
Abstract
Objective:
To derive new criteria sets for defining manic and hypomanic episodes (and thus for defining the bipolar I and II disorders), an international Task Force was assembled and termed AREDOC reflecting its role of Assessment, Revision and Evaluation of DSM and other Operational Criteria. This paper reports on the first phase of its deliberations and interim criteria recommendations.
Method:
The first stage of the process consisted of reviewing Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, and recent International Classification of Diseases criteria, identifying their limitations and generating modified criteria sets for further in-depth consideration. Task Force members responded to recommendations for modifying criteria and from these the most problematic issues were identified.
Results:
Principal issues focussed on by Task Force members were how best to differentiate mania and hypomania, how to judge ‘impairment’ (both in and of itself and allowing that functioning may sometimes improve during hypomanic episodes) and concern that rejecting some criteria (e.g. an imposed duration period) might risk false-positive diagnoses of the bipolar disorders.
Conclusion:
This first-stage report summarises the clinical opinions of international experts in the diagnosis and management of the bipolar disorders, allowing readers to contemplate diagnostic parameters that may influence their clinical decisions. The findings meaningfully inform subsequent Task Force stages (involving a further commentary stage followed by an empirical study) that are expected to generate improved symptom criteria for diagnosing the bipolar I and II disorders with greater precision and to clarify whether they differ dimensionally or categorically.
Keywords
Introduction
The status and definition of the bipolar disorders and of mixed states have been issues extensively considered in this journal in recent years (Berk et al., 2005; Fletcher et al., 2018; Ghaemi and Dalley, 2014; Kuiper et al., 2012; Malhi and Berk, 2014; Malhi et al., 2016a, 2016b, 2018), with the valid differentiation of the bipolar subtypes being of particular concern. Such detailed considerations reflect to some degree issues with the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) and recent International Classification of Diseases (ICD) classifications of the bipolar disorders, with both inviting challenges concerning the extent to which they validly distinguish mania and hypomania, and thus the bipolar I (BP I) and bipolar II (BP II) disorders.
As a consequence of such concerns, the AREDOC (Assessment, Revision and Evaluation of DSM and other Operational Criteria) Task Force of international experts on the bipolar disorders was formed to review and iteratively develop a set of revised criteria and, after testing them empirically, finalise their structure. If valid, the revised criteria should facilitate research into whether the bipolar disorders differ dimensionally (i.e. simply by severity) or categorically, and whether they show differential responses to specific medications.
We first overview DSM-5 decision rules and their limitations. A DSM-5 diagnosis of a BP I disorder requires the individual to meet criteria for a current or past manic episode (which may oscillate with hypomanic or major depressive episodes), while a diagnosis of BP II disorder requires meeting criteria for a current or past hypomanic (but never manic) episode and a current or past major depressive episode. The diagnostic criteria for both disorders therefore weight lifetime features. As the distinction between mania and hypomania effectively defines the distinction between BP I and BP II disorders, we first focus here on how manic and hypomanic episodes are defined and differentiated in DSM-5.
DSM-5 Criteria A and B are very similar for manic and hypomanic episodes. Criterion A (a global descriptor) for manic and hypomanic episodes is virtually identical except for a difference in duration (i.e. at least four consecutive days for hypomania and 1 week for mania) but allows any duration for mania (i.e. briefer than 1 week) if the individual is hospitalised, and with an addition of ‘goal-directed’ preceding reference to activity and energy for manic (but not hypomanic) episodes. Specifically, this criterion requires ‘a distinct period of abnormally and persistent elevated, expansive, or irritable mood and abnormally and persistently increased (goal-directed) activity or energy’, and lasting respectively at least four consecutive days as against 1 week for hypomania and mania (or any duration for mania if the patient is hospitalised) … ‘and present most of the day nearly every day’. Thus, Criterion A differences between manic and hypomanic episodes are slight, while Criterion B lists an identical set of symptoms for mania and for hypomania and imposes the same cut-off in symptom numbers, thus effecting no differentiation at all.
