
Abstract
Objective:
To examine and describe telehealth use and attitudes among mental health professionals in Australia and New Zealand during the initial stages of the COVID-19 pandemic.
Methods:
Participants completed a brief online survey between May and July 2020. Participants were recruited via peak and professional organisations and through psychology-focused social media groups and networks. The survey examined frequency of telehealth use, reasons for non-use, telehealth modalities, prior use, attitudes towards use, plans for future use, and training, information or resource needs.
Results:
A total of 528 professionals (85.2% female) participated in the survey, of which 98.9% reported using telehealth and 32.2% reported using telehealth exclusively. Respondents were less likely to use telehealth if they worked with clients experiencing complex issues (e.g. trauma), had more hours of weekly client contact, had a choice about whether to use telehealth or felt less positive about using technology. Respondents were more likely to hold positive views towards telehealth if they were female, had used online programmes with clients previously, were frequent telehealth users and were comfortable using technology. Participants expressed mixed views on client safety and the impact of telehealth on therapeutic process and effectiveness.
Conclusion:
Telehealth has a clear and ongoing role within mental healthcare and there is a need for strong guidance for professionals on how to manage client risk, privacy, security and adapt therapy for delivery via telehealth. In particular, there is a need for individual-, organisational-, professional- and policy-level responses to ensure that telehealth remains a viable and effective healthcare medium into the future.
Introduction
The first community-wide lockdowns of the COVID-19 pandemic in Australia and New Zealand necessitated a rapid change in the delivery of mental health and other health services. To continue providing essential care, mental health professionals were required to transition to using telehealth, which involves the delivery of health services via telecommunication technologies, such as video-conferencing and telephone (International Organisation for Standardisation, 2004). This transition to telehealth was unprecedented and likely presented challenges for many mental health professionals.
Like other technology-based interventions, telehealth offers several advantages. Telehealth services may overcome barriers to care associated with accessibility and travel, availability of services and stigma (Mohr et al., 2013). For these reasons, it has been particularly useful for people living in rural areas and others who have difficulty accessing face-to-face services (Moffatt and Eley, 2010). Importantly, studies have demonstrated equivalence between face-to-face and telehealth therapies in terms of feasibility, acceptability and effectiveness across a range of formats (e.g. individual, group, family), therapeutic approaches, client populations and presenting problems (Backhaus et al., 2012; Irvine et al., 2020; Jenkins-Guarnieri et al., 2015; Norwood et al., 2018; Simpson and Reid, 2014b).
However, routine uptake of telehealth among mental health professionals prior to COVID-19 was low (Richardson and Simpson, 2015; Simpson and Reid, 2014a). A number of barriers impeded the use of telehealth, including lack of clinician training, concern about the safety and effectiveness of telehealth, the impact of telehealth on therapeutic processes, inadequate or complicated funding systems for provision of services, lack of digital infrastructure and lack of knowledge regarding the technological, ethical and legal requirements for engaging in telehealth practice (Connolly et al., 2020; Ganapathy et al., 2021; Knott et al., 2020; Richardson and Simpson, 2015; Tuerk et al., 2019; Vis et al., 2018).
According to the World Health Organization, 93% of countries experienced disruptions to mental health service provision as a result of the COVID-19 pandemic, with the greatest disruptions affecting community-based services (World Health Organization, 2020). Crises such as pandemics highlight the need for mental health services to be adaptable and readily deployable to populations in need. Accordingly, uptake of telehealth in mental health services worldwide rose sharply in the initial phases of the pandemic (Corruble, 2020; Fagiolini et al., 2020; Guinart et al., 2021; Pierce et al., 2021). In Australia, changes to the Medicare Benefits Schedule (MBS) were made to allow temporary telehealth access for all citizens and permanent residents (Australian Government Department of Health, 2021). Prior to the pandemic, telehealth was only subsidised for people living in rural and remote areas in Australia (Australian Government Department of Health, 2017). In New Zealand, telehealth was government-supported prior to the COVID-19 pandemic (Ministry of Health, 2017).
There is much to be gained from knowledge of how mental health professionals transitioned to telehealth during the initial stages of the COVID-19 pandemic. Safe and effective use of telehealth relies on having a good understanding of the current state of practice and the factors that enable or impede good practice. Moreover, clinicians serve as gatekeepers for the implementation and sustainability of telehealth services, and the attitudes they hold towards telehealth may have important implications for telehealth acceptability and adoption among service users (Cowan et al., 2019).
However, limited research has examined telehealth use by mental health professionals during the COVID-19 pandemic. Surveys of professionals have been conducted in the United States (Guinart et al., 2021), but only two studies have examined telehealth use among mental health professionals in Australia. One was conducted with youth mental health clinicians and service users (Nicholas et al., 2021), and the other was a qualitative study of clinicians working within a community-managed provider of psychosocial interventions (Venville et al., 2021). To date, no published studies have examined telehealth use by mental health professionals in New Zealand during the pandemic. The aim of the current study was to examine and describe telehealth use and attitudes among Australian and New Zealand mental health professionals during the initial stages of the COVID-19 pandemic. A bi-national survey of mental health professionals was conducted to examine frequency of telehealth use, reasons for non-use, telehealth modalities, prior use, attitudes towards use, plans for future use, and training, information or resource needs.
