service responses for women with mental health needs during these phases of life.
Introduction
Maternal suicide is a leading cause of maternal death in Australia (Australian Institute of Health and Welfare, 2020; Goldman-Mellor and Margerison, 2019; Knight et al., 2019; Queensland Health, 2020; State of Victoria, 2018). Recent data from North America suggests that maternal suicidality may be increasing (Admon et al., 2021; Goldman-Mellor and Margerison, 2019). Based on a nationwide data set of commercially insured individuals in the United States of America, prevalence of suicidality, combining suicidal ideation and intentional self-harm, was estimated to be 0.6% among childbearing women aged 15–44 years, between 1 year before and 1 year after giving birth (Admon et al., 2021). Previously published studies of suicide and suicide attempt rates in the peripartum period provide far lower estimates, with reported rates of 0.43–6.85 maternal suicide deaths per 100,000 live births within 12 months of infant birth or death (Meurk et al., 2021), suicide attempt rates during pregnancy of 40 per 100,000 pregnancies (Gandhi et al., 2006), and a similar rate among postnatal women of 43.9 suicide attempts per 100,000 live births up to 12 months following birth or foetal death (Schiff and Grossman, 2006). A rate of suicidality of 0.6% is approximately 10-fold higher than previously reported suicide attempt rates, but is not out of proportion to the ratio of suicidal ideation to suicide attempts that is observed in the general population (Johnston et al., 2009). Moreover, the estimate of prevalence of suicidality of 0.6% may be conservative, as it is based on administrative data from a commercially insured population and may also be subject to survivor bias (Admon et al., 2021).
Perinatal maternal stress, trauma and suicidality are associated with adverse mental, behavioural and cognitive outcomes for children (Orri et al., 2019; Paquin et al., 2021). One of few studies to examine the impacts of maternal suicidality examined preconception self-harm on perinatal mental health and mother–child bonding. This Victorian study found that self-harming in 20- to 29-year-old women was associated with higher levels of perinatal depressive symptoms and mother–infant bonding problems (Borschmann et al., 2019). The prominence of harmful substance use among women who experience suicidality, and of poisoning as a means of suicide attempt, are also of particular concern, given the potential impacts on infant development, including risk of Foetal Alcohol Spectrum Disorders (Meurk et al., 2014; Clarke and Gibbard, 2003).
Maternal mental health and well-being is an important contributor to infant development, and both current and future well-being of the child (World Health Organization, 2014). Yet, there is a lack of evidence to guide service delivery and a lack of tailored, appropriate services for women to access. Current suicide prevention pathways may not meet the needs of pregnant and postnatal women in relation to clinically meaningful timeframes of care relevant to pregnancy and postpartum periods, or the specific needs of women, mothers, their infants and families (Rubio et al., 2021). There is evidence to suggest that women in the peripartum period who attempted or died by suicide have high levels of health services contact, including hospitalization, compared to women who do not experience suicidality or die by suicide; however, these contacts are not necessarily with a mental health professional or specialist (Meurk et al., 2021).
The primary aim of this article is to present key demographic characteristics, and characteristics of the first response and initial health services contacts of women who were between 6 months preconception and up to 2 years postpartum at and following the time of a suicide-related interaction with police or paramedics. Secondarily, we estimated the prevalence of suicidality among women in this cohort who were pregnant and up to 2 years postpartum.
Methods
Sample and data sources
The study sample for this paper is drawn from the Partners in Prevention–linked data study (PiP-Study), which is a population-wide linked data study comprising 219,164 suicide-related calls to Queensland Police Service (QPS) or Queensland Ambulance Service (QAS) over a 3-year period (1 February 2014 to 31 January 2017). A total of 69,388 individuals were identifiable via record linkage to a range of Queensland Health data sets, namely: The Queensland Hospital Admitted Patients Data Collection (QHAPDC); Emergency Data Collection (EDC); Perinatal Data Collection (PDC); Consumer Integrated Mental Health Application (CIMHA); Alcohol, Tobacco and Other Drugs Information System (ATODS-IS); and the Queensland Death Register (QDR). The cohort linked to more than 7,000,000 health records. Full details of the methodology used to construct this data set, and the profile of the full cohort have been previously outlined (Meurk et al., 2022). Individuals were included in the overall cohort if they were determined to be the subject of a suicide-related call to QPS or QAS during the period being examined:
A suicide crisis was defined as a documented instance or account of suicidal ideation, threatened suicide, threatened intentional self-harm, intentional self-harm, suicide behaviours and suicide attempts. A suicide death was a documented instance or account of first responder attendance to a suicide death. A suicide-related call to emergency services was a call to emergency services that was initially or subsequently determined to be suicide related, as identified in QAS and/or QPS records. (Meurk et al., 2022)
Data were extracted for the period spanning 1 February 2013 to 31 January 2018, ensuring that data were available for at least 12 months pre- and post- an index police or paramedic contact.
Ethical clearances
The study protocol was approved by the Royal Brisbane and Women’s Hospital Health Research Ethics Committee (HREC/17/QRBW/666), the Queensland Police Service research committee (DOC17/1772716), the Queensland Ambulance Service (20170428-15A) and health data were released under Queensland’s Public Health Act (RD007804).
Cohort
The cohort for this study (hereafter PiP-Maternal cohort) is a sub-cohort within the PiP-Study. A woman was included in the PiP-Maternal cohort, if she was within 6 months preconception, and up to 2 years postpartum at the time of her first recorded suicide-related police or paramedic contact over the period of our data set. This time period was arrived at through a number of iterations of analysis, during which we incrementally expanded the phases examined to a maximum meaningful cohort. This was informed by apparent coherence in key characteristics across phases. Cases were identified via QHAPDC, based on a dated hospital admission associated with an International Classification of Diseases, 10th Revision (ICD-10) code O80-O84, indicating that a birth had taken place (Supplementary Table 1).
