
Abstract
Objective:
Physical inactivity, sugar sweetened beverage consumption, alcohol use, smoking, poor sleep and excessive recreational screen time (the ‘Big 6’ lifestyle risk behaviours) often co-occur and are key risk factors for psychopathology. However, the best fitting latent structure of the Big 6 is unknown and links between multiple lifestyle risk behaviours and hierarchical dimensions of psychopathology have not been explored among adolescents. This study aimed to address these gaps in the literature.
Methods:
Confirmatory factor analysis, latent class analysis and factor mixture models were conducted among 6640 students (Mage = 12.7 years) to identify the latent structure of the Big 6 lifestyle risk behaviours. Structural equation models were then used to examine associations with psychopathology.
Results:
A mixture model with three classes, capturing mean differences in a single latent factor indexing overall risk behaviours, emerged as the best fitting model. This included relatively low-risk (Class 1: 30%), moderate-risk (Class 2: 67%) and high-risk (Class 3: 3%) classes. Students high on externalizing demonstrated significantly greater odds of membership to the high-risk class (odds ratio = 8.75, 99% confidence interval = [3.30, 23.26]) and moderate-risk class (odds ratio = 2.93, 99% confidence interval = [1.43, 5.97]) in comparison to the low-risk class. Similarly, students high on internalizing demonstrated significantly higher odds of membership to the high-risk class (odds ratio = 1.89, 99% confidence interval = [1.06, 3.37]) and the moderate-risk class (odds ratio = 1.66, 99% confidence interval = [1.03, 2.67]) in comparison to the low-risk class. Associations between lower order factors of psychopathology and lifestyle risk behaviours were mostly accounted for by the more parsimonious higher order factors.
Conclusion:
Classes representing differences in probabilities of the Big 6 lifestyle risk behaviours relate to varying levels of hierarchical dimensions of psychopathology, suggesting multiple health behaviour change and transdiagnostic intervention approaches may be valuable for reducing risk of psychopathology.
Adolescence is a critical period for psychopathology (i.e. the manifestation of mental disorders), with half of all conditions beginning by age 14 (Kessler et al., 2007). Globally, 10–20% of children and adolescents experience psychopathology, most commonly including anxiety and depressive disorders, attention-deficit/hyperactivity disorder (ADHD) and disruptive disorders (Kessler et al., 2007; Polanczyk et al., 2015). In Australia, among those aged 12–17, 7% have an anxiety disorder, 6.3% have ADHD, 5% have major depressive disorder, 2.1% have conduct disorder and 20% have high or very high levels of psychological distress (Lawrence et al., 2015).
Several lifestyle risk behaviours have been associated with adolescent psychopathology, including physical inactivity, sugar sweetened beverage (SSB) consumption, alcohol and tobacco use, poor sleep and sedentary behaviours, including recreational screen time (Hayward et al., 2016; Sunderland et al., 2021a). These lifestyle risk behaviours, collectively referred to as the ‘Big 6’, often emerge during adolescence when young people gain more autonomy (Spring et al., 2012). Once established, these risk behaviours are not only associated with increased risk for psychopathology but also other chronic diseases, such as cardiovascular disease, in later life (Ding et al., 2015).
Evidence suggests that the Big 6 co-exist in predictable patterns, with certain behaviours commonly co-occurring (Champion et al., 2018; Gardner et al., 2020). This is concerning given the risk of disease and mortality due to increasing lifestyle risk behaviours is not simply additive (Ding et al., 2015), and the likelihood of engaging in multiple risk behaviours increases throughout adolescence (Australian Institute of Health and Welfare, 2017; Spring et al., 2012). Clusters of the Big 6 have been shown to relate to psychopathology in older adolescents (Mage = 18.88 years), with clusters characterized by smoking and binge drinking along with poor fruit/vegetable intake linked to the highest levels of psychological distress, depression and anxiety (Champion et al., 2018). However, it is unknown whether these clusters derived from latent class analysis (LCA) best represent the correlations among the Big 6. It is also possible that the underlying structure of lifestyle behaviours might be best represented by one or more continuous dimensional factors, or a combination of both categorical and continuous latent factors (Clark et al., 2013). The best fitting structure has several implications regarding the measurement and clinical utility of these behaviours. Understanding associations between the underlying structure of the Big 6 and psychopathology could guide targeted prevention efforts to improve adolescent health. However, to our knowledge, no study has explored this research question.
Previous research examining associations between risk behaviours and psychopathology has predominantly focused on single disorder relationships, and in the same way that complexities across multiple risk behaviours have been ignored, so too have the complex associations between multiple psychopathological conditions. There is growing evidence that psychopathological conditions often co-occur more than expected by chance, particularly among young people (McElroy et al., 2018). The Hierarchical Taxonomy of Psychopathology (HiTOP) model has emerged as a way of accounting for this comorbidity and has garnered support (Kotov et al., 2017). This model conceptualizes psychopathology as a range of indicators within a hierarchy of dimensions that range from specific symptoms at the lowest level to a broad general psychopathology factor accounting for the shared relationships across all conditions at the highest level. Sitting below the broad general factor in the hierarchy are the internalizing and externalizing spectra, which are thought to explain the co-occurrence of some of the more common psychopathological conditions and have received the most empirical attention (Kotov et al., 2017; Krueger et al., 1998). Internalizing is thought to represent the shared relationships among mood and anxiety disorders, whereas externalizing is thought to represent the relationships among antisocial, conduct, oppositional defiance, substance use and impulsivity-related disorders (Krueger et al., 1998).
Studies among adults (Slade, 2007; Van de Pavert et al., 2017) have demonstrated the potential utility of a hierarchical approach to psychopathology by examining associations between transdiagnostic factors, including internalizing and externalizing, and chronic physical conditions (e.g. respiratory conditions, arthritis, digestive conditions), as well as individual lifestyle risk behaviours (e.g. smoking status). However, there is a dearth of evidence examining associations with multiple lifestyle risk behaviours during the critical period of adolescence. Initial research by Sunderland et al. (2021b) suggests that sleep problems among adolescents are related to the broad tendency to experience all disorders, but also specifically related to internalizing when controlling for broad general psychopathology. In contrast, there does not appear to be significant associations between individual symptom indicators of psychopathology and sleep after accounting for the relationships with the broad latent factors. Additional research is required to comprehensively investigate the associations between general psychopathology and the structure of multiple lifestyle behaviours.
To address these gaps in the literature, the present study aims to:
Identify the best fitting latent structure of the Big 6 among adolescents.
Examine relationships between the best fitting model of the Big 6 and general (higher order) and specific (lower order) psychopathology dimensions.