Method
Participants and procedure
Participants were mental health professionals in Australia and New Zealand involved in the provision of psychological therapy or support directly to clients. Participants were invited to complete a 15-minute online survey hosted on Qualtrics during an 8-week period between May and July 2020. The first national lockdowns associated with COVID-19 were introduced in Australia and New Zealand in late March 2020. By mid-May 2020, lockdowns in Australia and New Zealand were eased, but reinstated in the Australian state of Victoria in mid-June following a ‘second-wave’ outbreak.
Several recruitment methods were used, including the distribution of survey invitations through newsletters, announcements and on the websites of peak and professional organisations. Study information was also e-mailed to professional networks of psychologists and psychiatrists, private practitioners, staff working in organisations delivering clinical care and through profession-focused social media groups and networks.
Participants were eligible for the study if they were at least 18 years old and were involved in the provision of direct psychological, psychiatric or mental health care to clients. The survey was not restricted to specific professions. Participants were not compensated for their participation. The study protocol was approved by the Australian National University Human Research Ethics Committee (protocol no. 2020/249) and ratified by The University of Auckland Human Participants Ethics Committee.
Measures
Demographic and professional characteristics
The following demographic information was collected: gender, age, country of residence, state/geographical area of residence, region (metropolitan, rural, remote) and highest level of education completed. The following professional characteristics were assessed: profession, professional endorsement/scope, professional registration type, years of experience providing clinical care, sector of practice, number of client contact hours per week, referral sources, therapies practised, client groups worked with, employment status, impacts of COVID-19 on employment, comfort with using technology (6-point scale ranging from ‘very comfortable/experienced’ to ‘very uncomfortable/inexperienced’) and current/previous use of digital mental health tools with clients. Respondents were asked if they had experienced any financial stress associated with the transition to telehealth. Minor adjustments were made to items in the survey sent to participants in New Zealand to reflect differences in terminology, organisations and regions.
Telehealth use and attitudes
Participants were asked if they had worked with clients via telehealth since the initial introduction of COVID-19 physical distancing requirements. Telehealth was defined in the survey as ‘working with clients via video-conferencing, telephone, e-mail, etc.’. Those who responded yes were asked to indicate the percentage of clients they were currently seeing via telehealth. Those who responded no and those who were seeing less than 100% of their clients via telehealth were asked to indicate their main reasons for not seeing clients via telehealth. Those currently seeing clients via telehealth were asked to indicate their most frequently used telehealth modality, which platforms/programmes they used, whether or not they had a choice to use telehealth and how their clients had responded to using telehealth (5-point scale ranging from ‘very positively’ to ‘very negatively’). All respondents (regardless of current telehealth use) were asked whether they had ever used telehealth prior to the pandemic, the percentage of clients they had previously seen via telehealth, whether they had received training in telehealth, their levels of exhaustion at work since the introduction of telehealth (5-point scale ranging from ‘a lot more exhausted than usual’ to ‘a lot less exhausted than usual’) and their willingness to use telehealth in the future (5-point scale ranging from ‘definitely’ to ‘definitely not’).
With regard to attitudes towards telehealth use, respondents were asked how they felt about using telehealth when it was first introduced (late March 2020) and how they felt about using telehealth at the time they responded to the survey (May–July 2020) (5-point scale ranging from ‘extremely positive’ to ‘extremely negative’). Respondents who were feeling negative about using telehealth were asked to describe their reasons for this in an open-ended question. Respondents were also asked to indicate their level of agreement with 22 statements assessing attitudes towards telehealth use (5-point scale ranging from ‘strongly disagree’ to ‘strongly agree’). The statements were developed by the authors to assess a range of attitudinal domains, including client safety/privacy, impact on therapeutic quality or practice, therapist confidence, experience, skills, and access to necessary resources, efficacy and telehealth use beyond COVID-19.
All respondents were asked whether they had any ‘wants’ or ‘needs’ with regard to telehealth use. Those who indicated that they wanted further training were asked in an open-ended question to describe the specific topic areas in which they would like to receive training.
Statistical analyses
Descriptive statistics were used to summarise the demographic and professional characteristics of the sample, frequency and characteristics of telehealth use, attitudes towards telehealth use, and wants and needs regarding current and future telehealth use. Ordinal regression was used to examine predictors of frequency of telehealth use (proportion of clients seen via telehealth) and attitudes towards telehealth use at the time of the survey (single item assessing how respondents felt about using telehealth, ranging from ‘extremely negative’ to ‘extremely positive’). Time (days since first survey completed), age (years), gender (male vs female), whether the respondent worked with complex or risky client groups (yes vs no), hours of client contact per week, prior use of telehealth (yes vs no), prior use of online programmes with clients (yes vs no), comfort with using technology (quite or very comfortable vs somewhat comfortable, somewhat uncomfortable, quite uncomfortable), prior training in telehealth (yes vs no) and choice to use telehealth (yes vs no) were modelled as predictors. Qualitative data obtained from open-ended responses were analysed using the reflexive thematic analysis approach developed by Braun and Clarke (2006, 2021). Responses were coded semantically, whereby coding and theme development reflected the explicit content of the data. A summary table of coding for the thematic analysis is available from the authors on request.