Classification
Individuals included in the cohort were classified into four categories: (1) preconception (up to 6 months prior to pregnancy); (2) pregnancy; (3) 0–12 months postpartum; and (4) 12–24 months postpartum, based on the phase they were in at the first police or paramedic contact identified within the data set (Supplementary Table 2).
Individuals in the cohort who gave birth multiple times over the time period examined could be included in multiple categories, depending on their phase with respect to all births at the index contact (e.g. a woman who gave birth twice over the period examined could be classified as both preconception and postpartum). For analysis of representations, we classified representations according to those whose representations occurred within the same phase as their index contact, versus those whose presentation occurred in a different phase.
Comparator
Two comparator groups were identified. First, initial analysis compared women within the PiP-Maternal cohort with women in the PiP-Study (hereafter PiP-Female cohort). For this analysis, the age-range of PiP-Female was limited to match the age range of the PiP-Maternal cohort. Overall demographic characteristics of the total PiP-Female cohort (age range 5–101) is also provided in Table 1, but no statistical analyses were conducted regarding comparison with this cohort. Second, in order to examine potential differences in rates of contact with public mental health services and emergency departments, a matched cohort was generated using propensity score matching. Samples were matched using nearest neighbour matching (Thoemmes and Kim, 2011). This computes differences between the two samples (maternal and non-maternal cohort) on selected covariates (age, Aboriginal and/or Torres Strait Islander background and remoteness level) and assigns as many matched non-maternal participants to maternal participants that are equivalent on selected characteristics.
Comparison of Demographic Characteristics of Cohorts.
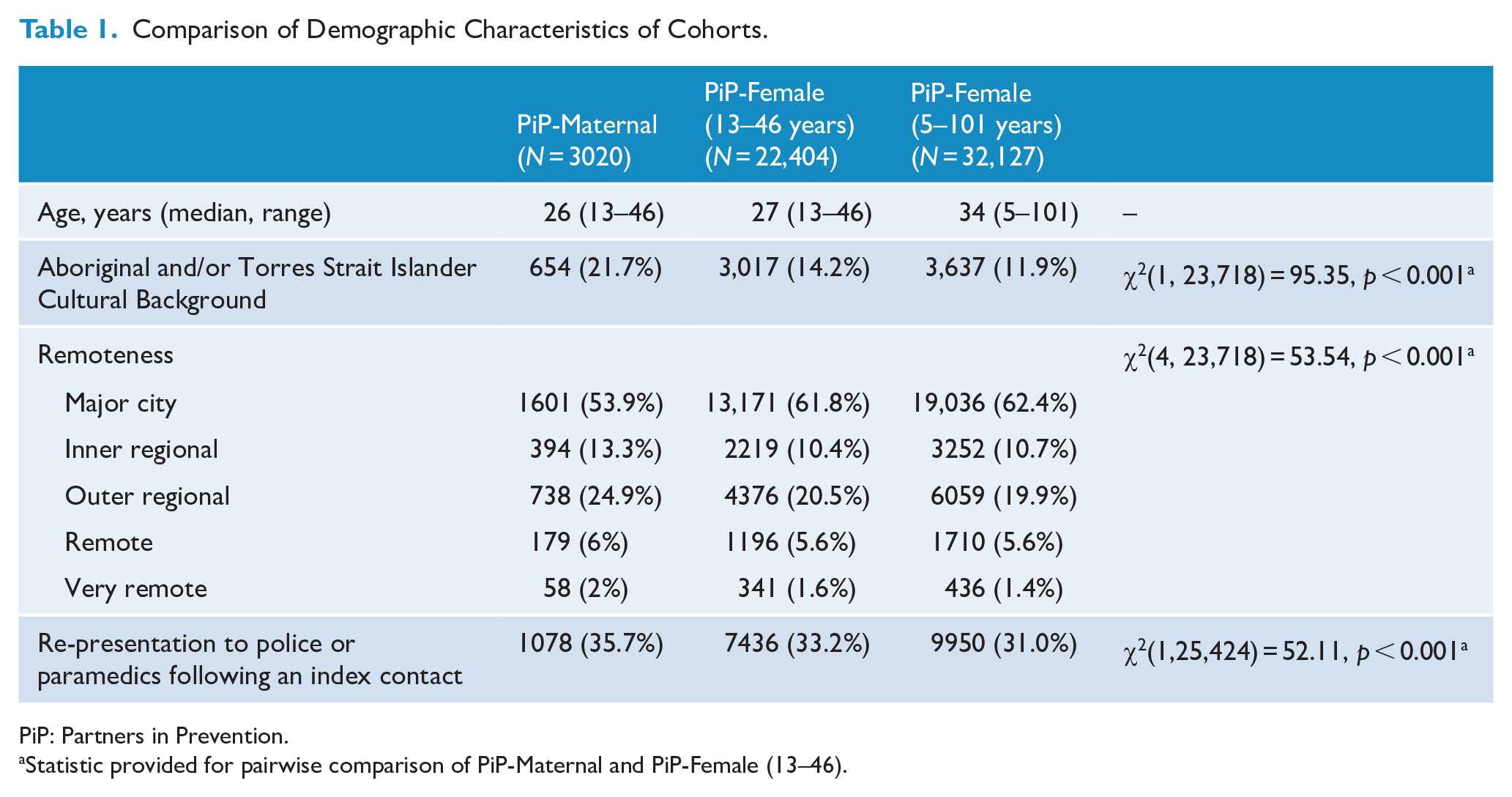
PiP: Partners in Prevention.
