
Abstract
Aims:
Medication cessation and service disengagement often precedes relapse in people with severe mental illnesses but currently specialist mental health services only become involved after a relapse. Early detection of non-adherence is needed to enable intervention to avert relapse. This paper aims to demonstrate how digitally automated non-adherence risk monitoring from Medicare data with active follow-up can work and perform in practice in a real-world mental health service setting.
Methods:
AI2 software is an automated risk monitoring tool to detect non-adherence using Medicare data. It was implemented prospectively in a cohort of 354 registered patients of a community mental health clinic between July 2019 and February 2020. Patients flagged as at risk by the software were reviewed by two clinicians. We describe the risks automatically flagged for non-adherence and the clinical responses. We examine differences in clinical and demographic factors in patients flagged at increased risk of non-adherence.
Results:
In total, 46.7% (142/304) were flagged by the software as at risk of non-adherence, and 22% (31/142) received an intervention following clinician review of their case notes. Patients flagged by the software were older in age and had more prior mental health treatment episodes. More alerts were associated with patients who had been transferred from the mental health service to the care of their general practitioners, and those with more alerts were more likely to receive a follow-up intervention.
Conclusion:
Digitally automated monitoring for non-adherence risk is feasible and can be integrated into clinical workflows in community psychiatric and primary care settings. The technology may assist clinicians and services to detect non-adherence behaviour early, thereby triggering interventions that have the potential to reduce rates of mental health deterioration and acute illness relapse.
Introduction
Antipsychotic, antidepressant and mood-stabilising medications are highly effective in reducing the risk of relapse for acute mental illness and are therefore routinely prescribed in the maintenance treatment of severe mental illnesses such as schizophrenia (Leucht et al., 2012), bipolar disorder (Vieta et al., 2011) and major depressive disorder (Sim et al., 2015). A meta-analysis found that in patients treated with antipsychotic medications who discontinued medication after clinical remission, the risk of relapse was 78% at 24 months and 84% at 36 months (Fusar-Poli et al., 2016). This is concerning given that at least half of patients who have been prescribed antipsychotics are either non-adherent or only partially adherent to medication protocols (Leucht and et al., 2015; Yaegashi et al., 2020). Some estimates suggest over 80% of patients relapse several times within the first 5 years of initial treatment (Valenstein et al., 2002), leading to adverse effects on the trajectory of the illness, worsening symptomatology and ultimately increases in public health costs (Knight, et al., 2018). Given the importance of maintenance of medication and service engagement in avoiding relapse and potential hospitalisation, improving adherence is a priority (Masand et al., 2009).
Non-adherence with psychotropic medications and service engagement is a complex phenomenon. While some patients actively choose to discontinue medication from a well-informed and considered standpoint, others may discontinue for other reasons. These can include intolerable side effects (Kim et al., 2020; Kreyenbuhl et al., 2009), poor understanding of the need for ongoing treatment due to impaired illness insight (Kim et al., 2020), the prescriptions not being discussed collaboratively (Kreyenbuhl et al., 2009), experiencing little benefit from medications (Lieberman et al., 2005) or due to circumstances such as forgetfulness, homelessness (Teesson et al., 2004) or transience (Gilmer et al., 2004).
Even though the risk of relapse increases with non-adherence (Tiihonen et al., 2017), patients usually only receive an intervention targeted at medication adherence after relapse has occurred. Patients identified as having relapsed due to non-adherence may receive short-term targeted interventions such as medication reviews, compliance aids, more frequent clinician contacts in the community or hospitalisation. However, due to resource limitations, mental health clinicians are not equipped to monitor non-adherence behaviour reliably in the long term. In addition, over 30% of patients with schizophrenia or bipolar disorder do not require long-term tertiary mental health support (O’Reilly et al., 2015), and as such these people receive their prescriptions and psychiatric monitoring from their general practitioner (GP) whose time to assess medication adherence is limited.