Results
Sample characteristics
The survey was completed by 528 mental health professionals. Table 1 (Supplementary material) shows the demographic characteristics of the sample. The sample was predominantly female (85.2%), with an average age of 47 years (SD = 11.8). Most respondents were from Australia (89.4%) and were working in metropolitan areas (78.8%). Respondents were obtained from all states and territories in Australia and 11 of 16 regions in New Zealand. Nearly 70% of the sample had obtained either a Master’s or Doctoral degree as their highest level of education. Table 2 (Supplementary material) shows the professional characteristics of the sample. The sample was composed mostly of psychologists (80.1%), followed by social workers (9.7%) and counsellors (5.3%). The sample had an average of 15 years (SD = 9.54) of experience providing clinical care to clients, and most respondents worked in private practice (72.9%). Most respondents worked with adult populations (83.9%), although a considerable proportion worked with young adults (57.6%) and adolescents (38.8%). Respondents received referrals most commonly from general practitioners (63.4%) and word of mouth (41.1%). The most commonly practised therapeutic approaches were cognitive behaviour therapy (CBT; 79.5%), followed by trauma-informed approaches (59.5%), acceptance and commitment therapy (ACT; 56.3%) and mindfulness-based approaches (54.2%). 90.3% of respondents reported using multiple therapeutic approaches. Most of the sample (74.8%) reported that their working conditions were impacted in some way by COVID-19 (e.g. reduced hours, job loss, working from home), 40.5% reported experiencing financial stress and nearly 80% of the sample reported that they felt a little or a lot more exhausted than usual since the introduction of telehealth. The majority of respondents (71.4%) reported that they felt quite or very comfortable with using technology, and just over one-third of the sample (34.5%) reported that they currently or had previously used online mental health programmes with their clients.
Telehealth use.
Predictors of frequency of telehealth use.
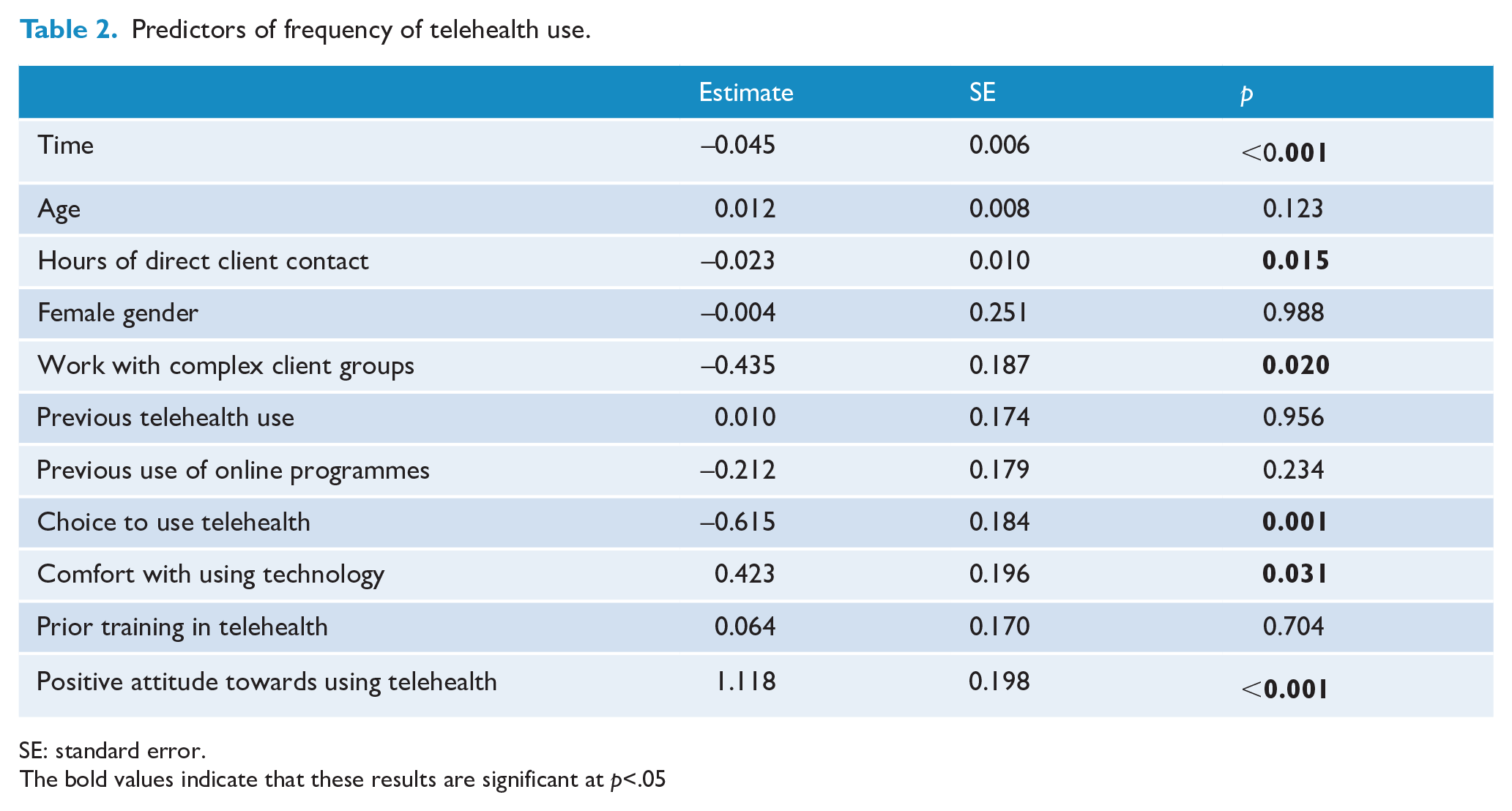
SE: standard error.
