
Abstract

In 2008, the World Health Organization warned that without action ‘prisons will move closer to becoming twenty-first Century asylums for the mentally ill’ (World Health Organization, 2008). We previously expressed alarm about rising imprisonment in Australia and New Zealand and its impact on people with mental illness and the wider community (Foulds and Monasterio, 2018). Public debate about the role of prisons in society is vital. Imprisonment damages family, and economic and social bonds; harms the mental health of children and adolescents; and leads to long-run increases in both crime and morbidity.
Since its peak at 10,820 in March 2018, New Zealand’s prison population has reduced to 7702 in December 2021. This remarkable 29% decrease lowers New Zealand’s per capita incarceration rate to about 150 per 100,000 – similar to Australia and near the Organisation for Economic Co-operation and Development (OECD) average. The reduction has been even more dramatic for women, whose population has fallen 43% over that period. Here, we discuss how this has been achieved, what can be learned from New Zealand’s experience and what still needs to be done.
Rates of incarceration had been going up in New Zealand since the 1990s, despite little increase in serious crime. This increase accelerated after the Bail Amendment Act 2013, which raised the threshold for bail for many defendants. Similar bail law changes occurred in several Australian jurisdictions in the past decade (Auld and Quilter, 2020). In response to the rapid increase in the prison population, in 2017 the new Labour coalition government announced a goal to lower the prison population by 30% over 15 years. Plans to build a 2000-bed ‘mega-prison’ were scrapped. The government’s objectives were supported by the Chief Science Advisor, who commented publicly on the rising costs of incarceration and the need for justice sector reform (Lambie and Gluckman, 2018).
As shown in Table 1, multiple government agencies were enlisted to help achieve this goal, including Police, the Department of Corrections and the Ministry of Justice. Altered policing practices encouraged frontline Police to resolve incidents without prosecution. The multi-agency ‘High Impact Innovation Programme’ led by the Department of Corrections brought in new bail support services, changes to electronically monitored bail, restructuring of home detention, better support for Police with preparing prosecution files and more help for parole readiness. The Ministry of Justice response, known as Hāpaitia te Oranga Tangata, aimed to improve the experience of people in contact with the justice system. For example, Māori community panels were set up to help Police address low-level offending without involvement of the Courts.
Justice sector reform: New Zealand examples and selected international context.
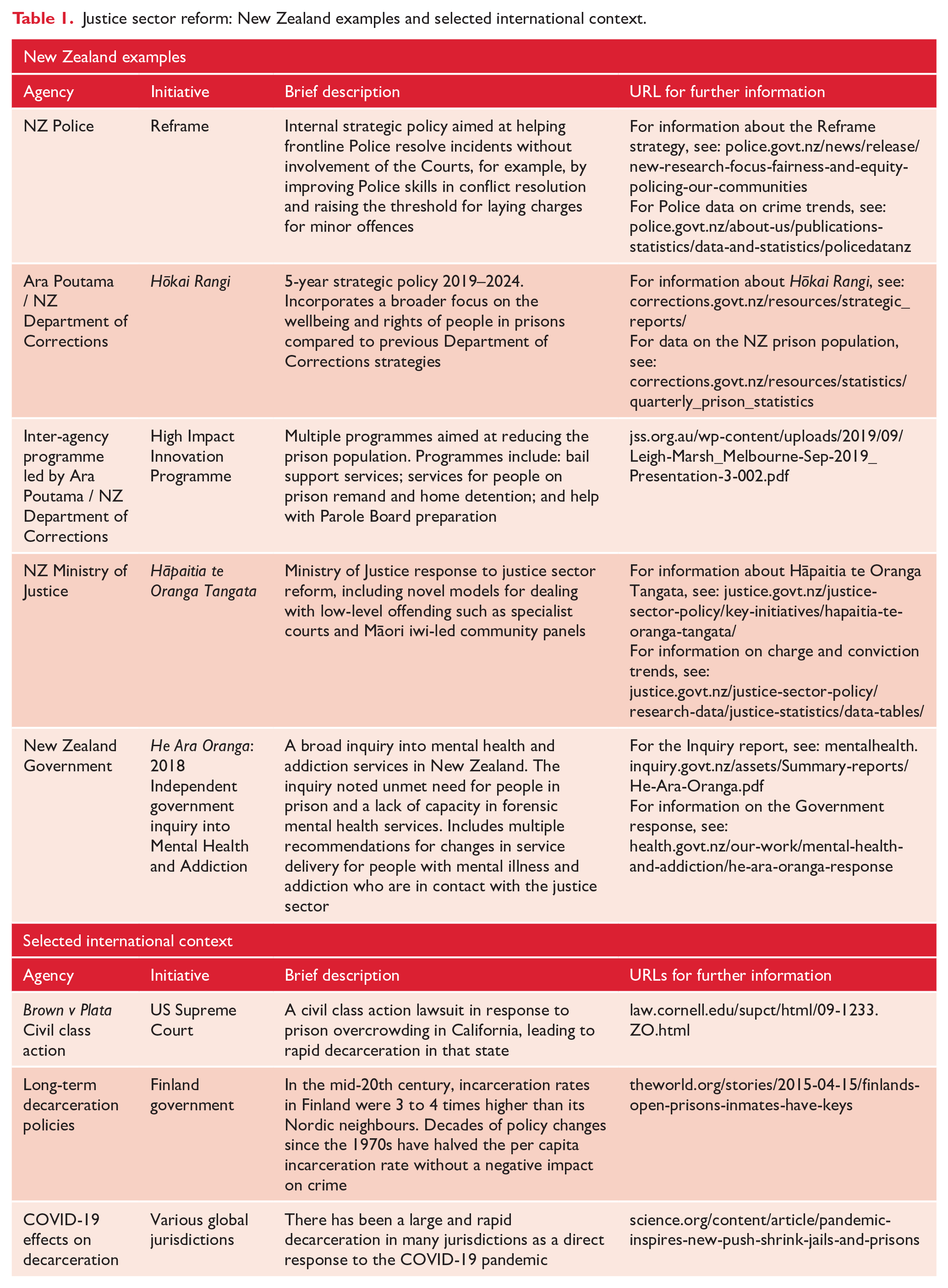
Within the Department of Corrections, a new strategic policy Hōkai Rangi was introduced in 2019. This policy emphasises not just offending outcomes, but also the wellbeing of people in prison. So far so good, as 12-month reimprisonment rates have fallen from 32% to 24% between 2018 and 2021. Nonetheless, more work is needed to show what this has meant for offenders and victims: Ministry of Justice statistics data show convictions for violent offences have remained stable since 2017, but conversely Police data suggest there has been a recent sharp rise in serious violent offences (see URL links in Table 1). This anomaly warrants urgent study.
The COVID-19 pandemic has stimulated innovation in the justice sector globally (see Table 1). It has had complex effects on offending due to environmental factors such as reduced mobility, disruption to illicit drug markets and increased strain on partner relationships. However, while the pandemic has affected the New Zealand justice system, the drop in prison population started well before the pandemic. The relative contribution of the pandemic and justice sector reform to the changing patterns of offending and imprisonment needs investigation, and the answers will likely not be known until well after the pandemic has subsided.