Method
Participants and procedure
This study uses baseline data from the Health4Life Study, a cluster randomized controlled trial of an eHealth intervention targeting the Big 6 among Australian secondary school students (Teesson et al., 2020). The self-reported data were collected from July to November 2019. This study was approved by the University of Sydney Human Research Ethics Committee (2018/882), New South Wales (NSW) Department of Education (SERAP No. 2019006), the University of Queensland (2019000037), Curtin University (HRE2019-0083) and relevant Catholic school committees. A total of 71 schools from 3 Australian states (37 from NSW, 18 from Queensland and 16 from Western Australia) agreed to participate, including independent/private (n = 38), government (n = 24) and Catholic (n = 9) schools. Only students who gave written consent (95%) and had parental consent (77%) were eligible to participate. The final analysed sample comprised 6640 students.
Measures
Sociodemographic characteristics
Students self-reported information on gender (male, female, non-binary/gender fluid, missing), age and socioeconomic status (SES). The Family Affluence Scale III was used to assess relative SES compared to other individuals in the sample. The scale was re-scored to represent a ridit score ranging from 0 to 1 with high scores indicating higher relative SES. The continuous ridit scores were converted into three groups to aid interpretation based on the relative distribution of SES in this population, representing individuals who fall in a lower (ridit < 0.2), middle (ridit ⩾ 0.2 and ⩽ 0.6) and upper (ridit > 0.6) range (Elgar et al., 2017).
The Big 6
Sleep was evaluated by the Modified Sleep Habits Survey (Short et al., 2013). Total sleep time was calculated by finding the difference between the time sleep was first attempted to the time they finally woke up in the morning, minus the time taken to fall asleep from first attempt. Self-reported bedtime, waketime and sleep duration are reliable and valid in adolescent populations (Nascimento-Ferreira et al., 2016). The weighted average sleep duration for school and weekend nights was recoded into a binary variable representing the Australian recommended health guideline for sleep: 9–11 hours/night for those aged 11–13 years and 8–10 hours/night for those aged 14–17 years (The Australian Government Department of Health, 2019).
Sedentary recreational screen time was assessed using the International Sedentary Assessment Tool (Prince et al., 2017) to evaluate time spent on a typical weekday and weekend day over the past 7 days watching television/DVDs/streaming services or using an electronic device. Those who spent more than 2 hours/day on sedentary recreational screen time were coded as at risk, as per the Australian health guideline (Australian Government Department of Health, 2019).
SSB consumption was assessed using an item adapted from the self-reported NSW School Physical Activity and Nutrition Survey (SPANS; Hardy et al., 2016). A dichotomized variable was created to reflect high and low consumption, using the threshold of 5–6 cups or more per week for high consumption.
Physical inactivity was assessed using the item (Active Healthy Kids Australia, 2016): Over the past 7 days, on how many days were you engaged in moderate to vigorous physical activity (activity that increases heart rate and gets you out of breath some of the time) for at least 60 minutes? Physical activity can be accumulated over the entire day (e.g., in multiple different blocks of 10 minutes).
A binary variable was created based on the Australian guidelines for children and young people, which recommend at least 60 minutes of moderate-to-vigorous physical activity (MVPA)/day (The Australian Government Department of Health, 2019).
Alcohol and tobacco use were measured using two dichotomous (yes/no) items: ‘Have you had a full standard alcoholic drink in the past 6 months?’ and ‘In the past 6 months, have you tried cigarette smoking, even one or two puffs?’. Both items have been used in large-scale trials and population-based epidemiological surveys (Australian Institute of Health and Welfare, 2017).
Psychopathology
Indicators of psychopathology were derived from multiple measures. Symptoms of anxiety over the past 7 days were assessed using the Patient-Reported Outcomes Measurement and Information System Anxiety scale for children (PROMIS-A; Irwin et al., 2010). Symptoms of depression were measured using a modified version of the Patient Health Questionnaire-9 (PHQ-9; Johnson et al., 2002); however, the question regarding thoughts of death was removed due to ethical concerns. Individual items from the emotional symptoms, hyperactivity/inattention and conduct problems subscales of the Strengths and Difficulties Questionnaire (SDQ; Goodman, 2001) were used to provide broad and specific indicators of psychopathology. All measures have been extensively tested among adolescents and demonstrate strong psychometric properties (Goodman, 2001; Irwin et al., 2010; Johnson et al., 2002).
Statistical procedure
Descriptive analysis
The sample characteristics were outlined using descriptive statistics along with prevalence estimates of the Big 6 (at risk vs not at risk). Additional correlation analyses using tetrachoric and polychoric correlations were conducted using individual items from each of the scales and are reported in Supplementary Tables 1 and 2.
Structure of the Big 6
To determine the latent structure of the Big 6, a series of LCA, item factor analysis (IFA) and factor mixture models (FMM) were used based on a methodology described in Clark et al. (2013). A series of LCA models were run with an increasing number of classes until either there was no improvement in model fit or there was insufficient information to fit additional classes. Next, an IFA model was estimated that tested the assumption that all behaviours represent a single dimension with higher scores indicating greater probability of all lifestyle risk behaviours. Finally, a series of FMMs, which comprise a hybrid of continuous and categorical latent factors, were estimated that fit a single dimension and an increasing number of latent classes. There are several variants of FMM proposed in the literature. For the current study, FMMs were estimated that held the item thresholds and factor loadings invariant across latent classes whereas the factor mean is allowed to vary (factor variances were fixed to zero). This model can be interpreted as a non-parametric factor model with the latent classes representing homogeneous groups of people with different scores on the latent dimension, therefore enabling the estimation of a non-normal distribution (Clark et al., 2013).
The models were estimated using a robust maximum likelihood estimator (MLR) and a logit link with an increased number of random starting values to ensure multiple replications of the best log-likelihood value. The best model was adjudicated using a combination of Bayesian information criterion (BIC) values as well as the Lo-Mendell-Rubin log-likelihood difference test used to compare a model with k classes with a model with k − 1 classes (Nylund et al., 2007). All models were estimated using Mplus version 8.4.
Higher order structure of psychopathology
To estimate the higher order factor structure of individual items from the psychopathology measures, a series of IFA models were estimated based on previous literature (Sunderland et al., 2021b). Five models were estimated using a weighted least squares estimator (WLSMV) and a probit link: (1) a one-factor model with all indicators of psychopathology loading on a single factor; (2) a correlated two-factor model with factors representing internalizing symptoms (PHQ, PROMIS-A, SDQ-emotion) and externalizing symptoms (SDQ-hyperactivity, SDQ-conduct); (3) a correlated five-factor model with factors representing depression symptoms (PHQ), anxiety symptoms (PROMIS-A), emotionality (SDQ-emotion), hyperactivity (SDQ-hyperactivity) and conduct problems (SDQ-conduct); (4) a higher order model with five lower order factors (described in model 3) loading onto a single higher order factor; and (5) a higher order model with five lower order factors (described in model 3) loading onto correlated internalizing (anxiety, depression, emotionality) and externalizing higher order factors (hyperactivity, conduct problems).