The bold values indicate that these results are significant at p<.05
Telehealth use
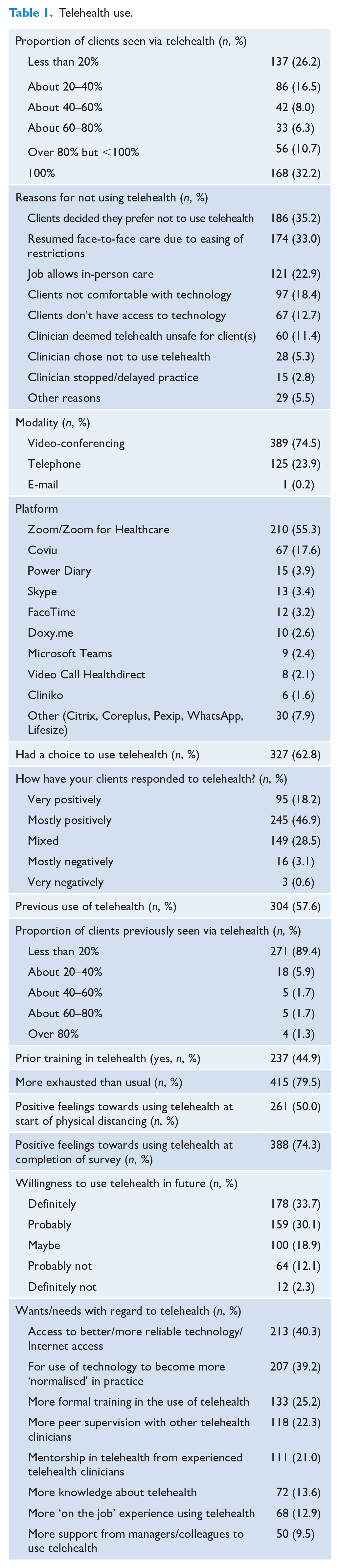
Table 1 shows telehealth use among the sample. Just over half (57.7%) of the sample reported having used telehealth in their practice before the pandemic. However, the frequency of telehealth use prior to the pandemic was minimal, with 89.7% of respondents reporting that they had previously used telehealth with less than 20% of their clients. After the start of the pandemic, 522 (98.9%) respondents reported having used telehealth, and one-third (n = 168; 32.2%) of respondents reported that they were currently seeing all of their clients via telehealth. Among those who were not seeing all of their clients via telehealth, the most commonly reported reasons for not using telehealth were related to clients (client preference or client lack of access/familiarity with technology) and job or situational factors (easing of COVID-19 restrictions, having a job that allows face-to-face care). Relatively few respondents indicated their own preference as a reason for not using telehealth.
Table 2 shows predictors of frequency of telehealth use. Lower rates of telehealth use were reported by participants who were recruited later in the survey recruitment period (p < 0.001). Lower use was also reported by respondents who worked with clients experiencing complex issues (e.g. trauma) (p = 0.020), those who had more hours of direct client contact per week (p = 0.015) and those who had a choice about whether or not to use telehealth (p = 0.001). Higher rates of telehealth use were found among those who were more comfortable with using technology (p = 0.031) and those who felt positively towards using telehealth (p < 0.001). However, telehealth training, previous telehealth use and clinician demographics were not associated with the use of telehealth.
Video-conferencing was the most commonly used telehealth modality (74.5%) and Zoom and Coviu were the most commonly reported platforms used. The majority of the sample reported that they used telehealth by choice (62.6%). Very few respondents reported that their clients responded negatively to using telehealth, but one-third reported that their client’s responses were mixed. Over 60% of the sample reported that they would probably or definitely use telehealth in the future.
Attitudes towards telehealth use
Half of the sample reported feeling somewhat or extremely positive about using telehealth when physical distancing was first introduced. Those who reported feeling neutral or negative about using telehealth reported a range of concerns, including the impact of telehealth on the therapeutic relationship and connection to clients, the reliability of technology, the quality and effectiveness of conducting assessments and delivering therapy via telehealth, uncertainty and lack of confidence using new technology, client safety, privacy and confidentiality, and reluctance among clients to use telehealth. However, when asked how they felt about using telehealth at the time when they completed the survey, the proportion of respondents who felt positive increased to 74.3%. Table 3 shows predictors of positive attitudes towards telehealth use. The likelihood of feeling positive towards using telehealth was higher among those who completed the survey later in the survey recruitment period (p < 0.001). Respondents were more likely to feel positive about using telehealth if they were female (p < 0.001), had used online programmes with clients previously (p = 0.040) and were comfortable with using technology (p = 0.027). Frequency of telehealth use was also related to attitudes. Those who used telehealth with less than 60% of their clients were less likely to report feeling positively about using telehealth, compared to those who saw 100% of their clients via telehealth. Due to the significant main effect of gender and the predominance of psychologists in the sample, we explored whether gender and profession (psychologist vs other) modified the effects of the other significant independent predictors of attitudes towards telehealth. Two interactions significantly improved model fit. A significant interaction between gender and amount of telehealth use was found, such that males with no or minimal telehealth use were more likely to hold negative attitudes (estimate = 1.521, SE = 0.678, p = 0.025). A significant interaction was also found between profession and previous use of online programmes (estimate = −1.600, SE = 0.503, p = 0.001). Non-psychologists who had never used online programmes were more likely to hold negative attitudes towards telehealth.