Automated and objective medication and service engagement monitoring across the course of the illness, when combined with standard care, could provide added value for both patients and clinicians. For example, clozapine patient management system uses an electronic database to monitor and improve adherence of clozapine patients (Takeuchi et al., 2020). The clozapine database allows clinicians to detect non-adherence and service disengagement thus generating an alert or action. Similar management of patients on other psychotropics requires a low cost, scalable, integrated and easily implementable database. In Australia, the Medicare universal health system maintains a near real-time record of all medical occasions of service received by all patients and all prescriptions collected from pharmacies. We have developed a software application – AI2 (an extension of MyHR conformant software HealthTimeline) – that is automated to detect risk of non-adherence and disengagement using the Medicare data in near real time. By monitoring prescription refills, medication reviews and laboratory testing, we can determine patterns in these data for individuals on psychotropic medication treatments. The application alerts clinicians when risk observations are detected in the data: (a) lapsed script refills, (b) bi-annual mental health care plan reviews by the GP has not occurred in the preceding 6 months and (c) annual blood test screening for metabolic syndrome (e.g. HbA1C, lipids) not carried out in the preceding 12 months (Bidargaddi et al., 2018). The system requires no data entry by patients, uses routinely collected electronic data and is scalable nationally.
This study aimed to test the feasibility of the automated Medicare claims enabled risk monitoring software for non-adherence and disengagement in a real-world mental health service setting. We conducted an 8-month prospective trial of the AI2 software with the full range of community psychiatric patients prescribed ongoing psychotropic medications. We report implementation methodology, describe automatically flagged non-adherence and disengagement risks and clinical responses, and examine differences in clinical and demographic factors in patients flagged at increased risk of non-adherence.
Methods
Automated adherence risk monitoring software
The AI2 software uses Medicare claims data from Australia’s national electronic health record, My Health Record (MyHR), to determine whether patients’ records of attendance for medical appointments from the Medical Benefit Schedule (MBS) and prescription refill records from the Prescription Benefit Schedule (PBS) reflect treatment appropriate for their condition (Knight et al., 2018). Algorithms in the software generate alerts when prescriptions have not been refilled, and when 6 monthly appointments for mental health care plan review with the GP have not occurred around expected times. Alerts are visually presented in a dashboard along with a timeline visualisation of all previous claims records (Figure 1). The decision rules for generating alerts are derived from best practice guidelines for the treatment of schizophrenia, bipolar disorder and major depression (Galletly et al., 2016; Malhi et al., 2015). For example, the algorithms were designed to detect whether a patient with schizophrenia picks up prescriptions for oral antipsychotic medication on a regular monthly basis and is medically reviewed at least every 6 months. Working details of the AI2 software and algorithms have been published previously (Bidargaddi et al., 2018).
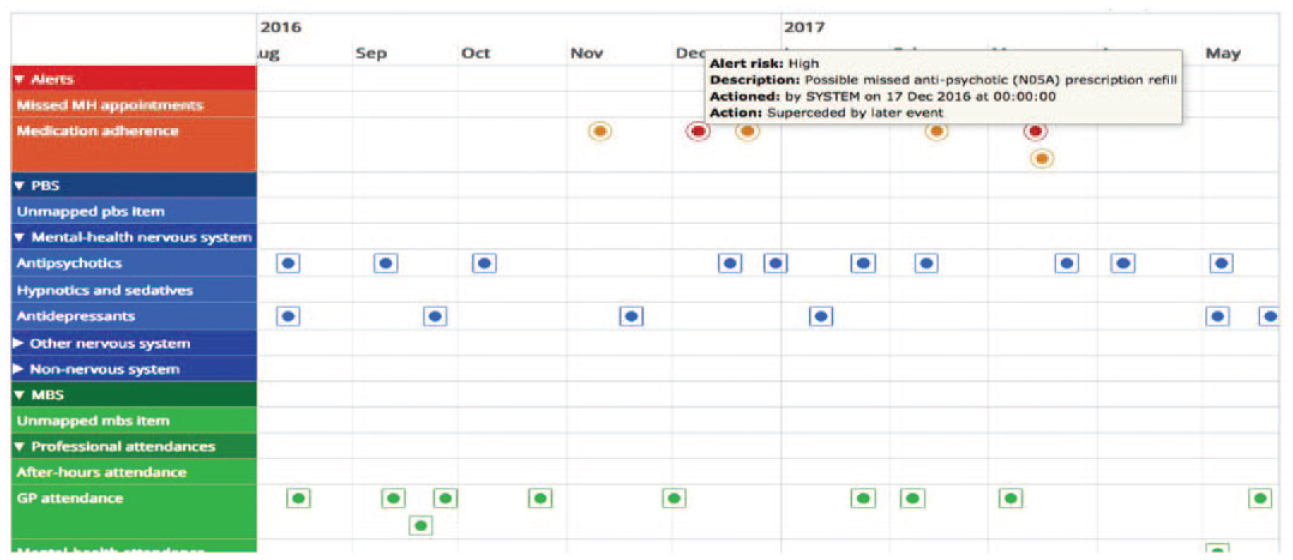
A timeline visualization of each patient showing interactions with different providers with alerts shown when patterns of interaction are deviating from best practice.