Statistic provided for pairwise comparison of PiP-Maternal and PiP-Female (13–46).
Measures
The present analysis is based on the following measures from the PiP-Study.
Demographic variables
Age (years of age, at index event).
Aboriginal and/or Torres Strait Islander background (Aboriginal and/or Torres Strait Islander vs neither Aboriginal and/or Torres Strait Islander).
Services contact variables
ICD-10 code (if O80-O84), with date.
Suicide-related contact with police or paramedics, with time and date.
Dispatch priority at index event.
Contact with a public mental health service, with date.
Contact with emergency departments, with date.
Geographic data
Residential postcode.
Outcomes
Mortality (all cause, and due to self-harm, with date).
Statistical analysis
Data analysis was undertaken using R version 4.0.3 (R Core Team, 2020) by L.W. and M.L., and included descriptive analysis and inferential statistics, namely, chi-square test (χ2) for associations between categorical variables and Kruskal–Wallis (H) for examination of age data. All percentages were calculated after removing missing data. The threshold for significance was nominated at p = 0.05. Remoteness areas for Queensland were estimated using residential postcode information according to the Australian Statistical Geography Standard Remoteness Structure (Australian Bureau of Statistics [ABS], n.d.). There are five classes of remoteness in Australia that are based on a measure of relative access to services: major cities, inner regional, outer regional, remote and very remote.
Estimates of calls placed outside of working hours were defined as any call placed outside of the hours of 8.30 a.m. to 5:00 p.m. Monday to Friday. Contacts with emergency departments were included for analysis, if they occurred within 24 hours of the index event, and for public mental health services, within 14 days after the index event.
Initial analysis was undertaken at a granular level (i.e. each phase within the PiP-Maternal cohort was analysed separately); however, obvious consistencies between groups warranted grouping of analyses in most cases. To estimate prevalence for women who were pregnant and up to 2 years postpartum, estimates of suicidality at index contact were pooled across the 3-year period 1 February 2014 to 31 January 2017 using data on registered births in Queensland, available online from the Australian Bureau of Statistics (ABS), as the denominator (ABS, 2021). ABS data indicate that there were a total of 186,652 registered births in Queensland over the 3-year period 2014–2016. Of these, there were 11,564 registered births to Aboriginal and Torres Strait Islander mothers and 175,088 registered births to non-Aboriginal or Torres Strait Islander mothers. Prevalence was provided as a percentage, averaged over the 3-year period examined, and provided with 95% confidence intervals (CIs).
A sub-analysis of women in the cohort who re-presented to police or paramedics was undertaken. A re-presentation was defined as any additional contact with police or paramedics on record, following the index event, while the woman was within the phases of 6 months preconception to 2-years postpartum.
Results
Cohort characteristics
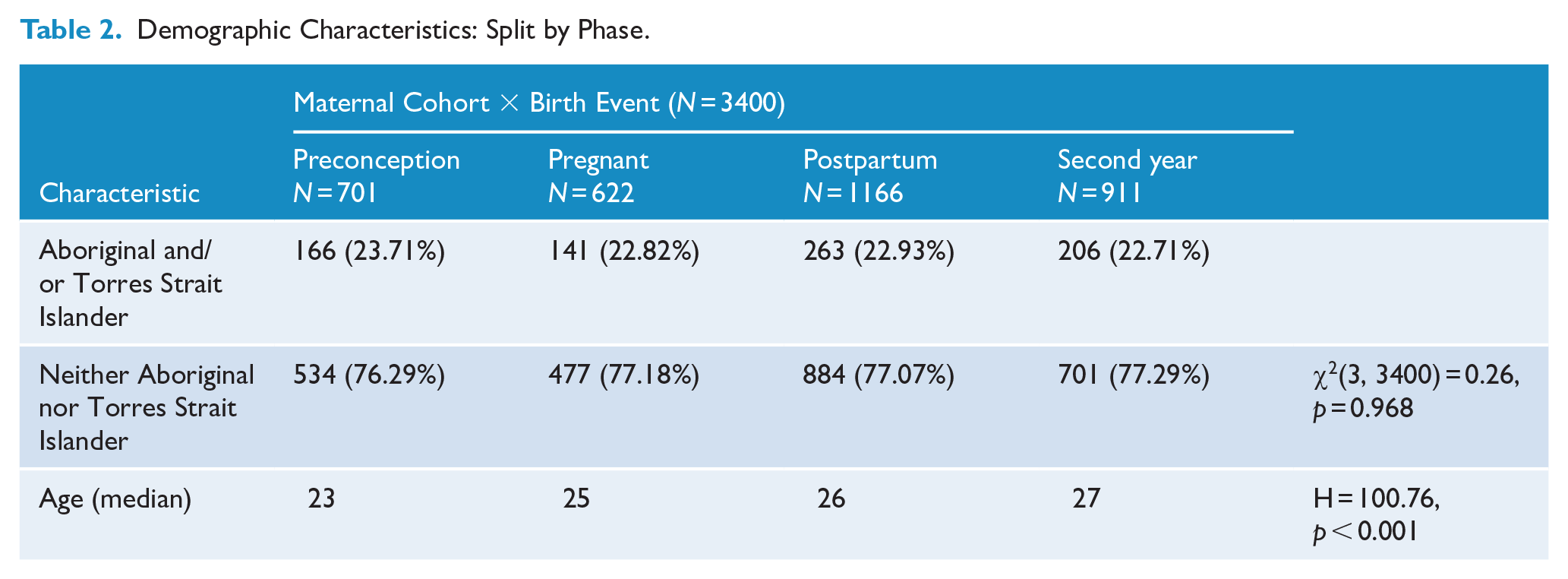
The PiP-Maternal cohort comprised 3020 individuals relating to 3400 birth events. At the index police or paramedic contact, 2460 women were pregnant and up to 2 years postpartum. There was little missing data in relation to key demographic characteristics of this cohort (0.04% missing Age, 0.01% missing Aboriginal and/or Torres Strait Islander status, 0.02% missing residential postcode information). Table 1 provides demographic characteristics of the PiP-Maternal cohort, in comparison to the PiP-Female cohort of the same age range (13–46 years), as well as the PiP-Female cohort from age 5 to 101 years. The median age of the cohort of Aboriginal and/or Torres Strait Islander women in the PiP-Maternal cohort (median age = 23 years: IQR = 13–45) was lower than that of the non-Aboriginal and Torres Strait Islander within this cohort (median age = 26 years of age: IQR = 13–46) (H = 69.75, p < 0.001). Aboriginal and/or Torres Strait Islander women in the PiP-Maternal cohort were also more likely to reside in regional and remote parts of Queensland than non-Aboriginal or Torres Strait Islander women in the PiP-Maternal cohort (35.2% major cities; 11.9% inner regional; 39.9% outer regional; 6.4% remote; and 6.6% very remote, χ2(4,32982) = 1931.9, p < 0.001). Table 2 provides demographic characteristics of the PiP-Maternal cohort, disaggregated by phase.