Predictors of positive attitudes towards telehealth use.
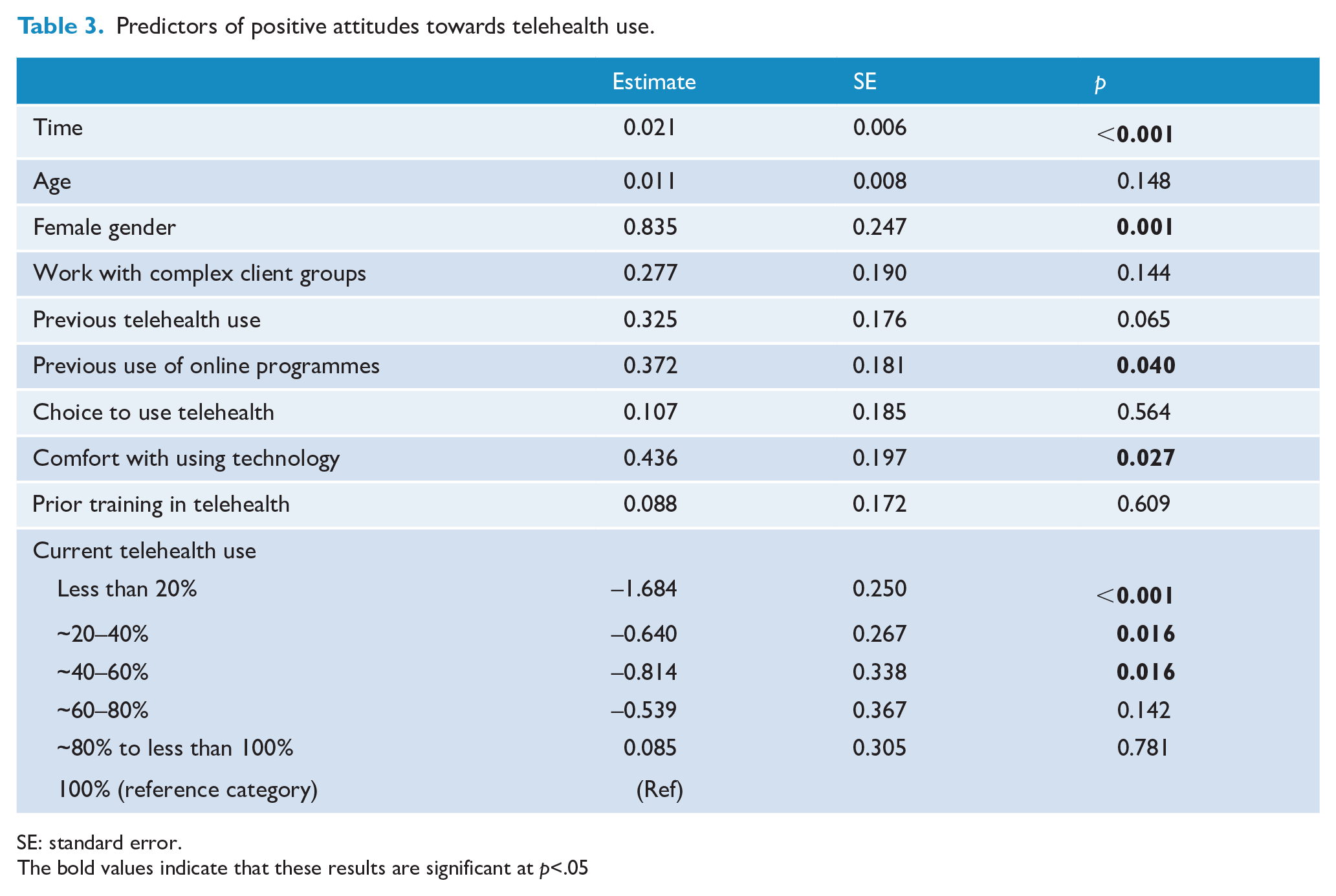
SE: standard error.