Models were compared using a range of model fit statistics and inspection of factor loading patterns, including the comparative fit index (CFI), the Tucker–Lewis fit index (TLI), the root mean square error of approximation (RMSEA) and the standardized root mean square residual (SRMR). Excellent model fit was determined using empirically derived cut-points (CFI and TLI > 0.95 and RMSEA and SRMR < 0.08) (Hu and Bentler, 1999). All models were estimated using Mplus V8.4.
Associations between the Big 6 and psychopathology
Regression models based on the best fitting measurement models were used to examine the broad and specific associations between indicators of psychopathology and the Big 6. The latent psychopathology variables were included as independent variables in models that treated the risk behaviour latent variables as outcomes, controlling for gender, age and SES. To examine the independent associations between lower order factors (depression, anxiety, emotionality, conduct and hyperactivity) with risk behaviours, a series of models were then estimated that included each lower order factor entered as a covariate along with the higher order factors (internalizing or externalizing), gender, age and SES. The contribution and magnitude of the direct association between the lower order factors and risk behaviours while holding the higher order factors constant was evaluated by inspecting the difference in BIC values between models that did and did not include the direct effect.
Results
Descriptive statistics
Descriptive statistics for the sample (n = 6640; Mage = 12.7 years, standard deviation [SD] = 0.50; range = 11–14, with 98% aged 12–13) are provided in Table 1. The sample comprised roughly an even split between male- and female-identifying students, and approximately 0.5% identified as non-binary/gender fluid. Most students exceeded guidelines for screen time (84%), did not achieve sufficient MVPA (75%) and just over half of the sample got inadequate sleep (56%). Conversely, only a relatively small percentage of students indicated risky SSB consumption (11%) and that they had used alcohol (3%) or tobacco (2%) in the prior 6 months.
Sample characteristics.
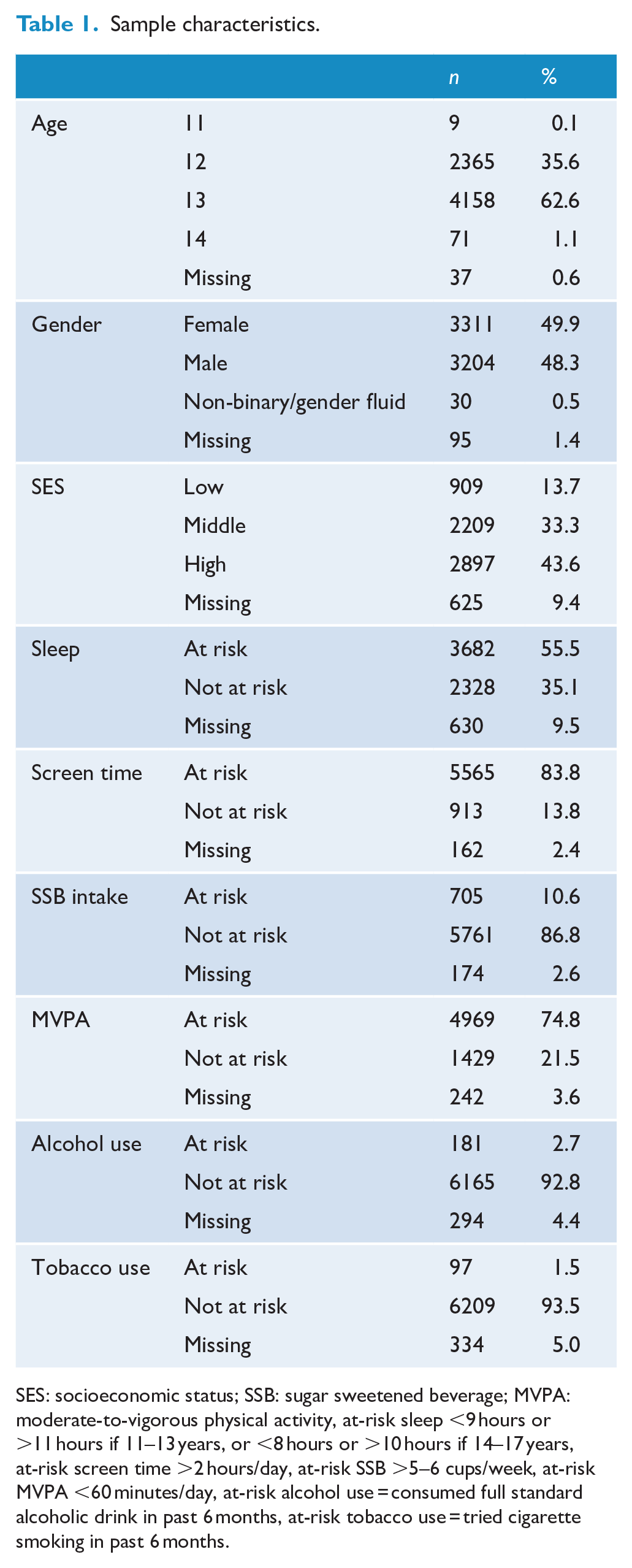
SES: socioeconomic status; SSB: sugar sweetened beverage; MVPA: moderate-to-vigorous physical activity, at-risk sleep <9 hours or >11 hours if 11–13 years, or <8 hours or >10 hours if 14–17 years, at-risk screen time >2 hours/day, at-risk SSB >5–6 cups/week, at-risk MVPA <60 minutes/day, at-risk alcohol use = consumed full standard alcoholic drink in past 6 months, at-risk tobacco use = tried cigarette smoking in past 6 months.
Structure of the Big 6
Structural models of the Big 6 were identified in the sample of 6535 students (105 cases removed due to missing data on all variables). The model fit statistics for LCA, IFA and FMM models are provided in Table 2. Overall, the one factor/three class FMM model demonstrated the best fit according to BIC values and was selected as the best fitting model for further analysis. The three classes were differentiated by significant differences in the mean factor scores, with Class 1 representing relatively low-risk and comprising 30% of the sample, Class 2 representing relatively moderate-risk and comprising 67% of the sample and Class 3 representing relatively high-risk and comprising 3% of the sample. The differences in the mean latent factor scores across the classes reflect different probabilities of risk behaviours and can be seen in Figure 1. The figure indicates the relative ranking of the three classes across each of the risk behaviours, except for MVPA, which evidenced poor discriminative performance across the classes. Moreover, the presence of alcohol use and tobacco use provided the greatest demarcation between the high-risk class in comparison to the moderate- and low-risk classes.