Differentiation between manic and hypomanic episodes predominantly arises from the criteria addressing occupational functioning and hospitalisation. Criterion C for mania states that impairment in social or occupational functioning must be ‘marked’, while Criterion E for hypomania states that it is ‘not severe enough’ to ‘cause marked impairment’. Criterion D for a hypomanic episode requires the individual’s unequivocal change in functioning to be observable by others, while there is no equivalent observational criterion for a manic episode. An episode is assigned as manic (and therefore bipolar I status is accorded) if the individual is hospitalised or if there are psychotic features present. While the latter appears categorical (and thus implying that such features are sufficient but not necessary to the definition of mania), it is contradicted by two later specifiers (p. 135) for BP II disorder, which allow individuals to have either mood-congruent or mood-incongruent psychotic features in relation to hypomanic as well as depressive episodes. Thus, there are only two absolute points of differentiation between DSM-5-defined manic and hypomanic episodes: if the patient is hospitalised, and/or if there is marked social or occupational impairment, then the mood episode is designated as manic in type.
Since the early descriptions of manic-depressive illness, its conceptualisation as a psychotic disorder has persisted with few challenges. For hypomania, its history is briefer and its status less clear. Mendel (1881) was one of the first to define the concept as expressed by elevated mood, pressured speech and increased motor activity, and with all such features consistent with mania but to a lesser degree – with this description essentially positioning mania and hypomania dimensionally and according to the level of severity of mood elevations. Early in the 20th century, cyclothymia and hypomania were categorised as ‘milder forms of the manic-depressive psychosis’ (Buzzard et al., 1930), but the concept of hypomania as a ‘milder’ form of bipolar disorder effectively disappeared from the literature until Dunner et al. (1976, 2017) described a (BP II disorder) group, the members of which were ‘in between’ BP I patients and unipolar major depressive disorder patients. Diagnostic and Statistical Manual of Mental Disorders (3rd ed.; DSM-III) subsequently formally introduced the concept of BP II disorder for the first time (albeit titled ‘Atypical Bipolar Disorder’) and briefly described as ‘an episode of illness with some manic features (hypomanic episode) but not of sufficient severity and duration to meet the criteria for a manic episode’. While defining hypomanic episodes (but not a BP II condition), Diagnostic and Statistical Manual of Mental Disorders (3rd ed.; rev.; DSM-III-R) simply stated that its features were similar to those of a manic episode except that delusions were never present during highs and that other symptoms tended to be less severe than for mania.
While multiple authors have continued to position hypomania as a ‘milder’ form of mania, some have argued for the respective presence or absence of psychotic features as defining and differentiating BP I and BP II disorder elevated mood states. In one empirical study (Parker et al., 2016) of 1081 patients clinically diagnosed with a bipolar disorder, a mixture analysis of core symptoms across two sub-populations showed a bimodal distribution (indicative of two separate ‘types’) and with psychotic features overrepresented in those in the group scoring highest in symptom severity. The suggested centrality of psychotic features to mania and their absence in hypomanic states is consistent with several previous studies (e.g. Vieta et al., 1997). Thus, automatic assignment of bipolar disorder patients experiencing psychotic features with an elevated mood to receive a DSM-5 diagnosis of mania is likely to be valid (although, as noted, this decision is confounded by DSM-5 specifiers allowing psychotic features to be present in hypomania).
The ‘absolute’ DSM-5 criterion whereby hospitalisation generates automatic assignment to manic status invites criticism on the grounds of reality and logic. Specifically, while hospitalisation may be a marker of severity, there are many regions in the world lacking psychiatric hospitals, while thresholds for hospital admission vary across treatment settings based on issues of access, availability and other resources. In terms of logic, we are unaware of any other psychiatric (or medical) condition that includes hospital admission as a diagnostic criterion. It also fails to capture the reality that some bipolar patients with hypomanic episodes may still require admission to protect their reputation, prevent risk-taking behaviour or manage their hypomanic state. For instance, in an Australian study (Parker and Graham, 2017) examining admissions to psychiatric hospitals from 2000 until 2014 (inclusive), there were 2882 admissions for those with ICD-10-diagnosed mania and 5373 for those with ICD-10-diagnosed hypomania. It therefore appears that hospitalisation is not restricted to those experiencing manic (as opposed to hypomanic) episodes unless hospitalisation becomes the defining criterion. Thus, if mania is to be distinguished from hypomania by severity as a criterion (which would seem logical), then it would be preferable to avoid using hospitalisation as a proxy for severity and instead define levels of severity for the two conditions more directly.