The bold values indicate that these results are significant at p<.05
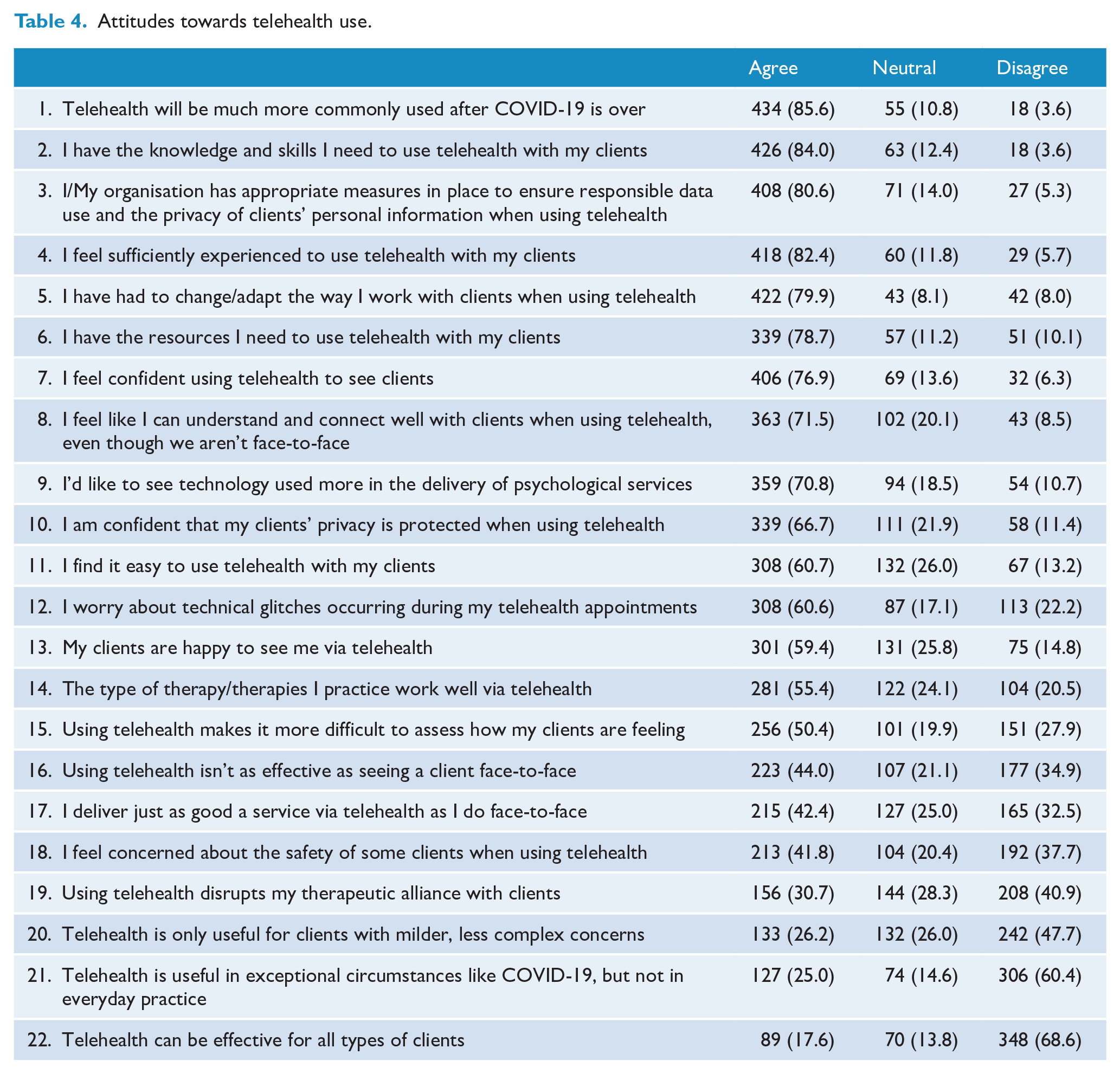
Table 4 shows respondents’ level of agreement with 22 statements assessing attitudes towards telehealth. The most strongly endorsed items related to confidence/preparedness to use telehealth and the ubiquity of telehealth use in the future. Most respondents agreed that they had the necessary skills, knowledge, experience, resources and confidence to use telehealth. The majority agreed that telehealth has utility beyond COVID-19 and that they would like to see technology used more in the delivery of psychological services generally. On the whole, respondents were not concerned that their client’s privacy is compromised when using telehealth and agreed that they and their organisations have appropriate measures in place to protect client privacy. Respondents were mixed, however, in their views about client safety. Approximately equal proportions of clients agreed and disagreed that they felt concerned about their clients’ safety when using telehealth. Despite more than half of the respondents reporting that they found it easy to use telehealth, the same proportion reported that they worried about technological glitches occurring when using telehealth. Respondents held mixed views on the impact of telehealth on therapeutic process and effectiveness. Just over half of the respondents agreed that the types of therapies they use worked well via telehealth, and half of the sample also agreed that telehealth makes it more difficult to assess how their clients are feeling. Similar proportions of respondents agreed and disagreed with the view that telehealth is not as effective as face-to-face care, that telehealth disrupts the therapeutic alliance and that they deliver just as good a service via telehealth as they do face-to-face. While respondents did not necessarily agree that telehealth is only useful for less complex clients, the majority did not agree that telehealth can be effective for all types of clients.
Attitudes towards telehealth use.
Wants and needs regarding telehealth use
The most commonly reported wants or needs with regard to telehealth were access to more reliable Internet service, for the use of technology to become more normalised in clinical practice and for more training in the use of telehealth. Other needs that respondents indicated in an open-ended question included ongoing support for telehealth under Medicare in Australia beyond COVID-19, guidelines for how to protect client confidentiality and data security, improved knowledge of how to effectively adapt therapy for delivery via telehealth and ways to help clients become better equipped to use telehealth. Respondents who indicated that they would like more training reported a desire for training on the following topics: how to adapt therapeutic techniques when using telehealth (including how to conduct assessments), how to build connection and therapeutic alliance via telehealth, how telehealth platforms work and how to get the most out of their functionality, managing client risk, confidentiality, privacy and data security, and how to use telehealth with specific populations (e.g. children).