Study site
The site for the AI2 software implementation was the Inner North Community Health Service, located in Gawler, South Australia. The mental health team comprised 10 Case Managers from a multidisciplinary background supervised by a Psychiatrist, a Clinical Nurse Consultant and a Team Leader. The service catchment has a population of approximately 52,000 (2016 census data). The study protocol was approved by the Southern Adelaide Local Health Network Clinical Research Ethics Committee and published (Oakey-Neate et al., 2020).
Patient inclusion criteria
Patients included for risk monitoring between 1 July 2019 and 28 February 2020 were (a) registered in the patient information system, (b) seen by the clinic at least once between 1 January 2019 and 30 June 2019, (c) had not opted out of MyHR and (d) were prescribed psychotropic medications at the commencement of the study. Patient diagnoses included schizophrenia, schizo-affective disorder, bipolar and other mood disorders and were made by clinic psychiatrists or referring services or GPs.
Procedure
Patient enrolment details were uploaded on to the AI2 software by the clinic’s administrative staff on 1 July 2019 and data were monitored until 28 February 2020. Two clinicians were given access to the dashboard to monitor the alerts (Figure 1), and a Local Work Site Instruction Manual was developed to integrate monitoring into usual workflows of patient care. My Health Records Act (2012) s.61.1 provides clinicians with rights to access the MyHR of patients without requiring explicit consent of patients for the purposes of care provision use cases. The MyHR data of patients on AI2 is only accessible to clinicians who are involved in their care.
The two clinical monitors reviewed all alerts that were displayed on the dashboard between 1 July 2019 and 28 February 2020. They assessed an alert as not requiring further action if there was an obvious clinical explanation for the alert on review of information available from the patient case notes. After investigating each alert, an outcome response, either ‘actioned’ or ‘not requiring action’, was recorded in the software along with reasons in an accompanying free text field.
For each ‘actioned’ alert, the patient was contacted by the case manager, the clinical monitors or by their GP. For case managed patients, the clinical monitor asked the responsible case manager to follow up. The case manager then followed up either with the patient directly or their carer, boarding house facilities, pharmacies or GPs to ascertain the patient’s clinical status. Once investigation and intervention were concluded, the case manager emailed the clinical monitor who entered the details of interactions into the AI2 software. If the patient had not been actively case managed or had been discharged from the service, then the clinical monitor themselves followed the same procedure. If the patient could not be contacted by either the case manager or the clinical monitor, then their GP was contacted and asked to investigate the patient’s non-adherence at the next opportunity. This approach was taken to ensure that the intervention was experienced by GPs as aiding their care rather than as an unwarranted intrusion. For this study, we retrieved de-identified alerts and assessments of alerts by clinicians.
Patient characteristics
We retrieved data from the electronic health records of the local mental health service regarding the following patient characteristics: age, gender, number of admissions to hospital or new episodes of care in the community in the previous 4 years, and current status of care, that is, case managed or discharged, applicable at the time of registration with the AI2 software. As indicators of clinical severity, we retrieved from the electronic health records the Health of the National Outcome Scale (HoNOS) scores, administered within 3 months of adherence monitoring commencing. The HoNOS is a validated clinician-rated scale providing assessment of severity and functional impairment of mental illness. It consists of 12 items measuring 4 broader categories: behaviour, impairment, symptoms and social functioning, with scores ranging between 0 and 48, and reliable psychometric validity with scores over 13 considered to indicate a severe level of impairment (Pirkis et al., 2005).