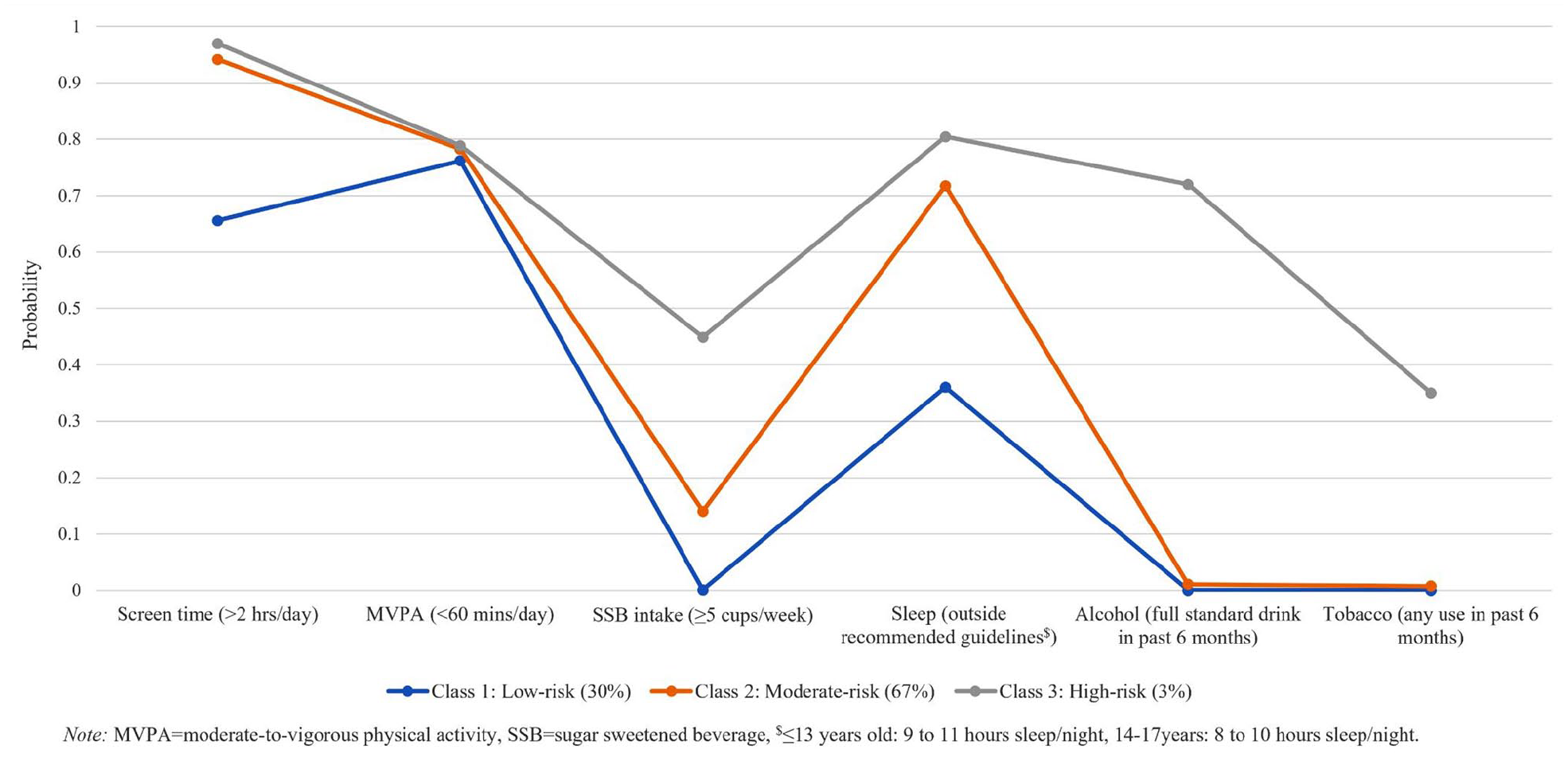
Estimated probability of the Big 6 lifestyle risk behaviours from the three class/one factor mixture model.
Model fit statistics for the latent class analysis, item factor analysis and factor mixture models.
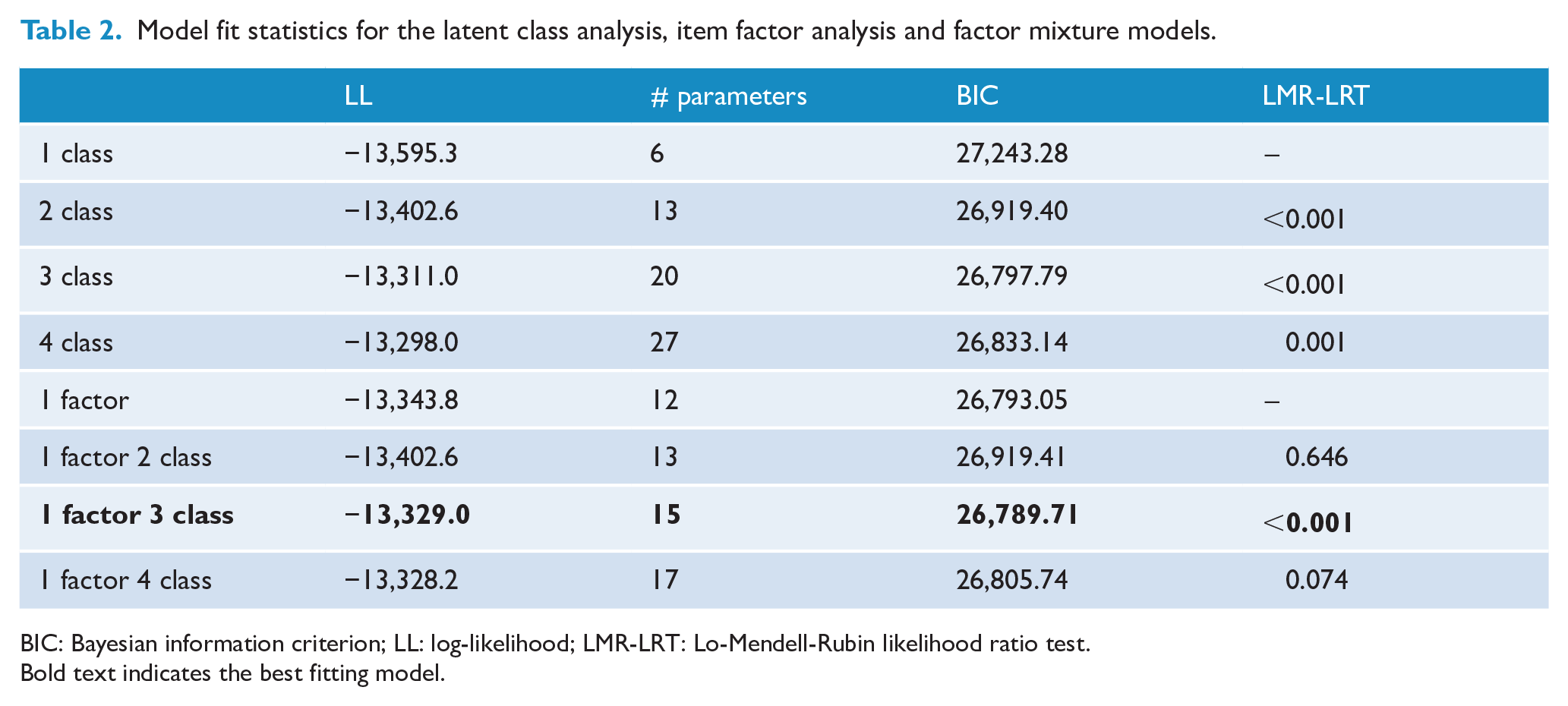
BIC: Bayesian information criterion; LL: log-likelihood; LMR-LRT: Lo-Mendell-Rubin likelihood ratio test. Bold text indicates the best fitting model.