The other absolute DSM-5 criterion for assignment of mania as against hypomanic status (i.e. functional impairment) also invites criticism. As noted earlier, the definitions require ‘marked impairment’ for mania, while for hypomania the episode is ‘not severe enough to cause marked impairment’. Such differentiation presents two issues: First, how can the level of impairment in social and occupational functioning be validly judged when it relies on subjective judgement by the patient and/or assessing clinician in the absence of clearly established thresholds? Second, this criterion fails to recognise that some individuals actually report (and demonstrate) improved social and occupational functioning and an increase in creativity when hypomanic. Thus, if an individual experiencing a hypo/manic episode has not been hospitalised, the only differentiating criterion to assign manic versus hypomanic (and thus BP I or BP II disorder) status is the degree of impairment, and with assessment of that criterion being limited by its intrinsic subjectivity and its variable presence.
Turning to duration criteria, DSM-III imposed a minimum duration of 1 week for a manic episode. However, lacking any formal BP II disorder, the manual effectively assigned an ‘atypical bipolar disorder’ diagnosis to those who experienced a hypomanic episode which was not of ‘sufficient severity and duration to meet the criteria for a manic episode’ (p. 223), and thus did not impose any minimum duration for hypomanic episodes. DSM-III-R did not include a duration criterion for mania but stated in the general text (p. 216) that episodes ‘usually last from a few days to months’. Thus, while DSM-III-R allowed brief durations for manic episodes, it did not position duration as integral to the definition of hypomania. Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) imposed the minimum duration periods for mania and hypomania (i.e. 7 and 4 days, respectively, unless those with mania are hospitalised) preserved in DSM-5. Such minimum periods have been challenged in relation to their validity. In a Zurich community study of those identified with BP II disorder, Angst (1998) compared subjects meeting Diagnostic and Statistical Manual of Mental Disorders (DSM) hypomania duration of four or more days with those having episodes lasting 1–3 days and found similar symptom profiles across 15 hypo/manic items. Several subsequent studies (e.g. Bauer et al., 2011; Benazzi and Akiskal, 2006; Judd et al., 2003; Parker et al., 2014; Tully and Parker, 2007) demonstrated that hypomanic states (in those diagnosed with BP II disorder) lasting less than 4 days did not differ phenotypically from those lasting four or more days. In another study of 49 clinically diagnosed BP I patients and 52 BP II patients (Parker et al., 2006), it was established that, in relation to their longest ever hypo/manic episode, 45.8% of the BP I patients had never had an episode lasting as long as a week and 43.7% of the BP II patients had never had an episode lasting longer than 2 days. Such studies are often discounted on the basis that, as subjects did not meet DSM duration criteria, their alternate defining criteria might also be invalid. However, their data (generally respecting DSM criteria other than duration) do suggest that current DSM duration criteria are problematic because, if an individual experiences a stereotypic hypo/manic episode that lasts less than the DSM-5-mandated duration (and which would appear to occur commonly), they cannot be diagnosed with either a BP I or a BP II condition and may hence be inappropriately diagnosed and treated.
Unlike in the current DSM, ICD-10’s criterion A did differ in defining hypomania and mania dimensionally – with mania having a higher level of severity, but also with manic episodes sub-classified as with or without psychotic features. Thus, psychotic features did assign a manic diagnosis, while the absence of psychotic features was a criterion for hypomania but also allowed for mania. Hypomania was defined as ‘a lesser degree of mania’ and lasting ‘at least several days’, while episodes of mania ‘should last for at least 1 week’. ICD-10’s symptom sets did differ slightly for hypomania and for mania with or without psychosis, while hospitalisation did not automatically assign manic status and there was no impairment criterion. ‘Bipolar affective disorder’ was subtyped on the basis of the current episode being hypomanic, manic without psychotic features, manic with psychotic features, mild or moderate depression, severe depression without psychotic features, severe depression with psychotic features or ‘mixed’. Then, among the category of ‘other bipolar affective disorders’, BP II disorder was listed (without any description or criteria) and without any preceding reference to any BP I disorder.