Data analyses
Descriptive statistics derived were means (M) and standard deviations (SD) for continuous variables and proportions (%) for categorical variables. Patients who had at least one system generated alert between 1 July 2019 and 28 February 2020 were included in the alert group, and the remainder formed the non-alert group. Clinical monitors’ responses to all alerts generated between 1 July 2019 and 28 February 2020 recorded as either ‘requiring no action’ or ‘action to be taken’ were obtained from the AI2 software. Independent Welch approximation t-test and chi-square tests were conducted to investigate differences in patient characteristics between alert and non-alert groups, and by the type of response indicated by the clinical monitor in patients who had alerts.
Results
Overview of monitored patients
In total, 304 patients meeting the inclusion criteria were prospectively monitored for risk of non-adherence between July 2019 and February 2020 using AI2 software. Among the study sample, 51.6% (157/304) were females with an average age of 41.1 years (SD = 17.8). The mean HoNOS score was 11.2 (SD = 7.2) and the mean number of admissions in the previous 4 years was 1.4 (SD = 1.3). Based on care status at recruitment, 53.5% (152/284) had been discharged to GPs in the previous 6 months, while the remaining were actively case managed by the mental health service. The GP care group had a higher number of historical episodes of community care (M = 1.6, SD = 1.1 vs M = 1.1, SD = 1.4, t(282) = 3.1, p < 0.001) and were younger (M = 37.8 years, SD = 19.2 vs M = 45.2 years, SD = 15.2, t(282) = −3.6, p < 0.001), compared to the case managed group. There were no differences by gender or HoNOS scores.
Patients flagged by software
The software flagged 46.7% (142/304) patients as being at increased risk of non-adherence, with an average of 2.0 (1.4) alerts per flagged patient. Figure 2 shows the distribution of types of alert.
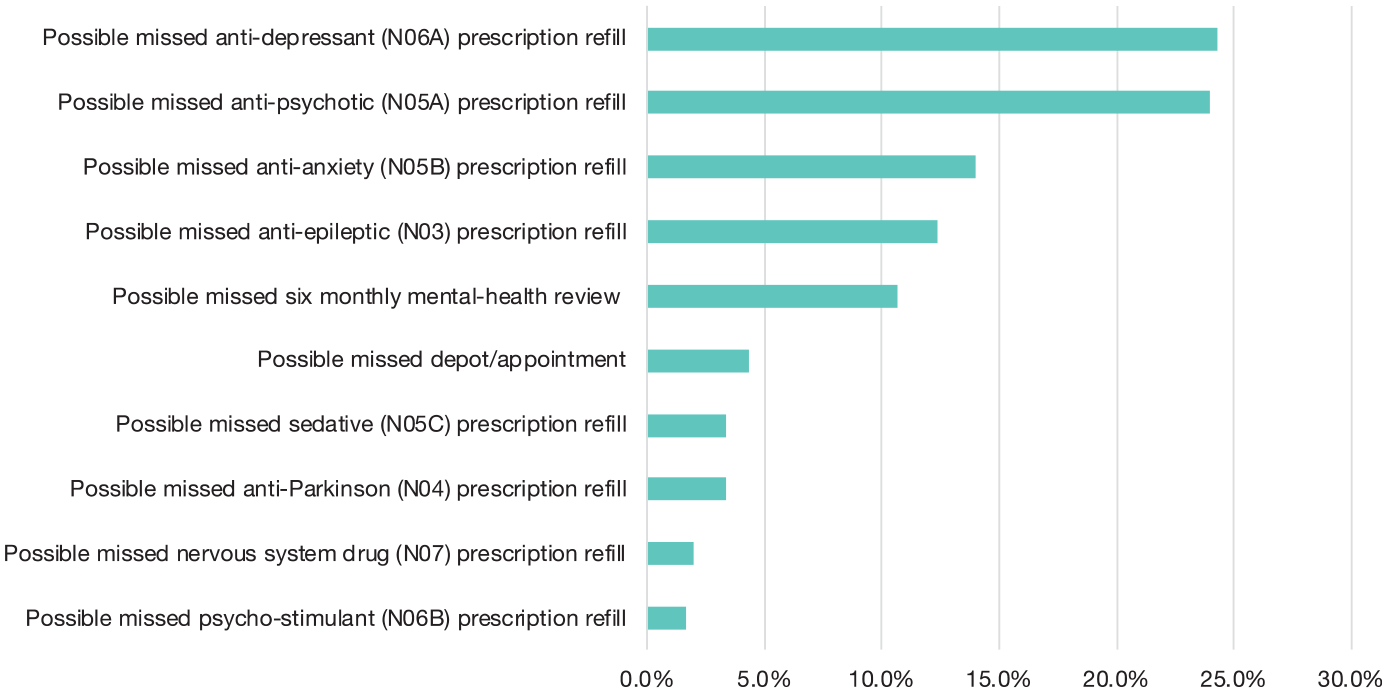
Distribution of types of alert.
Out of 142 patients with alerts, 111 patients were judged as ‘requiring no further action’ after their case notes were reviewed by the clinical monitors, as there were either appropriate clinical explanations for why the alert had been generated or a recent clinical intervention explaining the change in management. In 31 cases, there was no obvious clinical explanation for the alert and hence specific follow-up action was taken. Figure 3 shows the distribution of clinical responses (actioned vs no action taken) for the 10 different alert categories. The majority of alerts resulting in patient contact arose from three categories: missed antipsychotic refills, missed depot appointment and missed antidepressant refills.
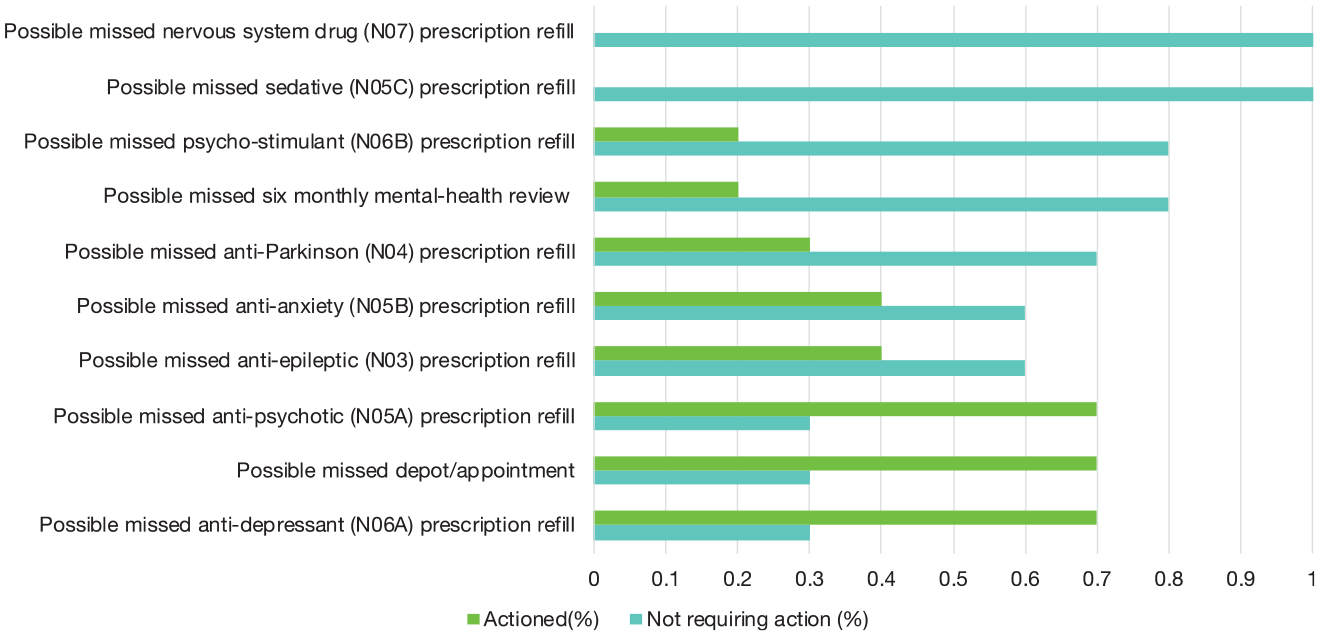
Clinical response by alert type.