Recent justice reform in New Zealand is not a complete success story. Despite the lower total prison population, the number of remand prisoners in New Zealand has changed little. This partly reflects Court delays, which have worsened during the pandemic. Delayed sentencing increases the length of time defendants spend with stress and uncertainty about their legal matters, and it impedes prison release planning. Second, although targeted decarceration strategies for Māori have resulted in an absolute decrease in the number in custody, Department of Corrections data show there has been less reduction among Māori compared to non-Māori. This suggests justice reforms have unintentionally exacerbated this inequality rather than improving it.
The impact of justice reform on people with serious mental illness has not yet been well studied. While the 2018 New Zealand Government Inquiry into Mental Health and Addiction (He Ara Oranga – see Table 1) noted the lack of forensic mental health services to meet the needs of a growing prison population, media reports suggest these services remain under extreme strain (e.g. see https://www.stuff.co.nz/national/health/125630165/staff-quitting-unsafe-unit-in-one-of-the-countrys-worst-mental-health-hospitals). Furthermore, people with serious mental illness who commit offences will struggle to fully benefit from justice reform unless they can also access stable housing, social services and adequate mental health care in the community. While He Ara Oranga noted the problems people with mental illness face in accessing these resources, there has arguably been little improvement since the Inquiry’s findings were published.
What then can be learned from New Zealand’s recent experience? First, while New Zealand has shown that the prison population can be rapidly lowered, research is urgently needed to show what policies have been most effective and what if any unintended consequences have occurred. This research should consider not only the impact on offending but also health outcomes, economic productivity, service utilisation and costs. As shown in Table 1, the international context can help guide this policy development and research. For example, the effects of decarceration in California since the 2011 US Supreme Court decision in Brown v Plata have been well studied. Similarly, Finland’s prison population has been declining for several decades, with no increase in crime. The COVID-19 pandemic has prompted mass decarceration in many places, and the results of this natural experiment will also be intriguing.
Second, even with targeted programmes, the New Zealand experience suggests justice sector reform may be less effective for some vulnerable groups, particularly Māori. This is concerning in view of the Crown’s obligations under the Treaty of Waitangi. Third, increased selection pressure stemming from a higher threshold to become incarcerated means people in prison have increasingly high and complex health and social needs. Therefore, a smaller prison population does not mean funding for health and social services in prisons or forensic mental health services can be cut. Continuing investment in the prison’s inreach mental health services is vital (McKenna et al., 2021).
COVID-19 has focused public attention on the ethics of restricting individual freedom. This should be a catalyst for public debate on the place of prisons in society, in particular how to achieve equity for people who come in contact with the criminal justice system. This can be done by embedding health outcomes and human rights principles across all government policies. The recent New Zealand experience shows it is possible to rapidly lower the use of prisons as a criminal justice tool, but the health and criminal justice implications of going down this path need to be carefully studied and publicly disseminated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Dr Monasterio holds a paid advisor role with Ara Poutama Aotearoa: Department of Corrections.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Young receives salary and research support from a National Health and Medical Research Council Investigator Grant (GNT1178027).