Demographic Characteristics: Split by Phase.
Prevalence
Overall, the prevalence of suicidality in women who were pregnant and up to 2 years postpartum at the time of an index contact with police or paramedics was 1.32% of registered births (95% CI = [1.27, 1.37]). Prevalence was higher among Aboriginal and/or Torres Strait Islander women, at 4.63% (95% CI = [4.25, 5.03]) of registered births to Aboriginal and Torres Strait Islander mothers, compared to those not of Aboriginal and/or Torres Strait Islander descent, at 1.09% (95% CI = [1.04, 1.13]).
Characteristics of re-presenters
Women in the PiP-Maternal cohort were more likely to re-present to police or paramedics than women in the PiP-Female cohort (Table 1). Table 3 provides demographic characteristics of individuals who re-represented to police or paramedics, in comparison to those who had a single contact only. For those who re-presented, the median days between contacts are provided. Overall, the characteristics differed of individuals who presented once only versus those who re-presented, with those who re-presented being younger (H = 18.85, p < 0.001) and more likely to be Aboriginal and/or Torres Strait Islander, χ2(1, 33,693) = 84.92, p < 0.001.
Characteristics of Women (For All Birth Events) Who Re-Presented in Comparison To Those Who Do Not, Along With Frequency and Timing of Re-Presentations.
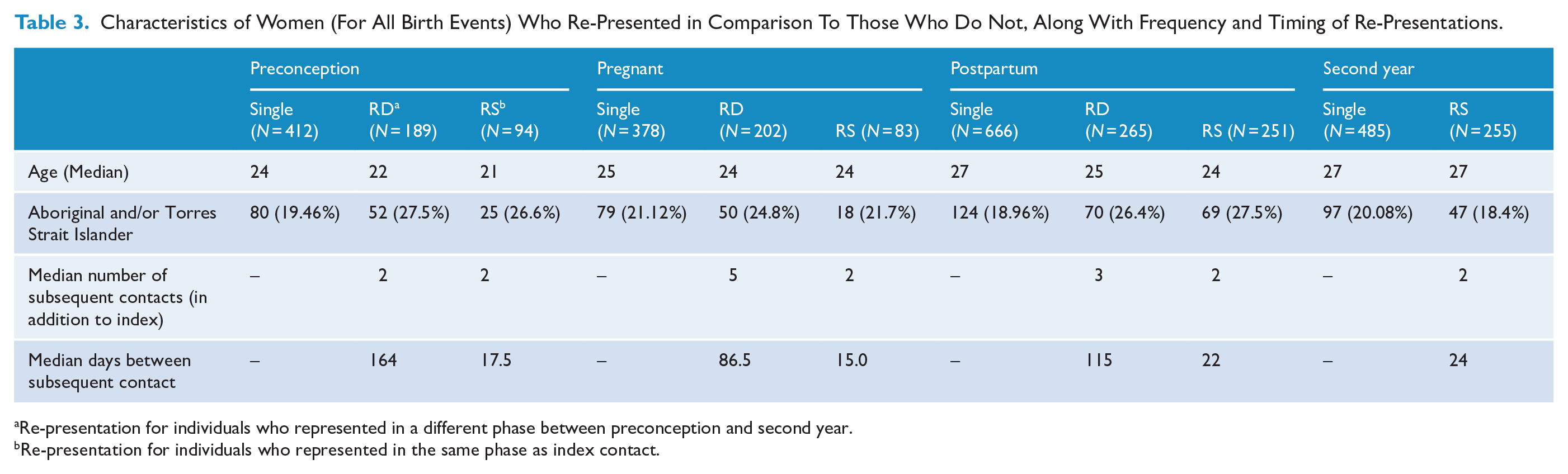
Re-presentation for individuals who represented in a different phase between preconception and second year.
Re-presentation for individuals who represented in the same phase as index contact.
Nature and timing of contacts with services
The majority of calls for service to police or ambulance occurred outside of working hours. Specifically, 68.8% of QAS calls for service to the PiP-Maternal cohort occurred outside of working hours, compared to 69.2% of the remainder of the PiP-Female cohort, χ2(1, 43,465) = 0.40, p = 0.527, and 71.1% of QPS calls for service to the PiP-Maternal cohort occurred outside of working hours compared to 70.1% of the PiP-Female cohort, χ2(1, 6278) = 0.69, p = 0.405. Variability was evident when contacts were disaggregated by Aboriginal and/or Torres Strait background and phase (Supplementary Table 3).