Patient differences between those with an alert and those without alerts
Table 1 compares characteristics of patients flagged as at increased risk of non-adherence with those not flagged. Flagged patients (M = 44.1 years, SD = 16.7) were significantly older (M = 38.5 years, SD = 18.3, t(302) = 2.8, p = 0.01). There was also a trend towards higher number of episodes of care in the last 4 years (M = 1.5, SD = 1.3 vs M = 1.2, SD = 1.2, t(282) = 1.9, p < 0.06). No differences were found with respect to the HoNOS scores of the patient or gender. Among all patients (n = 304), the GP care group trended towards having a higher number of alerts (1.4) compared to the case managed group (0.89), T = 1.8, p = 0.06.
Comparison of patients with alerts (n = 142) and without alerts (n = 162).
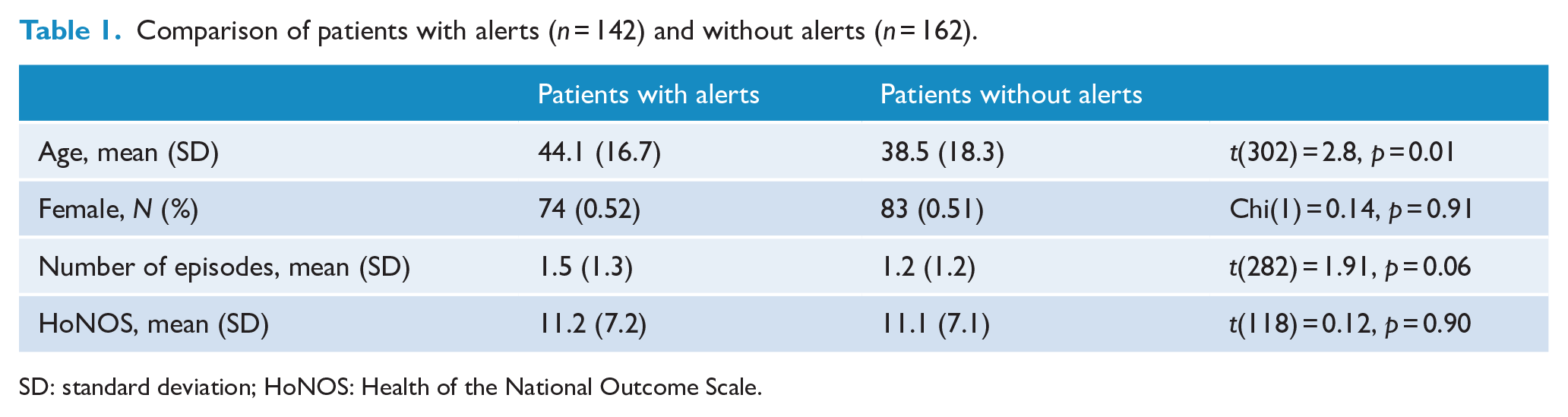
SD: standard deviation; HoNOS: Health of the National Outcome Scale.
Among all patients who had an alert (N = 142), patients whose alerts were actioned post-case note review had a significantly higher number of alerts (M = 2.9, SD = 2.0) compared to patients whose alerts were not actioned (M = 1.8, SD = 1.1, t(140) = 4.13, p < 0.001). No significant differences were found by gender, age, number of previous episodes or HoNOS sores (Table 2).
Patients with actioned alerts versus patients with non-actioned alerts.