Higher order structure of psychopathology
The model fit statistics associated with the estimated item factor models are provided in Table 3. The correlated five-factor model provided excellent fit in terms of the lower order factor structure with CFI/TLI > 0.95 and RMSEA/SRMR < 0.08. Additional models examining the higher order factor structure suggest that the correlation between the five lower order factors can be accounted for by two higher order correlated factors representing internalizing and externalizing behaviours/symptoms. This higher order model generated excellent model fit according to all fit statistics. The standardized higher order factor loadings are provided in Figure 2 with all lower order factors generating significant and high positive loadings (>0.80). The standardized factor loadings associated with the observed indicators and lower order factors are provided in Supplementary Table 3. A moderate correlation of 0.65 between the internalizing and externalizing higher order factors suggests that the two constructs are significantly related yet sufficiently distinct in this population.
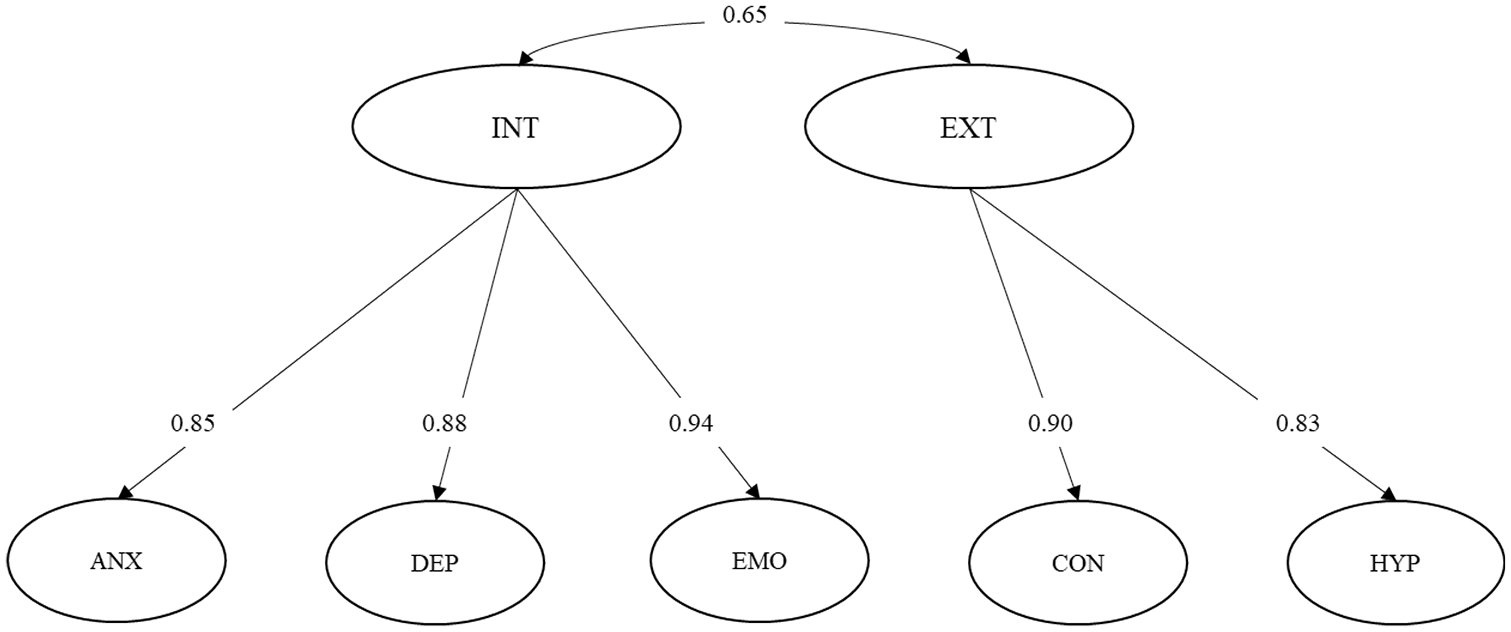
Path diagram and standardized factor loadings for the best fitting higher order model of psychopathology. Note: item level indicators are not presented to improve clarity.
Item factor analysis model fit statistics of psychopathology.