Table 4 shows the dispatch priority assigned to calls for service for the PiP-Maternal cohort, in comparison to the PiP-Female cohort, and shows that there was no statistically significant difference in perceived time criticality (i.e. distribution of dispatch priority) between these cohorts.
Dispatch Priority of Calls for Service.
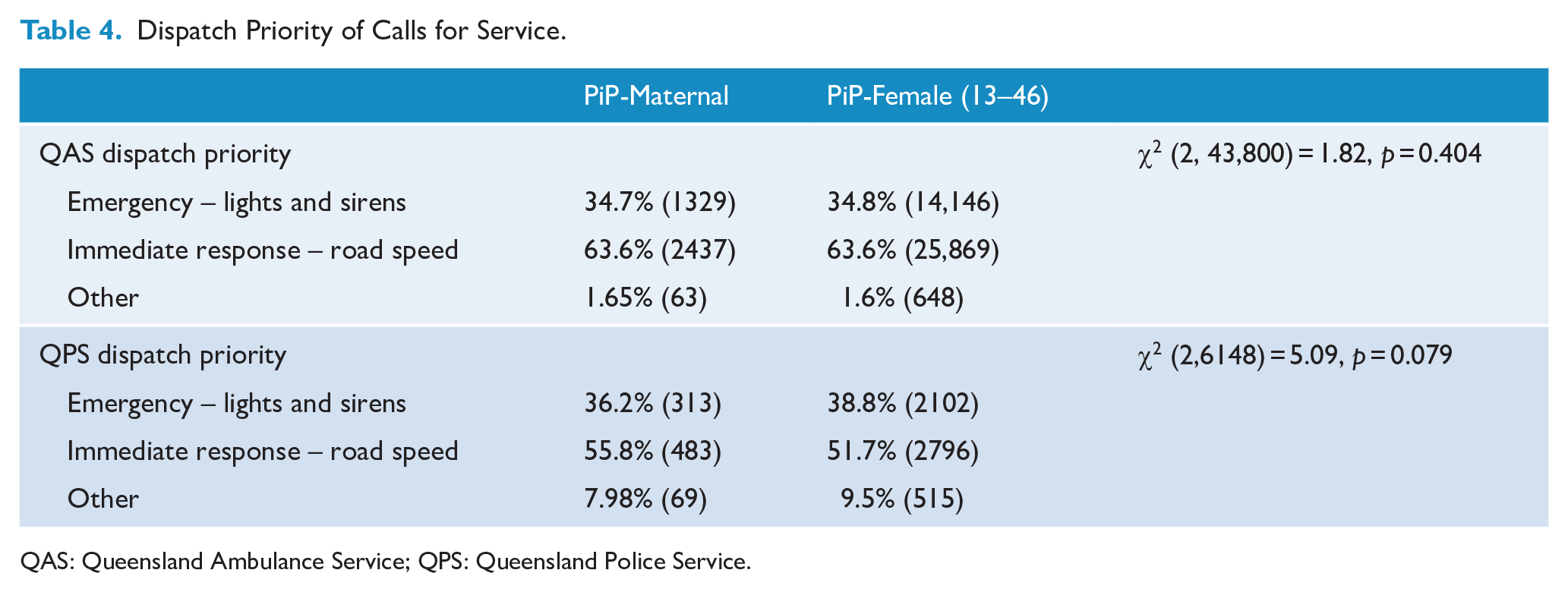
QAS: Queensland Ambulance Service; QPS: Queensland Police Service.
Just over two-thirds (68%) of women in the PiP-Maternal cohort presented to an emergency department within 24 hours of an index police or paramedic contact. This was significantly lower than those in the PiP-Female cohort, where the rate was 79.9%, χ2(1, 24,273) = 245.5, p < 0.001. There was no significant difference in presentations to an emergency department between Aboriginal and/or Torres Strait Islander women within the PiP-Maternal cohort and non-Aboriginal and/or Torres Strait Islander women in this regard, 66.7% versus 68.8% χ2(1, 2994) = 0.94, p = 0.332. Women in the PiP-Maternal cohort were less likely than the PiP-Female cohort to have at least one public mental health service record within 14 days after the index contact, 30.5% versus 34.23%, χ2(1, 24,273) = 33.82, p = < 0.001, while there was no significant difference between Aboriginal and/or Torres Strait Islander women in the PiP-Maternal cohort who had at least one public mental health service record within 14 days of the index contact and non-Aboriginal and/or Torres Strait Islander women, 29.5% versus 29.8%, χ2(1, 2994) = 0.01, p = 0.913.