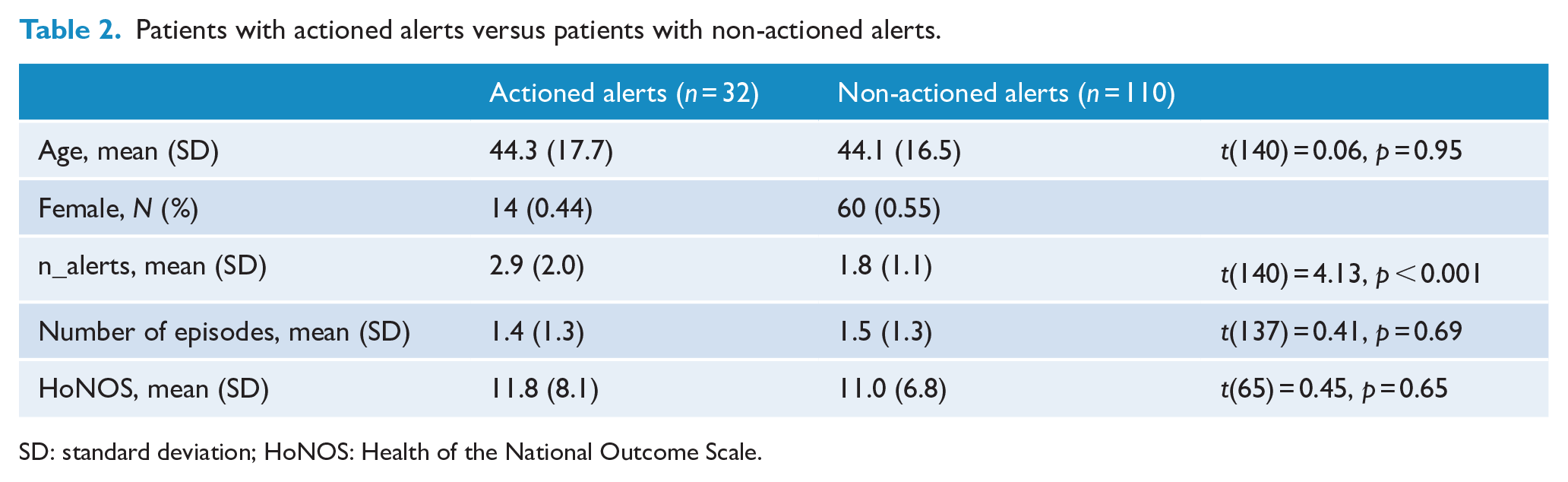
SD: standard deviation; HoNOS: Health of the National Outcome Scale.
Discussion
This study describes how a digitally automated monitoring system can operate in clinical practice. Previous automatic adherence measuring systems such as electronic monitoring of package entry (El Alili et al., 2016) have not been scalable, nor widely adopted. Since AI2 software integrates with existing clinical electronic health information systems to identify eligible patients, and relies on existing collected Medicare data, the adherence of nearly all registered clinic patients was able to be monitored, thus demonstrating the scalability of the system. Patients who were monitored spanned varied demographic and clinical characteristics and persons actively case managed by mental health services or person under GP care, showing that the system can monitor patients across the continuum of illness severity and phase of care.
In the span of 8 months, the software generated an alert for approximately one in two patients, but only one in five patients with alerts were assessed as needing further intervention following a brief review of their case notes. The case note review was a quick procedure (under 5 minutes per patient), and even more efficient when clinicians knew the patient well. This indicates the monitoring system has the potential to be relatively easily integrated into existing clinical workflows without over-burdening health practitioners. There were three main scenarios where it was judged that no follow-up action was required after case note review. First, when alerts were triggered by prescriptions used on a ‘when required’ basis. This most often occurred when benzodiazepines or other sedatives had been prescribed for short term of episodic use. Second, when drug packaging led to an alert being generated. For example, when the number of tablets in a pack exceeded the daily dosage prescribed by the doctor for that month. Third, when a mental health related GP billing alert occurred in a situation where there were other GP billing numbers billed in the preceding 6-month period. The algorithms generating alerts could easily be modified to exclude or automatically close alerts for the above three scenarios based on preferences of the clinician and thereby reduce workload for monitoring clinicians. Based on this the algorithm is being updated to automatically close alerts which will lead to even less requirement for clinical review and thereby further reduce workload for monitoring clinicians.