Discussion
The findings from this study suggest that the transition to telehealth at the start of the COVID-19 pandemic presented challenges for many clinicians. Respondents reported disruptions to work, increased levels of exhaustion and financial stress, in addition to the inherent difficulty of quickly transitioning to a new modality of working with minimal preparation. Moreover, a significant proportion of respondents had never used telehealth previously, and the majority of those who had used telehealth had done so infrequently. Rates of telehealth use were lower among those who responded later in the survey period (when lockdowns had eased in most parts of Australia and New Zealand) and those who had a choice about whether or not to use telehealth. This suggests that, unsurprisingly, many respondents retained a desire to work face-to-face in some capacity throughout the transition to telehealth.
However, acceptance of telehealth was generally high among the sample, which is consistent with other studies of clinician attitudes towards telehealth (Connolly et al., 2020). Although respondents showed a desire to resume some face-to-face work when possible, many wanted the option of telehealth to remain available to them and intended to use telehealth in the future. Respondents held generally positive views towards telehealth, and positive views were more likely among those who completed the survey later in the survey period, those who used telehealth more frequently and those who were more comfortable with using technology. These findings suggest that familiarity breeds confidence; the more the respondents used telehealth and were familiar and comfortable with using technology, the more likely they were to view telehealth more favourably. It is also possible that respondents viewed telehealth more favourably when they had the flexibility to choose how much and with whom they used telehealth, instead of being required to use telehealth universally (Venville et al., 2021).
Relatedly, there were nuances in respondents’ attitudes towards the suitability of telehealth for specific client groups. Respondents showed a reluctance to use telehealth with clients experiencing complex issues such as trauma and post-traumatic stress disorder (PTSD), did not agree that telehealth is effective for all types of clients and reported concerns about client safety when using telehealth. Further research is needed to elucidate the reasons for these beliefs, as well as the safety and efficacy of telehealth use among clients with different clinical presentations. Although there is robust evidence for the use of video-conferencing in the treatment of PTSD (Thomas et al., 2021), there is currently only limited evidence for the effectiveness of telehealth among those with other serious and/or complex mental illnesses and those facing social disadvantage (Santesteban-Echarri et al., 2020). However, new evidence is emerging that has documented the successful implementation of telehealth in populations with serious mental illness during the COVID-19 pandemic (Lynch et al., 2020; Miu et al., 2020). Although further research is needed to support the use of telehealth with particular client groups, in practice, this should be negotiated between individual clinicians and clients. ‘Blanket rules’ about the suitability of telehealth in particular contexts may risk further widening existing inequities in access to treatment among vulnerable client groups.
The most commonly reported reasons from clinicians for not using telehealth were related to client preference/access to technology and job or situational factors. Relatively few respondents indicated that they were not using telehealth because they personally did not feel comfortable or did not want to use telehealth. Noting that these data are not based on direct reports from clients, there may have been some level of apprehension among clients about the efficacy, safety or quality of telehealth in the early stages of the pandemic, despite some evidence suggesting that clients found telehealth largely acceptable (Guinart et al., 2020). For many clients, the pandemic may have been their first exposure to telehealth for psychological and psychiatric support, so their apprehension may largely reflect a lack of familiarity with this modality. Nonetheless, longitudinal research is required to rigorously examine changes in attitudes towards and acceptance of telehealth among clients, particularly as the COVID-19 pandemic evolves. It is also important to note that client reluctance to use telehealth may have also been influenced by any negative attitudes held and communicated to them by their clinician (either directly or indirectly).
A wide range of platforms were used by clinicians, and notably, some are more appropriate for use within healthcare settings than others. The variability observed in platform usage may be due to a number of factors: clinician inexperience with, lack of knowledge of, or lack of access to appropriate or recommended platforms, lack of knowledge among clients about how to use certain platforms (which may have led to the use of more familiar platforms already used for social communication) and the little time that clinicians had to source and learn how to use an appropriate platform during the transition to telehealth. Best practice involves the use of telehealth platforms that are purpose built for healthcare and ensure data security and privacy. It is essential that clinicians have access to high-quality information and guidance regarding how to choose and use an appropriate telehealth platform.
Respondents did not indicate that they felt inexperienced, lacked knowledge or felt unprepared to use telehealth at the time of the survey. This may reflect the high levels of technological literacy among the sample, or the amount of time that had passed between the introduction of telehealth (late March 2020) and the time of the survey (May to July 2020). Clinicians may have gained considerable practical experience using telehealth by the time recruitment for the survey commenced. In addition, having completed previous training in telehealth was not related to participant telehealth usage or attitudes. This is important given that most implementation interventions focus on clinician training, and while this may improve clinician confidence and reduce their perceptions of obstacles to using telehealth (Whiting et al., 2021), these factors may not be sufficient to lead to increased telehealth adoption. Instead, external requirements for telehealth use and availability of funding have resulted in a sharp increase in uptake. This suggests that efforts to implement and sustain broader uptake of high-quality telehealth require additional strategies beyond clinician training and education (e.g. accreditation/standards for use, incentives and support structures).