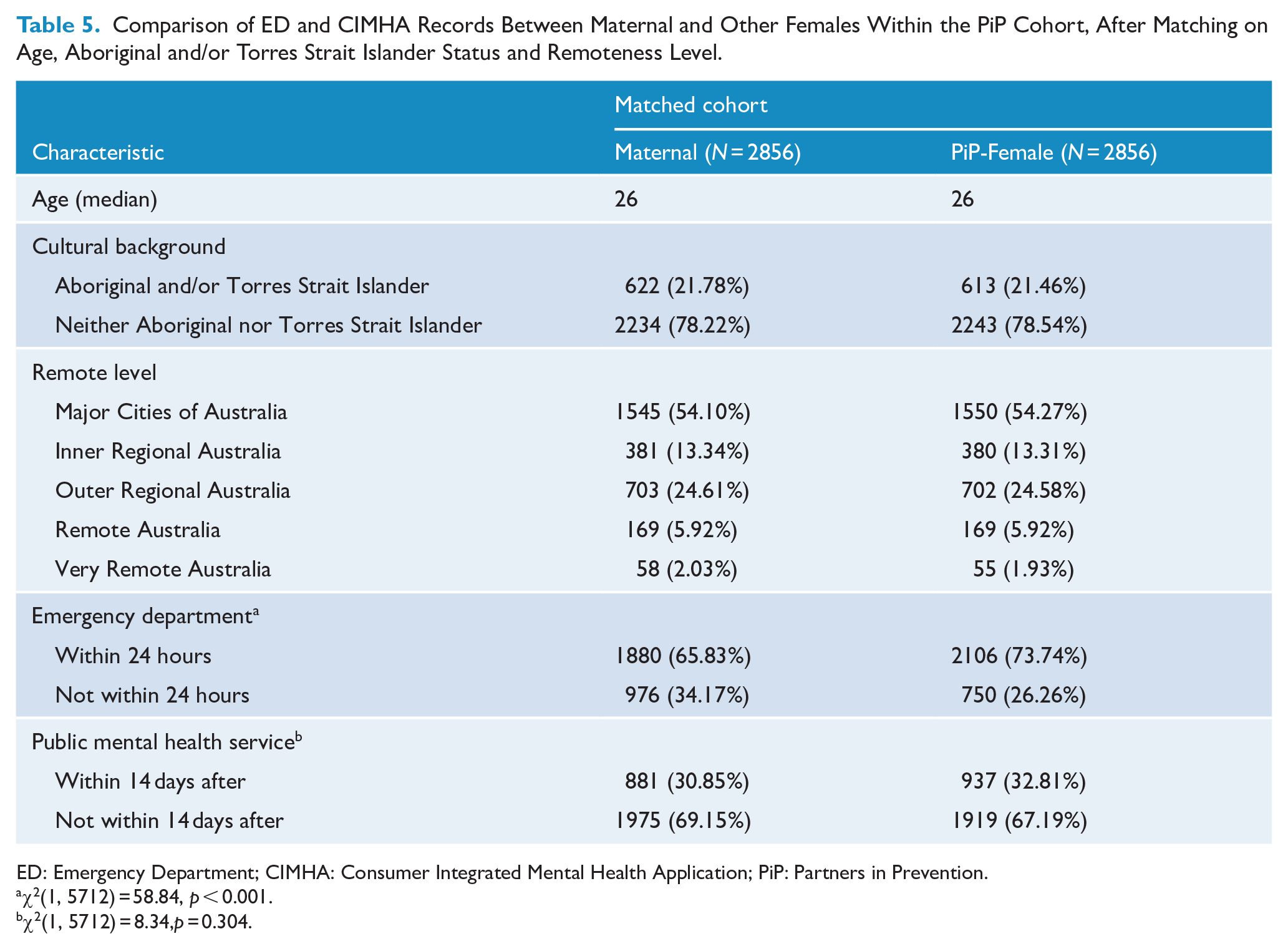
After matching for age, Aboriginal and/or Torres Strait background, and remoteness level, women in the PiP-Maternal cohort were still less likely than those in the PiP-Female cohort to have presented to an emergency department within 24 hours, and the finding remained statistically significant, χ2(1, 5712) = 58.84, p < 0.001. However, the difference in public mental health services records, while still lower for the PiP-Maternal cohort, was no longer statistically significant, χ2(1, 5712) = 8.34, p = 0.304 (Table 5).
Comparison of ED and CIMHA Records Between Maternal and Other Females Within the PiP Cohort, After Matching on Age, Aboriginal and/or Torres Strait Islander Status and Remoteness Level.
ED: Emergency Department; CIMHA: Consumer Integrated Mental Health Application; PiP: Partners in Prevention.
χ2(1, 5712) = 58.84, p < 0.001.
χ2(1, 5712) = 8.34,p = 0.304.
Death
Seventeen women, or 0.56% of the PiP-Maternal cohort, died over the period for which data were available (i.e. the 4-year period from 1 February 2014 to 31 January 2018). Of these, eight were identified as being deaths due to intentional self-harm (47% of all deaths in this cohort). Of the 17 deaths recorded, eight occurred within 12 months of the index event (0.26% of the PiP-Maternal cohort) and less than or equal to five of these were identified as death due to intentional self-harm. Causes of death that were not recorded as being due to intentional self-harm included ‘accidental poisoning’ and ‘undetermined intent’.
Discussion
This paper examines the profile and initial pathways for women between 6 months preconception and 2 years postpartum, compared with other women of a similar age, who had a suicide-related contact with police or paramedics. These phases are associated with a range of different relevant specialities and clinical services; accordingly, the clinical implications will vary. However, we deemed it important to consider these together, including the preconception phase, due to evidence, including clinical experience, that suggests there is continuity throughout pregnancy and postpartum of mental health problems that may have developed and/or manifested during the preconception period (Borschmann et al., 2019).
Over the 3-year period (February 2014–January 2017), prevalence of suicidality among the group of women who were either pregnant or up to 2 years postpartum was 1.32%. This is almost twice as high as previous comparable estimates (Admon et al., 2021). When we disaggregated by Aboriginal and/or Torres Strait Islander background, we found that suicidality among Aboriginal and/or Torres Strait Islander women was approximately four times as high as for non-Aboriginal and/or Torres Strait Islander women.