ICD-11 criteria allow several expressions of BP I disorder (e.g. current episode manic with or without psychotic features or evidencing hypomanic features) and allow that it may be diagnosed after a single manic or mixed episode but usually oscillates with depressive episodes. A manic episode is differentiated from a hypomanic episode by a longer duration of seven versus ‘several’ days, with psychotic features allowable in manic but not hypomanic states, and with the former described as an ‘extreme mood state’ and the latter as a ‘persistent mood state’, which are seemingly unaligned parameters. Each condition is described by sets of representative features with the manic ones being more severe than the ‘mild’ elevations of mood or increased irritability and activity integral to hypomanic states. ICD-11 defines BP II disorder as requiring one or more hypomanic episode – involving a number of symptoms lasting for at least ‘several days’, and not being severe enough ‘to cause marked impairment’ or to necessitate hospitalisation – and at least one depressive episode. The manual also lists a number of patterns and features associated with depressive episodes for both the BP I and BP II disorders (e.g. psychotic symptoms or not, being of mild versus severe versus unspecified severity, as well as mixed states with or without psychotic symptoms).
The ICD-11 system is in contrast with DSM-5 in building depressive features into the primary definition of the bipolar disorders, providing sets of representative symptoms rather than criteria sets and imposing no cut-offs in symptom numbers. Its most distinctive change from ICD-10 is the provision of a more detailed definition of BP II disorder as a separate condition and in providing criteria for its diagnosis. Some of its decision rules (e.g. minimum duration criteria and use of ‘marked impairment’ as a point of diagnostic distinction) have been critiqued in relation to the earlier overview of DSM-5.
We therefore judge that there are limitations to the current DSM and ICD criteria for differentiating mania from hypomania (and therefore BP I disorder from BP II disorder). Such concerns led to establishing the AREDOC Task Force with the objective of deriving a new set of criteria for better distinguishing manic and hypomanic episodes (and thus the BP I and BP II disorders) – whether dimensionally or categorically – that would address the issues overviewed here. This paper reports on the first stage of the revisional task, which sought to build on the DSM-5 template.
Method
An invitation and questionnaire were sent to an international group of mental health professionals recognised as having clinical and/or research expertise in the bipolar disorders. The questionnaire (which sought to weight the DSM-5 template) included current DSM criteria for mania and hypomania followed by amendments to those criteria as proposed by the first author (G.P.). The respondents were asked if they agreed with the proposed amendments and to offer any other modifications based on their clinical experience and research expertise. Amendments were generated in response to the questionnaire and in comments provided by members in preparing this paper.
Results
Of the 123 professionals invited, 71 (57.7%) accepted and 63 (51.2%) responded to the first questionnaire, thus making up a Task Force of 64 individuals from 14 countries spanning five continents.
The DSM-5 Criterion A was modified with the proposed questionnaire definition for both hypomanic and manic comprising: A distinct period of abnormal and persistently elevated, expansive, or irritable mood, with the individual feeling energised and ‘wired’, and which is perceived as an ‘overshoot’ and not simply a state of happiness, and generally oscillating with periods of depression.
The new definition builds on the DSM-5 criterion, captures the bipolar nature of the underlying condition (i.e. hypo/manic episodes oscillate with depressive periods), allows that individuals may have hypo/manic episodes before any depressive ones, seeks to address concerns about false-positive diagnoses of bipolar disorder but imposes no duration criterion (with this issue considered later).
In response, 16 Task Force members were in total agreement with the proposed definition and 19 were against including any reference to such states oscillating with periods of depression, with most suggesting that reference to depression would be better included in a general background description of the bipolar disorders and their longitudinal course. The reference to depression was therefore removed. Eight were against any reference to ‘happiness’, and this judgement was respected as superior wordings were offered by several members. Eight were against the ‘wired’ descriptor (either judging it as being too colloquial, not relevant across differing cultures or as redundant in light of the ‘energised’ descriptor). As seven were in favour of ‘wired’, with one noting that it went to the ‘heart’ of a hypo/manic state and one that it was important in capturing the sufferer’s own subjective experience rather than the judgement of a clinician rater, it was retained for later empirical testing.