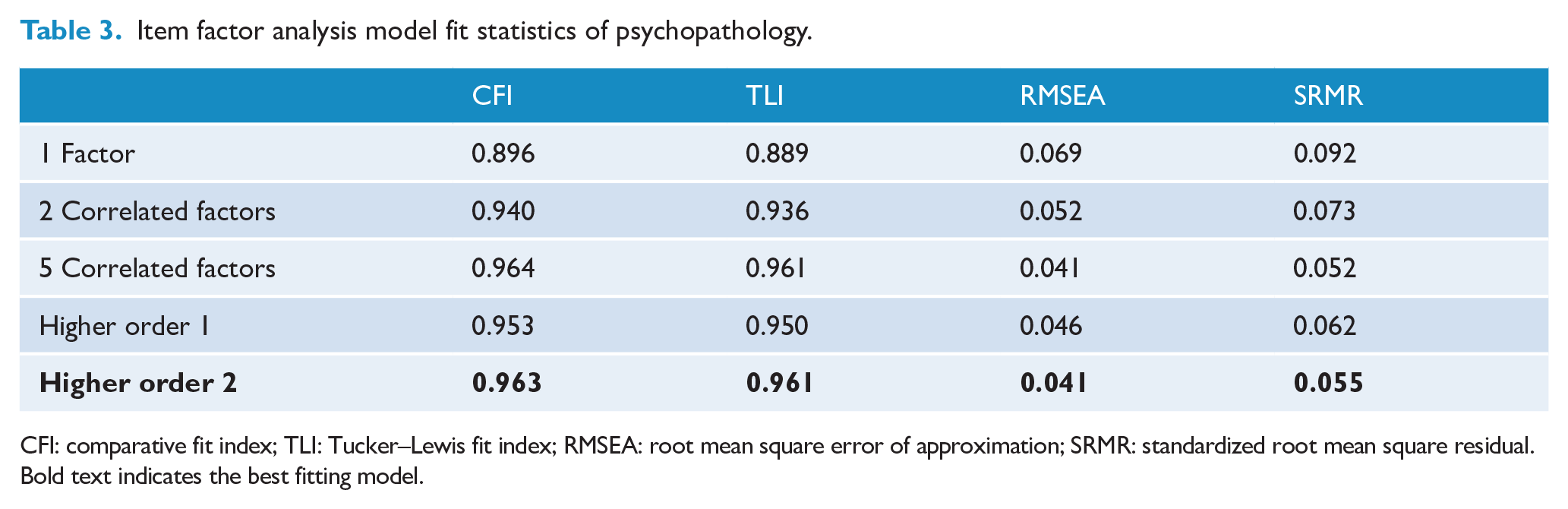
CFI: comparative fit index; TLI: Tucker–Lewis fit index; RMSEA: root mean square error of approximation; SRMR: standardized root mean square residual.Bold text indicates the best fitting model.
Associations between the Big 6 and psychopathology
Given the best fitting model for the Big 6 was a FMM with one factor and three classes, a three-step procedure was required to examine associations when treating the latent class membership as the outcome and factors of psychopathology as the covariates, while accounting for the misclassification error (Asparouhov and Muthen, 2014). Moreover, given it was computationally intractable to estimate a factor model with seven latent factors using numerical integration, the inclusion of psychopathology factors in the model with the latent classes was achieved via the use of Bayesian plausible values (only for the latent factors). See Figure 3 for a path diagram representing the general model. Plausible values for the seven latent factors were generated across 20 imputed datasets and have been shown to better account for the variance in the factor model in comparison to using single factor scores as observable variables (Asparouhov and Muthén, 2010). More detail regarding the methodology and example Mplus code is provided in the supplementary material.
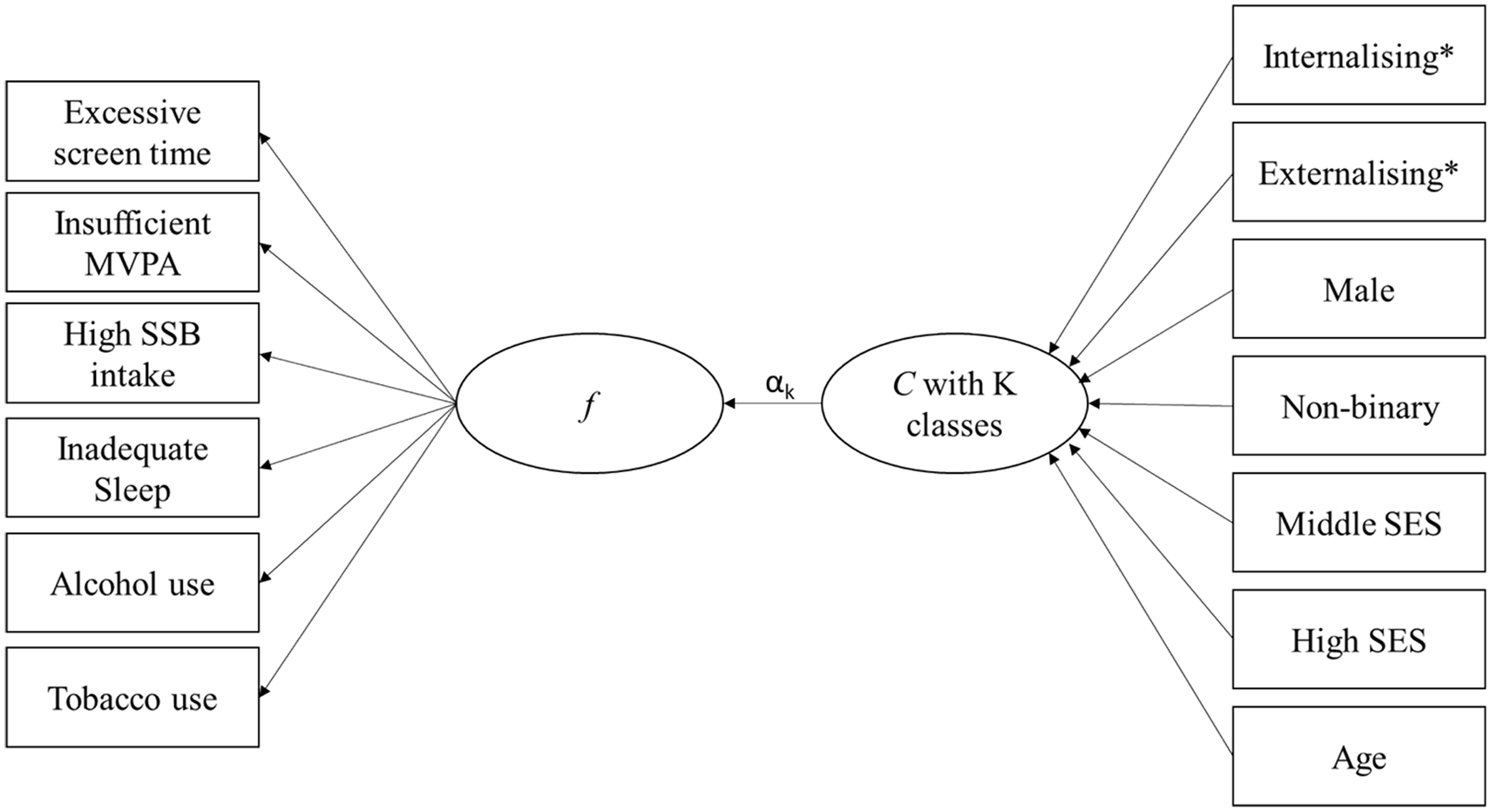
Path diagram representing associations between psychopathology and the best fitting factor mixture model representing lifestyle behaviours.