Overall, the PiP-Maternal cohort were younger, more likely to be of Aboriginal and/or Torres Strait Islander background, and more likely to live outside of a major city than other girls and women who were the subject of a suicide-related call to police or paramedics. Both overall median age of women within the PiP-Maternal cohort and median age within all sub-groups examined were lower than the median age of mothers who had registered births in 2017, which was 31.3 years of age (ABS, 2019). A consistent age profile was noted in women across phases from preconception through to postpartum (i.e. ageing across phases appeared to be consistent with the natural temporal progression of phases). Similarly, there was limited variability with respect to the percentages of women from Aboriginal and/or Torres Strait Islander backgrounds across phases. This consistency suggests similarity in each sub-cohort and, potentially, similarity in underlying reasons for presentations. It also lends support to the possibility that crises experienced during pregnancy and postpartum represent a continuation or exacerbation of issues that were present in the preconception period. Rates of presentation in the preconception period highlight the importance of giving consideration to both culturally responsive sexual and reproductive health as well as mental health needs of young women who experience suicide crisis. This includes addressing contraceptive needs, and the needs of women who experience unplanned pregnancies, as well as ensuring that mental health screening during pregnancy is undertaken and includes consideration and assessment of mental health problems or suicidality or self-harming that occurred prior to pregnancy.
Perceived time criticality of the emergency service attendances, as measured by the priority of dispatch by QAS or QPS, was not significantly different between women in the PiP-Maternal cohort and the PiP-Female cohort. Yet, following the police or ambulance attendance, women in the PiP-Maternal cohort were significantly less likely to present to an emergency department within 24 hours and less likely to have a public mental health services record within 14 days of an index contact. After matching to account for differences in age, Aboriginal and/or Torres Strait Islander background and remoteness, the difference in rates of presentation between the two cohorts to an emergency department remained significant. Possible reasons that explain differences in emergency department presentations include individual factors such as carer responsibilities or having other avenues of health contact related to pregnancy or postpartum. Alternatively, there may be factors related to first responders’ decision-making that influences whether women are transported to an emergency department or not. Further research is needed to identify the reasons for this finding.
After adjusting for differences in age, Aboriginal and/or Torres Strait Islander background and geographic location between women in the PiP-Maternal cohort, compared to women in the PiP-Female cohort, there was no statistically significant difference in the rates of individuals with a public mental health services record created within 14 days following an index police or paramedic contact. However, it is important to interpret this in the context of overall low rates of follow-up. It is difficult to know what optimal rates of mental health services follow-up would be for this group of women, particularly in the context of burgeoning service development to facilitate non-clinical and peer support pathways for individuals who experience mental health or suicide crises. These new pathways include safe havens, promoted in part through recognition that clinical pathways are not always a necessary or optimal caring response for individuals in crisis (Queensland Forensic Mental Health Service, Metro North Hospital and Health Service and Queensland Centre for Mental Health Research, 2020); how these alternative pathways may serve the needs of a mother in crisis with a baby, is as yet not established. However, the measure used for public mental health services contact covered all record types indicating that a public mental health service had become involved, including where a record was created for an individual, but the individual did not participate in a treatment episode. Furthermore, rates of public mental health service involvement within 14 days after an index contact were lower than the rates of dispatch priority classified as ‘emergency’ (i.e. ‘lights and sirens’ response) by police or paramedics and women in the PiP-Maternal cohort were more likely to re-present to first responders than women in the PiP-Female cohort, suggesting ongoing unmet need. Future research could usefully examine the relationship between perceived criticality at dispatch, as determined by first responders, and clinical assessment of risk, as determined by clinicians, as a means to evaluate whether both first responses and subsequent health services pathways are adequate and proportionate to need and risk.
Representations spiked among those whose index contact occurred during pregnancy. Whereas median re-presentations among those who re-presented following an index contact in other phases were stable between 2 and 3 re-presentations, re-presenting women whose index contact was during pregnancy had a median rate of re-presentations of 5. This outlier maybe attributable to chance or an artefact of the way data were segmented; however, it could also be that it indicates that women who re-present during pregnancy are experiencing more serious mental health problems (or an exacerbation), because factors relating to pregnancy are impacting on coping skills, or due to an association between intimate partner violence, which may worsen during this time, and suicidal distress. In support of this possibility, one study from North America found that pregnant women who died by suicide had higher odds of experiencing intimate partner problems than non-pregnant women who died by suicide (Gold et al., 2012). A further notable finding was identified with respect to apparent reductions in contact between Aboriginal and/or Torres Strait Islander women and police during pregnancy and an associated rise in police contact between non-Aboriginal and/or Torres Strait Islander women during this time. It is difficult to know what these findings during pregnancy might mean, and further examination of women who experience suicide crisis during pregnancy is warranted.
Strengths and limitations
This study provides an estimate of prevalence of suicidality among women who were pregnant and up to 2 years postpartum, using routinely collected data from police and paramedics, linked to health services records. A key strength of this study is that it draws from a population-wide linked data set. Consequently, and notwithstanding the limitations noted below, we believe this estimate provides the most accurate estimate of suicidality currently available for Queensland. Limitations to using hospital admissions data (including emergency department records) for identifying suicidality, insofar as they can miss cases, are well known (Sveticic et al., 2020). Among ascertainment challenges is the temporal nature of suicidality which, coupled with what can be long waiting times for emergency assessment and admission, may mean that an individual leaves without being assessed and/or is no longer experiencing a suicidal crisis at the point of assessment. These limitations highlight the significance of data presented here, based on police and paramedic calls for service, which may provide a more accurate means of measuring suicidal crisis. That said, there are reasons to think that the estimate provided here is conservative. First, identification is limited to suicide-related presentations that resulted in a call for service to police or paramedics only. Second, it is known that identification of individuals through police records is subject to undercount (Meurk et al., 2022). Finally, for the purposes of prevalence estimates, an individual was included if they met criteria for being pregnant and up to 2 years postpartum at an index admission. Consequently, some re-presenters who became pregnant at a later stage would be excluded, though the likely impact of this on undercount is low. Finally, the method used for identifying women across phases of preconception and postpartum did not allow for identification of cases relating to miscarriage, termination or foetal or infant death. Additional linkage of the Partners in Prevention study, to include MBS items relating to Termination of Pregnancy, will allow for identification of women who had a surgical termination of pregnancy via a combination of QHAPDC and MBS item data. It is anticipated that prevalence of suicide-related contacts will increase. This is an important area for future research.