The low number of alerts of patients on depot medication indicated that the existing monitoring process was working well. The finding that a small number of patients prescribed long-acting injection medications (depot) were flagged by the system may indicate some patient resistance to that form of administration. Although the literature (Tiihonen et al., 2011) suggests that patients prescribed depot medication have lower relapse rates, paradoxically some patients may perceive this treatment modality as coercive, whereas oral medication, under their own control, may be perceived as more respectful of their collaborative engagement in treatment. On the contrary, the prescription of depot medications in psychiatric services may be skewed towards those patients who have had adherence difficulties in the past, and the persistence of non-adherence even when receiving depot medication may not be unexpected. Digital automated monitoring may allow patients to take oral medication with a subjective sense of empowerment and control while providing a safety net for early detection of non-adherence.
We found a trend for more alerts to be generated for patients who had been transferred to the care of their GPs than to those who were case managed in the clinic. This may be due to the more intense follow up in the community clinic and may suggest that this form of automated non-adherence risk monitoring may be particularly useful for patients who have been recently discharged from the community clinic to the less intense follow up of their GP. Of note, participants flagged with an alert by the software had more episodes with mental health services in the previous 3 years than those not flagged. This suggests that these patients may have had enduring problems with adherence to treatment extending back over several years. They may also have been patients with more severe forms of illness with higher relapse rates or a wider range of general psychosocial difficulty. However, we found no evidence that the number of alerts were associated with indices of functional impairment (HoNOS), supporting the notion that non-adherence behaviour represents a discrete phenomenon in mental healthcare that is associated with impairments of illness insight and that is particularly evident in a subset of patients (Kim et al., 2020). In our analysis, people with alerts were older than those without alerts – contrary to outcomes observed in some but not all other studies; where more problems with adherence were found in younger patients (Semahegn et al., 2020). Our finding may relate to the fact that in our cohort, there were a number of older chronic patients living in a local residential facility, many of whom may have had long-standing difficulties with adherence; additionally, public community mental health settings such as ours may be selective for older patients with more chronic forms of mental illness.
The monitoring system was easy to integrate with the electronic health systems used by the mental health clinic and, unlike other approaches, it did not require patients to enter data. The time devoted to the monitoring of the dashboard, reviewing case note entries and the various subsequent communications with case managers amounted to approximately 2 hours per week each by the two clinician monitors. Early qualitative feedback from clinicians suggest that they were also able to save time on routine calls, as they would only need to call the GP only when necessary (e.g. missing refills) rather than routinely calling for information (e.g. checking if every patient on depot has picked up refills). Limitations of the study included that we were unable to stratify patients by diagnosis due to the approach to data capture and second, data on treatment decisions and patient outcomes after an in-person assessment were not collected.
Conclusion
A distinctive novel contribution of our study is the successful demonstration of a readily available, automated software solution, rapidly translatable Australia-wide to support early detection of potential non-adherence and service disengagement among people with severe mental illnesses. Once scaled to larger clinical settings, the system may create further opportunities for integrated telehealth approaches potentially incorporating personalised reminders (text messages) in order to improve medication adherence or health practitioner attendance. Monitoring could be extended to identify contextual factors at both an individual and epidemiologic level contributing to non-adherence and disengagement. This could then result in the development of both individualised and systemised approaches to reducing medication non-adherence and service disengagement rates at a population level.
Footnotes
Acknowledgements
The implementation of AI2 software (AI2 digital support tool for mental illness project) has received 1-year funding through approved disbursements from the Medical Research Future Fund (MRFF) Rapid Applied Research Translation Program. We wish to acknowledge Barossa and Fleurieu LHN and SA Health administrative staff in providing support with the software maintenance and hosting. The AI2 digital support tool project wishes to acknowledge the MRFF and Commonwealth Department of Health in supporting this project. This project is part of the work being undertaken by the SA Academic Health Science and Translation Centre.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.