A few respondents offered comments about the ‘irritable’ descriptor. Three favoured its rejection, judging that it is not associated with hypo/mania, while three argued for its retention in light of some bipolar patients only having irritable moods and never being elated. As a number of studies (see Graham et al., 2015) have demonstrated an ‘irritable’ or ‘irritable-racing thoughts’ factor as well as a contrasting ‘euphoric’ and ‘dysphoric’ hypo/manic phenotype, ‘irritable’ was retained but enriched with the suggested descriptor ‘quick-tempered’ being added. Seven were against ‘overshoot’, viewing it as either colloquial or redundant. One favoured an ‘overshoot’ synonym such as ‘unambiguous departure from one’s normal or usual state’. It was removed to respect the majority vote. Only two voted against use of the word ‘abnormal’ on the basis of its pejorative tone, with one of those favouring ‘unusual’ as an alternative. In other sections of the questionnaire, several members emphasised hypo/manic states as being ‘abnormal’, in the sense that both are (by definition) psychopathological and also distinct from ‘normal happiness-like’ states. Thus, ‘abnormal’ was retained. Several were against ‘perceived’, noting that the individual may not have insight, and thus this word was removed. In relation to whether ‘impairment’ should be retained or deleted, more argued for reframing this component as a ‘functioning’ construct. So ‘change in functioning’ was substituted.
Thus, the new Criterion A for hypo/mania for later evaluation was: A distinct period of either an abnormally elevated and expansive mood, or an irritable and quick-tempered mood, characterised by increased activity and cognition such that the individual feels unusually energised, ‘hyper’ or ‘wired’. Such changes are perceived at the time or on later reflection as excessive and an unambiguous change in functioning from the individual’s usual state.