Latent class membership was significantly associated with psychopathology, with higher scores on externalizing associated with greater odds of membership to the high-risk class (odds ratio [OR] = 8.75, 99% confidence interval [CI] = [3.30, 23.26]) and the moderate-risk class (OR = 2.93, 99% CI = [1.43, 5.97]) in comparison to the low-risk class. Likewise, higher scores on internalizing were associated with greater odds of membership to the high-risk class (OR = 1.89, 99% CI = [1.06, 3.37]) and the moderate-risk class (OR = 1.66, 99% CI = [1.03, 2.67]) in comparison to the low-risk class. Additional model constraints indicated that higher scores on externalizing were associated with higher odds of membership to the high-risk group in comparison to the moderate-risk group (OR = 2.99, 99% CI = [1.41, 6.34]). However, there was no evidence that scores on internalizing were associated with membership to the high-risk group in comparison to the moderate-risk group (OR = 1.14, 99% CI = [0.70, 1.84]). Finally, models that included each of the lower order factors of psychopathology in addition to the higher order factors did not improve model fit versus a model that only included the higher order factors, as indicated by larger BIC values.
Discussion
This study is the first to explore the structure of the Big 6 lifestyle risk behaviours (physical inactivity, SSB consumption, alcohol use, tobacco smoking, poor sleep and recreational screen time) using a comprehensive set of latent variable models and to demonstrate associations with psychopathology among adolescents (age range, 11–14 years [98% aged 12–13 years]). Three classes, capturing mean differences in a single latent factor indexing overall risk behaviours emerged as the best fitting model, were associated with varying levels of psychopathology. Both externalizing and internalizing scores were positively and significantly associated with class membership, with higher scores demonstrating increased odds of membership to the high- and moderate-risk classes, in comparison to the low-risk class. However, there was evidence that higher externalizing scores, but not internalizing, significantly differentiated the high-risk class from the moderate-risk class. Finally, findings suggest that the associations between lower order factors and class membership can be sufficiently accounted for by the more parsimonious higher order factors of psychopathology.
These results expand on previous Australian research that investigated the correlation structure of multiple lifestyle risk behaviours via testing an increased number of statistical models. Previous work has focused on LCA alone, assuming that individuals could be categorized into homogeneous classes of health behaviours that differ qualitatively. For example, Gardner et al. (2020) identified three clusters of the Big 6 among females of a similar age to the present sample (12–15 years; Mage = 13.82 years, SD = 0.88): one class characterized by relatively low risk, another by high screen time coupled with physical inactivity and poor sleep, and a third by physical activity and a healthy diet. However, among older adolescents (16–20 years; Mage = 18.88 years, SD = 0.42), Champion et al. (2018) identified similar classes to Gardner et al. (2020), with the addition of a class characterized by alcohol and tobacco use. However, the current results provide some evidence that the correlation structure of the Big 6 may be described using a single dimensional factor representing overall risk behaviours (i.e. non-normally distributed) and the population can be categorized based on differences in mean scores on this factor, rather than qualitative differences. These findings are somewhat consistent with previous research that found limited utility of qualitatively different latent classes over and above a simple continuous sum score of lifestyle behaviours (Wright et al., 2020).
Contrary to previous research on the correlation structure of health behaviours, where the majority of the samples have fallen into lower risk/healthy groups (Champion et al., 2020; Gardner et al., 2020; Wright et al., 2020), most of the current sample (67%) fell into the moderate-risk group, which was associated with greater psychopathology than the relatively low-risk group. Given all groups exhibited risky levels of screen time and physical inactivity, this may reflect trends of increasingly sedentary lifestyles (Yang et al., 2019) and highlights that adolescents continue to be at risk for psychopathology without necessarily engaging in traditional risk behaviours like alcohol and tobacco use. In line with the displacement hypothesis, spending time on screens may displace time spent in other activities that are protective of mental health, such as playing sport (Vella et al., 2019); however, evidence to suggest screen use displaces time spent in overall physical activity is weak (Pearson et al., 2014). Another potential mechanism for this association might be that increased screen time and physical inactivity lead to dysregulated sleep patterns that may further contribute to heightened psychopathology (Xu et al., 2019); however, further longitudinal and causal modelling is required.
Despite trends of decreasing alcohol and tobacco use among adolescents (Patalay and Gage, 2019), the high-risk group was primarily demarcated by alcohol and tobacco use which suggests that those who use these substances still represent a subgroup who demonstrate the highest rate of psychopathology, relative to the remainder of the population. The finding that the moderate- and high-risk groups differed in terms of externalizing, but not internalizing, may relate to the role of alcohol. Alcohol use has consistently been linked with externalizing problems during adolescence, but studies investigating links with internalizing problems have produced mixed results (Ning et al., 2020). Externalizing problems are underpinned by behavioural disinhibition and deviant behaviour which is thought to explain the links with alcohol use (Mezquita et al., 2018). In contrast, negative reinforcement and self-medication theories suggest that those with internalizing problems may use alcohol to avoid negative emotions (Hussong et al., 2011; Mezquita et al., 2018). Although some studies support these hypotheses, others have reported negative or no links between internalizing and alcohol use (Hussong et al., 2017; Ning et al., 2020). Explanations often centre on the differing forms of internalizing problems. For example, while depression has consistently been linked to alcohol use, evidence around anxiety is inconclusive, with some forms of anxiety, such as social anxiety, thought to lower risk of alcohol use due to reduced opportunities to engage in deviant behaviours (Hussong et al., 2017; Ning et al., 2020). Some studies have reported that the relationship between anxiety and alcohol use changes over time, with increased risk of alcohol use emerging later in adolescence (Hussong et al., 2017). We also note that recent trends show increases in depression, conduct and hyperactivity symptoms among adolescents, while substance use is decreasing (Patalay and Gage, 2019). These findings, along with those of the present study, suggest that there may be complex interactions with other health behaviours that explain links with psychopathology, and these may be changing over time.