Respondents were mixed with regard to their views on how telehealth impacts on therapeutic process and quality. Just over 40% of respondents expressed the view that telehealth is not as good as face-to-face care, despite evidence that telehealth care can be just as effective (Backhaus et al., 2012; Irvine et al., 2020; Norwood et al., 2018). Although some evidence suggests that telehealth does not negatively impact therapeutic alliance (Norwood et al., 2018; Simpson and Reid, 2014b), respondents were mixed regarding their views on this, with roughly equal numbers of respondents agreeing and disagreeing with this view. A variety of factors are likely to influence clinician attitudes, including their values and comfort levels with technology (Knott et al., 2020), how they personally experience telehealth delivery, their knowledge of the evidence for telehealth use, the quality of telehealth services (e.g. the extent to which telehealth is safe, accredited and sufficiently resourced) and how their clients respond to telehealth. It is unclear which of these or other factors have the strongest influence over clinician attitudes, and it is also important to recognise that these data were collected during a time of extreme community stress and among a workforce and a client base that were both largely unprepared for and unfamiliar with using telehealth.
It was clear among respondents that they believed that telehealth would remain an important part of mental health service delivery, and respondents were largely supportive of this. Indeed, the COVID-19 pandemic has been described as a ‘black swan’ moment for mental health care and e-mental health (Wind et al., 2020). Thus, it is important to identify the individual, organisational, professional and policy responses needed to enable the mental health workforce to continue to deliver telehealth safely and effectively (Thomas et al., 2020). Respondents identified a desire for the use of technology to become more normalised in clinical practice, and for more training in the use of telehealth (specifically in how to adapt therapy for delivery via telehealth and how to manage client risk, confidentiality, privacy and data security). It is likely that the implementation of telehealth during the pandemic has gone some way to normalising the use of technology in practice, and there is a need for implementation science research to identify how best to deliver telehealth, test strategies to address barriers and facilitators to telehealth use and to understand factors underlying normalisation of telehealth and organisational readiness for change.
Respondents identified a desire for access to more reliable Internet service, and Australian respondents identified a desire for ongoing support for telehealth under Medicare in Australia beyond COVID-19 (as noted, New Zealand had already adopted such a scheme prior to the pandemic). To date, the Australian Government has been successfully lobbied to extend financial support for telehealth under Medicare, but the permanency of this policy is currently unclear. There is a high risk of losing the significant gains that have been made towards the implementation of technology in clinical practice and improved access to care if government support for universal telehealth is not maintained.
Limitations
There were several limitations associated with the study. The sample was not representative, despite being large and diverse, with good geographical coverage, and broadly reflecting the demographic characteristics of clinicians in Australia and New Zealand. The sample had low representation of male participants, although this broadly reflects the gender distribution of mental health professionals, which is the population of interest. Some of the findings may reflect a lack of variability in the sample on particular variables, as well as sampling bias (e.g. those with an interest in telehealth and e-mental health, or those with greater time/capacity to respond to an online survey invitation may have been more likely to participate in the survey). Moreover, a high proportion of the sample were psychologists working in private practice, who, given their high use of Medicare subsidised video-conferencing, may have been more likely to equate the broader concept of telehealth with video-conferencing, and respond to the survey items using this frame of reference. The data are cross-sectional and were collected in a period of rapid flux, so additional research is needed to examine within-person change over time and how contextual factors may have influenced responses. Finally, although the focus of this study was to describe a broad range of clinician attitudes, brief self-report single-item measures were used to assess attitudes, and further research is needed to validate the attitudinal items and assess whether they represent underlying latent constructs.
Conclusion
This is the largest study of practitioner experiences and views towards telehealth use in Australia and New Zealand during the crucial transitional period early in the COVID-19 pandemic. Australian and New Zealand mental health clinicians adapted effectively to the rapid shift to telehealth, in spite of high levels of exhaustion and stress, primarily because many had no alternative to enable them to continue to provide care. Given that telehealth is likely to remain a feature of mental health service delivery into the future, it is important that the views and experiences of mental health professionals are considered in policy and practice decision-making and that clinicians are provided with the appropriate organisational, professional and policy-based support to continue to deliver telehealth safely and effectively.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221089229 – Supplemental material for Telehealth use by mental health professionals during COVID-19
Supplemental material, sj-docx-1-anp-10.1177_00048674221089229 for Telehealth use by mental health professionals during COVID-19 by Louise M Farrer, Bonnie Clough, Marthinus J Bekker, Alison L Calear, Aliza Werner-Seidler, Jill M Newby, Vikki Knott, Piers Gooding, Julia Reynolds, Leah Brennan and Philip J Batterham in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: L.M.F. is supported by Australian Research Council Discovery Early Career Research Award (DE190101382). A.L.C. is supported by National Health and Medical Research Council Fellowship (1173146). P.J.B. is supported by National Health and Medical Research Council Fellowship (1158707). J.M.N. is supported by a Medical Research Future Fund Fellowship (1145382). P.G. is supported by Australian Research Council Discovery Early Career Research Award (DE200100483). A.W.-S. is supported by National Health and Medical Research Council Fellowship (1197074).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.