DSM-5 Criterion B lists seven symptoms although several might be better viewed as broad constructs (e.g. increase in goal-directed activity). Task Force members were given a set of narrow symptoms and broad symptom constructs (including all DSM-5 criteria) for editorial revision as listed in Table 1. Two expressed concerns about non-specificity of some items, one argued for the need to have items that did not detect personality disorders, one recommended breaking down the at-risk activities into separate items, while several expressed the opposite concern of items having multiple and possibly overlapping constructs rather than a single one and the risk of moving into minutiae territory, and therefore some argued for a ‘lean and mean’ list. Some were concerned about the inclusion of delusions and hallucinations.
Symptoms and symptom constructs proposed to the Task Force and the resulting symptom set provided by Task Force members in response to the questionnaire.
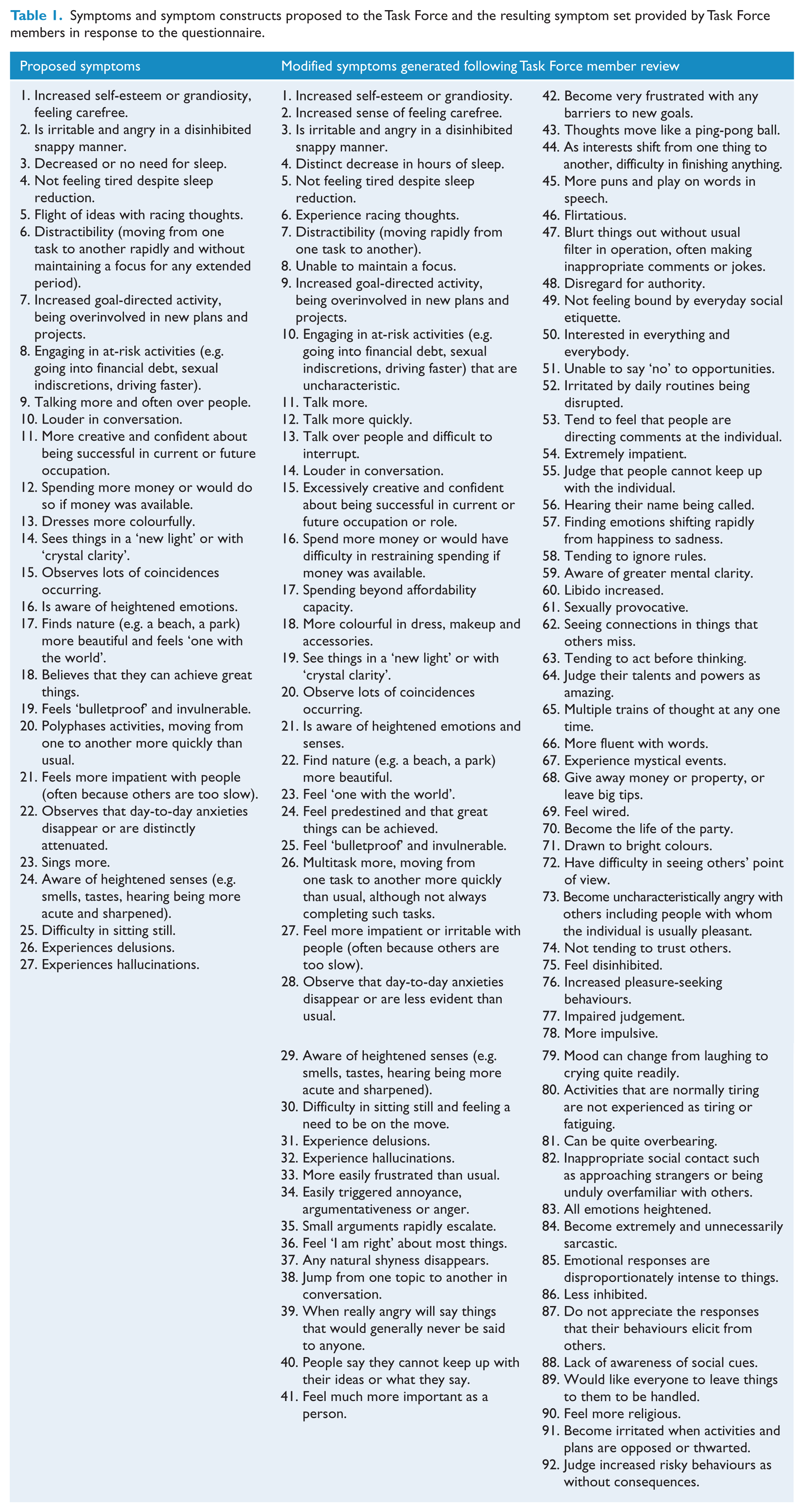
Members were also invited to contribute items that they had observed as capturing nuances of hypo/manic states, whether phenotypically ‘happy’ or ‘snappy’. Based on such feedback the original set of 27 items was reworked to remove overlapping items as well as accommodate editorial suggestions, and so generated the new list of 92 items (listed in Table 1). The concern about having too many items will be addressed at the empirical stage when we will have bipolar (and unipolar) subjects complete a self-report list of all candidate items. This will allow frequency estimates for all items to be calculated and their differential profile across BP I disorder, BP II disorder and unipolar states quantified, and those deleted if demonstrating low prevalence or differentiation rates – although we acknowledge that ‘snappy’ bipolar states will generate low prevalence estimates in the whole sample (reflecting the lower prevalence of the irritable phenotype). Highly correlated items will be consolidated into ‘construct’ items, and optimal cut-off numbers needed for defining hypomania and mania derived. Thus, rather than the current DSM-5 model of having the same symptom criterion sets and same cut-off criteria for hypomania and mania, we anticipate analyses generating a set of shared obligatory symptoms for both hypomania and mania as well as facultative ones that differ (categorically or dimensionally) across the bipolar subtypes, while the cut-off criteria numbers for hypomania and mania are likely to differ.