The current study found that physical inactivity was a poor indicator of class membership, therefore precluding the ability to examine the specific influence of MVPA on psychopathology. Previous research has consistently identified links between physical inactivity and internalizing disorders, while links with externalizing disorders have been less consistent (Monshouwer et al., 2012; Spruit et al., 2016). Inspection of the factor loadings of the risk behaviours may provide some explanation for these findings. Physical inactivity demonstrated relatively low loadings in comparison to the other risk behaviours and may indicate that physical inactivity represents a stand-alone factor or secondary correlated factor. A sensitivity analysis examining the model fit statistics of the LCA, IFA and FMM without the inclusion of the MVPA indicator was conducted and the results were substantively the same (see Supplementary Table 4). Likewise, the description of the latent classes without the MVPA indicator was similar (see Supplementary Figure 1). Additional follow-up exploratory modelling was conducted by regressing internalizing and externalizing on just physical inactivity as an observable outcome. In this model, the associations were similar to those found in the previous literature, with higher scores on internalizing significantly and positively associated with increased odds of physical inactivity (OR = 1.20, 99% CI = [1.3, 1.41]) whereas there was no evidence for an association between physical inactivity and externalizing (OR = 0.89, 99% CI = [0.72, 1.10]). Given the diagnostic criteria for depression include a reduction of physical movement and fatigue/loss of energy, the link between physical inactivity and internalizing is unsurprising (American Psychiatric Association, 2013). On the contrary, some externalizing symptoms, such as conduct problems, are associated with increased physical activity (Brodersen et al., 2005). Furthermore, the more tenuous link between externalizing and physical inactivity could potentially be explained by sex differences, with adolescent males typically more likely to exhibit externalizing symptoms and be physically active, compared to females who are more likely to exhibit internalizing symptoms and have lower rates of physical activity (Active Healthy Kids Australia, 2016; Iglesias Gallego et al., 2020; Lawrence et al., 2015; Spruit et al., 2016).
Finally, the finding that most of the associations between lower order factors of psychopathology and the lifestyle risk behaviours can be accounted for by the more parsimonious higher order factors complements existing research among adults and provides evidence for the utility of the HiTOP approach among adolescents (Slade, 2007; Van de Pavert et al., 2017). These findings support a shift from individual risk behaviours and specific psychopathological conditions to multiple lifestyle risk behaviours and a hierarchy of broad dimensions of psychopathology to inform prevention and early intervention efforts. Multiple health behaviour change and transdiagnostic interventions may be particularly valuable for young people, given the high prevalence of lifestyle risk behaviours, psychopathological comorbidity and rapid developmental changes within this population (Chu et al., 2016; McElroy et al., 2018; Spring et al., 2012). Adopting these approaches could lead to more efficient universal prevention interventions, and targeted approaches could be tailored to the identified risk groups. For example, if we assume there are causal relationships between the pattern of behaviours and psychopathology identified in this study, interventions that target broad levels of externalizing and internalizing behaviours may have flow-on effects in improving multiple lifestyle risk behaviours. Alternatively, much of the existing evidence around risk factors for the hierarchical dimensions of psychopathology has identified unmodifiable (e.g. genetics) or limited-modifiable risks (e.g. personality characteristics) (Lynch et al., 2021). The identification of modifiable lifestyle behaviours as risk factors for internalizing and externalizing is therefore novel and offers increased potential for preventing and treating psychopathology. However, the current study was not able to examine the potential causal nature of lifestyle risk behaviours and psychopathology. Additional longitudinal research, as well as randomized controlled trials of interventions to reduce broad factors of psychopathology, is required to investigate how changes might alter or interact with lifestyle risk behaviours over time.
Limitations of the research include the inability to infer causation and directionality of relationships due to cross-sectional data, the use of self-report measures which may have resulted in over- or under-reporting, and that measurement invariance across the comparison groups was assumed. Although the sampling design did not seek to obtain a representative sample, the sample was larger and more diverse than that used in previous research exploring the correlation structure of the Big 6 among adolescents (Gardner et al., 2020), including a gender distribution similar to that of the Australian population. Regarding the latent models, physical inactivity was a relatively poor discriminating indicator of the latent classes. To better discriminate between scores on the latent factor, it may be useful to consider other facets of behaviours or other approaches to measure physical activity, such as movement tracking or accelerometers, which provide a more nuanced and objective approach. It is also important to recognize that psychopathology and engagement in risk behaviours, such as alcohol and tobacco use, is likely to change throughout adolescence (Australian Institute of Health and Welfare, 2017). Although previous research among samples of a similar age (Gardner et al., 2020), and older adolescents (Champion et al., 2018), identified some similar patterns of behaviours, the present findings are limited to 11–14 year olds and may not generalize to older adolescents. Longitudinal research exploring changes in classes, or shifts between classes, may be useful. Finally, although sex differences were not examined in the present study, given there is evidence that patterns of risk behaviours vary according to sex (Wright et al., 2020), and that recent trends of increasing psychopathology are largely driven by increases among females (Patalay and Gage, 2019), future research could benefit from exploring interactions with sex.
Conclusion
Adolescence is a key period for psychopathology which coincides with the emergence of the Big 6. This study highlights that the correlation of these key behaviours can be accounted for by three classes that differ in mean scores on a single dimension of overall risk and relate to varying levels of hierarchical dimensions of psychopathology. Notably, the largest group, characterized by moderate risk, was associated with a greater rate of psychopathology in comparison to the low-risk group, despite not exhibiting traditional risk behaviours like alcohol and tobacco use that were observed in the high-risk group. These findings may inform prevention and early intervention efforts to address lifestyle risk behaviours and psychopathology during adolescence.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221080406 – Supplemental material for Multiple lifestyle risk behaviours and hierarchical dimensions of psychopathology in 6640 Australian adolescents
Supplemental material, sj-docx-1-anp-10.1177_00048674221080406 for Multiple lifestyle risk behaviours and hierarchical dimensions of psychopathology in 6640 Australian adolescents by Lauren A Gardner, Katrina E Champion, Cath Chapman, Nicola C Newton, Tim Slade, Scarlett Smout, Maree Teesson and Matthew Sunderland in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The Health4Life study was led by researchers at the Matilda Centre at the University of Sydney, Curtin University, the University of Queensland, the University of Newcastle, Northwestern University and UNSW Sydney: Teesson, M., Newton, N.C., Kay-Lambkin, F.J., Champion, K.E., Chapman, C., Thornton, L.K., Slade, T., Mills, K.L., Sunderland, M., Bauer, J.D., Parmenter, B.J., Spring, B., Lubans, D.R., Allsop, S.J., Hides, L., McBride, N.T., Barrett, E.L., Stapinski, L.A., Mewton, L., Birrell, L.E., & Quinn, C. & Gardner, L.A. The authors would like to acknowledge all the research staff who have worked across the study, as well as the schools, students and teachers who participated in this research. The research team also acknowledges the assistance of the New South Wales Department of Education (SERAP 2019006), the Catholic Education Diocese of Bathurst, the Catholic Schools Office Diocese of Maitland-Newcastle, Edmund Rice Education Australia, the Brisbane Catholic Education Committee (373) and Catholic Education Western Australia (RP2019/07) for access to their schools to conduct this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The Health4Life study was funded by the Paul Ramsay Foundation and the Australian National Health and Medical Research Council via Fellowships (K.E.C., APP1120641; M.T., APP1078407; and N.C.N., APP1166377) and via a Centre of Research Excellence in the Prevention and Early Intervention in Mental Illness and Substance Use (PREMISE; APP11349009). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.