While the prevalence estimate provided here is higher than recent figures from North America (Admon et al., 2021), it is lower than estimated prevalence of maternal suicidal ideation before and after pregnancy, as given in a recent systematic review and meta-analysis, which identified a prevalence of suicidal ideation in pregnancy and postpartum of 8% (Xiao et al., 2022). This estimate is very high and, the authors note, higher than prevalence among non-pregnant or postpartum women (Xiao et al., 2022). The review’s authors recommend caution in interpreting findings due to heterogeneity and lack of standardization of tools, with the majority of studies measuring suicidal ideation based on Item-10 of the Edinburgh Postnatal Depression Scale, which may have a high false-positive rate (Xiao et al., 2022). Taken together, these studies highlight the challenges of defining and measuring constructs relating to suicidal behaviours, as well as the limitations of pooling or comparing data at a global level, given a high degree of variability in cultural and regulatory contexts.
Limitations in identification of individuals who had a police contact impacts on prevalence but also on identification of re-presentations to police. Although biased low, the methodology used is unlikely to be subject to any systematic biases that would otherwise impact on interpretation of results (Meurk et al., 2022). The method used to identify individuals by Aboriginal and/or Torres Strait Islander background, involved identifying someone as Aboriginal and/or Torres Strait Islander based on identification in any data set included in the linkage. As such, our study mitigates known limitations relating to identification of individuals’ cultural background to some extent, although our findings are likely to still undercount Aboriginal and/or Torres Strait Islander people.
A final, minor, limitation is that there is a small (1 month) offset of date range between the date range of the numerator (which spans a year, encompassing February–January, the reason relating to the date of a relevant service implementation), and the denominator (which spans a calendar year) with respect to the prevalence estimate presented. The impact of this on estimates is likely to be minimal.
Future directions
To the best of our knowledge, this study is the first to examine suicidality among women across the preconception and postpartum phases, in the context of responses by police and paramedics. The fact that it has uncovered relatively high rates of these contacts highlights significant unmet needs and warrants further research to understand this cohort and enhance responses, including promoting early intervention to mitigate crises early.
Further research could undertake more detailed analysis of prevalence and incidence rates, including time trend analysis over a longer date range; suicide deaths and maternal mortality rate and the associations between suicidality and suicide death; diagnostic correlates, particularly relating to mental health diagnoses; characteristics of presentation to the emergency department; and health services pathways and contacts, including uptake of mental health services referrals and participation in treatment. Research and translational activities need to further examine the interplay of intimate partner violence, mental illness and suicidality, as they affect both women and their children, including initiatives to improve training and awareness in identification of intimate partner violence presenting as suicidality in women. Finally, additional research should seek to explore the lived experience of women who experience suicidality immediately before, during or after pregnancy, to inform optimal caring responses.
Conclusion
The extent of contacts with first responders by women from preconception and up to 2 years postpartum, and in particular the high rates of out of hours contacts with first responders, have significant implications for the provision of health services, including the need for culturally responsive services that meet the needs of Aboriginal and/or Torres Strait Islander women and mothers. Our findings highlight important differences in demographic characteristics but also health pathways following a crisis, between women who have contacts with first responders during or around the time of pregnancy versus women who are not in this phase of life, indicating the importance of developing responses that are tailored to heterogeneous need.
Given the enormous intergenerational impacts of suicidality during and around the time of pregnancy, investment in perinatal mental health and non-clinical crisis support services, including culturally responsive services, is critical. Important unanswered questions remain regarding these women’s services journeys, and further research, including research on lived experience is crucial to inform the future services landscape.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221101517 – Supplemental material for Suicide crises among women and mothers during and around the time of pregnancy: Prevalence and timing of initial contact with first responders and health services
Supplemental material, sj-docx-1-anp-10.1177_00048674221101517 for Suicide crises among women and mothers during and around the time of pregnancy: Prevalence and timing of initial contact with first responders and health services by Carla Meurk, Susan Roberts, Michael Lam, Lisa Wittenhagen, Leonie Callaway, Katherine Moss, Jayne Lucke, Ruth Barker, Elissa Waterson, Catherine Rawlinson, Natasha Malmstrom, Edward Weaver, Elisabeth Hoehn, Emma Bosley, Shelby Watson and Ed Heffernan in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors acknowledge Megan Steele, Emma Bosley and Denise Bunting for contributions to the compilation of the Partners in Prevention–linked data set. The authors also acknowledge the support and assistance from the Queensland Police Service and Queensland Ambulance Service in undertaking this research. The views expressed in this publication are not necessarily those of the Queensland Police Service or Queensland Ambulance Service and any errors of omission or commission are the responsibility of the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Funding for the Partners in Prevention study was provided by the Suicide Prevention Health Taskforce, Queensland Health. C.M. is employed by The Queensland Centre for Mental Health Research, which receives core funding from Queensland Health. E.H. is a recipient of an NHMRC Early Career Fellowship (APP1162565).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.