DSM-5’s Criterion C for hypomania alone (‘The episode is associated with an unequivocal change in functioning that is uncharacteristic of the individual when not symptomatic’) was modified to include an observational component which incorporated DSM-5’s Criterion D for hypomania (that the mood disturbance and change in functioning were ‘observable by others’) but with the criterion for both hypomania and mania allowing that such changes might only be observed by the individual and not necessarily by others. In response, 29 members supported this definition. Two noted that some individuals actually function better in such states (an issue addressed earlier and in more detail shortly), and 16 expressed concern about the risk of allowing subjectively experienced states alone to be accorded hypo/manic status and that true hypo/manic states should be observable by others. However, as a number of hypomanic individuals providing clear-cut symptoms have close relatives who fail to observe and confirm symptoms of hypomania, requiring such states to be observable by others would limit the diagnosis to only those individuals who have witnesses who actually observe such episodes. Thus, the allowance of observation of hypo/mania by the individual was retained and the new criterion for manic as well as for hypomanic states for later consideration became: ‘The episode is associated with an unequivocal change in functioning (as judged by the individual and/or observers) that is uncharacteristic of the individual when not symptomatic’.
As noted, DSM-5’s Criterion C for a manic episode includes a ‘marked impairment’ requirement, while DSM-5’s Criterion E for a hypomanic episode requires that the ‘episode is not severe enough to cause marked impairment in social or occupational functioning’. It was put to Task Force members that there should be no impairment requirement in light of (a) impairment being hard to judge, (b) the presence or absence of ‘marked’ (versus ‘less marked’) impairment also being hard to judge and (c) in many hypomanic states and occasionally in manic states, social or occupational functioning can be enhanced rather than compromised. The latter often self-reported observation has been supported empirically. For instance, both Jamison et al. (1980) and Judd et al. (2005) found that a sub-set of patients reported improved functioning while hypomanic, and with the second study finding improved social functioning in the BP II disorder but not the BP I disorder sub-set, a finding with distinct implications.
In response, 34 argued for retaining an impaired functioning criterion (as against 17 for its deletion), principally judging that its removal could lead to overdiagnosis. Many felt that it was central to defining mania, while for hypomania several also acknowledged that functioning might be unaffected or improved (and thus should be used to so distinguish the two conditions). The observation that functioning might actually be improved caused several to then suggest that it was then hard to define such hypomanic states as ‘abnormal’. Of those voting for the preservation of an impaired functioning criterion, several noted difficulties in its operationalising, with suggestions being that it should be more detailed than in DSM-5, and probably weighted by severity. Thus, the majority vote arguing for its inclusion was respected and proposed definitions will be noted after considering the issue of ‘hospitalisation’.
It was proposed that Criterion C (hospitalisation automatically assigning elevated individuals to manic status) be deleted, principally as no other condition is defined by hospital status, but also respecting earlier data that hospitalisation does not appear limited to those with manic states. A total of 42 members were in favour of such deletion, largely on the grounds of it being arbitrary as well as subject to local health service practices, insurance and other external factors. By contrast, 16 were in favour of maintaining the hospitalisation criterion, generally viewing it as a proxy for severe impairment or, for some, that it allowed mania to be diagnosed. Based on such feedback, the recommendation to the Task Force was to delete it as an absolute criterion (as employed in DSM-5) but use it as an exemplar of severe impairment.
Returning to impairment, new proposed definitions for mania and hypomania were derived. First, for mania: The mood disturbance is associated with marked impairment in functioning, which may be evidenced by the individual not being able to work or not being able to interact normally with family and friends, and with such a level of impairment that containment strategies including hospitalisation are commonly required.
Second, for hypomania: The mood disturbance may be associated with some level of impairment at work and in social functioning, and even need for containment strategies, but generally does not prevent the individual from being able to work or interact normally with family and friends. Some patients may even report an improvement in functioning in that they are genuinely more productive or creative at work.
These definitions position mania as distinctly more impairing than hypomania, while an improvement in functioning is conceded as possible for some of those with hypomania – as evidenced in the empirical study by Judd et al. (2005) – rather than viewing it as an invariably impairing condition.
In light of concerns about the DSM-5 duration criteria for mania and hypomania being too restrictive (in disallowing a bipolar diagnosis in individuals who meet phenotypic criteria but who have only brief episodes), Task Force members were asked whether the duration criteria should be deleted or preserved and if, in favour of the latter, their recommended minimum durations to be imposed were sought. This issue generated greater consideration than all other diagnostic nuances. Formally, 49 were in favour of imposing duration criteria, most commonly on the basis that deleting a duration criterion would risk overdiagnosis of the bipolar disorders in those with normative mood swings or those with personality-based emotional dysregulation and thus lead to the bipolar disorders being inappropriately diagnosed. Seven were in favour of their deletion, arguing that meeting the phenotypic picture should be sufficient. Comments focussed on the difficulty in deciding whether to guard against false-positive or false-negative scenarios, while one offered an analogy – that assigning a minimum period was akin to ‘assigning a minimum duration to a hurricane’. For those 36 nominating finite periods, minimum duration recommendations ranged from several hours to 7 days. The modal recommended minimum duration was 2 days for both mania and hypomania. Many argued that clarification of this criterion should be resolved by an empirical study, as will occur.
Discussion
The definitions and differentiation of the bipolar disorders remain contentious issues in the field of psychiatry (e.g. Fletcher et al., 2018; Malhi and Berk, 2014; Malhi et al., 2016b, 2018), with these issues being exacerbated by the many limitations of the DSM and the ICD criteria for classifying the bipolar disorders, as detailed in the ‘Introduction’. The AREDOC Task Force was formed to obtain points of commonality held by those with clinical and research expertise in assessing and managing the bipolar disorders so that revised criteria could be generated.
The aim of this paper is to expose readers to limitations of DSM-5 and recent ICD definitions, to describe potential corrective strategies that respect the DSM-5 template and to note the degree of consensus by Task Force members in relation to the first-stage revision proposal. We detail a set of modified criteria which will be considered and revised by members at the second stage of the project. Once relative consensus has been achieved, an empirical study will be undertaken to assess the validity of the generated criteria involving several hundred putatively diagnosed patients with BP I and BP II disorders as well as a group of unipolar depressed subjects. Thus, while those with a bipolar disorder were not consulted in this first stage, their views and ratings will be focussed on at the third stage and shape many of the final decisions. In addition to the ‘top-down’ analytic approach, a ‘bottom-up’ approach will be employed and, with diagnostic subtype being ignored, data from all bipolar patients will be analysed (principally by use of a mixture analysis) to determine if manic and hypomanic and thus BP I and BP II states can be differentiated categorically rather than dimensionally and, if so, the variables that generate such differentiation. Analyses are also likely to be iterative in varying the dependent and independent variables to sharpen the diagnostic criteria progressively.
Study patients will complete a structured questionnaire when euthymic that will allow testing of all our criteria (and their acceptability and judged validity by the patients). Defining constructs (and contributing items) will be derived for both ‘happy’ and ‘snappy’ hypo/manic states and ones that differentiate mania from hypomania identified, and cut-off scores generated for both the BP I and BP II conditions. Some criteria (especially imposition of minimum duration criteria) will be resolved, in part, by analysis of the generated data. If, however, a significant percentage of patients do report episodes never lasting more than a day, Task Force members will be required to determine how best to address the risk of false-positive diagnoses, an issue articulated by many of them with respect to several of the parameters.
Overall, by the end of this initiative, we hope to have developed and empirically derived criteria for defining mania and hypomania that capture quintessential clinical features as well as discriminate between manic and hypomanic states. Such criteria will consequently assist in distinguishing BP I and BP II states and determining whether this distinction is categorical or dimensional, so facilitating future research pursuing differential causes and treatments for the bipolar disorders. In exposing the reader to the first phase of this ambitious international project, we aimed to provide a persuasive argument for the need to modify current DSM-5 and ICD criteria, and capture the views of those with expertise in the bipolar disorders on how best to define and classify the two conditions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: M.B. was supported by a National Health and Medical Research Council (NHMRC) Senior Principal Research Fellowship (#1059660). G.P. was supported by an NHMRC Program Grant (#1037196). G.S.M. was supported by an NHMRC Program Grant (#1073041).